

Abstract
Background.
Primary care Practice-based Research Networks (PBRNs) are critical laboratories for generating evidence from real-world settings, including studying natural experiments. Primary care’s response to the novel coronavirus-19 (COVID-19) pandemic is arguably the most impactful natural experiment in our lifetime.
The OCHIN PBRN and the BRIDGE-C2 Center: Evaluating the Impact of COVID-19.
We briefly describe the OCHIN PBRN of community health centers (CHCs), its partnership with implementation scientists, and how we are leveraging this infrastructure and expertise to create a rapid research response evaluating how CHCs across the country responded to the COVID-19 pandemic.
COVID-19 Research Roadmap.
Our research agenda focuses on asking: How has care delivery in CHCs changed due to COVID-19? What impact has COVID-19 had on the delivery of preventive services in CHCs? What PBRN services (e.g., data surveillance, training, evidence synthesis) are most impactful to real-world practices? What decision-making strategies were used in the PBRN and its practices to make real-time changes in response to the pandemic? What critical factors in successfully and sustainably transforming primary care are illuminated by pandemic-driven changes?
Discussion & Conclusions.
PBRNs enable real-world evaluation of practice change and natural experiments, and thus are ideal laboratories for implementation science research. We present a real-time example of how a PBRN ‘Implementation Laboratory’ activated a response to study an historic natural experiment, to help other PBRNs charting a course through this pandemic.
Background
Primary care Practice-based Research Networks (PBRNs) are critical laboratories for studying the implementation of evidence-based practices in real-world settings. Close partnerships have developed between some PBRNs and academic institutions to facilitate ongoing bidirectional learning, and leverage emerging opportunities to conduct research that is both grounded in and relevant to primary care.
Their infrastructure makes PBRNs well positioned to conduct transformative dissemination and implementation (D&I) research. D&I research is, in many ways, an extension of practice-based research. For more than 40 years, PBRNs have produced “practice-based evidence”1 and built the infrastructure needed to gather data on best practices for implementing change. PBRN research evolved from descriptive studies to intervention research, and then to innovative ideas about tailoring interventions, the need for practice facilitation, and using mixed methods to understand what worked, what did not, and why. This relates directly to D&I research, which is the study of approaches to promote the adoption and integration of evidence-based practices, interventions and policies into routine health care settings.2,3
Recently, the National Cancer Institute funded six Implementation Science Centers in Cancer Control (ISC3)4 to develop and evaluate innovations supporting the adoption of evidence-based cancer control interventions. One of the funded Centers, the Building Research in Implementation and Dissemination to close Gaps and achieve Equity in Cancer Control (BRIDGE-C2) Center, was launched in September 2019 with the overarching goal of advancing implementation science to improve rates of cancer screening and prevention and reduce disparities in such care experiences by underserved populations. The BRIDGE-C2 Center builds on a twelve-year partnership between the Oregon Health & Science University (OHSU) Department of Family Medicine and the OCHIN [not an acronym] PBRN (formerly known as the Safety Net West PBRN).5
This partnership between a newly emerging implementation science center and a PBRN with a history of conducting D&I research has the potential to accelerate the science of how to quickly implement practice changes in response to an urgent need, such as the novel coronavirus-19 (COVID-19) pandemic. In this commentary, we use the lens of the COVID-19 pandemic to describe the research response that occurred in parallel with and in response to a rapid clinical response that took place in the OCHIN PBRN’s member clinics. We outline the roadmap we used to harness our PBRN laboratory and the BRIDGE-C2 Center’s implementation science expertise to learn how community-based practices transformed care in response to the pandemic.
The OCHIN PBRN and the BRIDGE-C2 Center: evaluating the impact of COVID-19
The OCHIN PBRN, registered with the Agency for Healthcare Research and Quality in 2012, aims to “improve the health of underserved populations, enhance their quality of care, and inform health policy through research.”6 It began supporting pragmatic implementation science studies at its inception and since has grown a portfolio of 18 D&I research studies over eight years.7–15
OCHIN hosts a central Epic© electronic health record for its >600 community health center (CHC) members, as well as numerous other population health data and analytics tools (e.g., Epic’s Healthy Planet). (The term CHC encompasses many types of community-based health care, including Federally Qualified Health Centers and look-alikes, rural health centers, school-based health centers, and behavioral and dental clinics co-located with primary care.) OCHIN provides central support to help its member practices implement practice changes, including coaches, trainers, an online training library, and “site specialists” who are employees of the practices and trained by OCHIN as technical assistance experts. Characteristics of the OCHIN PBRN are highlighted in Table 1.
