

Significance Statement
Healthy lifestyle behaviors reduce death and cardiovascular disease among individuals with preserved kidney function, but the benefits of these behaviors among those with reduced kidney function, a group at higher risk for cardiovascular disease, have not been established. In this pooled analysis of three community-based cohort studies that included 27,271 adults, healthy lifestyle behaviors (not smoking, maintaining body mass index in the recommended range, engaging in regular physical activity, consuming a healthy diet, and no more than a moderate intake of alcohol), analyzed individually and in combination, were associated with significantly reduced risk of death and cardiovascular disease events among individuals with or without reduced kidney function. These findings highlight the importance of lifestyle behaviors as potentially modifiable risk factors for people with kidney disease.
Keywords: cardiovascular disease, chronic kidney disease, chronic renal failure, mortality risk, heart failure, health behaviors, lifestyle
Visual Abstract

Abstract
Background
Adherence to healthy behaviors reduces risks of cardiovascular disease and death in the general population. However, among people with kidney disease, a group at higher risk for cardiovascular disease, such benefits have not been established.
Methods
We pooled data from three cohort studies with a total of 27,271 participants. Kidney function was categorized on the basis of eGFR (≥60, 45 to <60, and <45 ml/min per 1.73 m2). We used proportional hazard frailty models to estimate associations between healthy behaviors (not smoking, at recommended body mass index [BMI], physical activity, healthy diet, and moderate to no alcohol intake) and outcomes (all-cause death, major coronary events, ischemic stroke, and heart failure events).
Results
All recommended lifestyle behaviors were significantly associated with lower risks of death, regardless of eGFR. Not smoking (versus current) and any moderate to vigorous physical activity (versus none) was significantly associated with reduced risks of major coronary and heart failure events, regardless of eGFR. Any (versus no) moderate or vigorous physical activity significantly associated with decreased risk of ischemic stroke events only among those with eGFR ≥60. Moderate to no daily alcohol intake (versus excessive) was significantly associated with an increased risk of major coronary events, regardless of eGFR. For heart failure events, a BMI of 18.5 to 30 associated with decreased risk, regardless of eGFR. Across all eGFR categories, the magnitude of risk reduction for death and all cardiovascular outcomes increased with greater numbers of recommended lifestyle behaviors.
Conclusions
Recommended lifestyle behaviors are associated with lower risk of death and cardiovascular disease events among individuals with or without reduced kidney function, supporting lifestyle behaviors as potentially modifiable risk factors for people with kidney disease.
Cardiovascular disease is the leading cause of death in the United States.1 In epidemiologic studies, lifestyle behaviors that are generally regarded as healthy have been shown to strongly influence the risks of cardiovascular disease, independent of traditional risk factors and medications.2–15 However, many of these studies excluded groups at high risk for cardiovascular disease events, such as those with kidney disease.
Adults with kidney disease, estimated to be 15% of the US population, have a ten-fold higher risk of cardiovascular disease compared with the general population.16,17 Analyses of the effect of healthy lifestyle behaviors on preventing cardiovascular disease and death among individuals with kidney disease have not shown consistent results.18–22 Because the effect of healthy lifestyle behaviors among individuals with kidney disease is unclear, recommendations for lifestyle behaviors in kidney disease clinical practice guidelines are based largely on general population studies.23
This study aimed to determine the association of lifestyle behaviors, with the risk of all-cause death and cardiovascular events, including a composite of coronary events, ischemic stroke, and heart failure (HF) among adults with and without reduced kidney function. Due to a higher prevalence and differences in pathophysiology of vascular disease among those with kidney disease compared with the general population, we hypothesized that recommended lifestyle behaviors would have less benefit on all outcomes, and particularly on cardiovascular outcomes, among individuals with reduced kidney function, compared with those with preserved kidney function. We used a pooled dataset created from three community-based prospective cohort studies to evaluate the separate and joint associations of lifestyle behaviors with all-cause death and cardiovascular disease events among individuals with different levels of kidney function.
Methods
Data Sources
We obtained public-use datasets through the National Heart, Lung, and Blood Institute (NHLBI) Biologic Specimen and Data Repository Information Coordinating Center (BioLINCC) for three US cohort studies of cardiovascular disease risk factors: the Atherosclerosis Risk in Communities Study (ARIC), the Cardiovascular Health Study (CHS), and the Multi-Ethnic Study of Atherosclerosis (MESA). ARIC enrolled 15,792 participants aged 45–64 years from four communities (Jackson, Mississippi; Forsyth County, North Carolina; Minneapolis, Minnesota; and Washington County, Maryland) from 1987 to 1989. CHS enrolled 5201 participants aged 65 years and older between 1989 and 1990 from four communities (Sacramento, California; Washington County, Maryland; Forsyth County, North Carolina; and Pittsburgh, Pennsylvania), then purposely recruited 687 Black patients between 1992 and 1993 from three (excluding Washington County) of the four communities. MESA enrolled 6814 participants 45–84 years of age from six field centers from 2000 and 2002 (Baltimore, MD; Chicago, IL; Forsyth County, NC; Los Angeles, CA; New York, NY; St Paul, MN). We used follow-up data until 2017 for ARIC and MESA, and 2009 for the CHS that were available through BioLINCC. Participants provided informed consent before cohort enrollment.24–29 This study was deemed exempt by the University of Pennsylvania Institutional Review Board.
Study Sample
Our sample of 27,271 was generated by including cohort members with a serum creatinine measurement at baseline and excluding 181 individuals with a body mass index (BMI) <18.5 kg/m2 because eGFR categorization is challenging in this group because of low muscle mass. We included those with cardiovascular disease at baseline to maximize generalizability. To estimate the GFR, we utilized the CKD Epidemiology Collaboration equation,30 then each participant was grouped into one of three eGFR categories (≥60, 45 to <60, and <45 ml/min per 1.73 m2; hereafter referred to as: ≥60, 45 to <60, and <45, respectively) that corresponded to preserved, mild-to-moderately decreased, or moderate-to-severely decreased kidney function in accordance with the Kidney Disease Improving Global Outcomes classification system.31
Baseline Variables
Baseline data collection methods have been described.24–27,29,32–39 For our analyses, diabetes was defined by self-report, use of glucose-lowering agents, or fasting blood glucose ≥126 mg/dl. Hypertension was determined by self-report, measured systolic BP (SBP) >140 mm Hg, or use of antihypertensive medications. Cardiovascular disease at baseline was defined as a history of HF, myocardial infarction (MI), coronary revascularization, stroke, transient ischemic attack, or claudication. In all three studies, BP was recorded as an average of two readings after resting in a seated position.
Measures of Lifestyle Behaviors
We evaluated five lifestyle behaviors on the basis of prior literature demonstrating associations with the risk of cardiovascular disease or all-cause death: smoking, BMI (as an indicator of healthy weight maintenance), physical activity, alcohol intake, and dietary habits.4,9,12,14,40–42 Smoking status was self-reported. BMI (kg/m2) was calculated from measured height and weight. Weekly moderate-to-vigorous physical activity was estimated on the basis of self-reported frequency and duration of activities32–35 that corresponded to ≥3 metabolic equivalents.43 Dietary composition was determined from food frequency questionnaires.36–39 A diet score (0–5) was constructed by assigning one point for each component recommended by the American Heart Association (AHA): fruits and vegetables (≥4.5 cups or servings/d), fish (≥3.5 oz or ≥2 servings/wk), whole grains (≥3 1 oz servings/d), sodium (<1500 mg/d), and sugar-sweetened beverages (≤36 oz/wk or ≤4 glasses/wk).44 Self-reported alcohol intake was classified as none or moderate (≤28 g/d, or ≤2 standard alcoholic drinks, for men and ≤14 g/d, or ≤1 standard alcoholic drink, for women) or excessive (>28 g/d for men, >14 g/d for women) on the basis of national guidelines.45 Each lifestyle behavior was dichotomized as “recommended” versus “not recommended” on the basis of prior literature, including the AHA Life’s Simple 7 three categories of cardiovascular health (ideal, intermediate, and poor): BMI (18.5 to <30 versus ≥30 kg/m2), weekly moderate to vigorous physical activity (any versus none), diet score (≥2 versus 0–1), smoking status (never/former versus current), and daily alcohol intake (none/moderate versus excessive).4,9,12,13,40–42,46,47 The AHA intermediate and ideal categories were combined to define recommended because our primary analyses included those with a history of cardiovascular disease, and by definition, individuals with prevalent cardiovascular disease can, at best, achieve intermediate cardiovascular health. The AHA poor category defined not recommended behaviors. The dichotomization using ideal/intermediate versus poor, compared with ideal versus intermediate/poor AHA categories has been shown to have consistent associations with clinical outcomes.7
A lifestyle behavior score ranging from 0 (least healthy) to 5 (healthiest) was generated as the sum of recommended lifestyle behaviors. Because only 0.2%, 2.3%, and 12.9% of participants had lifestyle behavior score of 0, 1, and 2, respectively, we collapsed the lower three categories into a category named “0–2”.
