

Abstract
In families raising a child with an autism spectrum disorder (ASD), infant siblings are at elevated risk for ASD and other developmental concerns, including elements of the broader autism phenotype (BAP). Typically, the BAP is indexed using standardized developmental assessments; however, these measures do not capture a number of social difficulties commonly associated with the BAP. The present study aims to expand our developmental understanding of the BAP by comparing children exhibiting the BAP to their typically developing peers on, (1) standardized measures of development, and (2) social behaviors exhibited during dyadic play interactions.
As part of a prospective study, dyads were recruited from families with at least one older child with ASD (high-risk, n = 36), and families with no history of ASD (low-risk, n = 38). During laboratory visits at 12, 15, 18, and 24 months of age, infants completed a series of standardized assessments and a mother-child play interaction. Dyadic play interactions were micro-analytically coded for gaze, positive affect, and vocalizations to create theory-driven composites to index dyadic synchrony and responsiveness. Videos were also coded with an existing rating scheme for joint engagement and child responsiveness.
Multilevel models revealed significant group differences on select constructs within the first two years. Language and cognitive differences emerged by 24 months of age, whereas dyadic differences were evident as early as 15 months. Recognizing the increasing demand for elevated-risk interventions, these findings highlight several social constructs through which interventions may identify risk and promote optimal development.
Keywords: broader autism phenotype, infant sibling, autism spectrum disorder, mother-child interactions, responsiveness, joint engagement
LAY SUMMARY
In families raising children with an autism spectrum disorder (ASD), younger siblings are at an increased risk for social and developmental difficulties that characterize a “broader autism phenotype”. The present study explored the emergence of social, language, and cognitive differences in the first two years of life. Social differences were evident as early as 15 months of age for several play-based measures, and language and cognitive differences emerged by 24 months of age. For infant siblings of children with ASD, some of the earliest behavioral marks for subclinical features of ASD are evident within the first two years of life.
Introduction
In families raising children with autism spectrum disorder (ASD), subclinical features of ASD, often called the broader autism phenotype (BAP), are common (Constantino et al., 2010; Georgiades et al., 2013; Messinger et al., 2013). Studies of infant siblings of children with ASD document elevated rates of BAP features with standardized developmental assessments (Georgiades et al., 2013; Ozonoff et al., 2014). However, clinically and within research studies, it can be difficult to distinguish individuals with the BAP from those with ASD or typical development (TYP), especially early in development. To inform this differential risk/diagnosis gap, the goals of the current study were two-fold. First, we aimed to replicate previous research that distinguish BAP and TYP groups using standardized developmental assessments. Second, we aimed to expand our understanding of how dyadic interactions in early childhood may capture social difficulties associated with the BAP, in order to inform current developmental monitoring and early intervention efforts.
Defining the BAP
Multiple definitions of the BAP are currently used in research which build on self-report questionnaires, spousal reports, parent concerns, and clinical best estimates. However, due to the range of functioning levels within observed differences and countless possible combinations of risk factors, there is no current standardized criteria for the BAP (see review by Pisula & Ziegart-Sadowska, 2015). Initial measurement techniques for capturing BAP involved clinical interviews; however, now a variety of questionnaires exist for quickly measuring BAP characteristics in adults and/or children aged 3 and older (e.g., Autism Spectrum Quotient, Baron-Cohen et al., 2001; Broader Autism Phenotype Questionnaire, Hurley et al., 2007; Social Responsiveness Scale, Constantino, 2002). The self- or parent-reported questionnaires listed above have been used in numerous studies to either characterize BAP or distinguish between BAP and ASD in individuals beyond early childhood (e.g., Ruzich et al., 2015; Sasson et al., 2014; Maxwell et al., 2013; Wheelwright et al., 2010). However, for children under 3 years, clinical judgments and standardized developmental assessments typically inform impressions of the BAP (e.g., Ozonoff et al., 2014).
In early childhood, recent studies have explored criteria for capturing the BAP in high-risk infant siblings including clinical judgments, scores below average on standardized developmental assessments, and/or elevated scores on the Autism Diagnostic Observation Schedule (ADOS; e.g., Landa et al., 2012; Ozonoff et al., 2014; Messinger et al., 2013). For example, Messinger et al. (2013) used the Mullen Scales of Early Learning (MSEL) developmental quotients and ADOS severity scores to characterize non-ASD infants that may have features consistent with the BAP. In Messinger et al. (2013), five BAP trajectories/patterns were identified, two of which were statistically distinguishable from typically developing peers. In another BAP-specific study, Ozonoff and colleagues (2014) defined BAP outcome criteria as: (1) being a high-risk infant sibling, (2) not meeting clinical best estimate criteria for an ASD, and (3) having lower scores on the MSEL and/or elevated ADOS severity scores (i.e., severity scores of ≤ 3). To ground the current study within these frameworks, we used Ozonoff and colleagues’ (2014) explicit criteria for BAP outcome classifications and interpreted our findings, while considering Messinger et al.’s (2013) five BAP trajectories/patterns.
It is important to note that elements of the BAP may be present in any family - they are not restricted to families raising children with ASD. Several studies have addressed the BAP within general populations (e.g., Klusek et al., 2014; Swanson et al., 2013). Given our sampling constraints (data utilized from an existing infant sibling study), addressing the BAP in first-born children or more general populations (e.g., as discussed in Landry & Chouinard, 2016) was beyond the scope of the current study.
BAP Development
Prospective studies interested in atypical development have compared groups of infants with non-ASD and/or non-TYP outcomes (e.g., Chawarska et al., 2014; Clifford et al., 2013, Cornew et al., 2012; Rozga et al., 2011; Sullivan, et al., 2007; Yirmiya et al., 2006). Studies like Rozga et al. (2011) do provide evidence of emerging differences in social communication, though it is often unclear if all of these infants have features consistent with the BAP. In one of the few studies to explicitly focus on the BAP, Ozonoff and colleagues (2014) tracked high-risk infant siblings from 6 to 36 months and noted that by 12 months, infants exhibit features consistent with the BAP. Specifically, the BAP group (35% of the high-risk sample) displayed significantly slower growth in language and visual reception skills when compared to typically developing infants, as indexed by the MSEL.
When considering dyadic/social difficulties, the following infant sibling studies can inform our understanding of BAP development. Yirmiya et al.’s (2006) study included a parent-child interaction at 4 months of age and reported that five high-risk non-ASD infants with language delays were slightly less synchronous with their mothers than high-risk non-language delayed and typically developing peers. Sullivan and colleagues (2007) examined response to joint attention bids in high-risk infants with clearly defined outcomes of ASD, BAP, and non-BAP, and descriptively noted that infants with the BAP at 14 months looked less to target cues. Specific to social referencing, Cornew and colleagues (2012) found that 18 month old high-risk infants with non-ASD and non-typical outcomes only showed slightly lower frequencies of information seeking when playing with novel toys (than their typically developing peers). Overall, these findings highlight that distinct behavioral differences linked to later ASD and Non-TYP outcomes are present in early childhood. However, to date few studies evaluate distinct developmental patterns in the BAP, especially within a social context.
Importance of exploring BAP in early childhood
To fully understand ASD, it is necessary to understand similarities and differences in developmental trajectories and/or pathways in subclinical and typical populations. We do not yet completely understand what is contributing to the full manifestations of ASD; therefore, systematic longitudinal examination of children’s development allows researchers to track possible underpinnings that may lead to adaptive or maladaptive outcomes (Cicchetti, 2014). This approach allows developmental trajectories to be observed while considering equifinality and multifinality. Equifinality posits that a given outcome may result from multiple pathways and multifinality recognizes that multiple outcomes are possible from a common starting point. As a complement to studies of children with ASD, studies of children with the BAP can specifically inform the intermediate pathways (those that are often the most difficult to discern from typical and pathological pathways).
