

Abstract
Objective
To evaluate the reasons for permanent teeth extractions and related factors among adult patients visiting dental clinics in the Eastern Province of Saudi Arabia.
Materials and Methods
This retrospective cross-sectional study included data of patients who underwent teeth extractions. Data were collected from public and private dental clinics in different cities of the Eastern Province of Saudi Arabia (January–March 2020). The demographic information of patients and their reasons for teeth extractions were obtained from participating dentists.
Results
The study included data of 696 patients with 55.9% of males and 44.1% of females. The mean number of teeth extractions in the sample was 1.86 ± 1.8, and it increased significantly with advancing age (P ≤ 0.001). Saudi (1.97 ± 1.98) versus non-Saudi patients (1.55 ± 1.11) (P=0.02) and patients in public practice (2.03 ± 1.95) versus patients in private practice (1.50 ± 1.38) (P ≤ 0.001) showed significantly higher teeth extractions. Dental caries was the most common reason for teeth extractions (49.1%), followed by remaining roots (18.5%), periodontal disease (18.4%), and impactions (7.2%). Most commonly extracted teeth included tooth # 30 (9.8%), followed by tooth #16 (9.6%), tooth # 1 (8.8%), tooth # 19 (8.3%), and tooth # 4 (8.3%). On the other hand, upper incisors were the least commonly extracted teeth.
Conclusions
Dental caries, remaining roots, periodontal disease, and impactions were the most common reasons for teeth extractions in our sample of patients. The extractions increased significantly with increasing age. Saudis and patients in public clinics underwent significantly higher teeth extractions. Measures aimed at the prevention and treatment of oral conditions can help reduce teeth extractions and improve the quality of life of patients.
1. Introduction
Globally, total tooth loss affected 276 million people in 2015, and these estimates are expected to increase in the future due to population growth and aging [1]. Loss of permanent teeth can lead to masticatory dysfunction, pronunciation difficulty, malnutrition, limited choices of food, social isolation, and poor quality of life [2–4]. Tooth loss is a risk factor for cardiovascular disease and stroke, and there is a significant dose-response relationship between tooth loss and cardiovascular disease and stroke [5]. The literature also indicates that patients with tooth loss are 1.34 times more likely to develop dementia [2]. Recently, researchers confirmed a relationship between tooth loss susceptibility to all-cause mortality [6]. According to the Ministry of Health, 18,640 permanent teeth were extracted in 2019 in the Eastern Province of Saudi Arabia [7]. It was also reported that the numbers of extracted permanent teeth increased from the year 2011 to 2015 in the country [8].
Many recent studies conducted in adults around the world showed that caries was the leading cause of tooth extraction followed by periodontal disease [9–13]. A study conducted in Riyadh Saudi Arabia found that 50.2% of permanent teeth were extracted due to dental caries, and this was followed by orthodontic problems (18.2%), eruption problems (17.5%), and periodontal problems (8.2%) [14]. In Jizan, Saudi Arabia, dental caries was the most common reason for teeth extractions in younger patients whereas periodontal disease was the major reason for teeth extractions in older patients [15]. Dental caries accounted for 89.8% of teeth extracted in a study of 949 patients in Madinah [16]. A study evaluated reasons for teeth extractions in rural and urban populations of Al-Baha city. The authors showed that dental caries was the most frequent reason for teeth extraction in young patients whereas most teeth were extracted due to periodontal reasons in patients above 40 years of age [17].
Teeth extractions are very common in the Eastern Province of Saudi Arabia. However, the reasons for teeth extractions were not fully investigated. Therefore, the study aimed to evaluate the reasons for teeth extraction among adult populations in the Eastern Province of Saudi Arabia. The study will also explore the patterns of teeth extractions in private and public dental clinics. The study will inform policy makers to establish preventive programs to reduce the prevalence of teeth extractions. In addition, data may be used for the planning of oral health services and the dental workforce and revising dental curricula. This can also help decrease the cost of treatment and minimize the harmful effects of tooth loss.