Follow-Up and Outcomes
Each cohort ascertained death and cardiovascular events during follow-up.26,48–51 All of the studies had medical adjudication committees and standardized diagnoses (which were similar between studies) on the basis of medical records (see Supplemental Methods for further details). Our study outcomes included all-cause death and the initial occurrence after cohort entry of each of the following: a composite of major coronary events (definite or probable MI, definite fatal coronary heart disease, or revascularization procedure including coronary angioplasty or other revascularization procedure), ischemic stroke, and HF events. Participants were followed from baseline to death, loss to follow-up, or end of cohort follow-up, whichever occurred first.
Statistical Analyses
Comparisons of baseline characteristics across eGFR groups were made using chi-squared tests, ANOVA, or Kruskal-Wallis tests, as appropriate. Proportional hazards regression models were used to estimate the relationship of dichotomous lifestyle behaviors with each outcome, with the not recommended behavior serving as the reference group. To account for the study-to-study heterogeneity that may be caused by differences in the cohort studies’ patient populations or methods of data collection, frailty models were used for the time to event analyses.52 Frailty models treat the study as a random effect instead of fixed. The frailty term is an unobservable random variable that corresponds to each individual’s underlying modification to the baseline hazard function to account for unobserved heterogeneity.53 For all-cause death, adjusted Cox models were used. In the presence of competing events (i.e., death unrelated to major coronary events, ischemic stroke, and HF events), cause-specific hazards models were generated treating the competing events as censored. Proportional hazards models were also used to estimate the association of the lifestyle behavior score as a categorical variable with each outcome, with a lifestyle behavior category of 0–2 serving as the reference group. The proportional hazards frailty models were adjusted for age, sex, race/ethnicity, education, baseline cardiovascular disease, hypertension, diabetes, BMI, eGFR, SBP, and diastolic BP, and a cohort study was included as a random effect. Proportionality assumptions were visually examined with Schoenfeld residuals. Kaplan-Meier curves with log-rank testing were assessed for equality of survival distributions for all-cause death between lifestyle behavior score and eGFR groups. Fine and Gray’s competing risk regression models and Gray’s tests assessed the equality of cumulative event probabilities for the composite of major coronary events, ischemic stroke, and HF events. Effect modification was tested using interaction terms of lifestyle behaviors and eGFR categories (≥60, 45 to <60, and <45 ml/min per 1.732).
Missingness for covariates ranged from 0% to 0.2%, For lifestyle behaviors, the missingness was 0.2% for smoking, 2.2% for alcohol, 4.4% for diet score, and 2.4% for physical activity. Multiple imputation was performed for any missing lifestyle behavior variables (n=1265) with the following variables: sex, BMI, age, race, education, SBP, diastolic BP, baseline eGFR, diabetes, hypertension, history of cardiovascular disease, medications (ACE inhibitor, statins, aspirin, betablockers), and total cholesterol.54 Final models are on the basis of the imputed results. In sensitivity analyses, we modeled the individual lifestyle behavior regression analyses for diet and BMI as continuous variables, assessed the relationships of potassium and sodium intake with outcomes of interest, and repeated the lifestyle behavior score regression analyses excluding those with cardiovascular disease at baseline. Analyses were performed using STATA, version 16 (Stata Corp, College Station, TX). All P values were two tailed (α=0.05).
Results
Baseline characteristics of the study population are shown in Table 1. There were 16,347 participants with eGFR ≥60, 8257 participants with eGFR 45 to <60, and 2667 participants with eGFR <45. Participants with eGFR <45 were older and had less education, higher SBP, and more diabetes, cardiovascular disease, and hypertension. Healthy diet scores were more frequent among those with an eGFR 45 to <60. Moderate to vigorous physical activity, BMI ≥30 kg/m2, current smoking, and excessive alcohol use were more common among those with eGFR ≥60.
Table 1.
Baseline demographics, clinical characteristics, and lifestyle behaviors by eGFR category (n=27,271)
| Baseline Characteristics | All (n=27,271) | eGFR ≥60 (n=16,347) | eGFR 45 to <60 (n=8257) | eGFR <45 (n=2667) | P Valuea |
|---|---|---|---|---|---|
| Cohort study, n (%) | <0.001 | ||||
| Multiethnic study of atherosclerosis | 6740 (24.7) | 5861 (35.9) | 726 (8.8) | 153 (5.7) | |
| Cardiovascular health study | 14,833 (54.4) | 7806 (47.8) | 5817 (70.5) | 1210 (45.4) | |
| Atherosclerosis risk in communities study | 5698 (20.9) | 2680 (16.4) | 1714 (20.8) | 1304 (48.9) | |
| Demographics | |||||
| Age, mean (SD), yr | 60.1 (10.2) | 58.8 (9.8) | 60.3 (9.8) | 66.9 (10.8) | <0.001 |
| Male, % | 45.4 | 46.1 | 43.7 | 46.4 | 0.001 |
| Race, % | <0.001 | ||||
| White | 67.8 | 59.6 | 80.1 | 80.1 | |
| Black | 23.8 | 28 | 17.5 | 17.6 | |
| Hispanic | 5.5 | 8.2 | 1.4 | 1.2 | |
| Other | 3.0 | 4.3 | 1.1 | 1.1 | |
| Education, % | <0.001 | ||||
| Less than high school | 23.3 | 22.6 | 22.6 | 30.4 | |
| High school/some college | 44.4 | 44.2 | 44.7 | 44.0 | |
| 4 yr degree or more | 32.3 | 33.2 | 32.7 | 25.7 | |
| Clinical characteristics | |||||
| Systolic BP, mean (SD), mm Hg | 137 (20) | 135 (20) | 140 (19) | 142 (22) | <0.001 |
| Diastolic BP, mean (SD), mm Hg | 84 (16) | 82 (15) | 87 (15) | 81 (17) | <0.001 |
| eGFR, mean (SD), ml/min per 1.73 m2 | 66.1 (18.3) | 77.2 (14.1) | 53.6 (4.3) | 36.7 (8.0) | <0.001 |
| Total cholesterol, mean (SD), mg/dL | 208.9 (41) | 205.5 (40) | 213.9 (40.9) | 214.6 (44) | <0.001 |
| Diabetes, % | 13.9 | 13.9 | 11.5 | 20.8 | <0.001 |
| Cardiovascular diseaseb, % | 14.4 | 10.6 | 17.0 | 30.0 | <0.001 |
| Hypertension, % | 44.7 | 41.3 | 44.1 | 67.6 | <0.001 |
| HF, % | 3.1 | 2.2 | 4.0 | 5.9 | <0.001 |
| Ace-inhibitor use, % | 6.5 | 6.7 | 5.2 | 8.8 | <0.001 |
| Betablocker use, % | 10.5 | 9.7 | 10.6 | 15.0 | <0.001 |
| Statin use, % | 4.5 | 5.6 | 2.8 | 3.0 | <0.001 |
| Aspirin use, % | 37.6 | 33.8 | 43.7 | 42.4 | <0.001 |
| BMI, mean (SD), kg/m2 | 27.7 | 27.8 (5.3) | 27.5 (4.8) | 27.6 (18.8) | 0.01 |
| Sodium intake, mg/d, median (IQR) | 1641 (1175–2381) | 1654 (1185–2390) | 1565 (1129–2179) | 1923 (1312–2965) | <0.001 |
| Potassium intake, mg/d, median (IQR) | 2321 (1720–3047) | 2353 (1735–3085) | 2326 (1741–3033) | 2103 (1562–2829) | <0.001 |
| Lifestyle behaviors, % | |||||
| BMI | <0.001 | ||||
| ≥30 kg/m2 | 27.2 | 28.1 | 25.6 | 26.2 | |
| 18.5 to <30 kg/m2 | 72.8 | 71.9 | 74.5 | 73.8 | |
| Moderate-vigorous physical activity | <0.001 | ||||
| 0 min/wk | 48.5 | 46.7 | 51.2 | 51.3 | |
| ≥1 min/wk | 51.5 | 53.3 | 48.8 | 48.8 | |
| Diet score (range 0–5)c | <0.001 | ||||
| 0–1 | 39.6 | 41.7 | 35.8 | 38.6 | |
| ≥2 | 60.4 | 58.3 | 64.2 | 61.4 | |
| Smoking status | <0.001 | ||||
| Current | 19.9 | 21.7 | 17.9 | 14.4 | |
| Never/former | 80.1 | 78.3 | 82.1 | 85.6 | |
| Daily alcohol intake | <0.001 | ||||
| Excessived | 8.6 | 9.2 | 8.1 | 6.1 | |
| None/moderate | 91.4 | 90.8 | 91.9 | 93.9 | |
| Lifestyle Behavior Scoree | <0.001 | ||||
| 0–2 | 15.3 | 16.3 | 14.1 | 13.2 | |
| 3 | 29.6 | 30.3 | 28.5 | 28.9 | |
| 4 | 35.8 | 34.9 | 37.0 | 37.6 | |
| 5 | 19.3 | 18.6 | 20.4 | 20.4 | |
IQR, interquartile range.