Table 1:
Characteristics of the OCHIN PBRN, Serving as the BRIDGE-C2 Center Implementation Laboratory
| Total number of practices, # | 518 | Patients seen ever, # | 2,556,652 |
| Rural practices, # | 69 | Patients seen in 2017, # | 1,109,201 |
| Practice type / services provided*, # | Total number of providers, # | 2,926 | |
| Primary care / FQHC / FQHC look-alike | 438 | Provider training, # | |
| School-based health center | 120 | Physicians (MD/DO) | 1,719 |
| Dental | 139 | Nurse Practitioners | 915 |
| Behavioral health | 213 | Certified Nurse Midwifes | 43 |
| Specialty | 68 | Physician’s Assistants | 247 |
Note that if a practice site has more than one type of department, they are counted in each category.
The BRIDGE-C2 Center built on a long-standing partnership between OHSU Family Medicine and the OCHIN PBRN.5,16,17 The PBRN is the Implementation Laboratory for the BRIDGE-C2 Center. We leveraged this existing infrastructure and expertise to create a rapid research response to evaluate how CHCs across the country responded and adapted to the COVID-19 pandemic. This response focused on the impact of COVID-19-driven changes on preventive care, with the understanding that from a D&I perspective, learnings based on preventive care may have relevance for many health and healthcare outcomes. Two key elements of our PBRN were critical for this rapid launch of our COVID-19 research: 1) data surveillance capabilities, and 2) centralized support for practice change.1,18–22
The need for this rapid response was clear. The National Association of Community Health Centers (NACHC) reported on May 1, 2020 that CHCs faced “extreme challenges to operations, staffing, and budgets” due to COVID-19. Specifically, since the start of the pandemic, weekly visits were reduced by about half; 54% of visits occurred virtually; 12% of health center staff were unable to report to work, and 1,810 of approximately 14,000 CHC sites were temporarily closed (some may be closed permanently).23 This presented a unique opportunity to study change in CHCs.
PBRN Rapid Response and COVID-19 Research Roadmap:
In the first two months of the pandemic, we began using real-time surveillance data to observe primary care changes across the PBRN. For example, in March 2020, we saw that CHCs in our PBRN increased telemedicine visits by over 2000%, while in-person office visits and lab/imaging encounters declined by 80% and 70%, respectively (see Table 2).
Table 2:
Total number of encounters by type, in >500 CHCs in the OCHIN PBRN between November 2019 and April 2020
| Nov 2019 | Dec 2019 | Jan 2020 | Feb 2020 | Mar 2020 | Apr 2020 | |
|---|---|---|---|---|---|---|
| Lab and Imaging | 30,172 | 28,702 | 32,862 | 30,391 | 25,021 | 7,421 |
| Telemedicine Visit | 1,990 | 1,934 | 2,070 | 1,922 | 50,135 | 54,817 |
| Office Visit | 374,650 | 384,313 | 451,714 | 442,156 | 349,556 | 70,640 |
This information allowed us to quickly develop research questions designed to build knowledge about successful practice change by studying the COVID-19-driven changes occurring in the PBRN, informed by a conceptual framework that blends the practice change model and the Strategic Implementation Framework:24,25 How has care delivery in CHCs changed due to COVID-19? What impact has COVID-19 had on the delivery of preventive services in CHCs? What PBRN services (e.g., data surveillance, training, evidence synthesis) are most impactful to real-world practices? What decision-making strategies were used in the PBRN and its practices to make real-time changes in response to the pandemic? What critical factors in successfully and sustainably transforming primary care are illuminated by pandemic-driven changes?