2. Materials and Methods
This retrospective cross-sectional study included data of patients who underwent teeth extractions during the last one month. Patient data were obtained from oral surgeons and dentists practicing in different settings (governmental hospitals, governmental primary health care centers, private clinics, and teaching hospitals) in the Eastern Province of Saudi Arabia. The researchers visited these settings in person for data collection. A convenience sample was used for the selection of participating oral surgeons and dentists. The study included those oral surgeons and dentists who have been practicing in the province and provided their informed consent. After discussing the purpose and modalities of the study, a record form was handed to study participants. Researchers assured anonymity, privacy, and confidentiality of research data. The record form was printed in English language.
The information in the record form can be divided into two sections. The first section was filled by the participating dentists, which included the date of the extraction, patient's age, gender, tooth number, and the reasons for teeth extractions. The reasons for teeth extractions were assigned as the following groups: caries, remaining roots, periodontal diseases, orthodontic, prosthodontic, impaction, trauma, cosmetic/esthetic, cysts, and others. The second section was filled by the interns, and it included the sector (governmental, private, or educational) and the location of dental practice.
The researchers collected data from participating dentists on weekly basis during a period of three months (Jan–March 2020). Some oral surgeon and dentists returned the completed record form during the first visit of researchers. Those participants who were unable to provided patients data were visited again after one-two weeks. A maximum of three visits were made to those dentists who were busy and were unable to provide data in the first and second visits. The study was conducted in accordance with ethical principles of the Declaration of Helsinki.
Data were entered in MS Excel (2010) and then transferred to IBM SPSS for Windows version 22.0 (IBM Corp., Armonk, N.Y., USA) for statistical analysis. Descriptive statistics included frequencies, percentages, means, and standard deviations. The Pearson chi-square test was used to compare differences in the proportions of reasons for teeth extractions between males versus females, Saudi patients versus non-Saudi patients, and patients visiting the public sector versus the private sector. A Kolmogorov–Smirnov test was performed to confirm the normality of quantitative variable, and accordingly, a t-test and one-way ANOVA test were used in the study. An independent t-test was performed to compare the mean number of extracted teeth in male and female patients, Saudi and non-Saudi patients, and patients in public and private sectors. One-way ANOVA was used to compare mean differences in the number of teeth extractions in different categories of age. A P value of less than 0.05 was used for statistical significance.
3. Results
The study included data analysis of 696 patients with 64.5% in the age range of 25–54 years. There were 55.9% of males and 44.1% of females with 73.7% of Saudi patients in the study. More patients (67.4%) were from public practice than private practice (32.6%) (Table 1).
Table 1.
Demographic information of patients (N = 696).
| Variables | Patients, N (%) |
|---|---|
| Age | |
| 15–24 | 113 (16.2) |
| 25–34 | 198 (28.4) |
| 35–44 | 125 (18.0) |
| 45–54 | 126 (18.1) |
| 55–64 | 87 (12.5) |
| 65 and above | 47 (6.8) |
|
| |
| Gender | |
| Male | 389 (55.9) |
| Female | 307 (44.1) |
|
| |
| Nationality | |
| Saudi | 513 (73.7) |
| Non-Saudi | 183 (26.3) |
|
| |
| Type of practice | |
| Public | 469 (67.4) |
| Private | 227 (32.6) |
The mean number of teeth extractions in the sample was 1.86 ± 1.8. The study found a statistically significant difference in the mean number of extracted teeth in different age groups (P ≤ 0.001), and the mean number of teeth extractions increased with advancing age. A significantly higher mean number of extracted teeth was found in Saudi (1.97 ± 1.98) versus non-Saudi patients (1.55 ± 1.11) (P=0.02) and patients in public (2.03 ± 1.95) versus patients in private practice (1.50 ± 1.38) (P ≤ 0.001). Males had a greater mean number of extracted teeth than females, but the difference was not statistically significant (P=0.517) (Table 2).
