

Highlights
-
•
Evidence that calcium suppl. may reduce blood pressure is inconsistent in the general population.
-
•
We found a greater reduction in blood pressure in the calcium group for systolic pressure and MAP.
-
•
We found no interaction between previous pre-eclampsia severity and calcium supplementation.
Keywords: Hypertension, Calcium, Blood pressure, Supplementation, Preeclampsia
Abstract
Background
Low dietary calcium is associated with the hypertensive disorders of pregnancy, and evidence suggests that the risks associated with pre-eclampsia are reduced by calcium supplementation. In the general (non-pregnant) population, low dietary calcium intake is associated with hypertension with inconsistent evidence that calcium supplementation may reduce blood pressure. Women with pre-eclampsia are also at risk of hypertension later in life. An exploratory sub-study among early participants enrolled in the WHO long-term calcium supplementation in women at high risk of pre-eclampsia (CAP) study reported a trend to more blood pressure reduction with calcium in non-pregnant women with previous severe as opposed to non-severe pre-eclampsia. The current study reports the effects of low-dose calcium supplementation in non-pregnant women in the complete trial cohort.
Methods
The CAP Study was a multi-country randomized, double-blind placebo-controlled clinical trial to test the hypothesis that calcium deficiency may play a role in the genesis of pre-eclampsia in early pregnancy. From 2011 to 2016, non-pregnant women who had pre-eclampsia or eclampsia in their most recent pregnancy were randomized to receive either 500 mg/day elemental calcium or placebo. In this sub-study we compared the change in blood pressure from baseline to the 12-week visit between participants receiving calcium versus placebo for those not pregnant at the 12-week visit.
Results
Of 1355 women randomized, 810 attended a 12-week visit without being pregnant, of whom 791 had blood pressure measurements available for both baseline and 12-week visits. There was a greater reduction in blood pressure in the calcium group compared with the placebo group for systolic pressure (difference 3.1 mmHg, 95% CI 0.8 to 5.4) and mean arterial pressure (MAP) (difference 2.0 mmHg, 95% CI 0.1 to 3.8). The difference in diastolic blood pressure reduction (1.4 mmHg, 95% CI −0.5 to 3.3) was not statistically significant (p = 0.140).
For women with previous pre-eclampsia with severe features (n = 447), there was significantly greater reduction in blood pressure in the calcium than the placebo group (difference for systolic 4.0, 95% CI 0.7 to 7.3; diastolic 3.0, 95% CI 0.5 to 5.5 and mean arterial pressure 3.3, 95% CI 0.8 to 5.9 mmHg). For women with previous pre-eclampsia without severe features (n = 344), there were no significant differences between calcium and placebo groups. ANOVA analysis found no statistically significant interaction between previous pre-eclampsia severity and treatment, for systolic (p = 0.372), diastolic (p = 0.063) or mean blood pressure (p = 0.103).
Conclusions
Low-dose calcium supplementation significantly reduced systolic and mean arterial pressure in non-pregnant women with previous pre-eclampsia. We did not confirm a greater calcium effect in women with previous pre-eclampsia with severe versus non-severe features.
The effect of low-dose calcium is of importance since even modest blood pressure reductions at a population level may have important benefits in terms of reduced major complications of hypertension. This study adds to the mounting evidence of health benefits which could be achieved for populations with low dietary calcium through strategies to increase calcium intake, particularly among women at high risk due to previous pre-eclampsia.
Clinical Trial Registration
The trial was registered with the Pan-African Clinical Trials Registry, registration number PACTR201105000267371 (https://pactr.samrc.ac.za/TrialDisplay.aspx?TrialID=267).
1. Background
Pre-eclampsia is associated with low dietary calcium intake, and calcium supplementation in the second half of pregnancy has been associated with reductions in the prevalence of pre-eclampsia and its severe consequences in populations with low dietary calcium intake [1].
Low dietary calcium intake is also associated with hypertension in the non-pregnant population [2], [3]. Calcium supplementation has been associated with small reductions in blood pressure in some studies of non-hypertensive people [4], [5], [6], [7], while the effect in hypertension is unclear [8]. A 2020 meta-analysis of the effect of calcium and vitamin D co-supplementation found no difference in systolic blood pressure and a small reduction in diastolic blood pressure (0.29 mmHg) [9]. Hypertension is exceptionally common among low-income Southern African populations and is the primary risk factor of the global burden of disease [9], [10].
As both early and late onset of pre-eclampsia are associated with long-term metabolic dysfunction and cardiovascular risk including hypertension, it is important to assess the effect of calcium supplementation in women from low dietary calcium populations with previous pre-eclampsia [11].