X2 test of difference across eGFR categories.
Any cardiovascular disease: history of HF, MI, coronary revascularization, stroke, transient ischemic attack, or claudication.
Defined as sum of each AHA-recommended dietary component: fruits and vegetables (≥4.5 cups or servings/d), fish (≥3.5 oz or ≥2 servings/wk), whole grains (≥3 1 oz servings/d), sodium (<1500 mg/d), and sugar-sweetened beverages (≤36 oz/wk or ≤4 glasses/wk).
Excessive: >28 g/d, or >2 standard drinks, for men and >14 g/d, or >1 standard drink, for women.
Defined as sum of each healthy lifestyle behavior criterion met: BMI (18.5 to <30 kg/m2 [1 point] versus ≥30 [0 points]), physical activity (any weekly moderate to vigorous physical activity [1 point] versus no moderate to vigorous physical activity (0 points)], diet score [≥2 (1 point) versus 0–1 (0 points)], smoking status (never/former [1 point] versus current [0 points], and daily alcohol intake (no to moderate [1 point] versus excessive [0 points]).
Individual Lifestyle Behaviors and Outcomes
As shown in Table 2, during a median follow-up of 16.7 years (interquartile range, 8.6–22.7), there were 5238 composite major coronary events (1.3 in 100 person-years), 1985 ischemic strokes (0.5 in 100 person-years), 4473 HF events (1.2 in 100 person-years), and 9776 deaths from all-causes (2.3 in 100 person-years).
Table 2.
Outcome events and event rate (per yr) overall and by eGFR category
| Outcome Events | Overall | eGFR ≥60 | eGFR 45 to <60 | eGFR <45 |
|---|---|---|---|---|
| All-cause death | ||||
| Total all-cause deaths, n | 9756 | 4784 | 3264 | 1708 |
| Death rate (per 100 person-yr), median (IQR) | 2.36 (2.31–2.41) | 2.02 (1.97–2.08) | 2.29 (2.21–2.37) | 4.99 (4.76–5.23) |
| Noncoronary heart disease deaths, n | 7962 | 3993 | 2657 | 1312 |
| Noncoronary heart disease death rate (per 100 person-yr), median (IQR) | 1.93 (1.88–1.97) | 1.69 (1.64–1.74) | 1.86 (1.79–1.93) | 3.83 (3.63–4.05) |
| Composite of major coronary eventsa | ||||
| Total events, n | 5238 | 2584 | 1827 | 827 |
| Event rate (per 100 person-yr), median (IQR) | 1.34 (1.30–1.37) | 1.15 (1.10–1.19) | 1.36 (1.30–1.43) | 2.52 (2.36–2.70) |
| Incident MI events | 2802 | 1381 | 994 | 427 |
| Incident MI rate (per 100 person-yr), median (IQR) | 0.69 (0.67–0.72) | 0.60 (0.57–0.63) | 0.72 (0.67–0.76) | 1.26 (1.14–1.38) |
| Fatal coronary heart disease events, n | 1794 | 791 | 607 | 396 |
| Fatal coronary heart disease event rate (per 100 person-yr), median (IQR) | 0.43 (0.41–0.45) | 0.33 (0.31–0.36) | 0.43 (0.39–0.46) | 1.16 (1.05–1.28) |
| Revascularization procedures, n | 2582 | 1377 | 940 | 265 |
| Procedure event rate (per 100 person-yr), median (IQR) | 0.64 (0.62–0.67) | 0.60 (0.57–0.63) | 0.69 (0.64–0.73) | 0.79 (0.69–0.88) |
| Ischemic stroke | ||||
| Total ischemic strokes, n | 1985 | 986 | 682 | 317 |
| Ischemic stroke event rate (per 100 person-yr), median (IQR) | 0.48 (0.46–0.50) | 0.42 (0.39–0.45) | 0.48 (0.45–0.52) | 0.92 (0.82–1.03) |
| Heart failure | ||||
| Total heart failure events, n | 4473 | 2168 | 1520 | 785 |
| Heart failure event rate (per 100 person-yr), median (IQR) | 1.16 (1.12–1.19) | 0.97 (0.93–1.01) | 1.15 (1.09–1.21) | 2.49 (2.32–2.67) |
Definite or probable myocardial infarction, definite fatal coronary heart disease, and revascularization procedure including coronary angioplasty or other revascularization procedure.
All of the recommended lifestyle behaviors were associated with reduced all-cause death, regardless of eGFR (Figure 1A, Table 3). Former/never (versus current) smoking and any (versus no) moderate to vigorous weekly physical activity were associated with a protective effect of major coronary events (adjusted hazard ratio [aHR] 0.62; 95% confidence interval [95% CI], 0.57 to 0.66 and aHR, 0.85; 95% CI, 0.80 to 0.90, respectively) and HF events (aHR, 0.48; 95% CI, 0.45 to 0.52 and aHR, 0.84; 95% CI, 0.79 to 0.90, respectively) regardless of eGFR (Figure 1B, Table 3). None/moderate (versus excessive) daily alcohol intake was associated with an increased risk of major coronary events (aHR, 1.29; 95% CI, 1.16 to 1.44). Any (versus no) moderate to vigorous physical activity was associated with decreased risk of ischemic stroke events only among those with eGFR ≥60 (aHR, 0.80; 95% CI, 0.70 to 0.92; P value for interaction by eGFR group = 0.001) (Figure 1C, Table 3). For HF events, a BMI of 18.5 to <30 (versus ≥30) kg/m2 was associated with decreased risk events regardless of eGFR (aHR, 0.87; 95% CI, 0.78 to 0.97) (Figure 1D, Table 3).
Figure 1.
