

Abstract
Background and aim of the work:
The effect of tobacco smoking on COVID-19 disease is debated, with common sense and experts suggesting a deleterious effect, and manuscripts worldwide reporting a low prevalence of active tobacco smokers among intensive care unit patients.
Methods:
We categorized countries worldwide into three groups with <25%; 25-45%; >45% of active male smokers with data expressed as median and interquartile range [IQR] and extracted data on SARS-CoV-2 infections and COVID-19 deaths per million inhabitants from public available databases. We also applied multivariate regression techniques to adjust for several epidemiological factors.
Results:
COVID-19 mortality was 13 (5-24) per million inhabitants in countries with male smokers >45% and 33 (4-133) in countries where male smokers were <25%. SARS-CoV-2 infection rates were 436 (217-954) and 1139 (302-4084) per million inhabitants with data confirmed when dividing data for each continent and when controlling for confounding factors.
Conclusions:
We found a counterintuitive low COVID-19 mortality and SARS-CoV-2 infection in countries with high prevalence of male smokers at the global level and within each continent, suggesting that active smoking habit is protective. Further research should urgently investigate which is the possible mechanism of action. (www.actabiomedica.it)
Keywords: COVID-19, tobacco, smoking, critical care, intensive care, mortality
Introduction
As of October 6th 2020, >35 million SARS-CoV-2 cases were reported worldwide, with >1 million COVID-19 deaths1. Risk factors are still largely unknown, however, being male2 and being active tobacco smoker3 are surprisingly respectively associated with increased and reduced rates of SARS-CoV-2 infections and need for hospital and intensive care unit admission. We investigated whether countries with high prevalence of male smokers have a reduced rate of SARS-CoV-2 infections and COVID-19 deaths per million inhabitants.
Methods
SARS-CoV-2 infections and COVID-19 deaths per million inhabitants were extracted for all available countries on June 28th 20203 together with the percentage of adult male smokers in each country4. Countries with incomplete or missing data, either regarding the pandemic (n=14) or the smoking habits (n=91), were excluded. The remaining countries were categorized into three groups (with <25%; 25-45%; >45% of male smokers) with data expressed as median and interquartile range [IQR]. In order to explore the robustness of the unconditional results and to address potential omitted variable bias, we applied multivariate regression techniques (Ordinary Least Squares) to SARS-CoV-2 infections and COVID-19 deaths per million inhabitants as dependent variables. T-values on the estimated coefficients are robust to heteroskedasticity, i.e. to heterogeneity in the variance of the error term across countries. As explanatory variables we added (i) the starting date of the epidemics in each country; (ii) country population (expressed in millions), (iii) population density (number of inhabitants per square kilometer), (iv) the percentage of residents who were over 65 years old in the year 2017, to which we added in one specification real per capita Gross Domestic Product (GDP) in dollars in year 2017, adjusted for purchasing power parity to allow cross-country comparisons. The beginning of the epidemic in each country was defined as the day when the country reached 0.1 deaths per 1,000,000 population5. Total population and population density data were taken from the United Nations’ World Population Prospects 20196. Data on the percentage of citizens >65 years and on real per capita GDP were taken from the World Development Indicators at the World Bank7.
Results
The 110 countries included in the analyses are shown in table 1. COVID-19 median (IQR) mortality per million inhabitants was as low as 13 (5-24) in countries with male smokers >45% and as high as 33 (4-133) in countries where male smokers were <25% (figure 1). We found similar results for SARS-CoV-2 infection rates per million inhabitant: 436 (217-954) in countries with male smokers >45% and 1139 (302-4084) in countries where male smokers were <25% (figure 1). When splitting the data within each continent we found similar magnitude and direction of findings (Figures 2, 3 and 4).
