

Coronavirus disease 2019 (COVID-19) is a serious illness caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2 or CoV-2). Some reports claimed certain nucleoside analogs to be active against CoV-2 and thus needed confirmation. Here, we evaluated a panel of compounds and identified novel nucleoside analogs with antiviral activity against CoV-2 and HCoV-OC43 while ruling out others. Of significance, sofosbuvir demonstrated no antiviral effect against CoV-2, and its triphosphate did not inhibit CoV-2 RNA polymerase.
KEYWORDS: SARS-CoV-2, HCoV-OC43, antiviral agents, nucleoside analogs, remdesivir, sofosbuvir, emtricitabine, lamivudine, COVID-19, Coronaviridae
ABSTRACT
Coronavirus disease 2019 (COVID-19) is a serious illness caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2 or CoV-2). Some reports claimed certain nucleoside analogs to be active against CoV-2 and thus needed confirmation. Here, we evaluated a panel of compounds and identified novel nucleoside analogs with antiviral activity against CoV-2 and HCoV-OC43 while ruling out others. Of significance, sofosbuvir demonstrated no antiviral effect against CoV-2, and its triphosphate did not inhibit CoV-2 RNA polymerase.
INTRODUCTION
Coronavirus disease 2019 (COVID-19) has emerged as a global pandemic with significant morbidity and mortality caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2 or CoV-2). CoV-2-infected individuals usually develop mild to severe flulike symptoms, whereas other individuals (particularly the elderly harboring underlying chronic health complications, such as diabetes and heart disease, or immunocompromised individuals) are particularly prone to develop severe to fatal clinical outcomes (1, 2). SARS-CoV-2 is an enveloped virus with a positive-sense single-stranded RNA genome, which belongs to the genus Betacoronavirus (3). Human coronavirus OC43 (HCoV-OC43) is also a member of the Betacoronavirus genus and thought to be the most commonly encountered human coronavirus (3). The search for anticoronavirus agents is highly desirable for a rapid response to this pandemic.
One of the main druggable targets for coronaviruses (including CoV-2) is the RNA-dependent RNA polymerase (RdRp). This viral polymerase displays similar catalytic mechanisms and some key conserved amino acids in the active site among various positive-sense RNA viruses (4). Nucleoside analogs are a well-established class of antiviral agents for treatment of many human viruses. Widely used antiviral drugs are nucleoside analogs, including emtricitabine (FTC; HIV-1/HBV [hepatitis B virus]), lamivudine (3TC; HIV-1/HBV), tenofovir disoproxil fumarate (TDF; HIV-1/HBV), tenofovir alafenamide (TAF; HIV/HBV), entecavir (HBV), telbivudine (HBV), and sofosbuvir (HCV [hepatitis C virus]) (5–8).
In this study, we evaluated a defined library of compounds consisting of approved and experimental antiviral nucleoside analogs for their potential in vitro antiviral activity against SARS-CoV-2 and HCoV-OC43 (Fig. 1). We selected several reported anti-HCV agents, such as 2′-C-methylcytidine (compound 2) (9), sofosbuvir (compound 4), a novel prodrug of sofosbuvir (compound 3) (10), and two 2′-dihalogeno nucleoside prodrugs (compounds 6 and 7) (11, 12). We also selected ALS-8112 (compound 5) (13), the active form of lumicitabine, a drug developed until recently for the treatment of respiratory syncytial virus (RSV) (14). Note that our group previously demonstrated that ALS-8112 is also an inhibitor of Nipah virus replication (15). Finally, 7-deaza-7-fluoro-2′-C-methyladenosine (compound 1), a nucleoside showing anti-yellow fever virus activity, was also evaluated (16, 17). Remdesivir (compound 10) (18) and β-d-N4-hydroxycytidine (NHC; compound 17) were used as positive drug controls for these studies (19). Additional compounds were selected from our in-house library of nucleoside analogs based on their effectiveness against HCV in vitro.
FIG 1.

Chemical structures of nucleoside analogs evaluated in culture.
All compounds were evaluated for their cell toxicity profiles using an MTS [3-(4,5-dimethylthiazol-2-yl)-5-(3-carboxymethoxyphenyl)-2-(4-sulfophenyl)-2H-tetrazolium] method (20). Briefly, we determined the half-maximal cytotoxic concentration (CC50) value in a panel of different cell lines, including human peripheral blood mononuclear cells (PBM), human hepatoma cells (Huh-7), human lymphoblastic cells (CEM), and African green monkey kidney cells (Vero CCL-81 cells; ATCC) by treatment of exponentially growing culture of each cell line for 4 days (Table 1). Based on the cytotoxicity data, we chose the nontoxic concentration (range, 2.5 to 20 μM) as the highest concentration for our antiviral assays in subsequent studies to avoid any minor toxicity of the compounds.