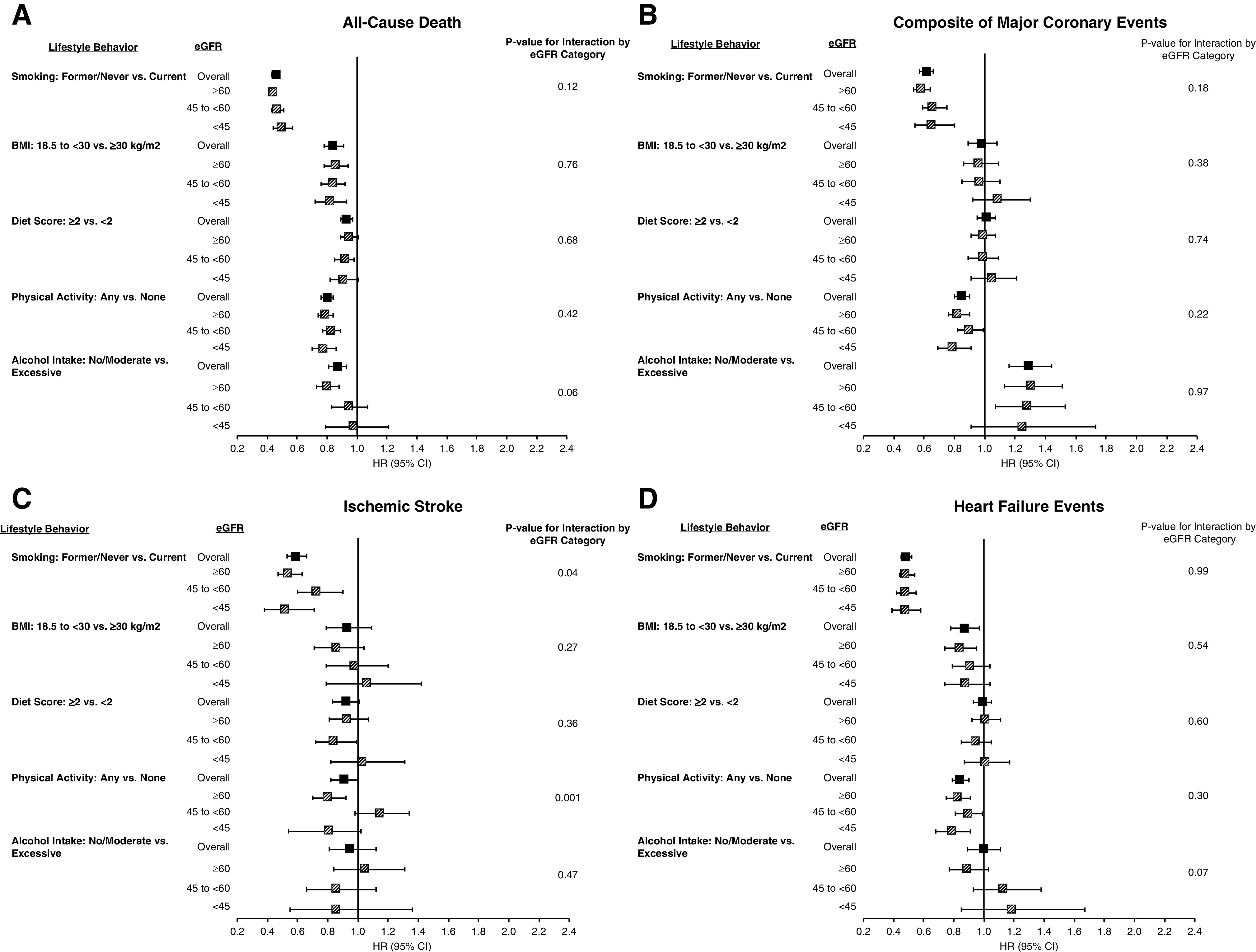
Risk of adverse outcomes according to individual lifestyle behaviors. (A) All-cause death, (B) composite of major coronary events, (C) ischemic stroke, and (D) HF events. Plots show HR and error bars indicate 95% CI.
Table 3.
Association of individual lifestyle behaviors with all-cause death, major coronary events, ischemic stroke, and HF
| Individual Lifestyle Behaviors | All eGFR Categories | P Value for Interaction by eGFR Category | |
|---|---|---|---|
| HR (95% CI) | P value | ||
| All-cause death | |||
| Smoking status | 0.12 | ||
| Current | Ref | ||
| Former/Never | 0.46 (0.43 to 0.48) | <0.0001 | |
| BMI | 0.76 | ||
| ≥30 kg/m2 | Ref | ||
| 18.5–<30 kg/m2 | 0.84 (0.78 to 0.91) | <0.0001 | |
| Diet score | 0.68 | ||
| 0–1 | Ref | ||
| ≥2 | 0.93 (0.89 to 0.97) | 0.001 | |
| Physical activity | 0.42 | ||
| 0 min/wk | Ref | ||
| ≥1 min/wk | 0.80 (0.76 to 0.84) | <0.0001 | |
| Daily alcohol intake | 0.06 | ||
| Excessivea | Ref | ||
| None/moderate | 0.87 (0.81 to 0.93) | <0.0001 | |
| Major coronary events | |||
| Smoking statusb | 0.18 | ||
| Current | Ref | ||
| Former/Never | 0.62 (0.57 to 0.66) | <0.0001 | |
| BMIc | 0.38 | ||
| ≥30 kg/m2 | Ref | ||
| 18.5–<30 kg/m2 | 0.98 (0.89 to 1.08) | 0.74 | |
| Diet scoreb | 0.74 | ||
| 0–1 | Ref | ||
| ≥2 | 1.01 (0.95 to 1.07) | 0.86 | |
| Physical activityd | 0.22 | ||
| 0 min/wk | Ref | ||
| ≥1 min/wk | 0.85 (0.80 to 0.90) | <0.0001 | |
| Daily alcohol intakeb | 0.97 | ||
| Excessivea | Ref | ||
| None/moderate | 1.29 (1.16 to 1.44) | <0.0001 | |
| Ischemic stroke | |||
| Smoking status | 0.04 | ||
| Current | Ref | ||
| Former/never | 0.59 (0.53 to 0.66) | <0.0001 | |
| BMI | 0.27 | ||
| ≥30 kg/m2 | Ref | ||
| 18.5 to <30 kg/m2 | 0.93 (0.79 to 1.09) | 0.37 | |
| Diet score | 0.36 | ||
| 0–1 | Ref | ||
| ≥2 | 0.92 (0.83 to 1.01) | 0.08 | |
| Physical activity | 0.001 | ||
| 0 min/wk | Ref | ||
| ≥1 min/wk | 0.91 (0.82 to 1.00) | 0.06 | |
| Daily alcohol intake | 0.47 | ||
| Excessivea | Ref | ||
| None/moderate | 0.95 (0.81 to 1.12) | 0.57 | |
| Heart failure | |||
| Smoking status | 0.99 | ||
| Current | Ref | ||
| Former/never | 0.48 (0.45 to 0.52) | <0.001 | |
| BMI | 0.54 | ||
| ≥30 kg/m2 | Ref | ||
| 18.5 to <30 kg/m2 | 0.87 (0.78 to 0.97) | 0.006 | |
| Diet score | 0.60 | ||
| 0–1 | Ref | ||
| ≥2 | 0.99 (0.93 to 1.05) | 0.77 | |
| Physical activity | 0.30 | ||
| 0 min/wk | Ref | ||
| ≥1 min/wk | 0.84 (0.79 to 0.90) | <0.001 | |
| Daily alcohol intake | 0.07 | ||
| Excessivea | Ref | ||
| None/moderate | 1.00 (0.89 to 1.11) | 0.11 | |
Models adjusted for age, race, sex, education, baseline eGFR, hypertension, BMI, SBP, diastolic BP, history of diabetes, history of cardiovascular disease, aspirin use, ACE-inhibitor use, betablocker use, statin use, total cholesterol, eGFR category, and original cohort as a random effect.
Excessive: >28 g/d, or >2 standard drinks, for men and >14 g/d, or >1 standard drink, for women.
Adjustment did not include history of cardiovascular disease or hypertension due to numerical infeasibility.
Adjustment did not include history of cardiovascular disease or total cholesterol due to numerical infeasibility.
Adjustment did not include history of cardiovascular disease due to numerical infeasibility.
In sensitivity analyses, an increase in BMI was associated with increased risk of major coronary and HF events regardless of eGFR category. An increase in diet score was associated with decreased risk of all-cause death and major coronary events regardless of kidney function (Supplemental Table 1). An increase in dietary sodium intake was associated with increased risk of all-cause death and increased potassium intake was associated with a decreased risk of stroke, but increased risk of HF events across eGFR groups (Supplemental Table 1).
Lifestyle Behavior Score and Outcomes
The frequencies of lifestyle behavior score are reported in Table 1. For each eGFR group, those with higher lifestyle behavior scores had better survival (Supplemental Figure 1; log-rank test, P<0.001) and lower incidence of cardiovascular disease events (Supplemental Figures 2–4; Gray’s tests P<0.001). Lifestyle behavior score categories of 3, 4, and 5 (versus 0–2) were each associated with dose-related lower risks of all-cause death, major coronary events, ischemic strokes, and HF events, regardless of kidney function (Figure 2, A–D, Table 4).
Figure 2.
