

ABSTRACT
Conventionally, rennin–angiotensin–aldosterone system (RAAS) inhibition has focused on angiotensin-converting enzyme (ACE) inhibitors, angiotensin receptor blockers and angiotensin receptor-neprilysin inhibitors (ARNI) are the latest addition to this armamentarium. However, mineralocorticoid receptor antagonists (MRAs) also constitute an integral part of this anti-RAAS brigade, which are perceived more often as diuretics and are often under prescribed in heart failure (HF) despite being universally advocated by all major guidelines. Apart from HF, they have also shown promise in the management of hypertension, post-myocardial infarction, and hyperaldosteronism. Eplerenone, Food and Drug Administration (FDA) approved in 2002, is an acceptable alternative to spironolactone due to its sparing androgenic effects. In two big pivotal trials in heart failure (EMPHASIS -HF) and post-myocardial infarction (EPHESUS), the drug has firmly shown a reduction in adverse cardiovascular events. It has an established place in the management of resistant hypertension too. In this article, we will discuss the role of RAAS and its pathophysiology, pitfalls of spironolactone, which led to success of its congener, eplerenone, major studies conducted on eplerenone, current role of eplerenone, and comparison of the two MRAs.
KEYWORDS: Eplerenone, gynecomastia, heart failure, hyperkalemia, mineralocorticoid receptor antagonist, resistant hypertension
INTRODUCTION
Rennin–angiotensin–aldosterone system (RAAS) has been proven to be key pathological component of heart failure (HF) syndrome and blocking it has been shown to have mortality benefit and reduction in HF hospitalization (HHF) rates.[1,2] According to current guidelines, mineralocorticoid receptor antagonists (MRAs) should be implemented in therapy after an angiotensin-converting enzyme (ACE) inhibitor (or an angiotensin II receptor blocker [ARB] in intolerant patients) has been already initiated.[3] Spironolactone is more commonly used MRA of the two MRAs approved by Food and Drug Administration (FDA). Although it has shown to have mortality benefit, it has quite low acceptability rates due to its various side effects. There was a high need for developing a congener of this important drug, which worked similarly sans the unacceptable side effects. Eplerenone has emerged as an alternative and was approved by FDA in 2002. However, it was found that not only HF, but also MRA has garnered an important place in the field of medicine and is recommended as therapy of choice in resistant hypertension too. Because of its better side effect profile, eplerenone has become MRA of choice in current clinical practice.
ROLE OF RENNIN–ANGIOTENSIN–ALDOSTERONE SYSTEM IN HEART FAILURE AND MYOCARDIAL INFARCTION
RAAS is a major feature in HF pathophysiology, which works as a double-edged sword. For a failing heart, initially it works as an adaptation by increasing HR thus maintaining cardiac output (cardiac output = heart rate × stroke volume), but when unabated its key component, angiotensin II, it leads to a syndrome of HF. Sympathetic nervous system (SNS) augments RAAS activity. Natriuretic peptides-atrial natriuretic peptide (ANP) and brain natriuretic peptide (BNP) antagonize the RAAS and SNS by natriuresis and vasodilation. But they have short half-lives and are soon degraded by endopeptidases, thus allowing relentless progression of HF syndrome. Apart from the conventional RAAS inhibitors-ACE inhibitors, ARBs and MRA, angiotensin receptor-neprilysin inhibitor (ARNI) is the new addition to this armamentarium. Blocking RAAS is important due to the detrimental effects of AT II on heart, that is, arrhythmogenicity, exacerbation of myocardial ischemia, and cardiac hypertrophy [Figure 1].[4,5]
Figure 1.
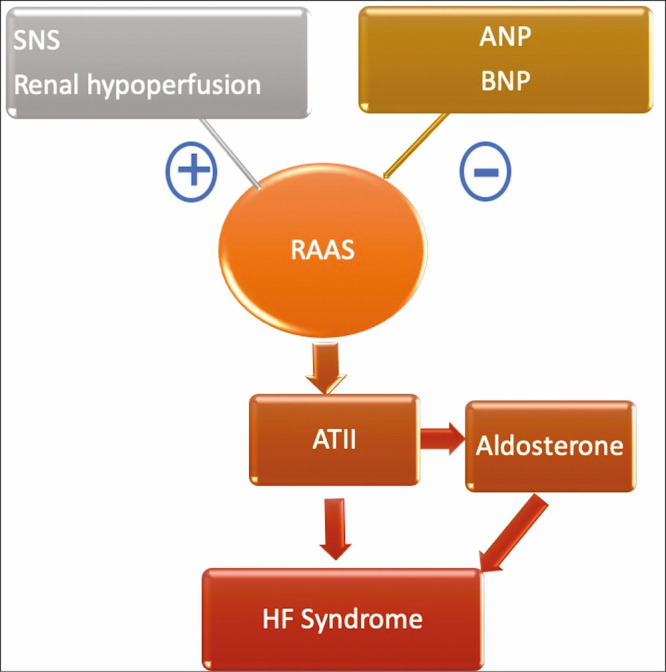
Heart failure syndrome resulting from angiotensin II: the key product of RAAS cascade. HF = heart failure, AT = angiotensin, SNS = sympathetic nervous system, ANP = atrial natriuretic peptide, BNP = brain natriuretic peptide
SPIRONOLACTONE AND PITFALLS