Table 1.
list of all nations with available data on active male smokers, SARS-CoV-2 infection rate and COVID-19 deaths per million inhabitants (from World Health Organization(ref4), in decreasing order of male smokers’ rate):
| Country | Male Smokers Rate % |
| Indonesia | 76.2 |
| Jordan | 70.2 |
| Russia | 59 |
| Georgia | 57.7 |
| Cuba | 52.7 |
| Greece | 52.6 |
| Armenia | 52.3 |
| Albania | 51.2 |
| Kyrgyzstan | 50.4 |
| Egypt | 49.9 |
| South Korea | 49.8 |
| Ukraine | 49.4 |
| Latvia | 48.9 |
| Bahrain | 48.8 |
| Montenegro | 47.9 |
| China | 47.6 |
| Bosnia and Herzegovina | 47.2 |
| Vietnam | 47.1 |
| Azerbaijan | 46.5 |
| Belarus | 46.2 |
| Moldova | 45.7 |
| Lebanon | 45.4 |
| Morocco | 45.4 |
| Mauritania | 44 |
| Kazakhstan | 43.9 |
| Serbia | 43.6 |
| Malaysia | 43 |
| Philippines | 43 |
| Bulgaria | 42.4 |
| Pakistan | 41.9 |
| Thailand | 41.4 |
| Estonia | 41.2 |
| Israel | 41.2 |
| Mauritius | 40.1 |
| Chile | 40 |
| Slovakia | 39.7 |
| Turkey | 39.5 |
| Croatia | 39.4 |
| Lithuania | 38.1 |
| Andorra | 37.2 |
| Nepal | 37.1 |
| Kuwait | 37 |
| Romania | 36.9 |
| Mali | 36.8 |
| Austria | 35.5 |
| Japan | 33.7 |
| Honduras | 33.3 |
| Germany | 32.4 |
| Poland | 32.4 |
| Hungary | 32 |
| Myanmar | 31.6 |
| Portugal | 31.5 |
| Mozambique | 31.4 |
| South Africa | 31.4 |
| Spain | 31.3 |
| Zimbabwe | 31.2 |
| Bangladesh | 30.98 |
| Bolivia | 30.5 |
| Jamaica | 29.9 |
| France | 29.8 |
| Malta | 29.7 |
| Argentina | 29.5 |
| Brunei | 29.3 |
| Czech Republic | 29 |
| Sri Lanka | 28.4 |
| Italy | 28.3 |
| Paraguay | 28.3 |
| Singapore | 28 |
| Saudi Arabia | 27.9 |
| Qatar | 26.9 |
| Switzerland | 26.9 |
| Uruguay | 26.7 |
| Belgium | 26.5 |
| Zambia | 26.5 |
| Netherlands | 26.2 |
| Luxembourg | 25.8 |
| Malawi | 25.4 |
| Uzbekistan | 24.9 |
| Kenya | 24.6 |
| Senegal | 23.4 |
| Finland | 23.2 |
| Ireland | 22.4 |
| Norway | 22.4 |
| Slovenia | 22.3 |
| Haiti | 22.1 |
| Iran | 21.5 |
| Peru | 21.5 |
| Oman | 21 |
| Mexico | 20.8 |
| India | 20.4 |
| Sweden | 20.4 |
| United Kingdom | 19.9 |
| United States | 19.5 |
| Brazil | 19.3 |
| Dominican Republic | 18.8 |
| Niger | 18.6 |
| Costa Rica | 18.5 |
| Benin | 17.7 |
| Canada | 17.7 |
| Denmark | 17.6 |
| Nigeria | 17.4 |
| New Zealand | 17.2 |
| Iceland | 17 |
| Australia | 16.7 |
| Colombia | 16 |
| Ecuador | 14 |
| Barbados | 13.1 |
| Ghana | 13.1 |
| Panama | 10.6 |
| Ethiopia | 8.9 |
Figure 1.
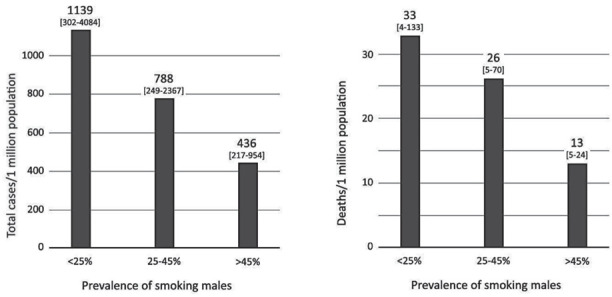
SARS-CoV-2 infections and COVID-19 deaths per million inhabitants worldwide
Figure 2.