Table 2.
Relationship between demographic factors and teeth extractions.
| Variables | Mean number of extracted teeth Mean ± SD |
P value |
|---|---|---|
| Age | ||
| 15–24 | 1.28 ± 0.55 | <0.001 |
| 25–34 | 1.45 ± 1.00 | |
| 35–44 | 2.06 ± 2.44 | |
| 45–54 | 2.06 ± 1.79 | |
| 55–64 | 2.30 ± 2.17 | |
| 65 and above | 3.04 ± 2.60 | |
|
| ||
| Gender | ||
| Male | 1.96 ± 2.09 | 0.517 |
| Female | 1.73 ± 1.35 | |
|
| ||
| Nationality | ||
| Saudi | 1.97 ± 1.98 | 0.02 |
| Non-Saudi | 1.55 ± 1.11 | |
|
| ||
| Type of practice | ||
| Public | 2.03 ± 1.95 | <0.001 |
| Private | 1.50 ± 1.38 | |
Dental caries was the most common reason for teeth extractions (49.1%), followed by remaining roots (18.5%), periodontal disease (18.4%), and impactions (7.2%) (Figure 1).
Figure 1.
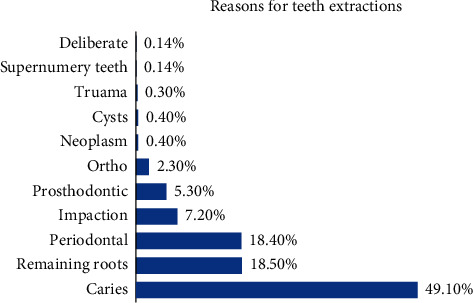
Distribution of reasons for teeth extractions in patients.
Table 3 shows the relationships of reasons for teeth extractions with gender, nationality, and type of dental practice. Higher proportions of males compared with females had teeth extracted due to caries, periodontal disease, remaining roots, impactions, and prosthodontics; however, differences were not statistically significant. A significantly higher proportion of Saudi (68.4%) than non-Saudi patients (31.6%) had tooth extracted due to caries (P=0.002). Overall, more Saudi versus non-Saudi patients had teeth extractions due to periodontal disease, remaining roots, impactions, and prosthodontics, but differences were not statistically significant (P > 0.05). The patients in public clinics had significantly greater extractions due to caries than those in private practice (P=0.003). On the other hand, more orthodontic extractions were performed in private than public practice, and the difference was statistically significant (P=0.041).
Table 3.
Distribution of reasons for teeth extractions among patients by gender, nationality, and type of dental practice.
| Male, N (%) | Female, N (%) | P value | Saudi, N (%) | Non-Saudi, N (%) | P value | Public, N (%) | Private, N (%) | P value | |
|---|---|---|---|---|---|---|---|---|---|
| Caries | 198 (57.9) | 144 (42.1) | 0.295 | 234 (68.4) | 108 (31.6) | 0.002 | 249 (72.8) | 93 (27.2) | 0.003 |
| Periodontal | 68 (53.1) | 60 (46.9) | 0.485 | 99 (77.3) | 29 (22.7) | 0.301 | 81 (63.3) | 47 (36.7) | 0.125 |
| Remaining roots | 65 (50.4) | 64 (49.6) | 0.163 | 100 (77.5) | 29 (22.5) | 0.276 | 76 (58.9) | 53 (41.1) | 0.023 |
| Impactions | 32 (64) | 18 (36) | 0.231 | 37 (74) | 13 (26) | 0.752 | 35 (70) | 15 (30) | 0.682 |
| Prosthodontic | 22(59.5) | 15 (40.5) | 0.653 | 27 (73) | 10 (27) | 0.917 | 29 (78.4) | 8 (21.6) | 0.143 |
| Orthodontics | 8 (50) | 8 (50) | 0.631 | 16 (100) | 0 | 0.016 Fisher |
7 (43.8) | 9 (56.3) | 0.041 |
Figure 2 presents the distribution of the types of teeth extracted among patients. Most commonly extracted teeth included tooth # 30 (9.8%), followed by tooth #16 (9.6%), tooth # 1 (8.8%), tooth # 19 (8.3%), and tooth # 4 (8.3%). On the other hand, upper incisors were the least commonly extracted teeth in the study.