Aldosterone is a mineralocorticoid hormone which being profibrotic contributes to deleterious processes in various organs of body including heart.[1,6] Aldosterone exerts its effects partly via the intracellular mineralocorticoid receptor (MR). Signaling via the MR regulates salt and water balance, but also prompts inflammation, vasoconstriction, and oxidative stress, which ultimately leads to tissue fibrosis. Several large-scale studies in congestive HF have highlighted the beneficial effect of MR antagonism on survival, partly explained by decreased myocardial fibrosis.[2,7,8] Spironolactone reduces the risk of death from cardiac cause as well as all-cause mortality. Not only it decreases hospitalization in patients with heart failure with reduced ejection fraction (HFrEF), but also improves its symptoms as assessed by New York Heart Association (NYHA) functional class. These advantages of spironolactone are in addition to that of standard therapy with ACE inhibitors and β-blockers. Patient acceptability of spironolactone is good except in few patients where sexual side effects may occur due to its affinity for androgen and progesterone receptors. Side effects reported in men such as gynecomastia, breast pain, loss of libido, impotence, reduction of size of male genitalia and menstrual irregularities, loss of libido, and vaginal bleeding in women can be very unacceptable in some patients, which frequently lead to discontinuation of the drug [Figure 2]. In Randomized Aldactone Evaluation Study (RALES) trial, gynecomastia or breast pain was reported by 10% of the men in spironolactone group and 1% of the men in placebo group (P < 0.001). Another important side effect is serious hyperkalemia which was observed to occur in 10 patients in the placebo group (1%) and 14 patients in the spironolactone group (2%, P = 0.42), in the same trial.[7] Although there are not any head-to-head trials small-scale studies have shown higher incidence of hyperkalemia with spironolactone as compared to eplerenone which is primarily attributed to active metabolites and long half-life of the drug.[9] Testosterone appears to have a protective effect against cardiomyocyte apoptosis which is antagonized by spironolactone but not by eplerenone.[10] In a recent study, spironolactone has been shown to have a negative impact on metabolic parameters. It increases glycosylated hemoglobin (HbA1c) and serum cortisol and decreases plasma adiponectin.[11]
Figure 2.

Pitfalls of spironolactone. HbA1C = glycosylated hemoglobin
Eplerenone revisited
After extensive research in HF pathophysiology, RAAS has been found to be the key feature of HF syndrome; thus, the focus has shifted on inventing better drugs to target the same. Eplerenone is the second aldosterone antagonist available. In 2002, FDA gave the approval to use it in patients with resistant hypertension and in 2003 it got approval for treatment of patients with HF. Recent advances in RAAS blockade in HF have focused on the role of eplerenone. Eplerenone is a selective aldosterone receptor antagonist (SARA); it is similar to spironolactone, but has a lower affinity for androgen and progesterone receptors than spironolactone.[12,13] Because of its more selectivity, it has a better side effect profile than spironolactone and minimal chances of sexual side effects in both sexes. But this advantage has come over the increased cost of eplerenone over spironolactone which is 10 times more costlier than the latter. Another disadvantage is that eplerenone is primarily dependent on cytochrome P450 enzyme (CYP3A4) for its metabolism and elimination from the body and thus is prone to interactions with other substrates or inhibitors of CYP3A4 (e.g., ketoconazole, erythromycin, verapamil, fluconazole).[14]Figure 3 summarizes advantages and disadvantages of eplerenone. Potential contraindications and cautions for eplerenone use in clinical practice are mentioned in Figure 4.
Figure 3.
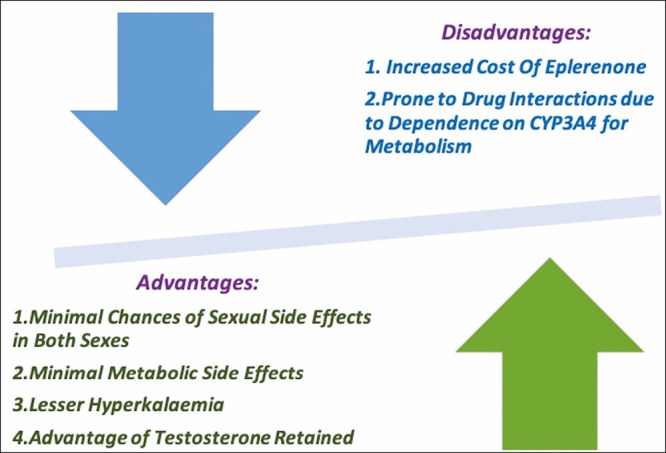
Advantages and disadvantages of eplerenone. CYP3A4 = cytochrome P450 3A4 enzyme
Figure 4.

Potential contraindications and cautions for eplerenone use in clinical practice. NSAID = nonsteroidal anti-inflammatory drugs
MAJOR STUDIES ON EPLERENONE
Studies establishing role in heart failure with reduced ejection fraction
RALES trial established the role of spironolactone as an “add-on” treatment to ACE inhibitors in HF [Table 1]. RALES trial was a double-blind randomized controlled trial (RCT) and included patients with NYHA class III or IV HF with left ventricular ejection fraction (LVEF) <35% and already taking ACE inhibitors. It was found that mortality rates dropped by 30% in patients receiving spironolactone. Not only it was found to improve NYHA functional class, but also reduces recurrent hospitalization rates by 35%.[7]
Table 1.