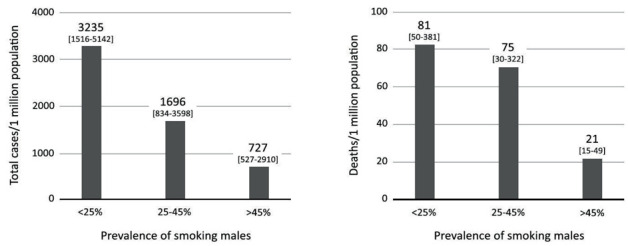
SARS-CoV-2 infections and COVID-19 deaths per million inhabitants in Europe (39 nations with available data), with different prevalence of active male smokers (<25%; 25-45%; >45%).
Figure 3.
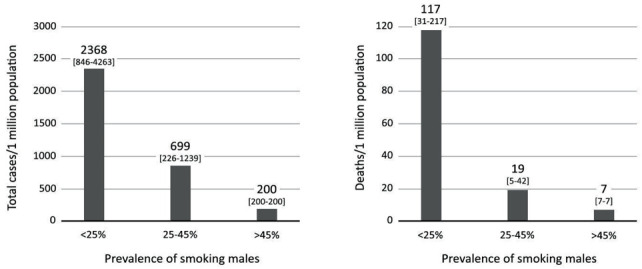
SARS-CoV-2 infections and COVID-19 deaths per million inhabitants in the Americas (20 nations with available data), with different prevalence of active male smokers (<25%; 25-45%; >45%).
Figure 4.
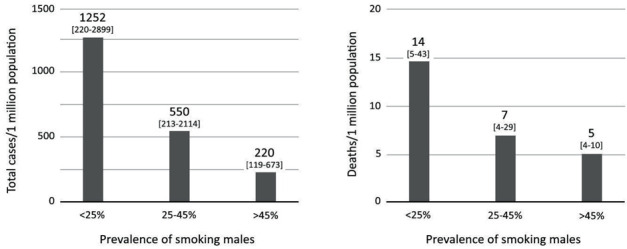
SARS-CoV-2 infections and COVID-19 deaths per million inhabitants in Asia (32 nations with available data), with different prevalence of active male smokers (<25%; 25-45%; >45%).
In Table 2 we show that the negative correlation between mortality rates per million and prevalence of male smokers is strongly significant (at the 1% confidence level) and robust to controlling for confounding factors. More precisely, a percentage point increase in the prevalence of male smokers was associated with about 3 deaths per million less (columns 3 and 4). On the other hand, the negative correlation between total cases and prevalence of male smokers appeared to be less robust: it was mildly significant at the 10% confidence level (column 1) when not controlling for real per capita GDP, while it was estimated to be positive and non-significant at ordinary confidence levels when controlling for real per capita GDP (column 2).
Table 2.
Multivariate regressions on COVID-19 total cases and deaths.
| Dependent Variable: | COVID-19 cases per million | COVID-19 deaths per million | ||
| [column 1] | [column 2] | [column 3] | [column 4] | |
| Prevalence of smoking males | -31.589* | 18.875 | -3.218*** | -2.709*** |
| (-1.704) | (0.855) | (-3.836) | (-3.368) | |
| Starting date of the epidemics | -53.210*** | -2.698 | -2.297*** | -1.809** |
| (-2.997) | (-0.186) | (-3.109) | (-2.493) | |
| Population | -2.569** | -0.438 | -0.033 | -0.013 |
| (-2.191) | (-0.801) | (-0.786) | (-0.319) | |
| Population density | 0.680*** | -0.371 | -0.010** | -0.020*** |
| (3.031) | (-0.767) | (-2.485) | (-3.312) | |
| Prevalence of over 65 citizens (2017 data) | -87.598 | -233.191** | 6.407*** | 5.044** |
| (-0.985) | (-2.008) | (3.016) | (2.311) | |
| Real per capita GDP (2017 data) | . | 0.129** | . | 0.001** |
| . | (2.419) | . | (2.212) | |
| Countries | 106 | 105 | 106 | 105 |
| R-squared | 0.094 | 0.436 | 0.281 | 0.299 |
Notes: OLS (Ordinary Least Squares) estimates for the total number of confirmedCOVID-19 cases (columns [1] and [2]) and deaths (columns [3] and [4]). Heteroskedasticity-robust t-values are reported below each coefficient. *** denotes significance of the coefficient at 1% confidence level, ** for 5% confidence, and * for 10% confidence.