Figure 2.
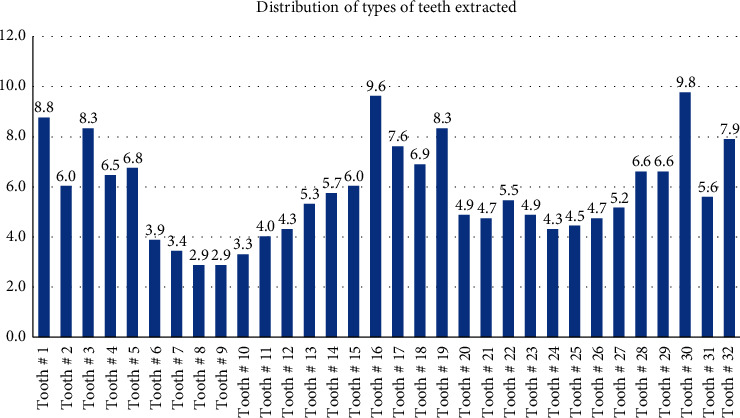
Distribution of type of teeth extracted among patients.
Figure 3 shows the number of teeth extractions in patients. Two-thirds of patients (64.5%) had one tooth extracted, 16.2% had two teeth extracted, and 9.2% had three teeth extracted. The extractions of more than 5 teeth were reported in 4.2% of patients.
Figure 3.
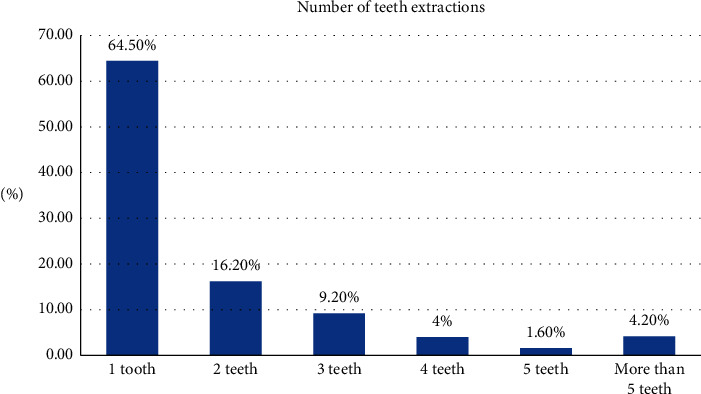
Distribution of the number of teeth extractions in patients.
4. Discussion
Dental caries and periodontal disease were the most common reasons for teeth extractions in the present study. Similar findings were reported in previous studies by Lesolang et al. [10] in South Africa, Byahatti and Ingafou [11] in Libya, Al-Shammari et al. [12] in Kuwait, Anand and Kuriakose [18] in India, Zafar et al. [19] in Pakistan, Taiwo et al. [9] in Nigeria, Lee et al. [20] in Taiwan, Morita et al. [13] in Japan, Angelillo et al. [21] in Italy, and Ong et al. [22] in Singapore. In Saudi Arabia, Asmat et al. also found that caries was the most frequent reason for teeth extractions followed by periodontal disease [23]. Gossadi et al. indicated caries as the main reason for teeth extractions in 20–29 year-old patients, and periodontal diseases were the most common reasons for teeth extraction in 40–59-year-old patients in Gizan, Saudi Arabia [15]. However, Alaboudi et al. reported that caries was responsible for 89.8% of teeth extractions in Madinah, Saudi Arabia [16].