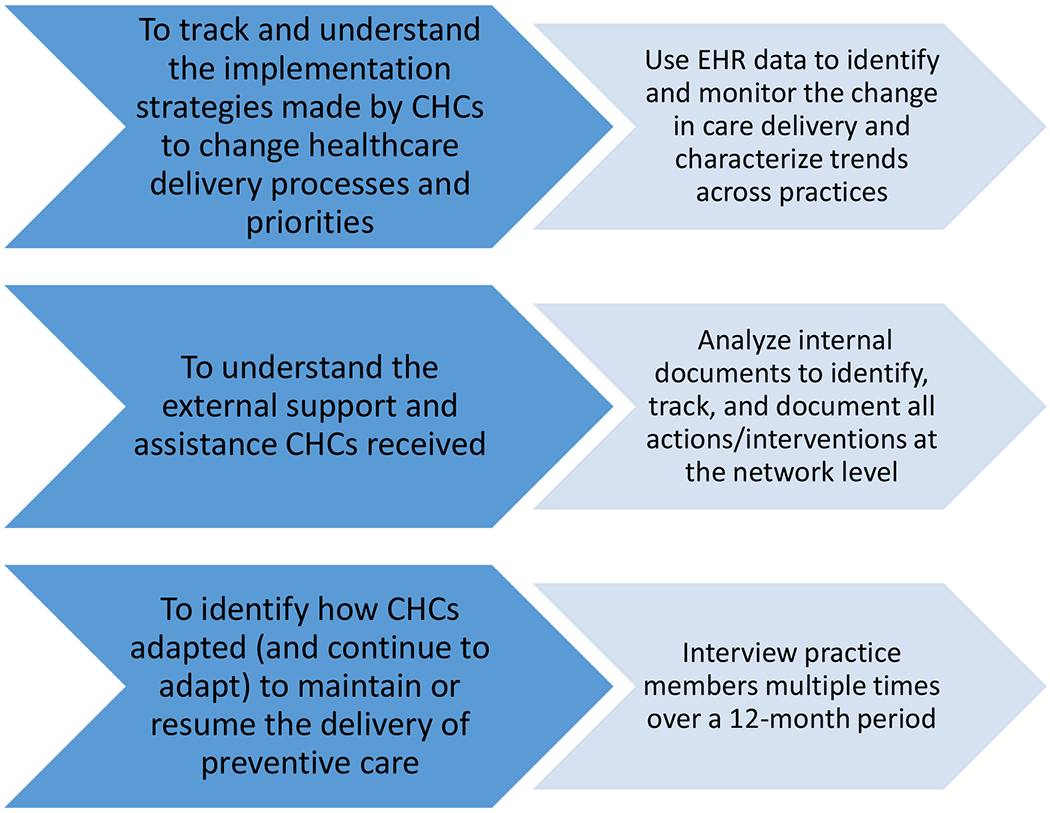
To track and understand how our PBRN’s CHCs implemented change in their care delivery processes and priorities, we are using EHR data to identify and monitor changes in care delivery and characterize trends across practices: visit types, personal portal use, COVID-19 testing, and services delivered over time. Additionally, because the OCHIN PBRN has CHCs in >20 states, we are assessing within- and across-state variations in how CHCs are responding. We are also considering that multi-level factors will be associated with practice variations in the response to COVID-19 and how they resume delivery of care. These include patient panel socio-demographic characteristics (e.g., race, ethnicity, insurance coverage); practice characteristics (e.g., state, number of patients); provider characteristics (e.g., number of clinicians); healthcare utilization (e.g., number of visits by types); and concurrent policy changes (e.g., payment for telehealth visits).
To understand the external support and assistance that our PBRN’s CHCs received to implement practice changes in response to the COVID-19 context, we are identifying, tracking, and documenting all actions taken to respond to the practices’ needs, including EHR modifications, telemedicine trainings, and requests from individual practices for centralized support and assistance. We will also interview practice members repeatedly over a 12-month period to identify how CHCs adapted (and continue to adapt) to maintain or resume the delivery of care. To do so, we are recruiting PBRN CHCs that: (1) had high performance on care quality indicators pre-COVID-19; and (2) are still actively delivering care, using in-person and / or telemedicine strategies, which suggests resilience and adaptive capacity.
CHCs are not representative of all primary care practices; there will be differences between the pandemic’s impacts on CHCs – and the changes they implemented in response – and those in other primary care practices. Thus, we created a matrix that stratifies the 600 CHCs in our PBRN by region, system / service organization, rurality, practice patient characteristics (e.g., rate of Hispanic, uninsured, complex patient). This stratification will help assess the extent to which findings of our assessments of implementation learnings from the COVID natural experiment may apply to other healthcare systems.