Measuring Dyadic Interactions
The present study sought to build on previous studies of the BAP by examining social behaviors in the context of dyadic social interactions, which we conceptualize using two complementary approaches. Given the complexity of dyadic interactions, no one measurement tool can capture all elements of an exchange. Therefore, dyadic data is heavily influenced by coding and quantification procedures. Varied measurement techniques likely reflect the types of research questions, as well as the age of the participants. For example, constructs requiring more context to the behavior, such as joint engagement, maternal sensitivity, or directedness, often use global rating scales that enable the rater to incorporate context when assigning a general impression (e.g., see Adamson et al., 2012, 2014; Campbell et al., 2015, Freeman & Kasari, 2013; Wan et al., 2012, 2013). Alternatively, when answering questions related to temporal order or process (e.g., synchrony), discrete micro-level codes – which capture directly observable, objective core social behaviors – allow researchers to document subtle behaviors that may not be easily captured at a broader level (e.g., Lambert-Brown et al., 2015; Leezenbaum et al., 2014, Ozonoff et al., 2010; Warlaumont et al., 2014). These diverse coding techniques, may be contributing to the reported mixed representations of observed behavioral differences across outcome groups (particularly within the first year), as well as an inability to directly compare results with similar samples across studies.
Most recently, Green and colleagues (2017) incorporated both global rating scales and discrete micro-level codes when examining mother-child interactions in a pre- and post-treatment study. They reported that global measures better captured between-person variability in select play behaviors (e.g., child attentiveness); however, micro-level codes were more successful at capturing shifts in social behavior that occurred in response to treatment. The current study builds upon two existing paradigms (i.e., discrete micro-level and global rating approaches) to provide a more complete representation of dyadic interactions. This two-pronged approach was used because (1) the BAP is not clearly defined and characterized in the field, and (2) it is unknown if a more micro-analytic or global/gestalt approach will better capture meaningful dyadic characteristics in individuals with the BAP over time.
Current Study
The goals of the current study are two-fold. Aim 1: to replicate previous research that distinguishes between BAP and TYP groups using standardized developmental assessments (e.g., Ozonoff et al., 2014; Landa et al., 2012). Specifically, we expect infants within the BAP group (compared to the TYP group) to perform lower on visual reception, language, communication, and socialization measures. Aim 2: to explore how dyadic interactions in early childhood may capture social difficulties associated with the BAP. Based on previous research, we expect children within the BAP group to exhibit less dyadic synchrony, responsiveness, and joint engagement (than children in the TYP group). We also expect dyadic differences in the BAP to be evident within the second year of life. The current study’s unique contribution includes a longitudinal examination of social/communication characteristics within the BAP during a naturalistic social task designed to capture dyadic exchanges.
Method
Participants
Ninety-nine mother-child dyads were recruited from the greater Lafayette area of Indiana to participate in a prospective infant-siblings study, which included high-risk (HR, n = 45) and low-risk (LR, n = 54) groups. The HR group included younger infant siblings from a family raising at least one child with a confirmed ASD diagnosis, and the LR group were of any birth order and had no familial history of ASD in 1st, 2nd, or 3rd degree relatives. Infants completed a series of developmental monitoring assessments at 12, 15, 18, 24, 30, and 36 months of age.
Outcome groups for infant siblings were assessed at their final laboratory visit at 24, 30, or 36 months of age. If a child attended more than one of these visits, the last visit was used for outcome determination. Outcome assessment age was based on time of enrollment, such that children enrolled earlier in the study could be followed to an older age. Based on outcome criteria developed by the Baby Siblings Research Consortium (BSRC; see Ozonoff et al., 2014), infants were classified into one of three defined groups: Typical Development (TYP; n = 52), Non-Typical Development (Non-TYP; n = 34), or Autism Spectrum Disorder (ASD; n = 6). Seven children did not complete a visit between 24 and 36 months and therefore did not receive an outcome classification (and were thus excluded). Non-TYP outcomes included children with language delays, clinically relevant behavioral challenges, global developmental delay, and children exhibiting sub-threshold autism characteristics.
Out of the 34 children within the Non-TYP group, 22 demonstrated features consistent with BAP based on Ozonoff et al.’s (2014) criteria, which include being an infant sibling of ASD, MSEL raw scores (i.e., subscale scores 1.5 to 2 standard deviations below the mean), and ADOS severity scores below the cutoff for an ASD (≤ 3). Within the current study, the 12 children not meeting Ozonoff et al.’s (2014) BAP criteria included children enrolled as low-risk siblings that demonstrated language difficulties, or other non-typical concerns by their outcome visit. These children were excluded from analyses. Thus, the final sample size for the current study included 74 families (BAP n = 22; TYP n = 52; see Figure 1). The majority of these families completed an outcome visit at 30 or 36 months (n = 67). Seven families completed their outcome visit at 24 months (BAP = 2, TYP = 5). Family demographic details are provided in Table 1. Families included in the present study did not differ from those in the larger study with respect to infant sex, maternal age, and education (all ps > .05).
Figure 1. Flowchart of prospective developmental monitoring risk status to assigned outcomes by 24 to 36 months of age.
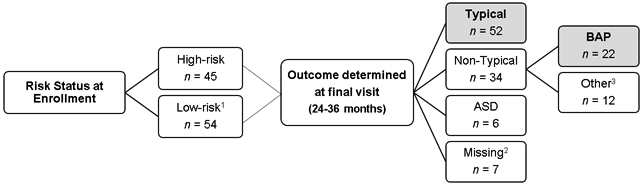
1 Of the 54 low-risk infants, 38 infants were later characterized as typically developing.
2 Seven children did not complete a final visit in order to be assigned an outcome classification.
3 The 12 “other” children refer to low-risk siblings that demonstrated language delays or other concerns by outcome.
Table 1.
Sample demographic information stratified by outcome status.
| BAP | TYP | |
|---|---|---|
| N | 22 | 52 |
| Infant sex, n(%) | ||
| Male | 15(68%) | 29(56%) |
| Infant race, n(%) | ||
| African American | 1(5%) | 1(1%) |
| Caucasian | 20(91%) | 46(92%) |
| Multiracial | 1(5%) | 3(4%) |
| Other | 0(0%) | 1(1%) |
| Unreported | 0(0%) | 1(1%) |
| Outcome Characteristics | ||
| Age in months, M(SD) | 31.83(4.3) | 31.56(4.4) |
| ADOS symptom severity, M(SD) | 2.41(1.5) | 1.24(0.7) |
| MSEL verbal DQ, M(SD) | 85.26(18.4) | 106.80(16.0) |
| MSEL nonverbal DQ, M(SD) | 89.28(11.3) | 108.06(15.6) |
| Maternal Characteristics | ||
| Maternal age in years, M(SD) | 30.17(4.2) | 31.67(4.1) |
| Maternal education, n(%) | ||
| High school or GED | 1(5%) | 2(4%) |
| Trade or vocational | 2(9%) | 0(0%) |
| Associates or 2 year degree | 7(32%) | 2(4%) |
| Some college | 2(9%) | 4(8%) |
| College degree | 8(36%) | 32(62%) |
| Master’s degree | 1(5%) | 9(17%) |
| Professional degree | 1(5%) | 3(6%) |
Note: ADOS = Autism Diagnostic Observation Schedule. MSEL = Mullen Scales of Early Learning. DQ = developmental quotient. GED = General Educational Development.
Measures and Procedure
All procedures and measures were approved by Purdue University’s Institutional Review Board. As a part of a larger developmental behavioral battery, infants/toddlers participated in a videotaped parent-child play task and completed developmental assessments at 12, 15, 18, and 24 months of age. At 24, 30, and 36 months of age, infants/toddlers completed a similar battery with the addition of the ADOS-2 to aid in their outcome classification.
Mother-child interactions.
During the mother-child play task a standardized set of age-appropriate toys were utilized, including: a baby-doll, blanket, ball, shape sorter, car, rattle, and a pair of toy phones. Mothers were asked to play with their children as they typically would at home for 5-10 minutes. Video recordings of the dyadic interactions were coded in Mangold INTERACT’s behavioral coding program, Version 15. Coders (N = 20) were unaware of risk and outcome status and were assigned to only one coding scheme (micro-analytic or global, detailed below) to avoid any bias from one code to another.
Micro-analytic coding.
