

Abstract
Schistosomiasis is a helminthic infection acquired through direct contact with contaminated fresh water. To the best of our knowledge, this is the first case pulmonary of schistosomias is evaluated with 18F-fluorodeoxyglucose (18F-FDG) positron emission tomography/computed tomography (PET/CT) reported in the literature. Functional imaging with 18F-FDG PET/CT may help in the diagnosis of schistosomiasis, leading to a correct definition of the disease extension.
Keywords: 18F-fluorodeoxyglucose, helminths, nuclear medicine, positron emission tomography, schistosomiasis
Introduction
Schistosomiasis is a helminthic infection and is endemic in tropical and subtropical regions, acquired through direct contact with contaminated fresh water.[1] In humans, this tropical parasitic disease is caused by the species Schistosoma haematobium, Mansoni, and Japonicum. Pulmonary manifestations of this parasitic disease can be acute or chronic, leading to pneumothorax, pulmonary fibrosis, pulmonary hypertension, and the right-sided heart failure.[2] There have been numerous studies on the application of 18F-fluorodeoxyglucose (18F-FDG) positron emission tomography/computed tomography (PET/CT) in the diagnosis of pulmonary lesions. The whole-body 18F-FDG PET/CT imaging not only makes early detection of tumors possible but also allows the detection of infections: 18F-FDG has been proposed for imaging infection/inflammation according to the EANM/SNMMI Guideline for 18F-FDG use in inflammation and infection.[3]
Nevertheless, to the best of our knowledge, this is the first case of pulmonary schistosomiasis evaluated with 18F-FDG PET/CT reported in the literature.
Case Report
A 32-year-old Ethiopian male, who had recently moved to Italy, came to our hospital with dry cough for 5 months associated with night sweats, fever, asthenia, and weight loss. Hypereosinophilia (eosinophils cells 2000/mm3) and a high value of IgE (137 kU/l) were found in the blood. All microbiological analyses for the detection of pathogens were resulted negative. A chest X-ray showed only a slight enlargement of the left pulmonary hilum [Figure 1]. For fever of unknown origin, the patient underwent a PET/CT scan with 18F-FDG (injected dose 175 MBq). Images showed multiple hypermetabolic areas of consolidation in the left lung (maximum standardized uptake value [SUVmax]: 9.2 g/ml bw) and multiple lymph nodes with a high uptake of 18F-FDG in the left hilum (SUVmax 10.4 with a maximum diameter of 30 mm), the mediastinum (SUVmax 9.8 g/ml bw with a maximum diameter of 28 mm), and the neck region (SUVmax 5.7 g/ml bw with a maximum diameter of 10 mm) [Figure 2]. After lung biopsy, histological examinations showed eosinophilic granulomatosis in the parenchyma with associated Schistosoma haematobium eggs, with a final diagnosis of pulmonary schistosomiasis.
Figure 1.
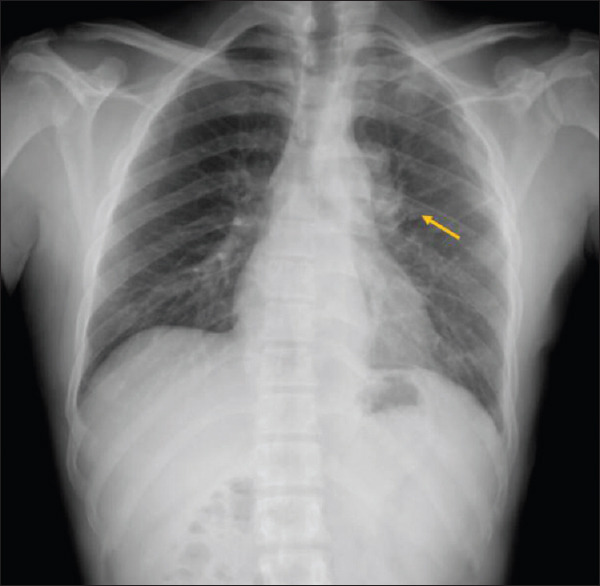
Chest X-ray shows a slight opacity in the left pulmonary hilum (orange arrow)
Figure 2.