The high prevalence of dental caries and periodontitis globally and locally explains the reasons for these findings in the international and local literature. Globally, dental caries and periodontal disease are widely distributed in different populations. According to the Global Burden of Disease Study (2017), 3.47 billion people suffered from oral disorders and dental caries in permanent teeth was the most common health condition affecting 2.3 billion people around the globe [24]. Similarly, severe periodontitis was the sixth most common condition affecting 10.8% of the world population in 2010 [25]. Locally, a study reported caries prevalence of 89.2% in adult patients in the Al-Ahsa region of Saudi Arabia [26]. Similarly, a high prevalence of periodontitis (36.8%) was observed in adult patients in Abha, Saudi Arabia [27]. It should be noted that the provision of dental care for caries or periodontal disease can prevent tooth loss. However, the prevention of tooth loss may result in a simultaneous increase in the prevalence and incidence of caries and periodontitis [28]. It is known that the direct treatment cost of oral conditions was US$298 billion in 2010 which represented 4.6% of healthcare expenditure worldwide [29]. Therefore, efforts should be focused on preventive measures to prevent caries, periodontitis, and other oral conditions.
Dental caries is a disease of the adults, and the incidence rate of dental caries in adults is as great as in adolescents and children [30]. However, dental caries being a chronic and cumulative disease increases with age [31]. The distribution of periodontal disease also varies in different life spans of an individual. Globally, the prevalence of periodontitis (periodontal pocket of 4-5 mm) is 9.1% in adolescents, 27.7% in adults, and 30.6% in older persons [32]. It is known that the severe periodontitis increases with advancing age, reaches its peak at 40 years of life, and stabilizes in old age [33]. Dental caries and periodontal diseases are the main causes of teeth extractions, and the distributions of these conditions increase with age. This explains the reasons for greater teeth extractions with advancing age in the present study.
A previous study in Saudi Arabia showed that Saudi patients demonstrated significantly higher gingivitis than non-Saudi patients [27]. In the present study, Saudi patients underwent significantly higher teeth extraction compared with non-Saudi populations. Poor oral hygiene, increased consumption of fermentable carbohydrates, low routine dental attendance, low awareness about oral health programs, and tobacco consumption are common among Saudi populations, and these factors increase their predisposition to oral diseases which can eventually lead to tooth mortality [27, 34, 35].
Dental practitioners in private dental clinics charge a fee for the delivery of oral care from their patients or health insurance companies. They are more likely to provide more conservative, endodontic, periodontal, and other dental treatments to achieve patient satisfaction and greater earning/profits for their clinics. On the contrary, dentists in public clinics are paid by the government for the services provided to patients and may be less interested in providing conservative and time consuming dental treatment. In addition, dentists may be unable to provide treatment to a large number of patients visiting public dental clinics because dental care is free in Saudi Arabia [36]. Moreover, patients attending public dental clinics may not be aware of treatments available to save the tooth and, hence, may agree to tooth extraction rather than availing other treatment options. These may account for a significantly greater number of teeth extractions in public than in private clinics in the present study.
Mandibular and maxillary molars were the most frequently extracted teeth in the present study. Similar findings were observed in previous studies [9, 14, 19, 20]. The reasons for increased extractions of molars in both dentitions can be explained by their morphology, the timing of eruption, and position in the oral cavity. The presence of deep pits and fissures increases the susceptibility of molars to the accumulation of food debris and retention of plaque which increases the risk of caries. First, permanent molars erupt earlier in the oral cavity which predisposes them to acid attack more than other teeth. In addition, caries in the first permanent molars can lead to caries in the second molars, premolars, and incisors [37]. The researchers suggest an association between caries and periodontal disease and excessive intake of fermentable carbohydrates can account for the development of caries and inflammation of periodontal tissues [38]. Additionally, the position of molars in the oral cavity can affect one's ability to maintain proper oral hygiene and plaque control resulting in caries and tooth loss. On the other hand, anterior teeth were least frequently extracted teeth in the present study. The morphology of anterior teeth and cleansing and buffering actions due to greater availability of saliva from submandibular and sublingual salivary glands may explain the reasons for their reduced extractions [39].