To investigate whether calcium intake before and in early pregnancy affects the subsequent evolution of pre-eclampsia, we conducted the WHO long term calcium supplementation in women at high risk of pre-eclampsia (Calcium and Pre-eclampsia, CAP) trial [12], [13]. We randomly allocated non-pregnant women with previous pre-eclampsia or eclampsia to calcium supplementation with 500 mg of elemental calcium daily versus placebo before pregnancy and until 20 weeks of pregnancy. All participants received 1500 mg calcium supplementation after 20 weeks according to WHO recommendations. The 20% overall reduction in pre-eclampsia in the calcium group was not statistically significant. However, for participants with 80% compliance during the first half of pregnancy (n = 393), pre-eclampsia was reduced by 34% (30/144 (21%) versus 47/149 (32%), RR 0.66 (95% CI 0.44 to 0.98), p = 0.037).
The CAP trial recruited women from July 2011 to September 2016. Using data available to 9 September 2014, we previously conducted an exploratory study of the effect of low-dose calcium supplementation on blood pressure in non-pregnant women with previous pre-eclampsia [14]. We found a trend to greater reduction in blood pressure from baseline to 12 weeks in the calcium group (n = 181) compared to the placebo group (n = 186) (systolic blood pressure mean difference 1.4, 95% confidence interval (CI) −1.6 to 4.4; diastolic blood pressure mean difference 1.0, 95% CI −1.3 to 3.4), which was statistically significant only for diastolic blood pressure in participants with previous pre-eclampsia with severe features (mean difference 3.4, 0.4 to 6.4; p = 0.025) [14]. The objective of the present study is to assess the effect of low-dose calcium supplementation on blood pressure in non-pregnant women with previous pre-eclampsia in areas of low calcium intake using the data of all women enrolled.
2. Methods
The CAP trial was a randomized, parallel arm, double-blind placebo-controlled clinical trial. Between July 2011 and September 2016, non-pregnant women who had experienced pre-eclampsia or eclampsia in their most recent pregnancy were randomly allocated to receive either 500 mg/day elemental calcium or placebo. The methodology of the trial has been described elsewhere [12]. A brief description is presented below.
2.1. Settings
This was a multi-centre trial in South Africa, Zimbabwe and Argentina. The sites in Africa were government secondary or tertiary urban referral hospitals with large obstetric units serving urban and rural populations. The South African hospitals were located in Cape Town, East London and Johannesburg. In Zimbabwe, the two maternity units included were in Harare. In Argentina, the sites included of one maternity hospital in Tucuman and two in Buenos Aires. These are all areas with low calcium intake [15], [16], [17], [18]. A nutritional interview conducted among 312 women enrolled in the trial at 20 weeks gestation confirmed that the included population had a low calcium intake (441.0 ± 97.7 (mean, standard deviation) mg of calcium a day in South Africa and 360.5 ± 171.4 mg of calcium a day in Zimbabwe) [17]. The nutritional assessment in the Argentinean sites did not allow for country-level estimates. However, evidence outside the CAP trial confirmed the low levels of calcium intakes in Argentina [15], [19].
2.2. Participants
Women were eligible if they had experienced pre-eclampsia or eclampsia in their most recent pregnancy, they were in a sexual relationship, not pregnant, not using reliable contraception and they gave informed consent. Exclusion criteria were: less than 18 years of age; chronic hypertension with persistent proteinuria; calcium supplement intake; and history or symptoms of urolithiasis, renal disease or parathyroid disease.
2.3. The intervention
Women in the intervention group received one chewable tablet containing 500 mg elemental calcium daily from enrolment (before pregnancy) until 20 weeks’ gestation. The women were asked to chew the tablet during the day, not close in time to taking food or iron supplements. Women in the control group received placebo tablets identical in shape, colour and taste to the intervention tablet. The women were encouraged not to take any additional calcium supplements. All women received unblinded calcium supplementation (1500 mg) from 20 weeks’ gestation until delivery, according to WHO recommendations [20]. Treatment compliance was calculated by dividing the number of used tablets by the total number of tablets that should have been taken [12].
2.4. Blood pressure measurement
Blood pressure measurement was standardized at the beginning of the trial according to recommendations by the British Hypertension Society (http://www.bhsoc.org/latest-guidelines/how-to-measure-blood-pressure/). Researchers measuring blood pressure were trained and certified according to the trial procedures and using tools from the British Hypertension Society. Blood pressure was measured with a standard mercury sphygmomanometer at the sites in Africa and with an automated sphygmomanometer at the sites in Argentina.