Child and mother gaze, positive affect, and vocalizations were independently coded using a discrete micro-analytic approach for the first three minutes of the interaction following coding criteria established in Ozonoff et al. (2010). Research assistants were trained to watch the digital records to capture within-second changes in each target behavior using the slow-motion feature in Mangold INTERACT. Consistent with Ozonoff et al. (2010), behaviors lasting 0.5 seconds or more were counted towards respective frequency counts. In addition for brief behaviors, (e.g., look face to look object) the shift must have occurred for at least 0.5 seconds to be counted as a separate behavior. With these base codes, frequency estimates for each behavior (gaze, positive affect, vocalizations) for mother and child, respectively, were exported from Mangold INTERACT and post-processed using a Python script (Version 2.7).
To index dyadic synchrony (DS), infant responsiveness (IR), and maternal responsiveness (MR), theory driven composites were adapted from Feldman (2007). Specific to DS, the frequency composite included instances of mutual synchrony for shared gaze and positive affect, respectively, and responsiveness to each play partner. The responsiveness composites (detailed note in Table 2) included frequency counts for social responses within 0.5 seconds of partner initiations (e.g., infant-led positive affect followed by a maternal vocalization).
Table 2.
Descriptive statistics for the standardized measures and social constructs at 12, 15, 18, and 24 months of age.
| 12 Months |
15 Months |
18 Months |
24 Months |
|||||
|---|---|---|---|---|---|---|---|---|
| BAP |
TYP |
BAP |
TYP |
BAP |
TYP |
BAP |
TYP |
|
| n(# Male) | 12(8) | 19(11) | 11(9) | 27(14) | 21(15) | 47(26) | 22(13) | 50(27) |
| MSEL Mean (SE) | ||||||||
| Visual Receptioni | 14.6 (0.8) | 15.6 (0.3) | 17.6 (0.7) | 18.6 (0.3) | 19.5 (0.5) | 20.1 (0.3) | 24.2 (0.8)* | 26.1 (0.6) |
| Receptive Languageim | 11.6 (0.6) | 13.4 (0.3) | 13.6 (0.3) | 14.7 (0.3) | 16.2 (1.0) | 18.1 (0.5) | 21.3 (1.0)** | 25.7 (0.4) |
| Expressive Language | 11.7 (0.8) | 12.1 (0.6) | 13.5 (0.5) | 14.7 (0.5) | 15.4 (0.7) | 16.7 (0.3) | 18.9 (0.8)** | 22.2 (0.5) |
| n(# Male) | 12(8) | 19(11) | 12(9) | 28(14) | 21(15) | 47(27) | 22(15) | 50(28) |
| VABS Mean (SE) | ||||||||
| Socialization | 100.8 (2.9) | 99.0 (1.6) | 98.9 (3.0) | 99.8 (1.5) | 99.0 (1.8) | 100.7 (1.4) | 98.3 (2.2)* | 103.1 (1.1) |
| Communicationi | 94.8 (4.6) | 99.4 (2.4) | 95.3 (3.1) | 100.3 (1.5) | 92.1 (2.4) | 97.7 (1.0) | 93.8 (2.8)* | 102.0 (1.1) |
| n(# Male) | 10(7) | 14(11) | 11(8) | 20(14) | 13(9) | 37(27) | 17(11) | 34(28) |
| Micro Mean (SE) | ||||||||
| Dyadic Sync | 20.6 (3.3) | 26.1 (3.3) | 23.6 (3.3) | 26.9 (2.9) | 24.5 (2.8) | 26.4 (2.0) | 25.8 (3.1) | 27.9 (2.3) |
| Infant Resp | 12.3 (1.8) | 15.4 (1.8) | 5.6 (2.1)* | 14.1 (1.8) | 13.2 (1.4) | 14.7 (1.0) | 14.2 (1.6) | 15.0 (1.2) |
| Maternal Resp | 8.3 (1.6) | 10.7 (1.7) | 11.2 (1.5)* | 11.6 (1.0) | 20.6 (3.3) | 26.1 (3.3) | 11.6 (1.6) | 12.9 (1.1) |
| Global Mean (SE) | ||||||||
| Total JE | 4.5 (.0.2) | 4.1 (0.3) | 3.6 (0.3)* | 5.2 (0.3) | 4.5 (0.4) | 4.9 (0.2) | 4.1 (0.3)* | 5.1 (0.2) |
| Supported JE | 4.8 (0.2) | 4.3 (0.4) | 3.9 (0.3)* | 5.1 (0.2) | 4.7 (0.3) | 5.1 (0.2) | 4.4 (0.3)* | 5.2 (0.2) |
| Coordinated JE | 2.1 (0.2) | 1.8 (0.2) | 1.7 (0.1)* | 2.8 (0.2) | 1.7 (0.2) | 2.0 (0.1) | 2.1 (0.2) | 2.4 (0.2) |
| CRP | 3.8 (0.3) | 3.9 (0.3) | 4.3 (0.2) | 4.6 (0.2) | 3.7 (0.2)* | 4.4 (0.2) | 3.9 (0.3) | 4.4 (0.2) |
Notes: MSEL: Mullen Scales of Early Learning. VABS: Vineland Adaptive Behavior Scales.
infant sex is a significant covariate.
maternal education is significant covariate.
Resp = responsiveness. JE = Joint engagement. CRP = child responsiveness pattern.
p values < .05
p values < .001
Coder training included reading the manual, co-coding with a master coder (1-3 interactions), completion of a practice set followed by feedback, and independent competition of a reliability set of ten interactions. Interactions in the reliability sets were coded by a master coder. All reliable coders achieved our a priori intra-class correlation coefficients (ICC) threshold of > .70 (Range: .77 to .99, M = .93). Periodic unannounced reliability checks were conducted and documented consistent ICCs above .70 (Range: .73 to .99, M = .94).
Global ratings.
Separate coders rated parent-child play interactions for joint engagement and child responsiveness on a 7-point Likert scale using a subset of Adamson, Bakeman, and Suma’s Joint Engagement Rating Inventory (JERI, 2016). The joint engagement ratings (i.e., total joint (TJE), supported joint (SJE), and coordinated joint (CJE)) are categorical variables with values ranging from 1 to 7 to index time spent and the quality of the engagement. Child responsiveness was also captured from the rating scheme (ranging from, 1 - almost always declining bids, to 7 - complying and anticipating most all bids). Henceforth we will refer to this rating as child responsiveness pattern (CRP) to avoid confusion with the micro-analytic IR code. CRP captures the global nature of the child’s responsiveness pattern (and the micro-analytic codes only capture if and how often an infant responded to a bid). The global rating training process paralleled the one described above (ICCs range: .80 to .90, M = .87). Coders also received periodic unannounced reliability checks which documented consistent ICCs above .70 (Range: .83 to 1.00, M = .94).
Autism Diagnostic Observation Scales, Second Edition (ADOS-2).
The ADOS-2 is a semi-structured standardized diagnostic tool to measure symptoms of autism in the social communication and restricted and repetitive behavior domains (Lord et al., 2000). At each child’s outcome visit, a graduate student (trained by an ADOS-2 certified trainer and supervised by a research-reliable ADOS-2 investigator) administered and scored the ADOS-2. For the current study, ADOS-2 severity scores were included to determine children’s outcome classification, using criteria established in Ozonoff et al. (2014).
Mullen Scales of Early Learning (MSEL).
The MSEL measures cognitive ability in children from birth to 68 months across five scales: gross motor (GM), fine motor (FM), visual reception (VR), receptive language (EL), and expressive language (EL; Mullen, 1995). Raw scores on the VR, RL, and EL subscales were used to determine whether children met BAP criteria, as presented in Ozonoff et al. (2014).
Vineland Adaptive Behavior Scales (VABS).
The VABS is a parent report measure that assesses children’s skills on four main domains: motor, communication, daily living skills, and socialization (Sparrow et al., 1984). In this study, the socialization (Soc) and communication (Com) domain scores were used to index developmental functioning over time.