Key RCTs of eplerenone in the field of HF with reduced EF (HFrEF)
| Study | Duration | N | Cases | Controls | Finding |
|---|---|---|---|---|---|
| 4E-left ventricular hypertrophy study[8] | 9 months | 202 | Group 1: Eplerenone Group 2: Enalapril Group 3: Eplerenone+Enalapril | Eplerenone significantly ↓ LV mass from baseline (–14.5 ± 3.36g; n = 50) similarly to enalapril (–19.7 ± 3.20g; n = 54; P = 0.258), but eplerenone+enalapril | |
| (–27.2 ± 3.39g; n = 49) was more effective than eplerenone alone (P = 0.007) | |||||
| All groups ↓ SBP and DBP from baseline (eplerenone, –23.8 and –11.9 mm Hg; enalapril, –24.7 and –13.4 mm Hg; and eplerenone+enalapril, –28.7 and –14.4 mm Hg, P = 0.048) | |||||
| EPHESUS[15] | 16 months | Cases: 3313 Controls: 3319 | Eplerenone | Placebo | ↓ in mortality and HFH 14.4% mortality in cases and 16.7% in controls; HR, 0.85; 95% CI, 0.75 to 0.96; P = 0.008 |
| 26.7% ↓ in hospitalization in cases and 29.9% in controls; HR,0.87; 95% CI, 0.79 to 0.95; P = 0.002 | |||||
| EMPHASIS-HF[14] | 21 months | Cases: 1364 Controls: 1373 | Eplerenone | Placebo | ↓ in mortality and HFH |
| 12.5% mortality in cases and 15.5% in controls; HR, 0.76; 95% CI, 0.62 to 0.93; P = 0.008 | |||||
| 29.9% ↓ in hospitalization in cases and 35.8% in controls; HR, 0.77; 95% CI, 0.67 to 0.88; P < 0.001 |
First ever major trial to examine the role of newer MRA, eplerenone, in patients with HF was EMPHASIS-HF. Patients with NYHA class II symptoms, an EF < 35% and a recent HF-related hospitalization or elevated BNP were randomized to eplerenone or placebo. The trial was stopped early after 21 months as it shown significant benefit on the combined end point of cardiovascular death or first HF hospitalization (hazard ratio [HR] 0.63, 95% confidence interval [CI]–0.54 to 0.74, P < 0.001). Significant reductions were also shown in secondary end points of all-cause mortality (HR 0.76, 95% CI 0.62 to 0.93, P = 0.008) and cardiovascular mortality (HR 0.76, 95% CI 0.62 to 0.93, P = 0.01).[15]
EPHESUS was a large multicentre RCT which established the role of eplerenone in post-MI patients. Patients with an LVEF <40% and clinical features of HF or diabetes were randomized 3–14 days post-MI to eplerenone or placebo. Both all-cause mortality (relative risk = 0.85, 95% CI 0.75 to 0.96, P = 0.008) and the combined end point of death from any cause or cardiac hospitalization were significantly reduced (relative risk=0.87, 95% CI 0.79 to 0.95, P = 0.002).[8] The 4E-left ventricular hypertrophy (LVH) study by Pitt et al.[16] showed that eplerenone was as effective as enalapril in LVH regression and blood pressure control. The combination of eplerenone and enalapril was more effective in reducing LV mass and systolic blood pressure (SBP) than eplerenone alone.
Studies of eplerenone in heart failure with reduced ejection fraction
The role of eplerenone, as well as spironolactone, is not well defined in patients of heart failure with preserved ejection fraction (HFpEF). In 2016 and 2017, the American College of Cardiology (ACC)/ American Heart Association (AHA)/Heart Failure Society of America (HFSA) published an updated to the 2013 guidelines for the management of HF. The 2017 update added new recommendation for the use of ARAs in the management of HFpEF based on the findings from the TOPCAT study.[17] Although there are several trials supporting use of spironolactone in HFpEF, data regarding eplerenone use in HFpEF are sparse.
The randomized aldosterone antagonism in heart failure with preserved ejection fraction (RAAM-PEF) trial by Deswal et al.[18] evaluated the efficacy of eplerenone vs. placebo in 44 patients with HFpEF in the single-center, randomized, double-blind trial (21 in eplerenone group and 23 placebo group). The primary end point was changes from baseline in 6-min walk distance (6MWD) after 24 weeks of treatment, improved significantly in both groups, with no significant differences between the eplerenone and placebo groups. In particular, 6MWD changed from 249.0 ± 66.8 to 286.3 ± 66.7 with placebo and from 271.4 ± 75.7 to 310.7 ± 89.8 with eplerenone (P = 0.91 between groups). No significant differences between the two groups were seen in quality of life scores, NYHA class or SBP. There was an improvement in NYHA class in 13% of placebo patients and in 33% of eplerenone patients. In the eplerenone group, however, there was a significant decrease in the LV diastolic dysfunction (E/E′ ratio on echocardiography, P = 0.01). HF hospitalizations occurred in one patient treated with eplerenone and two patients treated with placebo. HF worsening was identified in two patients treated with eplerenone and in five patients in the placebo arm (P = 0.27).
Kampourides et al.[19] evaluated the effect of eplerenone on the outcome of 303 post-ST-segment elevation acute myocardial infarction patients (201 patients on eplerenone, 102 not on eplerenone treatment) with preserved systolic pump function (LVEF ≥ 40%)in an open-label, randomized, parallel-group, clinical study. The primary endpoint of the study, that is, death from cardiovascular causes, nonfatal reinfarction, hospitalization for unstable angina, or decompensation of HF was not significantly different between patients on eplerenone or not. Notably, eplerenone was associated with a better prognosis only in patients with initially low matrix metalloproteinase (MMP-9) levels, whereas no significant difference was detected in event-free survival rate in patients with high MMP-9 levels at baseline. Although eplerenone has proven benefit in patients of HFrEF, data related to the use of eplerenone in patients with HFpEF are sparse and further data are needed to define the potential therapeutic role of in patients with HFpEF. The data on the use of eplerenone in the treatment of HFpEF are reported in Table 2.