TABLE 1.
Primer and probe sequences
| Primer/probe | Sequence |
|---|---|
| SARS-CoV-2 | |
| Forward primer | 5′-GAC CCC AAA ATC AGC GAA AT-3′ |
| Reverse primer | 5′-TCT GGT TAC TGC CAG TTG AAT CTG-3′ |
| Probe | 5′-FAM-ACC CCG CAT TAC GTT TGG TGG ACC-BHQ1-3′ |
| HCoV-OC43 | |
| Forward primer | 5-ATG TTA GGC CGA TAA TTG AGG ACT AT-3′ |
| Reverse primer | 5′-FAM-CAT ACT CTG ACG GTC ACA AT-BHQ1-3′ |
| Probe | 5′-AAT GTA AAG ATG GCC GCG TAT T-3′ |
HCoV-OC43 was obtained from ATCC (Manassas, VA), and SARS-CoV-2 was provided by BEI Resources (NR-52281: USA-WA/2020). HCoV-OC43 and SARS-CoV-2 were propagated in Huh-7 and Vero cells, respectively, and titrated by the 50% tissue culture infective dose (TCID50) method, followed by storage of aliquots at −80°C until further use.
To determine the kinetic replication for each virus in cell culture, a confluent monolayer of each cell line in a 96-well microplate was inoculated at a multiplicity of infection (MOI) of 0.1 for SARS-CoV-2 (21) and HCoV-OC43, and the yield of progeny virus production was assessed at various time points using a specific reverse transcription-quantitative PCR (qRT-PCR) for each virus. Two separate qRT-PCR assays were established to quantify the yield of SARS-CoV-2 and HCoV-OC43 from our antiviral assays in the supernatant of the infected cells through the different time points postinfection (Fig. 2). Briefly, a one-step qRT-PCR was conducted in a final volume of 20 μl containing extracted viral RNA, probe/primer mix (Table 1), and qScript-Tough master mix (Quantibio, USA). Quantitative PCR measurement was performed using the StepOnePlus real-time PCR system (Roche, Germany) according to the manufacturer’s protocol.
FIG 2.

Virus replication kinetic in cell culture. Replication kinetics of SARS-CoV-2 in Vero cells (A) and HCoV-OC43 in Huh-7 cells (B).
To determine the best time point for the virus-yield assay, a kinetic replication of SARS-CoV-2 and HCoV-OC43 in Vero and Huh-7 cells, respectively, was performed, and the yield of progeny virus was assessed from the supernatant of viral infected cells at different-interval time points using specific qRT-PCR for each virus as mentioned earlier. We determined that 48 and 72 h postinfection were the optimum time points for SARS-CoV-2 and HCoV-OC43, respectively (Fig. 2), because there was no observed cell death and cytopathic effect on infected cells; and, more important, a significant increase in the virus RNA copy numbers that were harvested from the supernatant of the infected cells was observed at that time for SARS-CoV-2 and HCoV-OC43.
Next, we evaluated our compounds for their potential in vitro inhibitory effects against each virus using a virus-yield inhibition assay with qRT-PCR, as mentioned above. The resultant inhibitory effect of each test compound was calculated as a percentage of virus-yield inhibition. Briefly, a monolayer of Vero cells was prepared in a 96-well plate. The cells were then treated with a single nontoxic dose of each compound in triplicate and infected with CoV-2 at an MOI of 0.1 (21) and for HCOV-OC43 with 1 h of incubation followed by removal of inoculum and overlaying with cell culture medium containing the compounds. As a vehicle control, cells in three wells were treated with 0.1% dimethyl sulfoxide diluted in cell culture medium. The plate was kept at 37°C for 48 h in the presence of 5% CO2, which was followed by a virus-yield inhibition assay using qRT-PCR on harvested supernatants from the wells. We identified four nucleoside analogs (compounds 1 to 3 and 11), along with our positive controls (compounds 10 and 17), that yielded a strong inhibitory effect (>90% virus-yield decrease) from a nontoxic single dose against in vitro replication of CoV-2. In addition, these four compounds showed marked inhibitory effects against HCoV-OC43. Interestingly, compounds 6 and 7 exhibited antiviral activity against HCoV-OC43 but not against CoV-2. All active compounds were chosen for a subsequent dose-response study to determine their potency in culture (Fig. 3). Selected compounds were further assessed in a dose-dependent manner for their antiviral activity against SARS-CoV-2 and HCoV-OC43 using a virus-yield inhibition assay by determining the viral RNA copy number in collected supernatants 2 days posttreatment compared to the results from infected but untreated cells and noninfected and untreated cells as necessary controls (Table 2). All experiments were performed in triplicate, and each experiment was repeated three times independently to achieve reliable and statistically meaningful results.