Data Analysis
All data were checked for analytic assumptions (i.e., homoscedasity and normality) and cleaned using IBM Statistical Package for the Social Sciences (SPSS) Version 24. Descriptive statistics for each variable of interest are provided in Table 2. Multilevel models were conducted in SAS Version 9.4 to account for the small sample size and missing data patterns. Additionally, to limit the possibility of making a Type I error, the Benjamini-Hochberg Procedure (1995) was applied to control for false discovery rates without invalidating the overall results for each aim, respectively.
Aim 1: To replicate previous studies describing the BAP using standardized developmental assessments, we first examined developmental functioning using the MSEL and VABS to determine if the BAP group is distinguishable across the selected domains/subscales. The final set of models included fixed effects for group membership, visit, the interaction between group and visit, and two covariates: infant sex and years of maternal education. We also included random effects for the intercept (see Supplement 1 for model fit details). To aid in interpretation, a series of post-hoc ANOVAs and multilevel models were also conducted. Post-hoc analyses for Aim 1 also included a series of models wherein children with 24-month outcomes ratings were removed. These models explored if partially tautological predictor-outcome determinations generated systematic differences (i.e., using language scores to determine outcome and then testing the difference in language scores across outcome groups).
Aim 2: For this aim, a series of multilevel models were conducted to examine: 1) if the BAP group is distinguishable from the TYP group within a social context, and 2) if differences exist, when do they emerge. Separate linear models were conducted for each variable. The final set of models included fixed effects for group membership, visit, the interaction between group and visit, and two covariates: infant sex and years of maternal education (ranging from 12 to 20 years). We also included random effects for the intercept. To aid in interpretation, a series of post-hoc ANOVAs and additional multilevel models were also conducted.
RESULTS
Aim 1
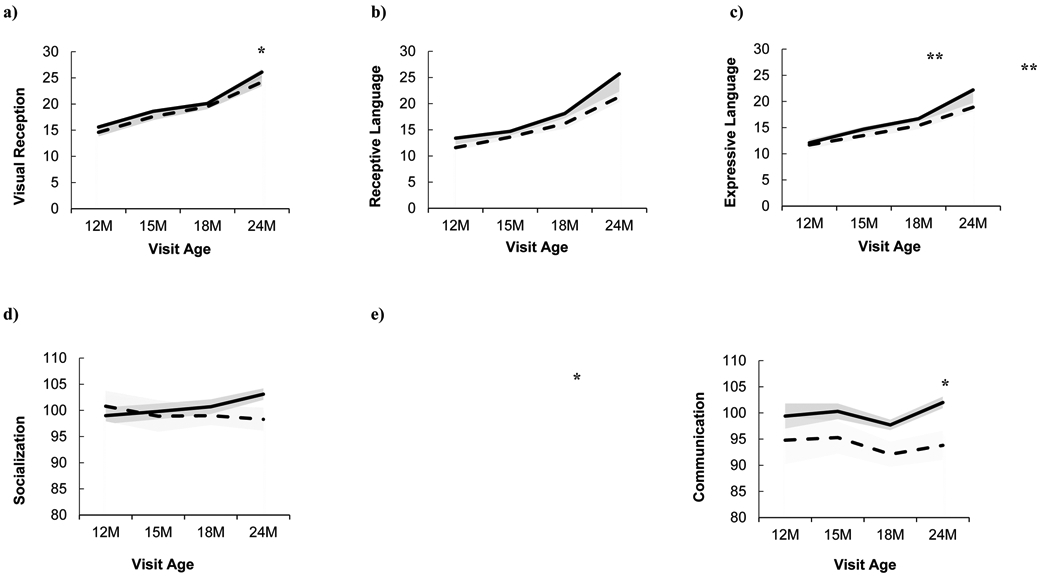
By 24 months of age, average group differences were evident for the five tested domains/subscales: VR, RL, EL, Soc, and Com (Table 3). Regardless of outcome group classification, developmental growth from 12 to 24 months was apparent for the MSEL VR, RL, and EL subscales, as well as for the VABS Com and Soc subscales (Figure 2). When considering group membership, although children in the BAP group demonstrated growth, children within the TYP group had significantly more growth on the RL and EL subscales, from 12 to 24 months of age. To isolate the age at which these trajectories diverged, estimated marginal means were analyzed by including visit as a categorical variable, revealing only a significant difference at 24 months of age across the five subscales. Infant sex was a significant covariate for VR and EL, with boys scoring higher than girls. Maternal education was only a significant covariate for RL.
Table 3.
Linear model parameter estimates for the MSEL and VABS developmental functioning measures.
| Visual Reception |
Receptive Language |
Expressive Language |
Socialization |
Communication |
||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Fixed Effects | Estimate (SE) | t | Estimate (SE) | t | Estimate (SE) | t | Estimate (SE) | t | Estimate (SE) | t |
| Group | 0.94(1.8) | 0.53 | 3.40(1.9) | 1.75 | 3.56(1.7) | 2.12* | 6.64(4.7) | 1.41 | 3.28(5.1) | 0.64 |
| Visit | 0.88(0.1) | 16.54** | 1.13(0.1) | 19.38** | 0.86(0.1) | 17.83** | 0.29(0.1) | 2.18* | 0.28(0.1) | 1.91 |
| Group x Visit1 | −0.09(0.1) | −1.01 | −0.29(0.1) | −2.87* | −0.27(0.1) | −3.21* | −0.49(0.2) | −2.15* | −0.42(0.3) | −1.69 |
| Infant Sex2 | −1.04(0.4) | −2.40* | −1.39(0.5) | −2.89* | −0.95(0.5) | −1.82 | −2.41(1.7) | −1.44 | −4.37(1.8) | −2.48* |
| Maternal Edu | 0.19(0.1) | 1.71 | 0.30(0.1) | 2.37* | 0.14(0.1) | 1.02 | −0.59(0.5) | −1.31 | 0.40(0.5) | 1.05 |
| Estimated Marginal Means3 | ||||||||||
| Group x 12M Visit | 0.80(1.0) | 0.77 | 1.55(1.1) | 1.40 | 0.13(1.0) | 0.13 | −1.08(3.0) | −0.36 | 3.54(3.2) | 0.27 |
| Group x 15M Visit | 0.32(1.0) | 0.32 | 0.02(1.1) | 0.02 | 0.03(1.0) | 0.03 | 1.96(2.9) | 0.68 | 1.57(3.1) | 0.51 |
| Group x 18M Visit | 0.28(0.7) | 0.37 | 1.46(0.8) | 1.79 | 1.03(0.8) | 1.31 | 1.85(2.3) | 0.79 | 4.24(2.5) | 1.72 |
| Group x 24M Visit | 1.57(0.74) | 2.12* | 3.81(0.8) | 4.77** | 3.01(0.8) | 3.97** | 5.17(2.3)* | 2.26* | 7.12(2.4) | 2.94* |
Note:
Minus denotes BAP.
Minus denotes Female.
Separate models were specified for marginal means treating visit as a categorical variable to identify when differences emerged.
p values < .05
p values < .001
Figure 2. BAP and TYP group standardized scores for (a) MSEL visual reception, (b) MSEL receptive language, (c) MSEL expressive language, (d) VABS socialization, (e) VABS communication.
Aim 1 Post-hoc Analyses
To address any potential tautological predictor-outcome determination concerns for the seven children with 24 month outcome classifications and the MSEL results in Aim 1, models for VR, RL, and EL were conducted both with and without these seven participants. The exclusion of these participants impacted an initially trending RL difference by group at 18 months (p = .07) to being significant (p = .03). In addition, maternal education was no longer a significant covariate for RL.
Aim 2
Children within the BAP group did exhibit significantly different scores on the micro-analytic composites for IR and MR (Figures 3b and c; Table 4) and global ratings for TJE, SJE, CJE, and CRP (Figures 4a-d; Table 5). Regardless of outcome classification, mothers were more responsive to child bids as children matured (see MR column, Table 4). Children also demonstrated significant growth from 12 to 24 months in SJE, regardless of outcome classification (Table 5). To examine when social-based differences emerged, estimated marginal means were examined and revealed that the TYP group demonstrated more social competence than the BAP group on the IR, MR, TJE, SJE, CJE (15 months), CRP (18 months), and TJE, SJE (24 months; Tables 4-5).