Blood pressure was measured at recruitment (baseline) and at all subsequent trial visits. The visits were scheduled every 12 weeks until the woman became pregnant, then at 8, 20, and 32 weeks of pregnancy. The first trial visit occurring between 6 and 18 weeks after enrolment was considered the 12-week visit.
2.4.1. Dietary assessment methods
Dietary intake was assessed in those participants who reached 20-weeks’ gestation during March 2013 to March 2016. The assessment was performed using a triple pass 24-h dietary recall adapted and piloted in South Africa, Zimbabwe and Argentina [17]. The 24-h recall is a guided interview to assess food intake of the previous day. A detailed description of the methodology for dietary assessment has been published elsewhere [17].
2.5. Sub-study population and methods
For the current prespecified sub-study, routine data collected during the trial visits were analysed. Women enrolled in the trial with blood pressure data available for baseline and at least one subsequent follow-up trial visit while still not pregnant were included.
Baseline data were compared between the calcium and placebo groups for the study population to ensure no selective loss to follow-up. We used an intention-to-treat (ITT) approach for the analysis.
For each woman, the changes in blood pressures were calculated by subtracting the measurement at baseline from the measurement at the first (ideally at 12 weeks) follow-up visit. The mean changes in systolic, diastolic and mean arterial pressures were compared between the calcium and placebo groups. The differences were expressed as mean differences with 95% confidence intervals. Mean arterial pressure is defined as the average arterial pressure throughout one cardiac cycle. It was calculated by doubling the diastolic blood pressure, adding the systolic blood pressure and dividing that composite sum by three.
Subgroup analyses were performed to compare the effect of calcium supplementation on blood pressure change at the 12-week visit between women with a history of pre-eclampsia with severe features and without severe features. Severe features were defined as: i) eclampsia, or ii) haemolysis, elevated liver enzymes and low platelets (HELLP) syndrome or iii) systolic blood pressure higher than 160 mmHg or iv) diastolic blood pressure higher than 110 mmHg or v) onset of pre-eclampsia earlier than 28 weeks, or vi) ICU admission. An ANOVA analysis was conducted controlling for treatment received (placebo vs. calcium) and history of pre-eclampsia with vs. without severe features. SPSS version 20 was used for all analyses.
3. Results
Fig. 1 shows the trial profile of the sub-study. Among 1355 women randomized, 810 attended a 12-week visit without being pregnant, of whom 791 had blood pressure measurements available for both baseline and 12-week visits.
Fig. 1.
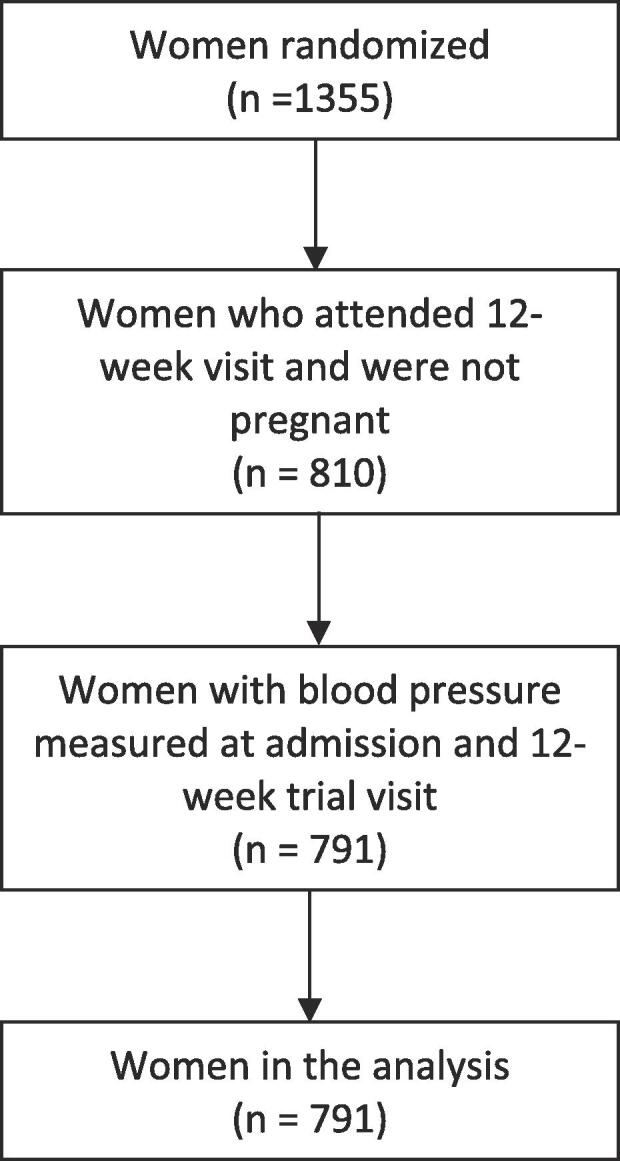
Flowchart of sub-study participants.