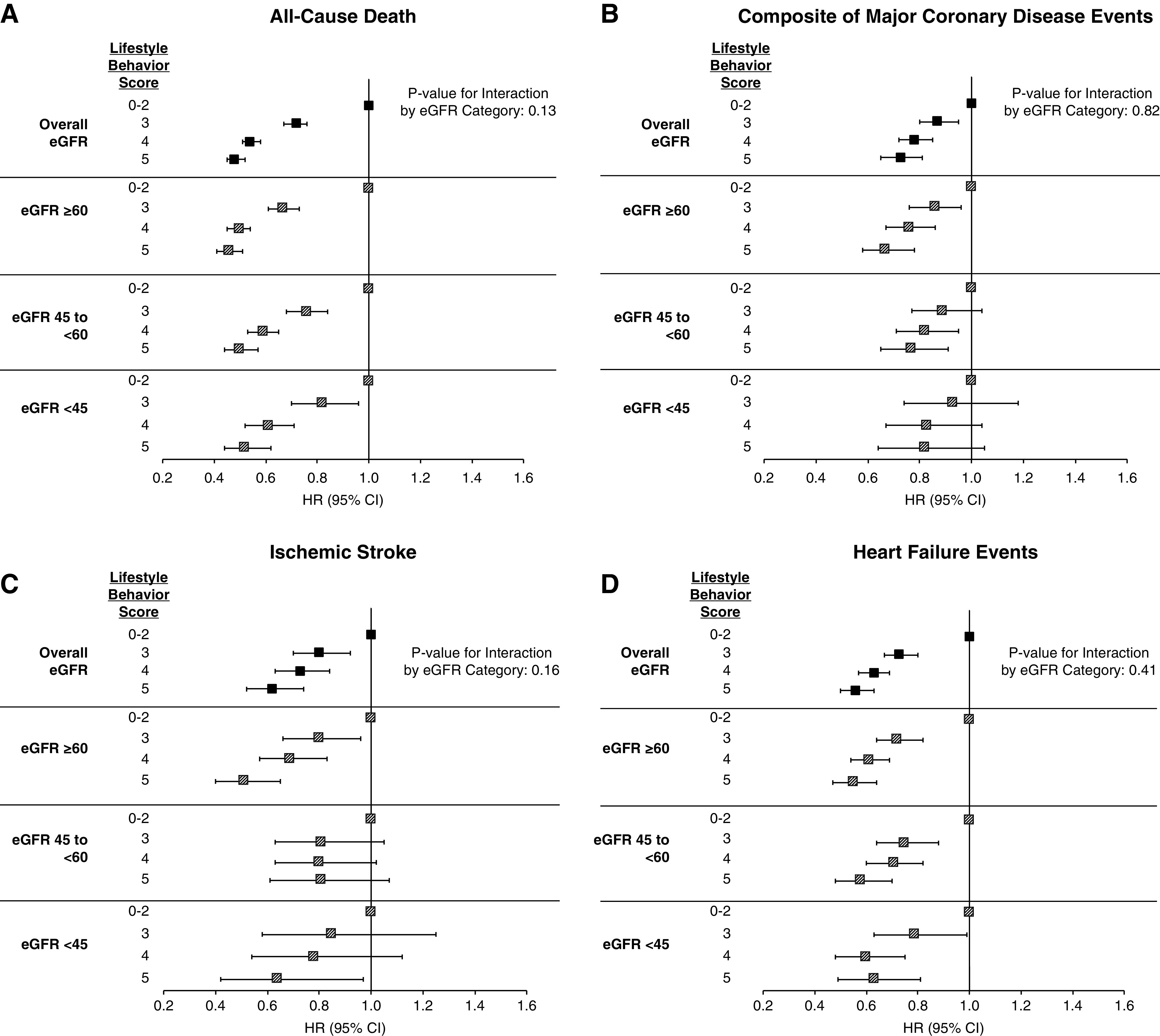
Risk of adverse outcomes according to combined lifestyle behavior score. (A) All-cause death, (B) composite of major coronary events, (C) ischemic stroke, and (D) HF events. Plots show HR and error bars indicate 95% CI.
Table 4.
Association of composite lifestyle behavior score with all-cause death, major coronary events, ischemic stroke, and HF
| Lifestyle Behavior Score | All eGFR Categories | P Value for Interaction by eGFR Category | |
|---|---|---|---|
| HR (95% CI) | P value | ||
| All-cause death | |||
| 0–2 | Ref | 0.13 | |
| 3 | 0.72 (0.67 to 0.76) | <0.0001 | |
| 4 | 0.54 (0.51 to 0.58) | <0.0001 | |
| 5 | 0.48 (0.45 to 0.52) | <0.0001 | |
| Major coronary eventsa | |||
| 0–2 | Ref | 0.82 | |
| 3 | 0.87 (0.80 to 0.95) | 0.002 | |
| 4 | 0.78 (0.72 to 0.85) | <0.001 | |
| 5 | 0.73 (0.65 to 0.81) | <0.001 | |
| Ischemic stroke | |||
| 0–2 | Ref | 0.16 | |
| 3 | 0.80 (0.70 to 0.92) | 0.002 | |
| 4 | 0.73 (0.63 to 0.84) | <0.0001 | |
| 5 | 0.62 (0.52 to 0.74) | <0.0001 | |
| Heart failure | |||
| 0–2 | Ref | 0.41 | |
| 3 | 0.73 (0.67 to 0.80) | <0.0001 | |
| 4 | 0.63 (0.57 to 0.69) | <0.0001 | |
| 5 | 0.56 (0.50 to 0.63) | <0.0001 | |
Models adjusted for age, race, sex, education, baseline eGFR, hypertension, BMI, SBP, diastolic BP, history of diabetes, history of cardiovascular disease, aspirin use, ACE-inhibitor use, betablocker use, statin use, total cholesterol, eGFR category, and original cohort as a random effect.
Adjustment did not include history of cardiovascular disease and hypertension due to numerical infeasibility.
When eGFR was analyzed as a continuous variable (per ml/min per 1.73 m2), interactions were evident between smoking and all-cause death (β coefficient −0.005; 95% CI, −0.008 to −0.003) and major cardiovascular events (β coefficient −0.005; 95% CI, −0.009 to −0.001), and between daily alcohol intake and all-cause death (β coefficient −0.008; 95% CI, −0.011 to −0.004) and HF events (β coefficient −0.008; 95% CI, −0.001 to −0.002) (Supplemental Table 2). The magnitude of protection associated with not smoking (compared with current smoking) or associated with no or moderate alcohol intake (compared with excessive intake) was greater among individuals with a higher baseline eGFR value. Results of sensitivity analyses excluding participants with baseline cardiovascular disease history were qualitatively similar to results of the primary analyses (Supplemental Table 3).
Discussion
In this study of individuals with a broad range of kidney function, we found that recommended lifestyle behaviors, analyzed individually and in combination, were associated with reduced risk of death and cardiovascular disease events. For all-cause death, each of the five recommended lifestyle behaviors was protective, and there was a strong graded lower risk as the number of recommended lifestyle behaviors increased. With the exception of nonsmoking and physical activity, relationships of individual recommended lifestyle behaviors were less evident for cardiovascular disease outcomes than for death, regardless of kidney function. When considered in combination, adherence to a greater number of recommended behaviors was clearly associated with reduced risk of death and cardiovascular disease events, regardless of kidney function.
Although most individuals with kidney disease die from cardiovascular disease,16,55 evidence is limited regarding optimal management and prevention of cardiovascular disease in this population. Kidney disease is often an exclusion criterion for cardiovascular outcomes trials, and recommendations for lifestyle behaviors included in kidney disease clinical practice guidelines are based largely on studies in the general population. The relevance of these recommendations to people with kidney disease who have both higher risk and different underlying pathophysiology of cardiovascular disease has not been established.16,17,56
We expected that healthy behaviors would have less of an effect on the risk of death and cardiovascular events among those with reduced, compared with preserved, kidney function, because of the higher prevalence, and greater severity of vascular disease among those with reduced kidney function.57,58 However, our study indicates the relative risk reductions associated with recommended behaviors are similar, regardless of the level of kidney function. Because the individuals with worse kidney function have a higher risk of death and cardiovascular events than those with preserved kidney function, the similar relative reductions in risk with healthy behaviors across eGFR categories translates into greater absolute reductions in outcome events for those with more severe kidney dysfunction than for those with more preserved kidney function.