Figure 3. BAP and TYP group means and standard errors for the micro-analytic codes (a) dyadic synchrony, (b) infant responsiveness, and (c) maternal responsiveness.
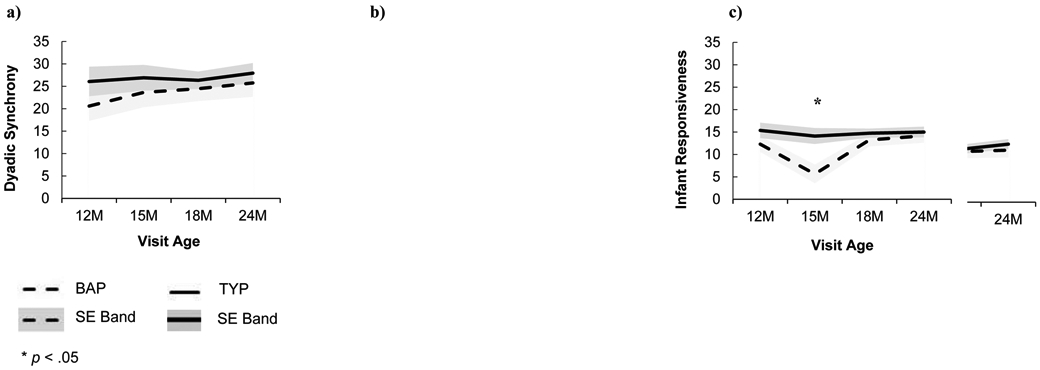
Table 4.
Linear model parameter estimates for the dyadic micro-analytic composites.
| Dyadic Synchrony |
Infant Responsiveness |
Mother Responsiveness |
||||
|---|---|---|---|---|---|---|
| Fixed Effects | Estimate (SE) | t | Estimate (SE) | t | Estimate (SE) | t |
| Group1 | −5.39(8.4) | −0.64 | −8.96(4.7) | −1.90 | −5.06(4.4) | −1.14 |
| Visit | 0.19(0.3) | 0.73 | 0.04(0.2) | 0.28 | 0.24(0.1) | 1.71* |
| Group x Visit | 0.17(0.4) | 0.40 | 0.35(0.2) | 1.42 | 0.18(0.2) | 0.78* |
| Infant Sex2 | −0.69(2.1) | −0.32 | −1.15(1.2) | −0.97 | −0.25(1.1) | −0.22 |
| Maternal Edu | 0.36(0.6) | 0.64 | 0.15(0.3) | 0.48 | 0.21(0.3) | 0.72 |
| Estimated Marginal Means3 | ||||||
| Group x 12M Visit | 4.57(4.9) | 0.93 | 2.73(2.68) | 1.02 | 1.99(2.6) | 0.78 |
| Group x 15M Visit | 2.23(4.6) | 0.49 | 7.78(2.5) | 3.13* | 5.09(2.4) | 2.14* |
| Group x 18M Visit | 1.40(4.0) | 0.35 | 1.08(2.2) | 0.50 | 0.02(2.1) | 0.01 |
| Group x 24M Visit | 1.72(3.6) | 0.63 | 0.59(2.0) | 0.76 | 1.05(1.9) | 0.58 |
Note:
Minus denotes BAP.
Minus denotes Female.
Separate models were specified for marginal means treating visit as a categorical variable to identify when differences emerged.
p values < .05
Figure 4. BAP and TYP group means and standard errors for the global ratings (a) total joint engagement, (b) supported joint engagement, (c) coordinated joint engagement, and (d) child responsiveness pattern.
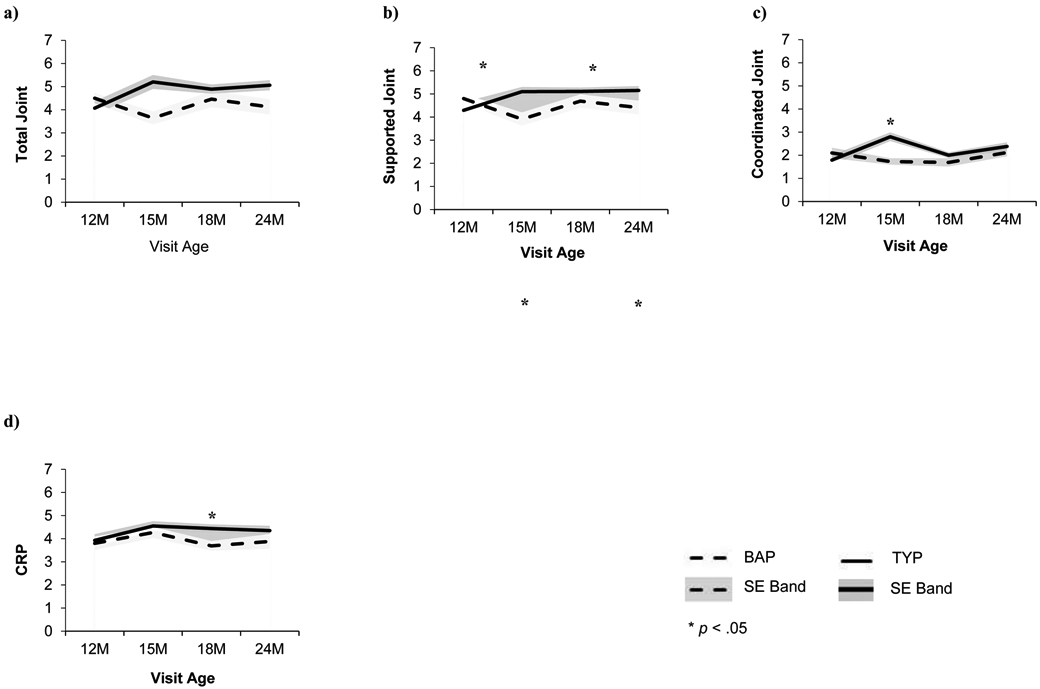
Table 5.
Linear model parameter estimates for the dyadic rating items.
| Total Joint Engagement |
Supported Joint Engagement |
Coordinate Joint Engagement |
Child Responsiveness Patterns |
|||||
|---|---|---|---|---|---|---|---|---|
| Fixed Effects | Estimate (SE) | t | Estimate (SE) | t | Estimate (SE) | t | Estimate (SE) | t |
| Group1 | 0.40(0.9) | 0.46 | 0.49(0.8) | 0.65 | −0.17(0.6) | −0.29 | −0.09(0.8) | −0.11 |
| Visit | 0.05(0.0) | 1.70 | 0.05(0.0) | 1.99* | 0.02(0.0) | 0.89 | 0.01(0.0) | 0.50 |
| Group x Visit | −0.05(0.1) | −1.18 | −0.05(0.0) | −1.37 | −0.00(0.0) | −0.06 | −0.02(0.0) | −0.51 |
| Infant Sex2 | −0.16(0.2) | −0.75 | 0.06(0.2) | 0.32 | −0.21(0.2) | −1.32 | −0.13(0.2) | −0.75 |
| Maternal Edu | 0.06(0.1) | 1.03 | 0.04(0.1) | 0.86 | 0.05(0.0) | 1.20 | −0.01(0.0) | −0.33 |
| Estimated Marginal Means3 | ||||||||
| Group x 12M Visit | −0.51(0.5) | −1.03 | −0.54(0.4) | −1.26 | −0.33(0.3) | −1.01 | 0.07(0.4) | 0.16 |
| Group x 15M Visit | 1.42(0.5) | 3.09* | 1.10(0.4) | 2.78* | 0.91(0.3) | 3.00* | 0.26(0.4) | 0.65 |
| Group x 18M Visit | 0.31(0.4) | 0.79 | 0.33(0.3) | 0.96 | 0.25(0.3) | 0.93 | 0.83(0.4) | 2.35* |
| Group x 24M Visit | 0.86(0.4) | 2.38* | 0.70(0.3) | 2.26* | 0.17(0.2) | 0.70 | 0.49(0.3) | 1.53 |
Note:
Minus denotes BAP.
Minus denotes Female.