FIG 3.

Dose-response antiviral activity. Dose response study of selected nucleoside analogs against SARS-CoV-2 in Vero cells (A) and HCoV-OC43 in Huh-7 cells (B). All experiments were done in triplicate.
TABLE 2.
Antiviral activity and cytotoxicity of compounds against SARS-CoV-2 and HCoV-OC43 in different cell lines
| Compound | Antiviral activity against (μM): |
Cytotoxicity (CC50 [μM]) |
||||||
|---|---|---|---|---|---|---|---|---|
| SARS-CoV-2 |
HCoV-OC43 |
|||||||
| Vero cells |
Huh7 cells |
|||||||
| EC50 | EC90 | EC50 | EC90 | PBM | CEM | Vero | Huh7 | |
| 1 (2′-MeC) | 9.2 0.1 | 29.6 0.4 | 10 0.7 | 15.1 0.1 | 65.4 | 84.3 | >100 | >100 |
| 2 | 7.6 0.4 | 28.8 0.8 | 6.7 1.1 | 13.8 0.2 | 72.4 | 63.9 | >100 | 38 |
| 3 (sofosbuvir cyclic phosphate prodrug) | 6.3 0.1 | 18.9 0.2 | >2a | NDb | 58.4 | 31.6 | 16.4 | 2.9 |
| 4 (sofosbuvir) | >20 | >20 | >20 | >20 | >100 | >100 | >100 | >100 |
| 5 (ALS-8112, lumicitabine) | >20 | >20 | >20 | >20 | 4.2 | 2.8 | >100 | 4.2 |
| 6 | >20 | >20 | 6.8 0.2 | 12.8 0.4 | >100 | >100 | >100 | 72.4 |
| 7 | >20 | >20 | 5.9 0.6 | 18.6 0.3 | >100 | >100 | >100 | >100 |
| 8 (favipiravir) | >20 | >20 | 6.8 | >10 | >100 | >100 | >100 | >100 |
| 9 (entecavir) | >20 | >20 | >20 | >20 | 21.5 | >100 | >100 | >100 |
| 10 (remdesivir) | 1.0 0.1 | 3.5 0.3 | 0.04 0.1 | 0.09 0.09 | 4.5 | 11.6 | >100 | 2.1 |
| 11 (parent nucleoside of remdesivir, GS-441524) | 8.2 ± 0.4 | 13.2 ± 0.8 | >10 | >20 | >100 | >100 | >100 | >100 |
| 12 (ribavirin) | >20 | >20 | 20.6 | >20 | >100 | 7.5 | >100 | 22.1 |
| 13 (3TC) | >20 | >20 | >20 | >20 | >100 | >100 | >100 | >100 |
| 14 (FTC) | >20 | >20 | >20 | >20 | >100 | >100 | >100 | >100 |
| 15 (TAF) | >20 | >20 | >20 | >20 | 50.8 | 13.67 | 36.4 | >100 |
| 16 (TDF) | >20 | >20 | >20 | >20 | 44.4 | 33.9 | >100 | >100 |
| 17 (NHC) | 0.3 ± 0.2 | 0.8 ± 0.1 | 0.8 ± 0.03 | 1.8 ± 0.1 | 44.3 | 3.5 | 12.6 | 80.3 |
To avoid the cytotoxicity, 2 μM was chosen as the highest concentration for antiviral assays for compound 3 for HCoV-OC43 in Huh-7 cells.
ND, not determined.
The median effective concentration (EC50) and the concentration with 90% of inhibitory effect (EC90) were calculated using GraphPad Prism for Mac, version 7 (GraphPad Software Inc., San Diego, CA) and reported as the mean ± standard deviation. The selectivity index (SI) for each effective compound was calculated as CC50/EC50.