Baseline data comparing the calcium and placebo groups for all women enrolled and for women included in this sub-study are shown in Table 1. There were no significant differences between groups.
Table 1.
Baseline characteristics of participants at trial entry and of those in the final sample for this sub-study (baseline and 12-week pre-pregnancy blood pressures available) according to study group.
| Outcome | All participants at trial entry (n = 1355) |
Participants included in this sub-study (n = 791) |
||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Calcium (n = 678) |
Placebo (n = 677) |
p value | Calcium (n = 387) |
Placebo (n = 404) |
p value | |||||||||
| N | n/mean | %/SD | N | n/mean | %/SD | N | n/mean | %/SD | N | n/mean | %/SD | |||
| Maternal age (y) | 678 | 30.2 | 5.8 | 677 | 30.4 | 5.9 | 0.518 | 387 | 30.5 | 5,7 | 404 | 30.9 | 5,7 | 0,315 |
| Maternal weight (kg) | 649 | 76.2 | 18.5 | 641 | 76.9 | 18.8 | 0.497 | 380 | 76.6 | 19.1 | 394 | 78.1 | 18.7 | 0.284 |
| Maternal height (cm) | 617 | 160.2 | 6.3 | 613 | 160.0 | 6,7 | 0.489 | 367 | 160.7 | 6.3 | 380 | 160.2 | 6.4 | 0.275 |
| Systolic BP at randomisation (mm Hg) | 675 | 127.0 | 19.3 | 674 | 127.3 | 19,2 | 0.749 | 387 | 128.6 | 18.3 | 404 | 127.6 | 19.1 | 0.477 |
| Diastolic BP at randomisation (mm Hg) | 675 | 81.6 | 14.1 | 674 | 82.3 | 13,9 | 0.340 | 387 | 82.8 | 13.9 | 404 | 82.7 | 14,0 | 0.954 |
| Any health complaint at randomization | 678 | 20 | (2.9) | 677 | 23 | (3·4) | 0.638 | 12 | 3.1% | 404 | 15 | 3.7% | 0.781 | 12 |
| Previous severe pre-eclampsia* | 403 | 309 | (76.7) | 414 | 343 | (82.9) | 0.028 | 217 | 56.1% | 404 | 230 | 56.9% | 0,864 | 217 |
| Previous eclampsia | 643 | 107 | (16.6) | 639 | 103 | (16.1) | 0.801 | 372 | 55 | 14.8% | 388 | 65 | 16.8% | 0.519 |
| Previous HELLP syndrome | 561 | 69 | (12.3) | 561 | 78 | (13.9) | 0.426 | 324 | 44 | 13.6% | 331 | 53 | 16.0% | 0.444 |
| Previous live birth | 678 | 349 | (51.5) | 677 | 337 | (49.8) | 0.532 | 387 | 195 | 50.4% | 404 | 189 | 46.8% | 0.346 |
BP: blood pressure; HELLP: haemolysis, elevated liver enzymes, low platelet count; SD: standard deviation.
*Defined as a systolic BP ≥ 160 mmHg or a diastolic BP ≥ 110 mmHg; * t-test for independent means, or chi-square test with continuity correction.
Table 2 shows the changes from baseline in blood pressure at the 12-week visit comparing calcium and placebo groups. There was a greater reduction in blood pressure in the calcium group compared with the placebo group for systolic (difference 3.1 mmHg, 95% CI 0.8 to 5.4) and mean arterial pressure (MAP) (difference 2.0 mmHg, 95% CI 0.1 to 3.8). The reduction in the diastolic blood pressure was 1.4 mmHg (95% CI to −0.5 to 3.3) greater in the calcium group, which was not statistically significant.
Table 2.