Separate models were specified for marginal means treating visit as a categorical variable to identify when differences emerged.
p values < .05
Aim 2 Post-hoc Analyses
To aid in our interpretation of the results a series of post-hoc analyses were conducted. First, given the distinct 15 month differences in our dyadic measures, a series of ANOVA’s were conducted to examine if within group differences in the BAP group at 15 months were distinct. Children in the BAP group at 15 months (n = 11) did not differ from the larger BAP group with respect to infant sex, maternal age, maternal education, ADOS-2 severity scores, nonverbal DQs, or verbal DQs (all ps > .05).
Additionally, multilevel models with splines at 15 months were conducted to further examine the slopes from 15 to 24 months of age, recognizing the descriptive differences in the majority of the dyadic variables occurred at 15 months. Spline models included fixed effects for group membership, visit (centered at 12 months), splines set at 15 months, the interaction between group and visit, the interaction between group and visit with spline at 15 months, and two covariates: infant sex and years of maternal education. No significant effects for these models were observed for the micro-analytic composites but several notable patterns emerged for the joint engagement ratings:
Developmental growth was apparent for TJE, SJE, and CJE. From 12 to 24 months, more growth was observed overall; however, with the spline at 15 months, less growth was observed from 15 to 24 months for TJE, SJE, and CJE (Table 6). When including group membership, the BAP group demonstrated less overall growth from 12 to 24 months of age, and from 15 to 24 months of age the TYP group demonstrated significantly more growth compared to BAP.
Table 6.
Parameter estimates for the dyadic rating spline models.
| Total Joint Engagement |
Supported Joint Engagement |
Coordinate Joint Engagement |
Child Responsiveness Patterns |
|||||
|---|---|---|---|---|---|---|---|---|
| Fixed Effects | Estimate (SE) | t | Estimate (SE) | t | Estimate (SE) | t | Estimate (SE) | t |
| Group1 | 0.51(0.5) | 1.02 | 0.58(0.4) | 1.25 | 0.36(0.3) | 1.05 | −0.09(0.4) | −0.20 |
| Visit | 0.31(0.1) | 2.52* | 0.25(0.1) | 2.42* | 0.18(0.1) | 2.29* | 0.22(0.1) | 2.02* |
| Spline | −0.31(0.1) | −2.19* | −0.24(.1) | −2.03* | −0.20(0.1) | −2.15* | −0.24(0.1) | −1.91 |
| Group x Visit | −0.48(0.2) | −2.41* | −0.45(0.2) | −2.65* | −0.32(0.1) | −2.45* | −0.13(0.2) | −0.77 |
| Group x Spline | 0.51(0.2) | 2.18* | 0.47(0.2) | 2.39* | 0.37(0.2) | 2.49* | 0.13(0.2) | 0.63 |
| Infant Sex2 | −0.14(0.2) | −0.66 | 0.08(0.2) | 0.40 | −0.20(0.2) | −1.28 | −0.10(0.2) | −0.55 |
| Maternal Edu | 0.05(0.1) | 0.87 | 0.03(0.1) | 0.70 | 0.04(0.0) | 1.03 | −0.02(0.1) | −0.37 |
Note: Splines were specified at 15 months to examine the developmental patterns between TYP and BAP groups from 15 to 24 months of age.
Minus denotes BAP.
Minus denotes Female.
p values < .05
DISCUSSION
The present study aimed to examine if children exhibiting the BAP are distinguishable from their typically developing peers, to inform current early developmental monitoring and intervention efforts. On select measures, the present study identified significant social/dyadic differences within the first two years for children exhibiting elements of the BAP (when compared to their typically developing peers). Though the present study did not find robust differences for each proposed measure, Figures 2 and 3 illustrate a consistent pattern for the BAP group to perform lower than the TYP group by 15 months of age on social indices.
Our results add to a growing literature base on the social development of children with the BAP. For example, Yirmiya et al. (2006) examined social constructs in high-risk infant siblings loosely characterized with the BAP and identified instances of social difficulty (e.g., more neutral affect; fewer higher-order behavioral requests; less infant-led synchrony); however, the majority of their measures did not identify significant group differences (e.g., joint attention bids; child responsiveness). Whereas, Sullivan et al. (2007) found significant differences for their BAP group on select joint attention indices (i.e., “look-only”) at 14 months. The inconsistency in identifying significant differences across studies highlights the complexity of capturing elements of the BAP in early childhood.
To address social/dyadic complexity, the present study included two distinct behavioral coding techniques (i.e., micro-analytic and global ratings) to examine social difficulties that may be present in the BAP. As speculated in Yirmiya and Ozonoff (2007), BAP demonstrated relatively similar core competencies as indexed by the micro-analytic results in the current study, whereas the global ratings better captured dyadic differences between BAP and TYP. This may reflect that a micro-analytic approach is not as informative as global ratings; however, disentangling the intricate dance at a minute level, may be especially salient when determining treatment effects, as it best represents the process for dyadic exchanges (e.g., child initiations, Green et al., 2017).
In addition, understanding social difficulties associated with BAP in early childhood may identify mechanisms that inform later developmental outcomes. For example, in typical development, early joint attention skills predict later language and cognitive development (Mundy et al., 2007; Kristen et al., 2011). And in families raising children with an ASD, copious research highlights difficulties in core social competencies (e.g., eye contact) that inform difficulties in more complex social interactions (e.g., joint engagement, theory of mind), which further inform developmental functioning in later childhood (Granat et al., 2016; Poon et al., 2012; Siller & Sigman, 2002). However, few studies to date have examined the BAP beyond early childhood, and to our knowledge have only reported on observed difficulties on standardized measures. For example, in high-risk infant siblings with non-ASD developmental concerns in early childhood (e.g., language delays, BAP, global developmental delays), school age concerns have been documented (e.g., language development, clinical concerns, social cognition, executive functioning; Gamliel et al., 2009; Miller et al., 2016; Shephard et al., 2016; Warren et al., 2011). Specific to BAP outcomes, Gamliel et al. (2009) followed children from 4 months to 7 years and identified significant group differences in language trajectories between BAP and TYP groups - on average the BAP group’s receptive, expressive, and total language scores were lower than the TYP group from 14 to 54 months. In addition, Shephard et al. (2016) conducted a follow-up visit of infant siblings at 7 years of age and found significant group differences between their loosely defined BAP group (i.e., HR-Non-ASD) and TYP group, with lower adaptive functioning and evidence of restricted and repetitive behaviors as indexed by the ADOS in the BAP group. The school-age difficulties faced by children with the BAP parallels those highlighted by early joint attention deficits/difficulties.
In sum, the present study moves the field forward by longitudinally examining dyadic social constructs in the BAP. By examining BAP and TYP group differences across four time points, the current study demonstrated that distinct patterns exist between BAP and TYP groups, such that the BAP group performs lower across standardized measures and select dyadic constructs, as early as 15 months. In addition, recognizing traditional associations between early social difficulties and later developmental psychopathologies within the larger ASD literature base, the current study highlights the importance of continuing to investigate the BAP in early childhood. It is also important to consider the practical implications of characterizing subclinical populations, like the BAP. At its core, ASD encompasses social difficulties with known cascading developmental effects if left untreated. Though elements of social difficulties may be observed in the BAP, it is important for us to limit creating unnecessary distress on families by overpathologizing symptoms, while also advocating for opportunities that may promote optimal development (e.g., elevated-risk interventions).
Limitations
These data provide preliminary support for examining BAP as a separate outcome category in elevated-risk research. However, these results are not without limitations. In most prospective infant sibling designs, robust sample sizes across outcome classifications are difficult to achieve. In the current study, 22 children were identified as exhibiting the BAP; however, at any given visit, data were only available for a subset of children in the BAP group (e.g., n = 11) due to various reasons (e.g., no visit, child distress, equipment malfunction). In addition, a more rigorous test of the clinically meaningful differences in dyadic exchanges observed for children with BAP would be to include a subset of children diagnosed with ASD; however, only six children received an ASD diagnosis in the current study, with a max of four of these children having valid data at a given visit age.