Table 2.
Key studies of eplerenone in the field of HF with preserved EF
| Study | Duration | N | Primary end point | Finding |
|---|---|---|---|---|
| RAAM-PEF Trial[18] | 24 weeks | 44 (21-eplerenone 23-placebo) | Changes from baseline in 6MWD | No significant difference in the change in 6-min walk test between the eplerenone and placebo arms. |
| Kampourides et al.[19] | 24 months | 303 (201-eplerenone, 102-placebo) | Death from cardiovascular causes, nonfatal reinfarction, hospitalization for unstable angina, or decompensation of HF | No significant different between patients on eplerenone or not |
Studies establishing role in hypertension
Eplerenone can be used individually or in combination with other medications to treat hypertension. A study by Tam et al.[20] showed that eplerenone 50–200 mg/day lowers blood pressure in people with primary hypertension by 9.21 mm Hg systolic and 4.18 mm Hg diastolic compared to placebo, with no difference of effect between doses of 50 and 200 mg/day. A dose of 25 mg/day did not produce a statistically significant reduction in systolic or diastolic BP and there is insufficient evidence for doses >200 mg/day. There is currently no available evidence to determine the effect of eplerenone on clinically meaningful outcomes such as mortality or morbidity in hypertensive patients. In a study by White et al.,[21] it was shown that eplerenone was as effective as amlodipine in lowering systolic BP and pulse pressure as well as pulse wave velocity in older patients with widened pulse pressure hypertension. It was seen that in patients with microalbuminuria at baseline (>30 mg albumin/g creatinine), eplerenone reduced the urinary albumin/creatinine ratio (UACR) by 52% compared with a reduction of 10% by amlodipine. A study by Weinberger et al.[22] showed that adjusted mean change of BP from baseline to final visit in seated and standing SBP and diastolic blood pressure (DBP) was significantly greater (P < .05) in all eplerenone groups than in the placebo group. Flack et al.[23] showed that eplerenone was as effective as losartan in reducing SBP and DBP in the high renin patient, but more effective than losartan in the low renin patient. Table 3 summarizes the data on eplerenone in Resistant Hypertension.
Table 3.
Major studies on eplerenone in evidence of hypertension
| Study | Duration | N | Cases | Control(s) | Finding |
|---|---|---|---|---|---|
| White et al.[21] | 24 weeks | 269 | Eplerenone | Amlodipine | Similar ↓ in SBP (eplerenone, –20.5 ± 1.1 mm Hg; amlodipine, –20.1 ± 1.1 mm Hg) |
| ↓ in DBP modestly larger on amlodipine | |||||
| (–6.9 ± 0.7 mm Hg) compared with eplerenone (–4.5 ± 0.7 mm Hg) (P = 0.014) | |||||
| Similar ↓ in pulse pressure(eplerenone, –15.9 mm Hg versus amlodipine, –13.4 mm Hg, P = 0.07) | |||||
| ↓ in urinary albumin/creatinine ratio by 52% in cases and by 10% in controls (P = 0.04) | |||||
| Tam et al.[20] | 16 weeks | 1437 | Eplerenone | Placebo | ↓ in SBP 9.21 mm Hg (95% CI –11.08 to –7.34) and DBP 4.18 mm Hg (95% CI –5.03 to –3.33) |
| Weinberger.[22] | 8 weeks | 409 | Eplerenone | Placebo | Significant ↓ in SBP and DBP (P < .05) |
| Flack et al.[23] | 16 weeks | 551 | Eplerenone | Losartan Placebo | ↓ in DBP –5.3 ± 0.7, –10.3 ± 0.7, and –6.9 ± 0.6 mm Hg in placebo, eplerenone-treated, and losartan-treated groups, respectively (mean ± SE, P < 0.001 eplerenone vs. placebo, P < 0.001 eplerenone vs. losartan). |
CLINICAL ROLE OF EPLERENONE
Heart failure
Eplerenone has established a role as RAAS modulator and has proven mortality benefit in RCTs. It is recommended as mainstay of therapy in HF patients with EF<35% along with ACE inhibitors and β-blockers [Table 4].
Table 4.
Current clinical uses of eplerenone
| Use | Evidence |
|---|---|
| Heart failure | EMPHASIS-HF trial[14] |
| 4E-left ventricular hypertrophy study[8] | |
| Myocardial infarction | EPHESUS study[15] |
| Hypertension | Weinberger et al.[22] |
| White et al.[21] | |
| Tam et al.[20] | |
| Flack et al.[23] | |
| Central serous retinopathy | Salehi et al.[24] |
| Idiopathic hyperaldosteronism | Asterios et al.[25] |
Myocardial infarction
Eplerenone is specifically indicated for the reduction of risk of cardiovascular death in patients with HF and LV dysfunction within 3–14 days of an acute myocardial infarction and EF < 40% along with ACE inhibitors and β-blockers.
Hypertension
Eplerenone can be used individually or in combination with other medications to treat hypertension. MRA are first-line add on therapy in cases of resistant hypertension.