The finding that recommended lifestyle behaviors are associated with better outcomes across levels of kidney function may reflect favorable effects of healthy behaviors on traditional cardiovascular disease risk factors, such as hypertension, obesity, insulin resistance, and hyperlipidemia, which are common to people with and without kidney disease.6 However, healthy behaviors may also counteract cardiovascular risk factors unique to kidney disease, such as albuminuria and mediators of inflammation and oxidative stress.59,60 Albuminuria, which has been linked to endothelial dysfunction and incident cardiovascular disease, can be reduced with dietary changes, such as moderate salt reduction.61 Physical activity may be particularly relevant for individuals with kidney disease because it lowers C-reactive protein levels in a dose-response manner,62 and potentially reduces frailty because physical activity has been associated with an increase in cardiovascular fitness and muscle strength.63 The effect of a healthy lifestyle on novel cardiovascular disease risk factors in kidney disease deserves further investigation.
We did not observe consistent associations between adherence to the AHA-recommended diet pattern and lower risk across all cardiovascular disease outcomes. In previous studies of cohorts that, for the most part, were without kidney disease, healthier diets were associated with lower risk of mortality and cardiovascular disease events.7,9 Our lack of finding an association with a recommended diet could be due to our use of a less-sensitive measure of a healthy diet, because we included the AHA intermediate and ideal categories to define a healthy diet (score ≥2), and several of the previous studies used an ideal category of the AHA-recommended diet (score >4). Additionally, for those with decreased kidney function, a diet rich in fruits and vegetables may result in hyperkalemia, and thereby possibly counteract beneficial effects of a “heart-healthy” diet. Additional research on effects of diet is needed among those with and without kidney disease.
Healthy lifestyle behaviors may be most effective when present in combination. Prior studies have demonstrated that, when analyzed at the per-person level, the number of healthy lifestyle behaviors has a strong graded inverse relationship with death,7,13 MI,64 cardiovascular mortality,7,8,10,13 stroke, and HF.65,66 However, most of these studies excluded individuals with a history of kidney disease. This study extends the investigation of potential protective effects of lifestyle behaviors to individuals with reduced kidney function, and found a similar graded inverse relationship of three or more recommended lifestyle behaviors with death and cardiovascular events regardless of kidney function.
This study further confirms that lifestyle behaviors should be viewed as major independent risk factors for poor health that require screening and treatment among all individuals, regardless of kidney function. In the past two decades, participation in healthy lifestyle behaviors has decreased,13 yet less than half of patients report being counseled about healthy behaviors during their most recent physician office visit.67,68 Further research is needed to understand how patients and providers prioritize these behaviors.
The results of our study need to be interpreted in the context of several limitations. First, the lifestyle behaviors are susceptible to measurement error due to self-report and possible inadequacies in data harmonization across studies. Second, the analyses incorporated measures of lifestyle behaviors only at baseline, and it is possible that behaviors changed over time. Third, dichotomizing the lifestyle behaviors with graded effects on risk would result in different interpretation of associations, compared with evaluating behaviors as continuous measures or by restricting to more extreme scores. Therefore, our findings likely underestimate the importance of each lifestyle behavior and their combined effects. Additional limitations include insufficient power to detect modest associations among the low kidney function group, and residual confounding and inability to establish causality due to the observational nature of the study.
Despite these limitations, our study has important strengths, including a large sample size, the use of data from three well-established cohorts, and inclusion of a substantial number of individuals with impaired kidney function. Additional strengths include rigorous assessments of lifestyle behaviors and outcomes that should minimize measurement error and misclassification, detailed data on important baseline risk factors to reduce confounding, and a diverse study population to increase generalizability.
In summary, healthy lifestyle behaviors were associated with lower risk of death and most of the cardiovascular disease outcomes, regardless of kidney function. Our findings extend previous demonstrations of protective effects of healthy lifestyle behaviors in the general population to those with kidney disease, a highly prevalent condition associated with markedly increased risks of cardiovascular disease morbidity and mortality. Our study supports the importance of lifestyle as a potentially modifiable risk factor for individuals with and without kidney disease.
Disclosures
A. Anderson reports personal fees from Kyowa Hakko Kirin, outside the submitted work. H. Feldman reports consultancy agreements with Kyowa Hakko Kirin Co, Ltd. (ongoing), National Kidney Foundation, InMed, Inc., and DLA Piper, LLP; reports receiving research funding from Regeneron; honoraria from Rogosin Institute (invited speaker); reports being a scientific advisor or member of the Steering Committee, Chronic Renal Insufficiency Cohort Study, Editor-in-Chief, and National Kidney Foundation (Member of Advisory Board). J. Hsu reports being a scientific advisor or member of AJKD as a Statistics/Epidemiology Editor and PLOS ONE as a Statistical Advisory Board member. L. Dember receives compensation from the National Kidney Foundation for her role as a Deputy Editor of the American Journal of Kidney Diseases; and reports consulting fees from Merck and GlaxoSmithKline.
Funding
This work was supported in part by National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) grant K23 DK118198-01A1 (to S. Schrauben). A. Anderson reports grants from National Institutes of Health/NIDDK, during the conduct of the study.
Supplementary Material
Acknowledgments
This manuscript was prepared using ARIC, CHS, and MESA research materials obtained from the NHLBI BioLINCC and does not necessarily reflect the opinions or views of ARIC, CHS, MESA, or the NHLBI.
S.J. Schrauben, L.M. Dember, and J.Y. Hsu designed the study; S.J. Schrauben and J.Y. Hsu analyzed the data; S.J. Schrauben, S. Amaral, J.Y. Hsu, A.H. Anderson, H.I. Feldman, and L.M. Dember drafted and revised the paper; and all authors approved the final version of the manuscript.
Footnotes
Published online ahead of print. Publication date available at www.jasn.org.
Supplemental Material
This article contains the following supplemental material online at http://jasn.asnjournals.org/lookup/suppl/doi:10.1681/ASN.2020040394/-/DCSupplemental.
Supplemental Methods. Ascertainment of outcome events.
Supplemental Figure 1. Kaplan-Meier curves for overall survival by eGFR category and Lifestyle Behavior Scores.
Supplemental Figure 2. Cumulative incidence functions for major coronary disease events across eGFR categories and Lifestyle Behavior Scores.
Supplemental Figure 3. Cumulative incidence functions for ischemic stroke events across eGFR categories and Lifestyle Behavior Scores.
Supplemental Figure 4. Cumulative incidence functions for HF events across eGFR categories and Lifestyle Behavior Scores.
Supplemental Table 1. Association of continuous measures of diet, BMI, sodium intake, and potassium intake with all-cause death, major coronary events, ischemic stroke, and HF by eGFR category.
Supplemental Table 2. Assessment of statistical interactions between lifestyle behaviors and clinical outcomes by continuous eGFR (centered).
Supplemental Table 3. Associations of Lifestyle Behavior Scores and all-cause death, major coronary events, ischemic stroke, and HF events by eGFR category among participants without a history of cardiovascular disease at baseline.