Implications for Future Research
The relatively small number of individuals with ASD and BAP within this study is a common problem in research, which can limit analytic approaches and generalizability. Recent considerations to account for small sample sizes and unbalanced groups include Bayesian approaches (as discussed in van de Schoot et al., 2014), as well as increased sampling opportunities (e.g., Burst designs; Stawski et al., 2015). However, trajectory information, as presented in the current study, particularly with rich dyadic or social indices can expand our understanding of development as it unfolds in quasi-quantitative ways. Documenting distinct trajectory differences in these social behaviors can provide clinicians, interventionists, and parents with a social marker of risk and an intervention target. With increasing interest in the feasibility and efficacy of early social communication interventions for infants at elevated risk for an ASD (e.g., Green et al., 2017; Jones et al., 2017; Rogers et al., 2014; see review Landa, 2018), the current study provides support for targeting joint engagement and child/infant responsiveness. Additionally, within this study, 15 months proved to be a trajectory diverging point and with replication can inform intervention timing and when socially-based risk assessments may be most fruitful.
Supplementary Material
Acknowledgements:
We would like to thank the families who participated in the study for their time and commitment to this early developmental monitoring project. We would also like to thank the research assistants of the Developmental Studies Laboratory for their hard work and contributions. The authors are grateful to Dr. Sally Ozonoff for her mentorship and design support for the larger project in which these data are embedded.
REFERENCES
- Adamson LB, Bakeman R, Deckner DF, & Nelson BP (2014). From interactions to conversations: The development of joint engagement during early childhood. Child Development, 85, 941–955. doi: 10.1111/cdev.12189 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Adamson LB, Bakeman R, Deckner DF, & Nelson PB (2012). Rating parent-child interactions: Joint engagement, communication dynamics, and shared topics in autism, Down syndrome, and typical development. Journal of Autism and Developmental Disorders, 42, 2622–2635. doi: 10.1007/s10803-012-1520-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baron-Cohen S, Wheelwright S, Skinner R, Martin J, & Clubley E (2001). The autism-spectrum quotient (AQ): Evidence from Asperger syndrome/high-functioning autism, males and females, scientists and mathematicians. Journal of Autism and Developmental Disorders, 31, 5–17. doi: 10.1023/A:1005653411471 [DOI] [PubMed] [Google Scholar]
- Benjamini Y, & Hochberg Y (1995). Controlling the false discovery rate: A practical and powerful approach to multiple testing. Journal of the Royal Statistical Society. Series B Methodological, 57, 289–300. doi: 10.2307/2346101 [DOI] [Google Scholar]
- Campbell SB, Leezenbaum NB, Mahoney AS, Day TN, & Schmidt EN (2015). Social engagement with parents in 11-month-old siblings at high and low genetic risk for autism spectrum disorder. Autism, 19, 915–924. doi: 10.1177/1362361314555146 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chawaska K, Shic F, Macari S, Campbell DJ, Brian J, Landa R, et al. (2014). 18-month predictors of later outcomes in younger siblings of children with autism spectrum disorder: A baby siblings research consortium study. Journal of the American Academy of Child & Adolescent Psychiatry, 53, 1317–1327. doi: 10.1016/j.jaac.2014.09.015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cicchetti D (2014). Illustrative developmental psychopathology perspectives on precursors and pathways to personality disorder: Commentary on the special issue. Journal of Personality Disorders, 28, 172–179. doi: 10.1521/pedi.2014.28.1.172 [DOI] [PubMed] [Google Scholar]
- Clifford SM, Hudry K, Elsabbagh M, Charman T, Johnson MH, & the BASIS Team. (2013). Temperament in the first 2 years of life in infants at high-risk for autism spectrum disorders. Journal of Autism and Developmental Disorders, 43, 673–686. doi: 10.1007/s10803-012-1612-y [DOI] [PubMed] [Google Scholar]
- Constantino JN (2002). The Social Responsiveness Scale. Los Angeles: Western Psychological Services. [Google Scholar]
- Constantino JN, Zhang Y, Frazier T, Abbacchi AM, & Law P (2010). Sibling recurrence and the genetic epidemiology of autism. American Journal of Psychiatry, 167, 1349–1356. doi: 10.1176/appi.ajp.2010.09101470 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cornew L, Dobkins KR, Akshoomoff N, McCleery JP, & Carver LJ (2012). Atypical social referencing in infant siblings of children with autism spectrum disorders. Journal of Autism and Developmental Disorders, 42, 2611–2621. doi: 10.1007/s10803-0121518-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Feldman R (2007). Parent-infant synchrony and the construction of shared timing: Physiological precursors, developmental outcomes, and risk conditions. Journal of Child Psychology and Psychiatry, 48, 329–354. doi: 10.1111/j.1469-7610.2006.01701.x [DOI] [PubMed] [Google Scholar]
- Freeman S & Kasari C (2013). Parent-child interactions in autism: Characteristics of play. Autism, 17, 147–161. doi: 10.1177/1362361312469269 [DOI] [PubMed] [Google Scholar]
- Gamliel I, Yirmiya N, Jaffe DH, Manor O, & Sigman M (2009). Developmental trajectories in siblings of children with autism: cognition and language from 4 months to 7 years. Journal of Autism and Developmental Disorders, 39, 1131–1144. doi: 10.1007/s10803-009-0727-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Georgiades S, Szatmari P, Zwaigenbaum L, Bryson S, Brian J, Roberts W, et al. (2013). A prospective study of autistic-like traits in unaffected siblings of probands with autism spectrum disorder. Journal of the American Medical Association Psychiatry, 70, 42–48. doi: 10.1001/2013.jamapsychiatry.1 [DOI] [PubMed] [Google Scholar]
- Granat A, Gadassi R, Gilboa-Schechtman E, & Feldman R (2017). Maternal depression and anxiety, social synchrony, and infant regulation of negative and positive emotions. Emotion, 17, 11–27. doi: 10.1037/emo0000204 [DOI] [PubMed] [Google Scholar]
- Green J, Pickles A, Pasco G, Bedford R, Wan MW, Elsabbagh M, et al. (2017). Randomised trial of a parent-mediated intervention for infants at high risk for autism: Longitudinal outcomes to age 3 years. Journal of Child Psychology and Psychiatry, 58, 1330–1340. doi: 10.1111/jcpp.12728 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hurley RSE, Losh M, Parlier M, Reznick JS, & Piven J (2007). The broad autism phenotype questionnaire. Journal of Autism and Developmental Disorders, 37, 1679–1690. doi: 10.1007/s10803-006-0299-3 [DOI] [PubMed] [Google Scholar]
- Jones EJH, Dawson G, Kelly J, Estes A, & Jane Webb S (2017). Parent-delivered early intervention in infants at risk for ASD: Effects on electrophysiological and habituation measures of social attention. Autism Research: Official Journal of the International Society for Autism Research, 10, 961–972. doi: 10.1002/aur.1754 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kristen S, Sodian B, Thoermer C, & Perst H (2011). Infants' joint attention skills predict toddlers' emerging mental state language. Developmental Psychology, 47, 1207–1219.doi: 10.1037/a0024808 [DOI] [PubMed] [Google Scholar]
- Klusek J, Losh M, & Martin GE (2014). Sex differences and within-family associations in the broader autism phenotype. Autism, 18, 106–116. doi: 10.1177/1362361312464529 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lambert-Brown BL, McDonald NM, Mattson WI, Martin KB, Ibañez LV, Stone WL, et al. (2015). Positive emotional engagement and autism risk. Developmental Psychology, 51, 848–855. doi: 10.1037/a0039182 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Landa R (2018). Efficacy of early interventions for infants and young children with, and at risk for, autism spectrum disorders. International Review of Psychiatry, 30, 25–39. doi: 10.1080/09540261.2018.1432574 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Landa R, Gross AL, Stuart EA, & Bauman M (2012). Latent class analysis of early developmental trajectory in baby siblings of children with autism. Journal of Child Psychology and Psychiatry, 53, 986–996. doi: 10.1111/j.1469-7610.2012.02558.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Landry O, & Chouinard PA (2016). Why we should study the broader autism phenotype in typically developing populations. Journal of Cognition and Development, 17, 584–595. doi: 10.1080/15248372.2016.1200046 [DOI] [Google Scholar]