Blood pressure change according to study group. Change in blood pressure (mmHg) at the 12-week visit compared with baseline, expressed as mean values with standard deviation (SD) and 95% confidence intervals (CI). Differences between calcium and placebo groups expressed as mean differences with 95% CI), for all women and for women with and without severe features of pre-eclampsia in the previous pregnancy.
| Calcium |
Placebo |
Difference (Placebo - Calcium) |
p (*) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| N | Mean (SD) | 95% CI | N | Mean (SD) | 95% CI | 95% CI | |||
| All | |||||||||
| Systolic | 387 | −5.3 (15.0) | −6.8, −3.8 | 404 | −2.2 (17.8) | −3.9, −0.5 | 3.1 | 0.8, 5.4 | 0.009 |
| Diastolic | 387 | −2.6 (13.0) | −6.8, −3.8 | 404 | −2.2 (17.8) | −3.9, −0.5 | 1.4 | −0.5, 3.3 | 0.140 |
| MAP** | 387 | −3.5 (12.4) | −4.7, −2.2 | 404 | −1.5 (14.1) | −2.9, −0.1 | 2.0 | 0.1, 3.8 | 0.038 |
| With Severe pre-eclampsia | |||||||||
| Systolic | 217 | −6.2 (15.2) | −8.2, −4.1 | 230 | −2.2 (20.1) | −4.8, 0.4 | 4.0 | 0.7, 7.3 | 0.018 |
| Diastolic | 217 | −3.7 (12.2) | −5.3, −2.0 | 230 | −0.6 (14.8) | −2.6, 1.3 | 3.0 | 0.5, 5.5 | 0.019 |
| MAP** | 217 | −4.5 (12.0) | −6.1, −2.9 | 230 | −1.2 (15.4) | −3.2, 0.8 | 3.3 | 0.8, 5.9 | 0.011 |
| Without Severe pre-eclampsia | |||||||||
| Systolic | 170 | −4.1 (14.8) | −6.4, −1.9 | 174 | −2.3(14.2) | −4.4, −0.1 | 1.9 | −1.2, 5.0 | 0.229 |
| Diastolic | 170 | −1.3 (13.8) | −3.4, 0.8 | 174 | −1.9 (13.1) | −3.9, 0.1 | −0.6 | −3.5, 2.2 | 0.673 |
| MAP** | 170 | −2.2 (12.9) | −4.2, −0.3 | 174 | −2.0 (12.3) | −3.9, −0.2 | 0.2 | −2.5, 2.9 | 0.873 |
p-value.
MAP: mean arterial pressure.
For women with previous pre-eclampsia with severe features, there was significantly greater reduction in blood pressure in the calcium than the placebo group (difference for systolic 4.0, 95% CI 0.7 to 3.3; diastolic 3.0, 95% CI 0.5 to 5.5 and mean arterial pressure 3.3, 95% CI 0.8 to 5.9 mmHg). For women with previous pre-eclampsia without severe features, there were no significant differences between calcium and placebo groups (Table 2). We used ANOVA analysis to compare the effect of calcium in the previous severe features group with the effect of calcium in the previous non-severe-features group. We found no statistically significant interaction between previous severity and treatment for systolic (p = 0.372), diastolic (p = 0.063) or mean blood pressure (p = 0.103).
4. Discussion
In this population of women with previous pre-eclampsia and low dietary calcium intake, 500 mg per day of calcium supplementation compared with placebo significantly lowered systolic and mean blood pressure over a 12-week period. The effect on diastolic blood pressure was similar in direction but smaller in magnitude, and it did not reach statistical significance. In sub-group analysis, there was a significantly greater reduction in all three elements of blood pressure in the calcium group for women with previous pre-eclampsia with severe features, but not those without severe features. However, the effect difference between those with and without severe features did not reach statistical significance.
Our study adds to the body of evidence on the effects of calcium supplementation on blood pressure in non-pregnant individuals.
The 500 mg calcium dose provided to our study population with low dietary calcium intake [12], [16], [17] was chosen to reach adequate calcium intake levels [21], as recommended in the Dietary Approaches to Stop Hypertension (DASH) diet [21]. DASH has been proven to decrease blood pressure and is recommended as part of a cardiovascular disease reduction strategy for hypertensive and normotensive individuals at increased risk of hypertension [22]. In contrast, calcium supplementation above adequate calcium intakes is not recommended to prevent or treat hypertension. There is contradictory evidence from cohort studies regarding the use of calcium supplementation above recommended levels which may actually increase coronary artery calcification and cardiovascular risk in older ages [23], [24], [25], [26].
Addressing modifiable risk factors is a key element of preventing future morbidity. Women with previous pre-eclampsia, particularly if the disease was of early onset or recurrent, are at increased risk of developing cardiovascular disease later in life [11], [27], [28]. Therefore, the reduction in systolic and mean arterial pressure with low-dose calcium supplementation in these non-pregnant women is of clinical importance. The magnitude of the blood pressure reduction observed in our trial is similar to the average 2.6/1.5 mmHg reduction seen following recommended reductions in dietary sodium intake [29]. Small changes (as low as a 2 mmHg reduction in systolic blood pressure) at a population level are associated with important reductions in vascular disease, including stroke, ischemic heart disease, and all-cause mortality [30], [31], [32]. The large dietary calcium intake deficiencies seen in low- and middle-income countries such as our trial sites [16] may be difficult to achieve without staple food fortification.