References
- 1.Mozaffarian D, Benjamin E, Go A, Arnett D, Blaha M, Cushman M, et al.: Executive summary: Heart disease and stroke statistics--2016 update: A report from the American heart association. Circulation 133: 447–454, 2016 [DOI] [PubMed] [Google Scholar]
- 2.Bibbins-Domingo K, Chertow GM, Coxson PG, Moran A, Lightwood JM, Pletcher MJ, et al.: Projected effect of dietary salt reductions on future cardiovascular disease. N Engl J Med 362: 590–599, 2010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Knowler WC, Barrett-Connor E, Fowler SE, Hamman RF, Lachin JM, Walker EA, et al.; Diabetes Prevention Program Research Group: Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med 346: 393–403, 2002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Stampfer MJ, Hu FB, Manson JE, Rimm EB, Willett WC: Primary prevention of coronary heart disease in women through diet and lifestyle. N Engl J Med 343: 16–22, 2000 [DOI] [PubMed] [Google Scholar]
- 5.Chiuve SE, McCullough ML, Sacks FM, Rimm EB: Healthy lifestyle factors in the primary prevention of coronary heart disease among men: Benefits among users and nonusers of lipid-lowering and antihypertensive medications. Circulation 114: 160–167, 2006 [DOI] [PubMed] [Google Scholar]
- 6.Mozaffarian D, Wilson PW, Kannel WB: Beyond established and novel risk factors: Lifestyle risk factors for cardiovascular disease. Circulation 117: 3031–3038, 2008 [DOI] [PubMed] [Google Scholar]
- 7.Ford ES, Greenlund KJ, Hong Y: Ideal cardiovascular health and mortality from all causes and diseases of the circulatory system among adults in the United States. Circulation 125: 987–995, 2012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Stamler J, Stamler R, Neaton JD, Wentworth D, Daviglus ML, Garside D, et al.: Low risk-factor profile and long-term cardiovascular and noncardiovascular mortality and life expectancy: Findings for 5 large cohorts of young adult and middle-aged men and women. JAMA 282: 2012–2018, 1999 [DOI] [PubMed] [Google Scholar]
- 9.van Dam RM, Li T, Spiegelman D, Franco OH, Hu FB: Combined impact of lifestyle factors on mortality: Prospective cohort study in US women. BMJ 337: a1440, 2008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Folsom AR, Yatsuya H, Nettleton JA, Lutsey PL, Cushman M, Rosamond WD; ARIC Study Investigators: Community prevalence of ideal cardiovascular health, by the American Heart Association definition, and relationship with cardiovascular disease incidence. J Am Coll Cardiol 57: 1690–1696, 2011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Ford ES, Zhao G, Tsai J, Li C: Low-risk lifestyle behaviors and all-cause mortality: Findings from the National Health and Nutrition Examination Survey III Mortality Study. Am J Public Health 101: 1922–1929, 2011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Knoops KT, de Groot LC, Kromhout D, Perrin AE, Moreiras-Varela O, Menotti A, et al.: Mediterranean diet, lifestyle factors, and 10-year mortality in elderly European men and women: The HALE project. JAMA 292: 1433–1439, 2004 [DOI] [PubMed] [Google Scholar]
- 13.Yang Q, Cogswell ME, Flanders WD, Hong Y, Zhang Z, Loustalot F, et al.: Trends in cardiovascular health metrics and associations with all-cause and CVD mortality among US adults. JAMA 307: 1273–1283, 2012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Akesson A, Weismayer C, Newby PK, Wolk A: Combined effect of low-risk dietary and lifestyle behaviors in primary prevention of myocardial infarction in women. Arch Intern Med 167: 2122–2127, 2007 [DOI] [PubMed] [Google Scholar]
- 15.Ford ES, Bergmann MM, Boeing H, Li C, Capewell S: Healthy lifestyle behaviors and all-cause mortality among adults in the United States. Prev Med 55: 23–27, 2012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY: Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med 351: 1296–1305, 2004 [DOI] [PubMed] [Google Scholar]
- 17.Sarnak MJ, Levey AS, Schoolwerth AC, Coresh J, Culleton B, Hamm LL, et al.; American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention: Kidney disease as a risk factor for development of cardiovascular disease: A statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Hypertension 42: 1050–1065, 2003 [DOI] [PubMed] [Google Scholar]
- 18.Muntner P, Judd SE, Gao L, Gutiérrez OM, Rizk DV, McClellan W, et al.: Cardiovascular risk factors in CKD associate with both ESRD and mortality. J Am Soc Nephrol 24: 1159–1165, 2013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Ricardo AC, Madero M, Yang W, Anderson C, Menezes M, Fischer MJ, et al.: Adherence to a healthy lifestyle and all-cause mortality in CKD. Clin J Am Soc Nephrol 8: 602–609, 2013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Ricardo AC, Anderson CA, Yang W, Zhang X, Fischer MJ, Dember LM, et al.; CRIC Study Investigators: Healthy lifestyle and risk of kidney disease progression, atherosclerotic events, and death in CKD: Findings from the Chronic Renal Insufficiency Cohort (CRIC) Study. Am J Kidney Dis 65: 412–424, 2015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Shlipak MG, Fried LF, Cushman M, Manolio TA, Peterson D, Stehman-Breen C, et al.: Cardiovascular mortality risk in chronic kidney disease: Comparison of traditional and novel risk factors. JAMA 293: 1737–1745, 2005 [DOI] [PubMed] [Google Scholar]
- 22.Beddhu S, Baird BC, Zitterkoph J, Neilson J, Greene T: Physical activity and mortality in chronic kidney disease (NHANES III). Clin J Am Soc Nephrol 4: 1901–1906, 2009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group: KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl 3: 1–150, 2013 [Google Scholar]
- 24.Fried LP, Borhani NO, Enright P, Furberg CD, Gardin JM, Kronmal RA, et al.: The cardiovascular health study: Design and rationale. Ann Epidemiol 1: 263–276, 1991 [DOI] [PubMed] [Google Scholar]
- 25.ARIC Investigators : Atherosclerosis Risk in Communities (ARIC) Study: Design and objectives. Am J Epidemiol 129: 687–702, 1989. [PubMed] [Google Scholar]
- 26.Bild DE, Bluemke DA, Burke GL, Detrano R, Diez Roux AV, Folsom AR, et al.: Multi-ethnic study of Atherosclerosis: Objectives and design. Am J Epidemiol 156: 871–881, 2002 [DOI] [PubMed] [Google Scholar]
- 27.Tell GS, Fried LP, Hermanson B, Manolio TA, Newman AB, Borhani NO: Recruitment of adults 65 years and older as participants in the Cardiovascular Health Study. Ann Epidemiol 3: 358–366, 1993 [DOI] [PubMed] [Google Scholar]
- 28.Psaty BM, Kuller LH, Bild D, Burke GL, Kittner SJ, Mittelmark M, et al.: Methods of assessing prevalent cardiovascular disease in the Cardiovascular Health Study. Ann Epidemiol 5: 270–277, 1995 [DOI] [PubMed] [Google Scholar]
- 29.Kumanyika SK, Tell GS, Shemanski L, Martel J, Chinchilli VM: Dietary assessment using a picture-sort approach. Am J Clin Nutr 65[Suppl]: 1123S–1129S, 1997 [DOI] [PubMed] [Google Scholar]
- 30.Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF 3rd, Feldman HI, et al.; CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration): A new equation to estimate glomerular filtration rate [published correction appears in Ann Intern Med 155: 408, 2011]. Ann Intern Med 150: 604–612, 2009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Levey AS, de Jong PE, Coresh J, Nahas MEI, Astor BC, Matsushita K, et al.: The definition, classification, and prognosis of chronic kidney disease: a KDIGO controversies conference report. Kidney Int 80: 17–28, 2011 [DOI] [PubMed] [Google Scholar]
- 32.Ainsworth BE, Irwin ML, Addy CL, Whitt MC, Stolarczyk LM: Moderate physical activity patterns of minority women: The Cross-Cultural Activity Participation Study. J Womens Health Gend Based Med 8: 805–813, 1999 [DOI] [PubMed] [Google Scholar]
- 33.Siscovick DS, Fried L, Mittlemark M, Rutan G, Bild D, O’Leary DH: Exercise intensity and subclinical cardiovascular disease in the elderly. The Cardiovascular Health Study. Am J Epidemiol 145: 977–986, 1997 [DOI] [PubMed] [Google Scholar]
- 34.McPhillips JB, Pellettera KM, Barrett-Connor E, Wingard DL, Criqui MH: Exercise patterns in a population of older adults. Am J Prev Med 5: 65–72, 1989 [PubMed] [Google Scholar]