The study added valuable information from the Eastern Province of Saudi Arabia to the existing knowledge base on the reasons for permanent teeth extractions. However, there are certain limitations to the study. The findings of the study should not be generalized to populations in other regions in Saudi Arabia. Moreover, self-reported data also are subjected to biases in the study.
5. Conclusions
The study found that dental caries was the most common reason for teeth extractions, followed by periodontal disease. Maxillary and mandibular molars were the most frequently extracted teeth. Saudis and patients in public clinics underwent greater extractions compared with non-Saudis and patients in private practice. The number of extractions enhanced with an increase in the age of patients. Oral health-care systems should focus on the effective prevention and treatment of oral conditions particularly caries and periodontal disease to reduce the burden of teeth extractions and improve the quality of life of patients.
Data Availability
The SPSS data file of this study is available from the corresponding author upon request.
Conflicts of Interest
The authors declare that there are no conflicts of interest regarding the publication of this paper.
References
- 1.Kassebaum N. J., Smith A. G. C., Bernabé E., et al. Global, regional, and national prevalence, incidence, and disability-adjusted life years for oral conditions for 195 countries, 1990–2015: a systematic analysis for the global burden of diseases, injuries, and risk factors. Journal of Dental Research. 2017;96(4):380–387. doi: 10.1177/0022034517693566. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Chen J., Ren C. J., Wu L., et al. Tooth loss is associated with increased risk of dementia and with a dose-response relationship. Frontiers in Aging Neuroscience. 2018;10:p. 415. doi: 10.3389/fnagi.2018.00415. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Gerritsen A. E., Allen P. F., Witter D. J., Bronkhorst E. M., Creugers N. H. Tooth loss and oral health-related quality of life: a systematic review and meta-analysis. Health and Quality of Life Outcomes. 2010;8(1):p. 126. doi: 10.1186/1477-7525-8-126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kossioni A. The association of poor oral health parameters with malnutrition in older adults: a review considering the potential implications for cognitive impairment. Nutrients. 2018;10(11):p. 1709. doi: 10.3390/nu10111709. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Cheng F., Zhang M., Wang Q., et al. Tooth loss and risk of cardiovascular disease and stroke: a dose-response meta analysis of prospective cohort studies. PloS One. 2018;13:p. e0194563. doi: 10.1371/journal.pone.0194563. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Peng J., Song J., Han J., et al. The relationship between tooth loss and mortality from all causes, cardiovascular diseases, and coronary heart disease in the general population: systematic review and dose-response meta-analysis of prospective cohort studies. Bioscience Reports. 2019;39(1):p. BSR20181773. doi: 10.1042/bsr20181773. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ministry of Health. Statistical Yearbook-2017. Saudi Arabia: Ministry of Health; 2017. https://www.moh.gov.sa/en/Ministry/Statistics/book/Pages/default.aspx. [Google Scholar]
- 8.Ministry of Health. Statistical Yearbook-2015. Saudi Arabia: Ministry of Health; 2015. https://www.moh.gov.sa/en/Ministry/Statistics/book/Pages/default.aspx. [Google Scholar]