Central serous retinopathy
Eplerenone is being explored as a treatment for central serous retinopathy (CSR). It is expected that as an antimineralocorticoid, eplerenone can inhibit over-activation of the MR pathway in the choroid. Separate trials are underway to determine if there are beneficial effects of eplerenone for acute and chronic CSR.[24]
Idiopathic hyperaldosteronism
A study by Asterios et al.[25] concluded that eplerenone was as effective as spironolactone in reducing BP in patients with Idiopathic Hyperaldosteronism. Eplerenone appeared to reduce SBP, but not DBP, faster than spironolactone. The risk of mild hyperkalemia was similar to spironolactone.
PHARMACOKINETICS
Eplerenone selectively binds to the MR, thereby competitively blocking the binding of aldosterone and thus inhibiting sodium reabsorption and other deleterious aldosterone-mediated mechanisms. The chemical structure is similar to aldosterone with two exceptions-17α thioacetyl group with a carboxymethyl group and addition of 9α-11α epoxy bridge.[26] The complete chemical structure can be depicted as 9,11-epoxy-7-(methoxycarbonyl)-3-oxo-17-pregn-4-ene-21,17-carbolactone.[27] The replacement of 17α thioacetyl group renders the molecule more selective for MR in contrast to androgen receptors. Despite the lower affinity (up to 20 times less) for aldosterone receptor vis-à-vis spironolactone, the potency is retained up to 75%. There are no active metabolites unlike its previous congener. Eplerenone is metabolized via the cytochrome P450 (CYP) 3A4 pathway. It has extensive metabolism, but its metabolites are inactive and its elimination half-life is short (4–6 h). Steady state is achieved within 2 days. Blood levels are potentiated and increased with concomitant use of CYP3 A4 inhibitors (e.g., ketoconazole, verapamil, erythromycin). The pharmacokinetics of eplerenone is similar between men and women. Steady-state area under the curve and maximum concentration are increased with renal and hepatic insufficiency. Hemodialysis does not remove eplerenone. Table 5 compares properties of eplerenone with that of spriononlactone.
Table 5.
Comparison of spironolactone and eplerenone
| Characteristics | Spironolactone | Eplerenone |
|---|---|---|
| Approval | 1950s | 2000s |
| Receptor selectivity | Less selective | More selective. Lower affinity for progesterone, androgen and glucocorticoid receptors |
| Metabolism | Extensive metabolism to three active metabolites with prolonged half-lives (13.8–16.5 h) | Extensive metabolism, but its metabolites are inactive and its elimination half-life is short (4–6 h) |
| Side effects specific to men | Gynecomastia | Less common |
| Impotence | ||
| Loss of libido | ||
| Side effects specific to women | Mensural irregularity | Less common |
| Vaginal bleeding | ||
| Loss of libido | ||
| Cost-effectiveness | Economical | Expensive |
| Hyperkalemia | Higher risk due to long half-life of metabolites | Lower risk. Higher if patient taking CYP3A4 inhibitors |
| Use in HT | Usually in combination with other drugs, for patients who cannot be treated adequately with other agents | May be used alone or in combination with other antihypertensive agents |
| Effect on testosterone and its implication | Testosterone appears to have a protective effect against cardiomyocyte apoptosis which is antagonized by spironolactone | No significant effect on testosterone levels |
ADVERSE EFFECTS
Receptor selectivity of eplerenone has imparted it a better side effect profile than spironolactone and minimal chances of sexual side effects in both sexes. Mastodynia reported in 0.8% and gynecomastia in 0.5% of men and abnormal vaginal bleeding in 0.6% of women. Eplerenone is primarily dependent on CYP3A4 for its metabolism and elimination from the body and thus is prone to interactions with other substrates or inhibitors of CYP3A4 (e.g., ketoconazole, erythromycin, verapamil, and fluconazole).[14,28] Hyperkalemia (serum potassium > 5 mEq/L) is reported in 33% of patients taking eplerenone. Caution should be used while prescribing it with other potassium raising drugs, most commonly being ACE inhibitor/ARB. Hypertriglyceridemia occurs at a rate of 15%. Hyponatremia can occur by 2.3%.
HYPERKALEMIA AND MINERALOCORTICOID RECEPTOR ANTAGONIST
Hyperkalemia (serum potassium >5 mEq/L) is an important side effect of MRA. MRA-induced hyperkalemia often limits their use, thereby offsetting their survival benefits. The risk is further magnified when potassium-sparing drugs are used in combination or patient is suffering from diseases, such as chronic kidney disease (CKD) or HF. In hypertensive patients without risk factors for hyperkalemia, the incidence of hyperkalemia with RAASi monotherapy is ≤2% and increases to ~5% with dual RAAS inhibition and to 5%–10% when dual therapy is administered in patients with HF or CKD.[29] In patients with chronic HFrEF, NYHA functional class II, and meeting specific inclusion and exclusion criteria, including an eGFR > 30 mL/min/1.73 m2 and K level <5.0 mmol/L, eplerenone was both efficacious and safe when carefully monitored, even in subgroups at high risk of developing hyperkalemia or worsening renal function.[30] Furthermore, in the RALES trial, the benefit of spironolactone was maintained in the setting of moderate hyperkalemia, and clinical outcomes with spironolactone were superior to placebo when K+ levels remained <6.0 mEq/L.[7] Patients with cardiovascular disease and CKD are at risk of hyperkalemia and ~50% of these patients have two or more recurrences within 1 year.[31] Incidence rates of hyperkalemia are higher in HFrEF patients on MRA in the real-world setting than in clinical trials (6%–12%), that is, when they are administered to higher-risk and unselected populations which did not receive K level and/or creatinine monitoring.[32] In the real-world setting, the incidence of hyperkalemia can be as high as 50% in unselected population of patients receiving RAASi.[33] Despite this evidence and guideline recommendations, K levels are frequently under-monitored in patients treated with RAASi. Therefore, quality improvement programs are needed to improve rates of laboratory monitoring for patients initiated on MRA therapy, particularly in high-risk patients. In situation of persistent higher potassium despite reducing dosage of MRA, various measures to combat hyperkalemia should be undertaken to continue obtaining benefit of MRA. However, when potassium fails to fall <5 mEq/L, it is prudent to withhold MRA and other offending drugs until hyperkalemia is resolved. Options for the management of hyperkalemia include discontinuation or reducing doses of culprit drugs, administration of loop diuretics, dietary potassium restriction, and corrective measures such as potassium binders (e.g., sodium polystyrene sulfonate). Various international guidelines like National Institute of Clinical Excellence (NICE, UK), European Society of Cardiology Heart Failure (ESC-HF) and National Disease Improvement in Global Outcomes (KDIGO)advice against starting RAASi if K>5.0 mEq/L.[3,34,35]Table 6 highlights the key points to be kept in mind while using MRA in hyperkalemia. Figure 5 outlines the management of hyperkalemia.