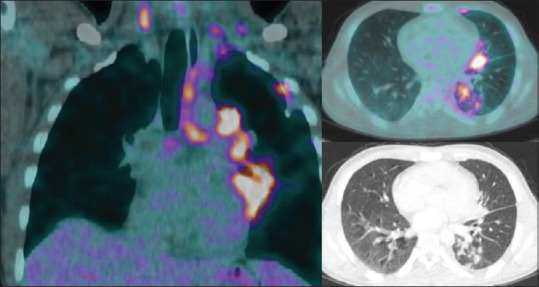
18F-fluorodeoxyglucose positron emission tomography/computed tomography and computed tomography images show multiple areas of consolidation with high uptake of 18F-fluorodeoxyglucose in the left lung and many hypermetabolic lymphadenopathies in the left pulmonary hilum, mediastinum, and neck region
Discussion
Schistosomiasis is infrequently seen in the Europe but remains an important cause of hematuria in endemic areas. The main human species are Schistosoma mansoni (endemic in Africa and South America) and Schistosoma japonicum (endemic in South and East Asia) causing intestinal and hepatosplenic involvement and S. haematobium (Africa). Acute schistosomiasis, a flulike syndrome, is a regular finding in travel clinics. Although the prevalence can be high, most infected people show limited, intermittent, or aspecific symptoms. Severe symptoms develop in predilected people with heavy and long-standing infections. The diagnosis of schistosomiasis relies on microscopic examination of stools or urine, serologic tests, and imaging.[4]
The role of 18F-FDG PET/CT imaging in infections/inflammation is well documented. The EANM/SNMMI guidelines recommended 18F-FDG PET/CT imaging in acute and chronic infection due to high levels of glucose transporters, and hexokinase and glycolytic activity of the cells involved and to an enhanced glucose consumption as a result of a stress reaction of the affected cells in response to cell damage (metabolic flare) in case of infections.[3] Some authors suggested the potential contribution of 18F-FDG PET/CT in the diagnosis of schistosomiasis: in a previous article concerning schistosomiasis, a pancreatic hypermetabolism has been reported. A mass-forming pancreatitis and granulomatous inflammation in old hepatic schistosomiasis mimicked metastatic pancreatic cancer on PET/CT have been described, with false-positive findings on CT, magnetic resonance imaging (MRI), endoscopic retrograde cholangiopancreatography, ultrasounds, and PET/CT suggestive of pancreatic cancer.[5] In 2016, hypermetabolism in the spinal cord schistosomiasis has been demonstrated.[6] Moreover, in 2019 Daghigh et al. presented an interesting case of a 36-year-old Eritrean patient with intestinal schistosomiasis evaluated with 18F-FDG PET/CT: the images showed enlarged lymph nodes below the diaphragm, widespread foci in peritoneum, omentum majus, terminal ilium, and ascites with increased metabolism.[7]
To the best of our knowledge, this is the first case of pulmonary schistosomiasis evaluated with 18F-FDG PET/CT reported in the literature and suggests that functional imaging may help in the timely triage and management of patients. The diagnosis was incidental, despite aspecific findings such as multiple hypermetabolic areas of consolidation in the lung and multiple supradiaphragmatic lymph nodes with increased metabolism, present in several inflammatory conditions, 18F-FDG PET/CT helped in clinching the diagnosis, leading to a correct definition of the disease extension.
Conclusions
We confirm the utility of 18F-FDG PET/CT imaging in the identification of schistosomiasis, helping the clinician in the diagnosis. Further studies are needed, but 18F-FDG PET/CT could be a useful tool for the evaluation of disease extension in schistosomiasis.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given his consent for his images and other clinical information to be reported in the journal. The patient understands that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Weber-Donat G, Donat N, Margery J. Acute pulmonary schistosomiasis: Computed tomography (CT) findings. Am J Trop Med Hyg. 2010;82:364. doi: 10.4269/ajtmh.2010.09-0425. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Chaudhry IU, Manah W, Alghamdi M, Mutairi H. Rare cause of asymptomatic solitary pulmonary nodule: Adult Schistosoma worm. [Last accessed on 2019 Nov 29];BMJ Case Rep. 2014 2014 doi: 10.1136/bcr-2013-202840. bcr2013202840. Available from: https://casereportsbmjcom/content/2014/bcr-2013-202840info . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Jamar F, Buscombe J, Chiti A, Christian PE, Delbeke D, Donohoe KJ, et al. EANM/SNMMI guideline for 18F-FDG use in inflammation and infection. J Nucl Med. 2013;54:647–58. doi: 10.2967/jnumed.112.112524. [DOI] [PubMed] [Google Scholar]
- 4.Gryseels B. Schistosomiasis. Infect Dis Clin North Am. 2012;26:383–97. doi: 10.1016/j.idc.2012.03.004. [DOI] [PubMed] [Google Scholar]
- 5.Ye S, Wang WL, Zhao K. F-18 FDG hypermetabolism in mass-forming focal pancreatitis and old hepatic schistosomiasis with granulomatous inflammation misdiagnosed by PET/CT imaging. Int J Clin Exp Pathol. 2014;7:6339–44. [PMC free article] [PubMed] [Google Scholar]
- 6.Altinyay ME, Alharthi A, Alassiri AH, Syed GM. 18F-FDG hypermetabolism in spinal cord schistosomiasis. Clin Nucl Med. 2016;41:211–3. doi: 10.1097/RLU.0000000000001003. [DOI] [PubMed] [Google Scholar]
- 7.Daghigh A, Grüner JM, Mørup P. Intestinal FDG-PET/CT imaging of an Eritrean with schistosomiasis seen in Denmark. Eur J Hybrid Imaging. 2019;3:17. doi: 10.1186/s41824-019-0064-4. [DOI] [PMC free article] [PubMed] [Google Scholar]