- 9.Taiwo A. O., Ibikunle A. A., Braimah R. O., Sulaiman O. A., Gbotolorun O. M. Tooth extraction: pattern and etiology from extreme Northwestern Nigeria. European Journal of Dentistry. 2017;11(3):335–339. doi: 10.4103/ejd.ejd_160_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Lesolang R. R., Motloba D. P., Lalloo R. Patterns and reasons for tooth extraction at the Winterveldt Clinic: 1998–2002. SADJ: journal of the South African Dental Association=tydskrif van die Suid-Afrikaanse Tandheelkundige Vereniging. 2009;64(5):214–218. [PubMed] [Google Scholar]
- 11.Byahatti S. M., Ingafou M. S. H. Reasons for extraction in a group of Libyan patients. International Dental Journal. 2011;61(4):199–203. doi: 10.1111/j.1875-595x.2011.00057.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Al-Shammari K. F., Al-Ansari J. M., Al-Melh M. A., Al-Khabbaz A. K. Reasons for tooth extraction in Kuwait. Medical Principles and Practice. 2006;15(6):417–422. doi: 10.1159/000095486. [DOI] [PubMed] [Google Scholar]
- 13.Morita M., Kimura T., Kanegae M., Ishikawa A., Watanabe T. Reasons for extraction of permanent teeth in Japan. Community Dentistry and Oral Epidemiology. 1994;22(5PT1):303–306. doi: 10.1111/j.1600-0528.1994.tb02056.x. [DOI] [PubMed] [Google Scholar]
- 14.Alesia K., Khalil H. S. Reasons for and patterns relating to the extraction of permanent teeth in a subset of the Saudi population. Clinical, Cosmetic and Investigational Dentistry. 2013;5:51–56. doi: 10.2147/CCIDE.S49403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Yahya I., Nahari H. H., Kinani H. M., Siddig I., Al Moaleem M. M. Reasons for permanent teeth extraction in Jizan region of Saudi Arabia. Journal of Dental and Medical Sciences. 2015;14:86–89. [Google Scholar]
- 16.Alaboudi A. K., Aboalshamat K. T., Mahfouz A., Alobodi A., Abualfaraj A. Reasons for teeth extraction in governmental hospitals in Madinah City, Saudi Arabia. IOSR Journal of Dental and Medical Sciences. 2016;15(7):01–05. doi: 10.9790/0853-1507110105. [DOI] [Google Scholar]
- 17.Preethanath R. S. Reasons for tooth extraction in urban and rural populations of Saudi Arabia. Pakistan Oral & Dental Journal. 2010;30:199–204. [Google Scholar]
- 18.Anand P. S., Kuriakose S. Causes and patterns of loss of permanent teeth among patients attending a dental teaching institution in south India. Journal of Contemporary Dental Practice. 2009;10:E057–E064. doi: 10.5005/jcdp-10-5-58. [DOI] [PubMed] [Google Scholar]
- 19.Zafar K. J., Iftikhar B., Ghaffar K., Khurram M., Hassan F., Javed M. Extraction of permanent teeth: etiology and pattern at a tertiary care hospital. Pakistan Oral & Dental Journal. 2019;39:243–246. [Google Scholar]
- 20.Lee C. Y., Chang Y. Y., Shieh T. Y., Chang C. S. Reasons for permanent tooth extractions in Taiwan. Asia-Pacific Journal of Public Health. 2015;27:2350–2357. doi: 10.1177/1010539512448814. [DOI] [PubMed] [Google Scholar]
- 21.Angelillo I. F., Nobile C. G. A., Pavia M. Survey of reasons for extraction of permanent teeth in Italy. Community Dentistry and Oral Epidemiology. 1996;24(5):336–340. doi: 10.1111/j.1600-0528.1996.tb00872.x. [DOI] [PubMed] [Google Scholar]
- 22.Ong G., Yeo J.-F., Bhole S. A survey of reasons for extraction of permanent teeth in Singapore. Community Dentistry and Oral Epidemiology. 1996;24(2):124–127. doi: 10.1111/j.1600-0528.1996.tb00828.x. [DOI] [PubMed] [Google Scholar]
- 23.Ullah A., Ullah F., Alkhamis A., et al. Reasons of teeth extraction in patients seen at dental clinics of college of dentistry, Al Jouf University, Kingdom of Saudi Arabia. Pakistan Oral & Dental Journal. 2020;40:37–39. [Google Scholar]
- 24.Global Health Metrics. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392:1789–1858. doi: 10.1016/S0140-6736(18)32279-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Frencken J. E., Sharma P., Stenhouse L., Green D., Laverty D., Dietrich T. Global epidemiology of dental caries and severe periodontitis-a comprehensive review. Journal of Clinical Periodontology. 2017;44(Suppl 18):S94–s105. doi: 10.1111/jcpe.12677. [DOI] [PubMed] [Google Scholar]