Table 6.
Hyperkalemia and MRA
| Hyperkalemia and MRA | |
|---|---|
| Patient population at risk | CKD (eGFR ≤45 mL/min per 1.73 m2) |
| HF | |
| Drug interactions such as NSAIDs, other nephrotoxic drugs | |
| Combination with other K sparing drug | |
| Initial serum potassium >4.5 mEq/L | |
| BMI <25g/m2 | |
| Incidence of hyperkalemia | RAASi monotherapy: ≤2% |
| Dual RAAS inhibition: ~5% | |
| Dual therapy in patients with HF or CKD: 5%–10% | |
| Target K level | <5 mEq/L |
| eGFR ≥50 mL/min/1.73 m2 with K+ in normal range | Usual dose |
| eGFR 30–49 mL/min/1.73 m2 with K+ in normal range | MRA every other day |
| Recommendations against starting MRA | When K>5 mEq/L (NICE, K/DOQI, ESC HF) |
Figure 5.

Outline of management of hyperkalemia in patients on MRA. MRA = mineralocorticoid receptor antagonist
FUTURE DIRECTIONS
The newer novel nonsteroidal MRA finerenone has been used to treat HFrEF. A systematic review and meta-analysis of three trials with 1520 congestive HF patients using the drug were included.[36] It was found that finerenone was equivalent to the existing steroidal mineralocorticoid antagonist (P < .05). However, the efficacy of finerenone appeared to be dose-dependent. At a dose of 10 mg/d, finerenone was found to be marginally better than that of steroidal MRAs (RR = 1.18, 95% CI 0.88, 1.57, P > .05). The incidence of treatment-related adverse events of finerenone at 10 mg/d was significantly lower than 25–50 mg/d of steroidal MRAs (RR = 0.81, 95% CI = 0.66–0.99, P = .04). Moreover, the serum potassium levels in the finerenone 10 mg/d group were lower than those in the 25–50 mg/d steroidal MRAs group (MD = –0.14, 95% CI –0.30–0.02, P = .09), whereas the estimated glomerular filtration rate (eGFR) was higher in finerenone versus steroidal MRA-treated patients (MD = 2.07, 95% CI –0.04–4.17, P = .05). Finerenone reduced NT-proBNP level, UACR, and other biochemical indicators, in a dose-dependent manner. In terms of antiventricular remodeling in patient with chronic HF, finerenone at 10 mg/day is as effective as 20–50 mg/day of steroidal MRAs. Also, finerenone has been found to be much safer for patients with CKD. The results of a trial comparing eplerenone and spironolactone in HF patients with diabetes are awaited (SNOW; NCT01586442).[37]
CONCLUSIONS
Eplerenone has emerged to be a newer and seemingly better alternative to spironolactone. Both eplerenone and spironolactone are efficacious and safe in the treatment of hypertension and HF, although eplerenone’s selectivity yields a superior tolerability profile in terms of sexual side effects. There is a general lack of direct comparative data for spironolactone and eplerenone and there are no head-to-head trials comparing efficacy; an evidence-based approach to their use seems reasonable. While using MRA, routine serum potassium evaluation is mandatory due to the common side effect of hyperkalemia. The newer MRA finerenone is currently in phase III clinical trials and more evidence and conclusive results are expected regarding its efficacy and safety in comparison to established MRAs-spironolactone or eplerenone.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Brown NJ. Contribution of aldosterone to cardiovascular and renal inflammation and fibrosis. Nat Rev Nephrol. 2013;9:459–69. doi: 10.1038/nrneph.2013.110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Richards AM, Nicholls MG. Aldosterone antagonism in heart failure. Lancet. 1999;354:789–90. doi: 10.1016/S0140-6736(99)80003-8. [DOI] [PubMed] [Google Scholar]
- 3.Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JG, Coats AJ, et al. Authors/Task Force Members; Document Reviewers. 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the heart failure association (HFA) of the ESC. Eur J Heart Fail. 2016;18:891–975. doi: 10.1002/ejhf.592. [DOI] [PubMed] [Google Scholar]
- 4.Chaggar PS, Malkin CJ, Shaw SM, Williams SG, Channer KS. Neuroendocrine effects on the heart and targets for therapeutic manipulation in heart failure. Cardiovasc Ther. 2009;27:187–93. doi: 10.1111/j.1755-5922.2009.00094.x. [DOI] [PubMed] [Google Scholar]
- 5.McMurray JJ, Packer M, Desai AS, Gong J, Lefkowitz MP, Rizkala AR, et al. PARADIGM-HF Investigators and Committees. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N Engl J Med. 2014;371:993–1004. doi: 10.1056/NEJMoa1409077. [DOI] [PubMed] [Google Scholar]