- Leezenbaum NB, Campbell SB, Butler D, & Iverson JM (2014). Maternal verbal responses to communication of infants at low and heightened risk of autism. Autism, 18, 694–703. doi: 10.1177/1362361313491327 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lord C, Risi S, Lambrecht L, Cook EH, Leventhal BL, & DiLavore PC (2000). The Autism Diagnostic Observation Schedule—Generic: A standard measure of social and communication deficits associated with the spectrum of autism. Journal of Autism and Developmental Disorders, 30, 205–223. doi: 10.1023/A:1005592401947 [DOI] [PubMed] [Google Scholar]
- Maxwell CR, Parish-Morris J, Hsin O, Bush JC, & Schultz RT (2013). The broad autism phenotype predicts child functioning in autism spectrum disorders. Journal of Neurodevelopmental Disorder, 5, 25–32. doi: 10.1186/1866-1955-5-25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Messinger D, Young GS, Ozonoff S, Dobkins K, Carter A, Zwaigenbaum L, et al. (2013). Beyond autism: A baby siblings research consortium study of high-risk children at three years of age. Journal of the American Academy of Child & Adolescent Psychiatry, 52, 300–308. doi: 10.1016/j.jaac.2012.12.011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller M, Iosif AM, Young GS, Hill M, Hanzel EP, Hutman T, et al. (2016). School-age outcomes of infants at risk for autism spectrum disorder. Autism Research, 9, 632–642. doi: 10.1002/aur.1572 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mullen EM (1995). Mullen scales of early learning (AGS ed.), Circle Pines, MN: American Guidance Service. [Google Scholar]
- Mundy P, Block J, Delgado C Pomares Y, Van Hecke AV, & Parlade MV (2007). Individual differences and the development of joint attention in infancy. Child Development, 78, 938–954. doi: 10.1111/j.1467-8624.2007.01042.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ozonoff S, Iosif AM, Baguio F, Cook IC, Hill MM, Hutman T, et al. (2010). A prospective study of the emergence of early behavioral signs of autism. Journal of the American Academy of Child Adolescent Psychiatry, 49, 256–266.doi: 10.1016/j.jaac.2009.11.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ozonoff S, Young GS, Belding A, Hill M, Hill A, Hutman T, et al. (2014). The broader autism phenotype in infancy: When does it emerge? Journal of the American Academy of Child & Adolescent Psychiatry, 53, 398–407.doi: 10.1016/j.jaac.2013.12.020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pisula E, & Ziegart-Sadowska K (2015). Broader autism phenotype in siblings of children with ASD: A review. International Journal of Molecular Science, 16, 13217–13258. doi: 10.3390/ijms160613217 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Poon KK, Watson LR, Baranek GT, & Poe MD (2012). To what extent do joint attention, imitation, and object play behaviors in infancy predict later communication and intellectual functioning in ASD? Journal of Autism and Developmental Disorders, 42, 1064–1074. doi: 10.1007/s10803-011-1349-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rogers SJ, Vismara L, Wagner AL, McCormick C, Young G, & Ozonoff S (2014). Autism treatment in the first year of life: A pilot study of infant start, a parent-implemented intervention for symptomatic infants. Journal of Autism and Developmental Disorders, 44, 2981–2995. doi: 10.1007/s10803-014-2202-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rozga A, Hutman T, Young GS, Rogers SJ, Ozonoff S, Dapretto M, et al. (2011). Behavioral profiles of affected and unaffected siblings of children with autism: Contribution of measures of mother-infant interaction and nonverbal communication. Journal of Autism and Developmental Disorders, 41, 287–301. doi: 10.1007/s10803-010-1051-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ruzich E, Allison C, Smith P, Watson P, Auyeung B, Ring H, & Baron-Cohen S (2015). Subgrouping siblings of people with autism: Identifying the broader autism phenotype. Autism Research, 9, 658–665. doi: 10.1002/aur.1544 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sasson NJ, Lam KSL, Childress D, Parlier M, Daniels JL, & Piven J (2014). The broad autism phenotype questionnaire: Prevalence and diagnostic classification. Autism Research, 6, 134–143. doi: 10.1002/aur.1272 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shephard E, Milosavljevic B, Pasco G, Jones EJH, Gliga T, Happe F, et al. (2016). Mid-childhood outcomes of infant siblings at familial high-risk of autism spectrum disorder. Autism Research, 10, 546–557. doi: 10.1002/aur.1733 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Siller M & Sigman M (2002). The behaviors of parents of children with autism predict the subsequent development of their children’s communication. Journal of Autism and Developmental Disorders, 32, 77–89. doi: 10.1023/A:1014884404276 [DOI] [PubMed] [Google Scholar]
- Sparrow SS, Balla DA, & Cicchetti DV (1984). Vineland Adaptive Behavior Scales. Minneapolis, MN: American Guidance. [Google Scholar]
- Stawski RS, MacDonald SWS, & Sliwinski MJ (2015). Measurement burst design. The Encyclopedia of Adulthood and Aging, 2, 854–859. doi: 10.1002/9781118521373.wbeaa313 [DOI] [Google Scholar]
- Sullivan M, Finelli J, Marvin A, Garrett-Mayer E, Bauman M, & Landa R (2007). Response to joint attention in toddlers at risk for autism spectrum disorder: A prospective study. Journal of Autism and Developmental Disorders, 37, 37–48. doi: 10.1007/s10803-006-0335-3 [DOI] [PubMed] [Google Scholar]
- Swanson MR, Serlin GC, & Siller M (2013). Broad autism phenotype in typically developing children predicts performance on an eye-tracking measure of joint attention. Journal of Autism and Developmental Disorders, 43, 707–718. doi: 10.1007/s10803-012-1616-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- van de Schoot R, Kaplan D, Denissen J, Asendorpf JB, Neyer FJ, & van Aken MAG (2013). A gentle introduction to Bayesian analysis: Applications to developmental research. Child Development, 85, 842–860. doi: 10.1111/cdev.12169 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wan MW, Green J, Elsabbagh M, Johnson M, Charman T, & Plummer F (2012). Parent-infant interaction in infant siblings at risk of autism. Research in Developmental Disabilities, 33, 924–932. doi: 10.1016/j.ridd.2011.12.011 [DOI] [PubMed] [Google Scholar]
- Wan MW, Green J, Elsabbagh M, Johnson M, Charman T, Plummer F (2013). Quality of interaction between at-risk infants and caregiver at 12-15 months is associated with 3-year autism outcome. Journal of Child Psychology and Psychiatry, 54, 763–771. doi: 10.1111/jcpp.12032 [DOI] [PubMed] [Google Scholar]
- Warlaumont AS, Richards JA, Gikerson J, & Oller DK (2014). A social feedback loop for speech development and its reduction in autism. Psychological Science, 25, 1314–1324. doi: 10.1177/0956797614531023 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Warren ZE, Foss-Feig JH, Malesa EE, Lee EB, Taylor JL, Newsom CR, et al. (2011). Neurocognitive and behavioral outcomes of younger siblings of children with autism spectrum disorder at age five. Journal of Autism and Developmental Disorders, 42, 409–418. doi: 10.1007/s10803-011-1263-4 [DOI] [PubMed] [Google Scholar]
- Wheelwright S, Auyeung B, Allison C, & Baron-Cohen S (2010). Defining the broader, medium, and narrow phenotype among parents using the Autism Spectrum Quotient (AQ). Molecular Autism, 1:10. doi: 10.1186/2040-2392-1-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yirmiya N, Gamliel I, Pilowsky T, Feldman R, Baron-Cohen S, & Sigman M (2006). The development of siblings of children with autism at 4 and 14 months: Social engagement, communication, and cognition. Journal of Child Psychology and Psychiatry, 47, 511–523. doi: 10.1111/j.1469-7610.2005.01528.x [DOI] [PubMed] [Google Scholar]
- Yirmiya N, & Ozonoff S (2007). The very early autism phenotype. Journal of Autism and Developmental Disorders, 37, 1–11. doi: 10.1007/s10803-006-0329-1 [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.