Regarding the other explanatory factors, it is interesting to note that the country-specific starting date of the epidemics was negatively and significantly correlated with mortality, thus confirming the previous result obtained by Landoni et al. on a smaller sample of 15 European and American countries5. Not surprisingly, the prevalence of citizens over 65 was positively and significantly correlated with COVID-19 mortality, while it was negatively and significantly correlated with total COVID-19 cases when controlling for real per capita GDP. Finally, real per capita GDP was positively and significantly correlated with both total confirmed cases and deaths.
Discussion
We found a low COVID-19 mortality and SARS-CoV-2 infection in countries with high prevalence of male smokers at the global level and within each continent, confirming3 that active smoking habit is protective.
The reason why active smoking is protective against SARS-CoV-2 infection and its progression towards the most severe forms of the disease is unknown. Nicotine may play a major role by modulating the expression of the different isomers of the angiotensin converting enzyme receptors [ACE]8, including ACE-211, which is currently considered to be one of the entry doors for COVID-19 virus within the target cells9.
Our work has several limitations, including its observational nature and the possibility that other non-included country-dependent factors might have influenced COVID-19 mortality.
In conclusion, a high male smoker prevalence was associated with low SARS-CoV-2 infections and COVID-19 deaths per million inhabitants worldwide and in each continent. Further research should urgently investigate which is the mechanism of action and whether surrogate techniques (with the obvious purpose of avoiding the drawbacks of tobacco smoking) could be used to prevent morbidity and mortality during the epidemic.
Copyright
The Corresponding Author had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
The Corresponding Author declares that this manuscript is an original article and that he is able to prove its originality, if required from the Referees.
The Authors confirm that this manuscript has not been published before, either whole or in part, and that it is not currently under consideration for publication elsewhere.
The same Authors assign all rights, including but not limited to the copyright, for the present manuscript to Acta Biomedica upon its acceptance for publication.
Conflict of Interests:
Each author declares that he or she has no commercial associations (e.g. consultancies, stock ownership, equity interest, patent/licensing arrangement etc.) that might pose a conflict of interest in connection with the submitted article.
References
- 1. Worldometer. COVID-19 Coronavirus Pandemic. Available from: https://www.worldometers.info/coronavirus/ . [Last accessed on October 6th 2020] [Google Scholar]
- 2.Ciceri F, Castagna A, Rovere-Querini P, et al. Early predictors of clinical outcomes of COVID-19 outbreak in Milan, Italy. Clin Immunol. 2020 doi: 10.1016/j.clim.2020.108509. [Epub ahead of print] https://doi.org/10.1016/j.clim.2020.108509 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Landoni G, Moro M, Belletti A, et al. Recent exposure to smoking and COVID-19. Crit Care Resusc. 2020;22:253–256. doi: 10.1016/S1441-2772(23)00393-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.World Health Organization. Prevalence of tobacco smoking. Available from: https://www.who.int/gho/tobacco/use/en/ [Last accessed on October 6th 2020] [Google Scholar]
- 5.Landoni G, Losi D, Fresilli S, et al. Is time our ultimate ally in defying the pandemic? Pathogens and Global Health. 2020;114:279–280. doi: 10.1080/20477724.2020.1785199. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.United Nations Department of Economic and Social Affairs. World Population Prospects. Available from: https://population.un.org/wpp/Download/Files/1_Indicators%20(Standard)/CSV_FILES/WPP2019_TotalPopulationBySex.csv. [Last accessed on October 6th 2020] [Google Scholar]
- 7.World Bank World Development Indicators. Available from: https://databank.worldbank.org/reports.aspx?source=2. and [Last accessed on October 6th 2020] [Google Scholar]
- 8.Garcia Calzado MC, Garcia Rojas JF, Mangas Rojas A, et al. Tobacco and arterial pressure (II.). The acute effects on the angiotensin-converting enzyme. An Med Interna. 1990;7:392–395. [PubMed] [Google Scholar]
- 9.Kai H, Kai M. Interactions of coronaviruses with ACE2, angiotensin II, and RAS inhibitors-lessons from available evidence and insights into COVID-19. Hypertens Res. 2020;43:648–654. doi: 10.1038/s41440-020-0455-8. [DOI] [PMC free article] [PubMed] [Google Scholar]