- 6.Jaisser F, Farman N. Emerging roles of the mineralocorticoid receptor in pathology: toward new paradigms in clinical pharmacology. Pharmacol Rev. 2016;68:49–75. doi: 10.1124/pr.115.011106. [DOI] [PubMed] [Google Scholar]
- 7.Pitt B, Zannad F, Remme WJ, Cody R, Castaigne A, Perez A, et al. The effect of spironolactone on morbidity and mortality in patients with severe heart failure. Randomized Aldactone Evaluation Study investigators. N Engl J Med. 1999;341:709–17. doi: 10.1056/NEJM199909023411001. [DOI] [PubMed] [Google Scholar]
- 8.Pitt B, Remme W, Zannad F, Neaton J, Martinez F, Roniker B, et al. Eplerenone Post-Acute Myocardial Infarction Heart Failure Efficacy and Survival Study Investigators. Eplerenone, a selective aldosterone blocker, in patients with left ventricular dysfunction after myocardial infarction. N Engl J Med. 2003;348:1309–21. doi: 10.1056/NEJMoa030207. [DOI] [PubMed] [Google Scholar]
- 9.Kashyap A, Dezellem S, Vardeny O. A retrospective evaluation of spironolactone versus eplerenone on potassium homeostasis and renal function. J Card Fail. 2013;19:S28. [Google Scholar]
- 10.Sánchez-Más J, Turpín MC, Lax A, Ruipérez JA, Valdés Chávarri M, Pascual-Figal DA. Differential actions of eplerenone and spironolactone on the protective effect of testosterone against cardiomyocyte apoptosis in vitro. Rev Esp Cardiol. 2010;63:779–87. doi: 10.1016/s1885-5857(10)70162-6. [DOI] [PubMed] [Google Scholar]
- 11.Yamaji M, Tsutamoto T, Kawahara C, Nishiyama K, Yamamoto T, Fujii M, et al. Effect of eplerenone versus spironolactone on cortisol and hemoglobin A1© levels in patients with chronic heart failure. Am Heart J. 2010;160:915–21. doi: 10.1016/j.ahj.2010.04.024. [DOI] [PubMed] [Google Scholar]
- 12.Delyani JA, Rocha R, Cook CS, Tobert DS, Levin S, Roniker B, et al. Eplerenone: a selective aldosterone receptor antagonist (SARA) Cardiovasc Drug Rev. 2001;19:185–200. doi: 10.1111/j.1527-3466.2001.tb00064.x. [DOI] [PubMed] [Google Scholar]
- 13.de Gasparo M, Joss U, Ramjoué HP, Whitebread SE, Haenni H, Schenkel L, et al. Three new epoxy-spirolactone derivatives: characterization in vivo and in vitro. J Pharmacol Exp Ther. 1987;240:650–6. [PubMed] [Google Scholar]
- 14.Busti AJ. [Last accessed on 2019 Aug 8]. Why does eplerenone (Inspra) cause more drug interactions than spironolactone (Aldactone)? Evidence based medicine––consult. [Internet] (updated August 2015). Available from: https://www. ebmconsult.com/articles/ eplerenone- inspra-drug-interactions-spironolactone-aldactone-diuretic .
- 15.Zannad F, McMurray JJ, Krum H, van Veldhuisen DJ, Swedberg K, Shi H, et al. EMPHASIS-HF Study Group. Eplerenone in patients with systolic heart failure and mild symptoms. N Engl J Med. 2011;364:11–21. doi: 10.1056/NEJMoa1009492. [DOI] [PubMed] [Google Scholar]
- 16.Pitt B, Reichek N, Willenbrock R, Zannad F, Phillips RA, Roniker B, et al. Effects of eplerenone, enalapril, and eplerenone/enalapril in patients with essential hypertension and left ventricular hypertrophy: the 4E-left ventricular hypertrophy study. Circulation. 2003;108:1831–8. doi: 10.1161/01.CIR.0000091405.00772.6E. [DOI] [PubMed] [Google Scholar]
- 17.Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE, Jr, Colvin MM, et al. 2017 ACC/AHA/HFSA focused update of the 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines and the Heart Failure Society of America. Circulation. 2017;136:e137–61. doi: 10.1161/CIR.0000000000000509. [DOI] [PubMed] [Google Scholar]
- 18.Deswal A, Richardson P, Bozkurt B, Mann DL. Results of the randomized aldosterone antagonism in heart failure with preserved ejection fraction trial (RAAM-PEF) J Card Fail. 2011;17:634–42. doi: 10.1016/j.cardfail.2011.04.007. [DOI] [PubMed] [Google Scholar]
- 19.Kampourides N, Tziakas D, Chalikias G, Papazoglou D, Maltezos E, Symeonides D, et al. Usefulness of matrix metalloproteinase-9 plasma levels to identify patients with preserved left ventricular systolic function after acute myocardial infarction who could benefit from eplerenone. Am J Cardiol. 2012;110:1085–91. doi: 10.1016/j.amjcard.2012.05.049. [DOI] [PubMed] [Google Scholar]
- 20.Tam TS, Wu MH, Masson SC, Tsang MP, Stabler SN, Kinkade A, et al. Eplerenone for hypertension. Cochrane Database Syst Rev. 2017;2:CD008996. doi: 10.1002/14651858.CD008996.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.White WB, Duprez D, St Hillaire R, Krause S, Roniker B, Kuse-Hamilton J, et al. Effects of the selective aldosterone blocker eplerenone versus the calcium antagonist amlodipine in systolic hypertension. Hypertension. 2003;41:1021–6. doi: 10.1161/01.HYP.0000067463.13172.EA. [DOI] [PubMed] [Google Scholar]