The strengths of this study are the double masked, randomized nature of calcium supplementation, recorded dietary calcium intake, and supplementation in a dose that could be achieved by food fortification and dietary intake [12]. With 791 participants, our trial increases by 25% the data available in the 2015 Cochrane review of calcium supplementation to prevent hypertension and is almost double the size of the subgroup less than 35 years of age (9 trials; 399 women) [7]. Also, blood pressure was measured in a standardized fashion and analysis was by intention-to-treat.
The baseline characteristics of the participants of this sub-study provided reassurance that the effectiveness of randomization was preserved in this group of women. However, interpretation of our results should take into account the fact that pre-pregnancy effects of calcium supplementation was not the primary purpose of the main trial.
In conclusion, modest calcium supplementation (500 mg/day) designed to achieve levels associated with adequate dietary intake was associated with a clinically important reduction in systolic and mean arterial pressure among women with prior pre-eclampsia, who are at increased cardiovascular risk. Our results would support strategies to improve calcium intake in women from low dietary calcium intake populations at higher risk for hypertension due to previous pre-eclampsia. Such approaches could include food fortification [21] or individualized supplementation of women with previous pre-eclampsia or eclampsia.
Acknowledgments
Acknowledgement
The calcium and pre-eclampsia (CAP) study is part of the PRE-EMPT (Pre-eclampsia-Eclampsia, Monitoring, Prevention and Treatment) study and is supported by the University of British Columbia, a grantee of the Bill & Melinda Gates Foundation; the UNDP/UNFPA/UNICEF/WHO/World Bank Special Programme of Research, Development and Research Training in Human Reproduction (HRP) at the Department of Sexual and Reproductive Health and Research at the World Health Organisation; and Argentina Fund for Horizontal Cooperation of the Argentinean Ministry of Foreign Affairs. We are grateful to the women who participated in the study and all who contributed to its conduct.
Ethics statement
Ethical approval was obtained from appropriate national and institutional ethical review bodies as applicable for each study site. The protocol of this trial has been approved by the Research Project Review Panel of the UNDP/UNFPA/UNICEF/WHO/World Bank Special Programme of Research, Development and Research Training in Human Reproduction (HRP) at the Department of Sexual and Reproductive Health and Research of WHO, and the WHO Research Ethics Review Committee, Geneva, Switzerland.
Calcium and Pre-eclampsia Study Group
Argentina: Fernando Althabe, José M Belizán, Eduardo Bergel, Alvaro Ciganda, Gabriela Cormick. Canada: Diane Sawchuck, Marianne Vidler. South Africa: Saadiqa Allie, John Anthony, Karlyn Frank, Annmarie de Greeff, Sue Fawcus, David Hall, Justus Hofmeyr, Mvuseleli Kovane, Patience Kovane, Theresa Lawrie, Simpiwe Mose, Nolundi Mshweshwe, Velisa Mqikela, Pamela Njikelana, Natalia Novikova, Adegboyega Oyebajo, Catherine Parker, Angel Phuti, Mandisa Singata-Madliki, Erika van Papendorp, Xoliswa Williams. Switzerland: Ana Pilar Betrán, Tina Dannemann, Armando Seuc. United Kingdom: Laura Magee, Peter von Dadelszen. USA: France Donnay, Sharla Drebit, James Roberts. Zimbabwe: Bothwell Guzha, Emilia Makaza, Sarah Manyame, Stephen Munjanja, Eunice Tahuringana.
Sources of funding
The original trial was funded by the University of British Columbia, a grantee of the Bill & Melinda Gates Foundation; UNDP/UNFPA/UNICEF/WHO/World Bank Special Programme of Research, Development and Research Training in Human Reproduction (HRP) at the Department of Sexual and Reproductive Health and Research of WHO, the Argentina Fund for Horizontal Cooperation of the Argentinean Ministry of Foreign Affairs and the Centre for Intervention Science in Maternal and Child Health, University of Bergen (CISMAC). The analysis presented in this manuscript has no funding to disclose.
Declaration of Competing Interest
The authors have declared that no competing interests exist.