This mixed-methods research roadmap is designed to assess the implementation of practice changes made as a result of the COVID-19 pandemic, including multi-level barriers and facilitators; the development and use of documentation, training, and health information technology tools for this purpose; and the impacts of these changes on the quality of cancer prevention in the PRBN. This roadmap will inform developing interventions that aim to improve the delivery of primary care in general, and cancer preventive services in specific, in underserved populations. In future transformative events such as pandemics, earthquakes, etc, primary care will need to know how to expeditiously reconfigure itself for effectiveness, including: which visits can safely be done with telemedicine, what implementation strategies are most successful to assist with practice change, and what training is needed to support adoption of needed changes. These questions and more can be answered and accelerated by PBRNs partnering with D&I science centers.
Discussion & Conclusions:
The pandemic and primary care’s response to it are arguably among the most impactful natural experiments in our lifetime, presenting an unprecedented opportunity to demonstrate PBRNs’ power and value in supporting cutting-edge D&I science. PBRNs allow for real-world, real-time evaluation to generate practice-based evidence; here, we demonstrate how one PBRN’s structure supported learning from historic natural experiments. Pairing emerging implementation science centers with PBRNs with expertise in D&I research will accelerate and expand on this scientific work. As COVID-19-driven ‘natural experiments’ impact our society, we propose to harness the power and value of PBRNs to understand what primary care is doing now that we learn from to positively impact tomorrow. At the same time, we recognize that we are at risk of losing primary care practices and providers within our PBRNs. These losses will be devastating for the health of communities, but also the loss of valuable community laboratories for conducting research to inform primary care’s future. Thus, as COVID-19 uncovers the holes in our fragmented healthcare system and the inequities in our society, PBRNs and the primary care practices within these laboratories are needed now more than ever. The real-time example of how the BRIDGE-C2 Center is partnering with the OCHIN PBRN to rapidly respond to the need to study what is happening in this historic moment is presented to help other PBRNs chart a course through this pandemic.
Figure 1:
OCHIN PBRN’s COVID-19 Evaluation Building Blocks
Acknowledgements:
The authors gratefully acknowledge the participation of partnering community health centers in the OCHIN Community Health Information Network.
Funding statement: This publication was supported by the National Cancer Institute of the National Institutes of Health under award P50CA244289. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. This program is supported by funding provided through the Cancer Moonshot.
Footnotes
Conflicting and competing interests: The authors have no conflicts or competing interests to disclose.
References
- 1.Green LW. Making research relevant: if it is an evidence-based practice, where’s the practice-based evidence? Fam Pract. 2008;25 Suppl 1:i20–24. [DOI] [PubMed] [Google Scholar]
- 2.Century J, Cassata A, Rudnick M, Freeman C. Measuring enactment of innovations and the factors that affect implementation and sustainability: moving toward common language and shared conceptual understanding. J Behav Health Serv Res. 2012;39(4):343–361. [DOI] [PubMed] [Google Scholar]
- 3.Baumann AA, Morshed AB, Tabak RG, Proctor EK. Toolkits for dissemination and implementation research: Preliminary development. J Clin Transl Sci. 2018;2(4):239–244. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.National Cancer Institute Division of Cancer Control & Population Sciences. Implementation Science Centers in Cancer Control (ISC3). https://cancercontrol.cancer.gov/IS/initiatives/ISC3.html. Accessed January 30, 2020.
- 5.Devoe JE, Gold R, Spofford M, et al. Developing a network of community health centers with a common electronic health record: description of the Safety Net West Practice-based Research Network (SNW-PBRN). J Am Board Fam Med. 2011;24(5):597–604. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Agency for Healthcare Research and Quality. AHRQ PBRN Registry: OCHIN Practice-Based Research Network (formerly SafetyNet West). https://pbrn.ahrq.gov/pbrn-registry/ochin-practice-based-research-network-formerly-safetynet-west. Accessed June 10, 2020.