- 22.Weinberger MH, Roniker B, Krause SL, Weiss RJ. Eplerenone, a selective aldosterone blocker, in mild-to-moderate hypertension. Am J Hypertens. 2002;15:709–16. doi: 10.1016/s0895-7061(02)02957-6. [DOI] [PubMed] [Google Scholar]
- 23.Flack JM, Oparil S, Pratt JH, Roniker B, Garthwaite S, Kleiman JH, et al. Efficacy and tolerability of eplerenone and losartan in hypertensive black and white patients. J Am Coll Cardiol. 2003;41:1148–55. doi: 10.1016/s0735-1097(03)00054-8. [DOI] [PubMed] [Google Scholar]
- 24.Salehi M, Wenick AS, Law HA, Evans JR, Gehlbach P. Interventions for central serous chorioretinopathy: a network metaanalysis. Cochrane Database Syst Rev. 2015;12:CD011841. doi: 10.1002/14651858.CD011841.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Karagiannis A, Tziomalos K, Papageorgiou A, Kakafika AI, Pagourelias ED, Anagnostis P, et al. Spironolactone versus eplerenone for the treatment of idiopathic hyperaldosteronism. Expert Opin Pharmacother. 2008;9:509–15. doi: 10.1517/14656566.9.4.509. [DOI] [PubMed] [Google Scholar]
- 26.Brown NJ. Eplerenone: cardiovascular protection. Circulation. 2003;107:2512–8. doi: 10.1161/01.CIR.0000071081.35693.9A. [DOI] [PubMed] [Google Scholar]
- 27.National Center for Biotechnology Information. [Last accessed on 2020 Jun 3]. PubChem database. Eplerenone, CID=443872. Available from: https://pubchem.ncbi.nlm.nih.gov /compound/Eplerenone .
- 28.Inspra. [Product Information] Chicago, IL: GD Searle; 2003. [Google Scholar]
- 29.Weir MR, Rolfe M. Potassium homeostasis and renin-angiotensin-aldosterone system inhibitors. Clin J Am Soc Nephrol. 2010;5:531–48. doi: 10.2215/CJN.07821109. [DOI] [PubMed] [Google Scholar]
- 30.Eschalier R, McMurray JJ, Swedberg K, van Veldhuisen DJ, Krum H, Pocock SJ, et al. EMPHASIS-HF Investigators. Safety and efficacy of eplerenone in patients at high risk for hyperkalemia and/or worsening renal function: analyses of the EMPHASIS-HF study subgroups (eplerenone in mild patients hospitalization and survival study in heart failure) J Am Coll Cardiol. 2013;62:1585–93. doi: 10.1016/j.jacc.2013.04.086. [DOI] [PubMed] [Google Scholar]
- 31.Ramadan FH, Masoodi N, El-Solh AA. Clinical factors associated with hyperkalemia in patients with congestive heart failure. J Clin Pharm Ther. 2005;30:233–9. doi: 10.1111/j.1365-2710.2005.00638.x. [DOI] [PubMed] [Google Scholar]
- 32.Shah KB, Rao K, Sawyer R, Gottlieb SS. The adequacy of laboratory monitoring in patients treated with spironolactone for congestive heart failure. J Am Coll Cardiol. 2005;46:845–9. doi: 10.1016/j.jacc.2005.06.010. [DOI] [PubMed] [Google Scholar]
- 33.Cooper LB, Hammill BG, Peterson ED, Pitt B, Maciejewski ML, Curtis LH, et al. Consistency of laboratory monitoring during initiation of mineralocorticoid receptor antagonist therapy in patients with heart failure. JAMA. 2015;314:1973–5. doi: 10.1001/jama.2015.11904. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.National Institute for Health and Care Excellence (NICE) [Last Accessed on 2019 Aug 5]. Chronic kidney disease: early identification and management of chronic kidney disease in adults in primary and secondary care [CG182]. Available from: http://www.nice.org.uk/guidance/cg182 . [PubMed]
- 35.Levin A, Stevens PE, Bilous RW, Coresh J, De Francisco ALM, De Jong PE, et al. Kidney disease: improving global outcomes (KDIGO) CKD work group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl. 2013;3:1–150. [Google Scholar]
- 36.Pei H, Wang W, Zhao D, Wang L, Su GH, Zhao Z. The use of a novel non-steroidal mineralocorticoid receptor antagonist finerenone for the treatment of chronic heart failure: a systematic review and meta-analysis. Medicine (Baltimore) 2018;97:e0254. doi: 10.1097/MD.0000000000010254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Korol S, White M, O’Meara E, Tournoux F, Racine N, Ducharme A, et al. A comparison of the effects of selective and non-selective mineralocorticoid antagonism on glucose homeostasis of heart failure patients with glucose intolerance or type II diabetes: a randomized controlled double-blind trial. Am Heart J. 2018;204:190–5. doi: 10.1016/j.ahj.2018.07.002. [DOI] [PubMed] [Google Scholar]