References
- 1.Hofmeyr G.J., Lawrie T.A., Atallah A.N., Torloni M.R. Calcium supplementation during pregnancy for preventing hypertensive disorders and related problems. Cochrane Database Syst. Rev. 2018 doi: 10.1002/14651858.CD001059.pub5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Villa-Etchegoyen C., Lombarte M., Matamoros N., Belizan J.M., Cormick G. Mechanisms involved in the relationship between low calcium intake and high blood pressure. Nutrients. 2019;11(5):1112. doi: 10.3390/nu11051112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Centeno V., de Barboza G.D., Marchionatti A., Rodriguez V., de Talamoni N.T. Molecular mechanisms triggered by low-calcium diets. NutrResRev. 2009;22(2):163–174. doi: 10.1017/S0954422409990126. [DOI] [PubMed] [Google Scholar]
- 4.Griffith L.E., Guyatt G.H., Cook R.J., Bucher H.C., Cook D.J. The influence of dietary and nondietary calcium supplementation on blood pressure: an updated metaanalysis of randomized controlled trials. Am. J. Hypertens. 1999;12(1 Pt 1):84–92. doi: 10.1016/s0895-7061(98)00224-6. [DOI] [PubMed] [Google Scholar]
- 5.Reid I.R., Horne A., Mason B., Ames R., Bava U., Gamble G.D. Effects of calcium supplementation on body weight and blood pressure in normal older women: a randomized controlled trial. J. Clin. Endocrinol. Metab. 2005;90(7):3824–3829. doi: 10.1210/jc.2004-2205. [DOI] [PubMed] [Google Scholar]
- 6.Belizan J.M., Villar J., Pineda O., Gonzalez A.E., Sainz E., Garrera G. Reduction of blood pressure with calcium supplementation in young adults. JAMA. 1983;249(9):1161–1165. [PubMed] [Google Scholar]
- 7.Cormick G., Ciapponi A., Cafferata M.L., Belizan J.M. Calcium supplementation for prevention of primary hypertension. Cochrane Database Syst. Rev. 2015 doi: 10.1002/14651858.CD010037.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Dickinson H.O., Nicolson D.J., Cook J.V., Campbell F., Beyer F.R., Ford G.A. Calcium supplementation for the management of primary hypertension in adults. Cochrane Database Syst. Rev. 2006 doi: 10.1002/14651858.CD004639.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Global Burden of Disease (GBD): Institute of Health Metrics; 2020 [Available from: http://www.healthdata.org/gbd.
- 10.Seedat Y.K. Why is control of hypertension in sub-Saharan Africa poor? Cardiovasc. J. Afr. 2015;26(4):193–195. doi: 10.5830/CVJA-2015-065. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Dall'Asta A., D'Antonio F., Saccone G., Buca D., Mastantuoni E., Liberati M. Cardiovascular events following pregnancies complicated by preeclampsia with emphasis on the comparison between early and late onset forms: a systematic review and meta-analysis. Ultrasound Obstet. Gynecol. 2020 doi: 10.1002/uog.22107. [DOI] [PubMed] [Google Scholar]
- 12.Hofmeyr G.J., Betran A.P., Singata-Madliki M., Cormick G., Munjanja S.P., Fawcus S. Prepregnancy and early pregnancy calcium supplementation among women at high risk of pre-eclampsia: a multicentre, double-blind, randomised, placebo-controlled trial. Lancet. 2019;393(10169):330–339. doi: 10.1016/S0140-6736(18)31818-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Lawrie T.A., Betran A.P., Singata-Madliki M., Ciganda A., Hofmeyr G.J., Belizan J.M. Participant recruitment and retention in longitudinal preconception randomized trials: lessons learnt from the Calcium And Pre-eclampsia (CAP) trial. Trials. 2017;18(1):500. doi: 10.1186/s13063-017-2220-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Hofmeyr G.J., Seuc A.H., Betran A.P., Purnat T.D., Ciganda A., Munjanja S.P. The effect of calcium supplementation on blood pressure in non-pregnant women with previous pre-eclampsia: An exploratory, randomized placebo controlled study. Pregnancy Hypertens. 2015;5(4):273–279. doi: 10.1016/j.preghy.2015.04.001. [DOI] [PubMed] [Google Scholar]