- 26.Al-Ghannam N., Khan N., Al-Shammery A., Wyne A. Trends in dental caries and missing teeth in adult patients in Al-Ahsa, Saudi Arabia. Saudi Dental Journal. 2005;17:57–62. [Google Scholar]
- 27.Hossain M. Z., Fageeh H. N., Elagib M. F. A. Prevalence of periodontal diseases among patients attending the outpatient department at the college of dentistry, King Khalid University, Abha, Saudi Arabia. City Dental College Journal. 2013;10:9–12. [Google Scholar]
- 28.Kassebaum N. J., Bernabé E., Dahiya M., Bhandari B., Murray C. J. L., Marcenes W. Global burden of severe tooth loss. Journal of Dental Research. 2014;93(7):20s–28S. doi: 10.1177/0022034514537828. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Listl S., Galloway J., Mossey P. A., Marcenes W. Global economic impact of dental diseases. Journal of Dental Research. 2015;94(10):1355–1361. doi: 10.1177/0022034515602879. [DOI] [PubMed] [Google Scholar]
- 30.Broadbent J. M., Page L. A. F., Thomson W. M., Poulton R. Permanent dentition caries through the first half of life. British Dental Journal. 2013;215(7):p. E12. doi: 10.1038/sj.bdj.2013.991. [DOI] [PubMed] [Google Scholar]
- 31.Bernabé E., Sheiham A. Age, period and cohort trends in caries of permanent teeth in four developed countries. American Journal of Public Health. 2014;104(7):e115–e121. doi: 10.2105/ajph.2014.301869. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Nazir M., Al-Ansari A., Al-Khalifa K., Alhareky M., Gaffar B., Almas K. Global prevalence of periodontal disease and lack of its surveillance. The Scientific World Journal. 2020;2020:8. doi: 10.1155/2020/2146160.2146160 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Kassebaum N. J., Bernabé E., Dahiya M., Bhandari B., Murray C. J. L., Marcenes W. Global burden of severe periodontitis in 1990-2010. Journal of Dental Research. 2014;93(11):1045–1053. doi: 10.1177/0022034514552491. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Moradi-Lakeh M., El Bcheraoui C., Tuffaha M., et al. Tobacco consumption in the Kingdom of Saudi Arabia, 2013: findings from a national survey. BMC Public Health. 2015;15:p. 611. doi: 10.1186/s12889-015-1902-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Idris A. M., Vani N. V., Almutari D. A., Jafar M. A., Boreak N. Analysis of sugars and pH in commercially available soft drinks in Saudi Arabia with a brief review on their dental implications. Journal of International Society of Preventive and Community Dentistry. 2016;6:S192–S196. doi: 10.4103/2231-0762.197190. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Alshahrani A. M., Raheel S. A. Health-care system and accessibility of dental services in kingdom of Saudi Arabia: an update. Journal of International Oral Health. 2016;8:883–887. [Google Scholar]
- 37.Nazir M. A., Bakhurji E., Gaffar B. O., Al-Ansari A., Al-Khalifa K. S. First permanent molar caries and its association with carious lesions in other permanent teeth. Journal of Clinical Diagnosis Research. 2019;13:ZC36–ZC39. [Google Scholar]
- 38.Nyvad B., Takahashi N. Integrated hypothesis of dental caries and periodontal diseases. Journal of Oral Microbiology. 2020;12(1) doi: 10.1080/20002297.2019.1710953.1710953 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Anyanechi C., Chukwuneke F. Survey of the reasons for dental extraction in eastern Nigeria. Annals of Medical and Health Sciences Research. 2012;2(2):129–133. doi: 10.4103/2141-9248.105659. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The SPSS data file of this study is available from the corresponding author upon request.