- 35.Baecke JA, Burema J, Frijters JE: A short questionnaire for the measurement of habitual physical activity in epidemiological studies. Am J Clin Nutr 36: 936–942, 1982 [DOI] [PubMed] [Google Scholar]
- 36.Block G, Woods M, Potosky A, Clifford C: Validation of a self-administered diet history questionnaire using multiple diet records. J Clin Epidemiol 43: 1327–1335, 1990 [DOI] [PubMed] [Google Scholar]
- 37.Mayer-Davis EJ, Vitolins MZ, Carmichael SL, Hemphill S, Tsaroucha G, Rushing J, et al.: Validity and reproducibility of a food frequency interview in a Multi-Cultural Epidemiology Study. Ann Epidemiol 9: 314–324, 1999 [DOI] [PubMed] [Google Scholar]
- 38.Kumanyika S, Tell GS, Shemanski L, Polak J, Savage PJ: Eating patterns of community-dwelling older adults: The Cardiovascular Health Study. Ann Epidemiol 4: 404–415, 1994 [DOI] [PubMed] [Google Scholar]
- 39.Willett WC, Sampson L, Stampfer MJ, Rosner B, Bain C, Witschi J, et al.: Reproducibility and validity of a semiquantitative food frequency questionnaire. Am J Epidemiol 122: 51–65, 1985 [DOI] [PubMed] [Google Scholar]
- 40.Liu K, Daviglus ML, Loria CM, Colangelo LA, Spring B, Moller AC, et al.: Healthy lifestyle through young adulthood and the presence of low cardiovascular disease risk profile in middle age: The Coronary Artery Risk Development in (Young) Adults (CARDIA) study. Circulation 125: 996–1004, 2012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Djoussé L, Driver JA, Gaziano JM: Relation between modifiable lifestyle factors and lifetime risk of heart failure. JAMA 302: 394–400, 2009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Mozaffarian D, Kamineni A, Carnethon M, Djoussé L, Mukamal KJ, Siscovick D: Lifestyle risk factors and new-onset diabetes mellitus in older adults: The cardiovascular health study. Arch Intern Med 169: 798–807, 2009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Ainsworth BE, Haskell WL, Whitt MC, Irwin ML, Swartz AM, Strath SJ, et al.: Compendium of physical activities: An update of activity codes and MET intensities. Med Sci Sports Exerc 32[Suppl]: S498–S504, 2000 [DOI] [PubMed] [Google Scholar]
- 44.Lloyd-Jones DM, Hong Y, Labarthe D, Mozaffarian D, Appel LJ, Van Horn L, et al.; American Heart Association Strategic Planning Task Force and Statistics Committee: Defining and setting national goals for cardiovascular health promotion and disease reduction: The American Heart Association’s strategic Impact Goal through 2020 and beyond. Circulation 121: 586–613, 2010 [DOI] [PubMed] [Google Scholar]
- 45.U.S. Department of Health and Human Services and U.S. Department of Agriculture : 2015-2020 Dietary Guidelines for Americans. 8th Edition. 2015. Available at: https://health.gov/our-work/food-nutrition/previous-dietary-guidelines/2015
- 46.Wändell PE, Carlsson AC, Theobald H: The association between BMI value and long-term mortality. Int J Obes 33: 577–582, 2009 [DOI] [PubMed] [Google Scholar]
- 47.Piercy KL, Troiano RP, Ballard RM, Carlson SA, Fulton JE, Galuska DA, et al.: The physical activity guidelines for Americans. JAMA 320: 2020–2028, 2018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Ives DG, Fitzpatrick AL, Bild DE, Psaty BM, Kuller LH, Crowley PM, et al.: Surveillance and ascertainment of cardiovascular events. The Cardiovascular Health Study. Ann Epidemiol 5: 278–285, 1995 [DOI] [PubMed] [Google Scholar]
- 49.White AD, Folsom AR, Chambless LE, Sharret AR, Yang K, Conwill D, et al.: Community surveillance of coronary heart disease in the Atherosclerosis Risk in Communities (ARIC) Study: Methods and initial two years’ experience. J Clin Epidemiol 49: 223–233, 1996 [DOI] [PubMed] [Google Scholar]
- 50.Loehr LR, Rosamond WD, Chang PP, Folsom AR, Chambless LE: Heart failure incidence and survival (from the Atherosclerosis Risk in Communities study). Am J Cardiol 101: 1016–1022, 2008 [DOI] [PubMed] [Google Scholar]
- 51.Rosamond WD, Folsom AR, Chambless LE, Wang CH, McGovern PG, Howard G, et al.: Stroke incidence and survival among middle-aged adults: 9-year follow-up of the Atherosclerosis Risk in Communities (ARIC) cohort. Stroke 30: 736–743, 1999 [DOI] [PubMed] [Google Scholar]
- 52.Ha ID, Sylvester R, Legrand C, Mackenzie G: Frailty modelling for survival data from multi-centre clinical trials. Stat Med 30: 2144–2159, 2011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Therneau T, Grambsch P: Modeling Survival Data: Extending the Cox Model. Statistics for Biology and Health, New York, NY, Springer, 2000 [Google Scholar]
- 54.Klebanoff MA, Cole SR: Use of multiple imputation in the epidemiologic literature. Am J Epidemiol 168: 355–357, 2008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Keith DS, Nichols GA, Gullion CM, Brown JB, Smith DH: Longitudinal follow-up and outcomes among a population with chronic kidney disease in a large managed care organization. Arch Intern Med 164: 659–663, 2004 [DOI] [PubMed] [Google Scholar]
- 56.Weiner DE, Tabatabai S, Tighiouart H, Elsayed E, Bansal N, Griffith J, et al.: Cardiovascular outcomes and all-cause mortality: Exploring the interaction between CKD and cardiovascular disease. Am J Kidney Dis 48: 392–401, 2006 [DOI] [PubMed] [Google Scholar]
- 57.Arroyo D, Betriu A, Martinez-Alonso M, Vidal T, Valdivielso JM, Fernández E; investigators from the NEFRONA study: Observational multicenter study to evaluate the prevalence and prognosis of subclinical atheromatosis in a Spanish chronic kidney disease cohort: Baseline data from the NEFRONA study. BMC Nephrol 15: 168, 2014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Mathew RO, Bangalore S, Lavelle MP, Pellikka PA, Sidhu MS, Boden WE, et al.: Diagnosis and management of atherosclerotic cardiovascular disease in chronic kidney disease: A review. Kidney Int 91: 797–807, 2017 [DOI] [PubMed] [Google Scholar]
- 59.Menon V, Greene T, Wang X, Pereira AA, Marcovina SM, Beck GJ, et al.: C-reactive protein and albumin as predictors of all-cause and cardiovascular mortality in chronic kidney disease. Kidney Int 68: 766–772, 2005 [DOI] [PubMed] [Google Scholar]
- 60.Young JM, Terrin N, Wang X, Greene T, Beck GJ, Kusek JW, et al.: Asymmetric dimethylarginine and mortality in stages 3 to 4 chronic kidney disease. Clin J Am Soc Nephrol 4: 1115–1120, 2009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Stehouwer C, Henry R, Dekker J, Nijpels G, Heine R, Bouter L: Microalbuminuria is associated with impaired brachial artery, flow-mediated vasodilation in elderly individuals without and with diabetes: Further evidence for a link between microalbuminuria and endothelial dysfunction--the Hoorn Study. Kidney Int 92: S42–S44, 2004 [DOI] [PubMed] [Google Scholar]
- 62.Plaisance EP, Grandjean PW: Physical activity and high-sensitivity C-reactive protein. Sports Med 36: 443–458, 2006 [DOI] [PubMed] [Google Scholar]
- 63.Barbieri E, Agostini D, Polidori E, Potenza L, Guescini M, Lucertini F, et al.: The pleiotropic effect of physical exercise on mitochondrial dynamics in aging skeletal muscle. Oxid Med Cell Longev 2015: 917085, 2015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Akesson A, Larsson SC, Discacciati A, Wolk A: Low-risk diet and lifestyle habits in the primary prevention of myocardial infarction in men: A population-based prospective cohort study. J Am Coll Cardiol 64: 1299–1306, 2014 [DOI] [PubMed] [Google Scholar]
- 65.Kulshreshtha A, Vaccarino V, Judd SE, Howard VJ, McClellan WM, Muntner P, et al.: Life’s Simple 7 and risk of incident stroke: The reasons for geographic and racial differences in stroke study. Stroke 44: 1909–1914, 2013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Agha G, Loucks EB, Tinker LF, Waring ME, Michaud DS, Foraker RE, et al.: Healthy lifestyle and decreasing risk of heart failure in women: The Women’s Health Initiative observational study. J Am Coll Cardiol 64: 1777–1785, 2014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Ma J, Urizar GG Jr, Alehegn T, Stafford RS: Diet and physical activity counseling during ambulatory care visits in the United States. Prev Med 39: 815–822, 2004 [DOI] [PubMed] [Google Scholar]
- 68.Delgado C, Johansen KL: Deficient counseling on physical activity among nephrologists. Nephron Clin Pract 116: c330–c336, 2010 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.