- 7.DeVoe JE, Hoopes M, Nelson CA, et al. Electronic health record tools to assist with children’s insurance coverage: a mixed methods study. BMC Health Serv Res. 2018;18(1):354. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.DeVoe JE, Huguet N, Likumahuwa-Ackman S, et al. Testing health information technology tools to facilitate health insurance support: a protocol for an effectiveness-implementation hybrid randomized trial. Implement Sci. 2015;10:123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Gold R, Bunce A, Cowburn S, et al. Adoption of Social Determinants of Health EHR Tools by Community Health Centers. Ann Fam Med. 2018;16(5):399–407. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Gold R, Bunce A, Cowburn S, et al. Cardiovascular care guideline implementation in community health centers in Oregon: a mixed-methods analysis of real-world barriers and challenges. BMC Health Serv Res. 2017;17(1):253. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Gold R, Cottrell E, Bunce A, et al. Developing Electronic Health Record (EHR) Strategies Related to Health Center Patients’ Social Determinants of Health. J Am Board Fam Med. 2017;30(4):428–447. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Gold R, et al. Challenges Encountered in Linking Community Health Centers’ EHR Data to a Web-based Clinical Decision Support Tool. Paper presented at: American Medical Informatics Association; Nov. 4, 2018; San Francisco, C.A. [Google Scholar]
- 13.Gold R, Hollombe C, Bunce A, et al. Study protocol for “Study of Practices Enabling Implementation and Adaptation in the Safety Net (SPREAD-NET)”: a pragmatic trial comparing implementation strategies. Implement Sci. 2015;10(1):144. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Gold R, Muench J, Hill C, et al. Collaborative development of a randomized study to adapt a diabetes quality improvement initiative for federally qualified health centers. J Health Care Poor Underserved. 2012;23(3 Suppl):236–246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Gold R, Nelson C, Cowburn S, et al. Feasibility and impact of implementing a private care system’s diabetes quality improvement intervention in the safety net: a cluster-randomized trial. Implement Sci. 2015;10:83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.DeVoe JE, Likumahuwa S, Eiff MP, et al. Lessons learned and challenges ahead: report from the OCHIN Safety Net West practice-based research network (PBRN). J Am Board Fam Med. 2012;25(5):560–564. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Heintzman J, Likumahuwa S, Nelson C, et al. “Not a kidney or a lung:” research challenges in a network of safety net clinics. Fam Med. 2014;46(2):105–111. [PMC free article] [PubMed] [Google Scholar]
- 18.DeVoe JE, Gold R, Cottrell E, et al. The ADVANCE network: accelerating data value across a national community health center network. J Am Med Inform Assoc. 2014;21(4):591–595. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Devoe JE, Sears A. The OCHIN community information network: bringing together community health centers, information technology, and data to support a patient-centered medical village. J Am Board Fam Med. 2013;26(3):271–278. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Crabtree BF, Miller WL, Stange KC. Understanding practice from the ground up. J Fam Pract. 2001;50(10):881–887. [PubMed] [Google Scholar]
- 21.Green LW, Glasgow RE, Atkins D, Stange K. Making evidence from research more relevant, useful, and actionable in policy, program planning, and practice slips “twixt cup and lip”. Am J Prev Med. 2009;37(6 Suppl 1):S187–191. [DOI] [PubMed] [Google Scholar]
- 22.Westfall JM, Mold J, Fagnan L. Practice-based research--”Blue Highways” on the NIH roadmap. Jama. 2007;297(4):403–406. [DOI] [PubMed] [Google Scholar]
- 23.National Association of Community Health Centers. National Findings on Health Centers’ Response to COVID-19 As of May 1, 2020. https://www.nachc.org/wp-content/uploads/2020/05/Health-Center-Response-to-COVID-19-Infographic-2pg-5.1.pdf. Accessed June 10, 2020.
- 24.Cohen D, McDaniel RR Jr., Crabtree BF, et al. A practice change model for quality improvement in primary care practice. J Healthc Manag. 2004;49(3):155–168; discussion 169–170. [PubMed] [Google Scholar]
- 25.Mitchell SA, Chambers DA. Leveraging Implementation Science to Improve Cancer Care Delivery and Patient Outcomes. J Oncol Pract. 2017;13(8):523–529. [DOI] [PMC free article] [PubMed] [Google Scholar]