In this study, the reference compounds remdesivir and NHC displayed EC50 values of 1.0 and 0.3 μM, respectively, against SARS-CoV-2 in Vero cells, similar to data reported in the literature (19, 22). Note, however, that appreciable toxicity was observed in human PBM and CEM cells (CC50, 4.5 and 11.6 μM, respectively) for remdesivir, narrowing the therapeutic index of this compound. Cytotoxicity in the low micromolar range was also observed for NHC in our panel of cell lines (Table 2). This toxicity may be related to the high mutagenic activity of NHC and/or other factors (23, 24). Anti-RSV compound ALS-8112 (compound 5) and compounds 6 and 7 did not have a marked effect on CoV-2 replication up to 20 μM. Sofosbuvir showed weak (40% inhibition) antiviral activity at 20 μM against CoV-2 in Vero cells. Several studies using molecular modeling suggested that sofosbuvir could be used to treat COVID-19 patients (25, 26). Surprisingly, no enzymatic or cell culture antiviral data were presented in either paper to support their modeling data. To confirm that sofosbuvir is inactive against CoV-2, we determined that the active 5′-triphosphate precursor of sofosbuvir (namely, β-d-2′-fluoro-2′-methyluridine-5′-triphosphate) did not inhibit purified CoV-2 polymerase up to 10 μM (see the supplemental material and Fig. 4, lane 6) while the precursor of remdesivir inhibited the polymerase (Fig. 4, lane 7). We also confirmed that the lack of activity was not related to a cell transport or a prodrug cleavage issue by evaluating sofosbuvir against CoV-2 and HCoV-OC43 in various cells in addition to those mentioned above. We did not observe any significant activity in some cells, including human rhabdomyosarcoma (RD), human intestinal (Caco-2), and human lung (Calu3) cells, with an EC50 of >20 μM for all three cell lines. Note that a novel thio-prodrug of sofosbuvir (compound 3; cyclic phosphate prodrug of sofosbuvir) (Fig. 1), previously reported to be more potent than sofosbuvir itself against HCV (10), displayed an EC50 of 6.3 μM and against SARS-CoV-2 was ∼6 times less potent than remdesivir (6.3 versus 1.0 μM). However, the activity observed for that compound is likely secondary to the toxicity noted in Vero cells (CC50, 16.4 μM). This compound was tested against HCoV-OC43 in Huh-7 cells in a dose-dependent manner, but because of the toxicity of the compound observed in Huh-7 cells (CC50, 2.9 μM), the highest concentration chosen for the antiviral assays was 2 μM (Table 2). 2′-C-methylcytidine (compound 1) and 7-deaza-7-fluoropurine derivative (compound 2) exhibited activities in the single-digit micromolar range (EC50, 9.2 μM [SI >10] and 7.6 μM [SI >10], respectively) with no toxicity in Vero cells up to 100 μM.
FIG 4.
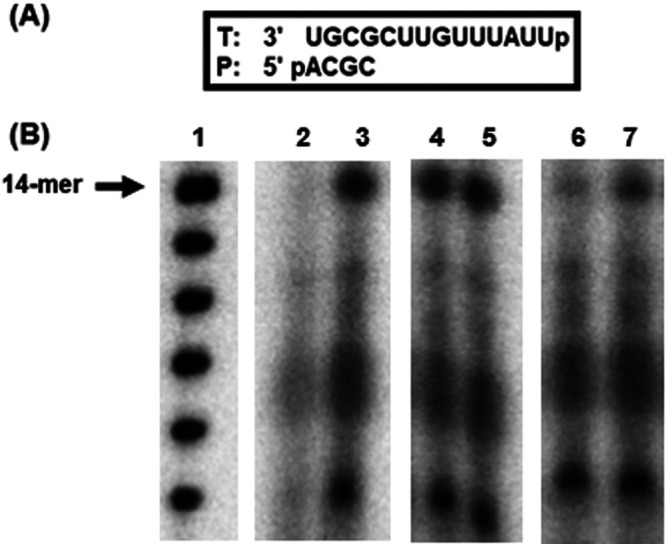
SARS-CoV-2 RdRp inhibition by triphosphate forms of sofosbuvir and remdesivir. (A) RNA 4-mer primer/14-mer template used in the RdRp reactions. (B) Full-length 14-mer RNA product syntheses by SARS-CoV-2 RdRp in the presence/absence of each compound. Respective lanes were labeled as indicated: 1, size marker; 2, no enzyme control; 3, SARS-CoV-2 RdRp control reaction without inhibitors; 4 and 5, SARS-CoV-2 RdRp reactions with 10 μM and 1 μM sofosbuvir triphosphate; 6 and 7, SARS-CoV-2 RdRp reactions with 10 μM and 1 μM remdesivir triphosphate.