- 15.Cormick G., Gibbons L., Belizan J.M. Impact of water fortification with calcium on calcium intake in different countries: a simulation study. Public Health Nutr. 2020;1–14 doi: 10.1017/S1368980020002232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Cormick G., Betran A.P., Romero I.B., Lombardo C.F., Gulmezoglu A.M., Ciapponi A. Global inequities in dietary calcium intake during pregnancy: a systematic review and meta-analysis. BJOG. 2019;126(4):444–456. doi: 10.1111/1471-0528.15512. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Cormick G., Betrán A.P., Harbron J., Dannemann Purnat T., Parker C., Hall D. Are women with history of pre-eclampsia starting a new pregnancy in good nutritional status in South Africa and Zimbabwe? BMC Preg. Childbirth. 2018;18(1):236. doi: 10.1186/s12884-018-1885-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Kumssa D.B., Joy E.J., Ander E.L., Watts M.J., Young S.D., Walker S. Dietary calcium and zinc deficiency risks are decreasing but remain prevalent. Sci. Rep. 2015;5:10974. doi: 10.1038/srep10974. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Cormick G., Zhang N.N., Andrade S.P., Quiroga M.J., Di Marco I., Porta A. Gaps between calcium recommendations to prevent pre-eclampsia and current intakes in one hospital in Argentina. BMC Res Notes. 2014;7:920. doi: 10.1186/1756-0500-7-920. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Guideline W.H.O. World Health Organization; Geneva: 2013. Calcium Supplementation in pregnant Women. [PubMed] [Google Scholar]
- 21.Cormick G., Belizan J.M. Calcium intake and health. Nutrients. 2019;11:7. doi: 10.3390/nu11071606. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Jee S.H., Miller E.R., 3rd, Guallar E., Singh V.K., Appel L.J., Klag M.J. The effect of magnesium supplementation on blood pressure: a meta-analysis of randomized clinical trials. Am. J. Hypertens. 2002;15(8):691–696. doi: 10.1016/s0895-7061(02)02964-3. [DOI] [PubMed] [Google Scholar]
- 23.Tankeu A.T., Ndip Agbor V., Noubiap J.J. Calcium supplementation and cardiovascular risk: A rising concern. J Clin Hypertens (Greenwich). 2017;19(6):640–646. doi: 10.1111/jch.13010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Lewis J.R., Calver J., Zhu K., Flicker L., Prince R.L. Calcium supplementation and the risks of atherosclerotic vascular disease in older women: results of a 5-year RCT and a 4.5-year follow-up. J. Bone Miner. Res. 2011;26(1):35–41. doi: 10.1002/jbmr.176. [DOI] [PubMed] [Google Scholar]
- 25.Lewis J.R., Radavelli-Bagatini S., Rejnmark L., Chen J.S., Simpson J.M., Lappe J.M. The effects of calcium supplementation on verified coronary heart disease hospitalization and death in postmenopausal women: a collaborative meta-analysis of randomized controlled trials. J. Bone Miner. Res. 2015;30(1):165–175. doi: 10.1002/jbmr.2311. [DOI] [PubMed] [Google Scholar]
- 26.Lewis J.R., Zhu K., Prince R.L. Adverse events from calcium supplementation: relationship to errors in myocardial infarction self-reporting in randomized controlled trials of calcium supplementation. J. Bone Miner. Res. 2012;27(3):719–722. doi: 10.1002/jbmr.1484. [DOI] [PubMed] [Google Scholar]
- 27.Bokslag A., Teunissen P.W., Franssen C., van Kesteren F., Kamp O., Ganzevoort W. Effect of early-onset preeclampsia on cardiovascular risk in the fifth decade of life. Am. J. Obstet. Gynecol. 2017;216(5) doi: 10.1016/j.ajog.2017.02.015. 523 e1-e7. [DOI] [PubMed] [Google Scholar]
- 28.Brouwers L., van der Meiden-van Roest A.J., Savelkoul C., Vogelvang T.E., Lely A.T., Franx A. Recurrence of pre-eclampsia and the risk of future hypertension and cardiovascular disease: a systematic review and meta-analysis. BJOG. 2018;125(13):1642–1654. doi: 10.1111/1471-0528.15394. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Cormick G., Betran A.P., Metz F., Palacios C., Beltran-Velazquez F., Garcia-Casal M.L.N. Regulatory and policy-related aspects of calcium fortification of foods. Implications for implementing national strategies of calcium fortification. Nutrients. 2020;12(4) doi: 10.3390/nu12041022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Lewington S., Clarke R., Qizilbash N., Peto R., Collins R., Prospective S.C. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360(9349):1903–1913. doi: 10.1016/s0140-6736(02)11911-8. [DOI] [PubMed] [Google Scholar]
- 31.Whelton P.K., He J., Appel L.J., Cutler J.A., Havas S., Kotchen T.A. Primary prevention of hypertension: clinical and public health advisory from The National High Blood Pressure Education Program. JAMA. 2002;288(15):1882–1888. doi: 10.1001/jama.288.15.1882. [DOI] [PubMed] [Google Scholar]
- 32.Stamler J. Blood pressure and high blood pressure. Aspects of risk. Hypertension. 1991;18(3 Suppl.):I95–I107. doi: 10.1161/01.hyp.18.3_suppl.i95. [DOI] [PubMed] [Google Scholar]