Since the global onset of COVID-19, several studies have been conducted to evaluate the effects of nucleoside analogs or their bases against CoV-2. A recent study suggested that favipiravir, an approved anti-influenza drug acting as a guanine nucleoside analog, may be a potential candidate for the treatment of SARS-CoV-2 infection, showing effective antiviral activity in vitro in Vero cells, with a reported EC50 of 61.9 μM (27). Favipiravir is being studied in two separate clinical trials in combination therapy with other antiviral agents, such as interferon-α or baloxavir marboxil (28). However, our data showed that favipiravir (compound 8) did not exhibit significant in vitro activity against SARS-CoV-2 and HCoV-OC43 up to 20 μM (Table 2). Therefore, this drug is unlikely to be promising for COVID-19 treatment unless large amounts are administered safely to achieve blood levels in the double-digit micromolar range. Ribavirin (compound 12), another approved nucleoside analog for HCV infections, has been considered for COVID-19 treatment. It was shown that ribavirin inhibited SARS-CoV-2 replication in Vero cells, with an EC50 of 109.5 μM (22); and according to our findings, this compound up to 20 μM just showed a 12% inhibitory effect against CoV-2 in vitro with concomitant cytotoxicity in human cells (Table 2). Notably, ribavirin has been used to treat people infected with SARS or Middle East respiratory syndrome (MERS) without successful clinical outcome (29, 30). Furthermore, there are well-known significant side effects reported for this drug, including anemia at high doses, and efficacy and safety of the drug are uncertain (30). Nevertheless, ribavirin is being used for COVID-19 treatment in combination with pegylated interferon (31). However, our cell-based data showed that ribavirin did not exhibit a marked inhibitory effect against both coronaviruses tested (Table 2). Some scientists speculated that 3TC/FTC plus TDF/TAF may contribute to lower COVID-19 incidence and severity among people living with HIV (32). However, in our hands, 3TC, FTC, TAF, and TDF (compounds 13 through 16) did not show any activity against CoV-2 or HCoV-OC43 when tested up to 20 μM. These data indicate that it is unlikely these drugs would have any clinical benefit in COVID-19-infected individuals (Table 2).
As expected, the two positive controls used, i.e., remdesivir and NHC, demonstrated activity in culture against CoV-2. Others have shown that compound 11 (GS-441524), the parent nucleoside of remdesivir, is more potent than remdesivir in Vero E6 cells, with EC50s of 0.47 and 1.85 μM, respectively (33). However, in our study, compound 11 showed weak activity against SARS-CoV-2 and no activity against HCoV-OC43 (EC50, 8.2 μM [SI = 12] and >10 μM) compared to remdesivir (EC50, 1.0 μM [SI >100] and 0.04 μM [SI = 52] against SARS-CoV-2 and HCoV-OC43, respectively) (Table 2). Remdesivir, a nucleoside analog originally developed for HCV, was recently studied in humans for the treatment of Ebola virus (34) and showed antiviral activity against SARS-CoV-2 in culture (33). There are clinical trials showing the benefit of remdesivir in COVID-19-infected patients (35, 36). In one of the largest NIH-sponsored studies, involving 1,063 hospitalized patients, those that received the drug recovered in 11 days compared with 15 days for those who received placebo (P < 0.0001). The data also suggested a reduction in mortality on treatment, but it was not significant. Despite a controversial unpublished non-peer-reviewed open-label WHO SOLIDARITY trial reporting that remdesivir had no effect on mortality and apparently no clinical benefit (https://www.who.int/emergencies/diseases/novel-coronavirus-2019/global-research-on-novel-coronavirus-2019-ncov/solidarity-clinical-trial-for-covid-19-treatments), the FDA approved Veklury (remdesivir) on 23 October 2020 as the first treatment for COVID-19 (https://www.fda.gov/news-events/press-announcements/fda-approves-first-treatment-covid-19) for use in adult and pediatric patients aged ≥12 years and weighing at least 40 kg for patients requiring hospitalization. Finally, EIDD-2801, the ester prodrug of NHC (EIDD-1931) has antiviral activity against different coronaviruses, including SARS-CoV-2 (19). The parent molecule (NHC) was active in our study (Table 2), with an EC50 of 0.3 μM and SI of 42 for SARS-CoV-2 and an EC50 of 0.8 μM and SI of 100 for HCoV-OC43. However, this molecule is known to be mutagenic (23, 24), suggesting that reproductive toxicology will be needed going forward with EIDD-2801 into the clinic.
In conclusion, the work presented here should help eliminate some of the muddied information in the literature and provide guidance to decision makers and clinicians on which repurposed drug to advance efficiently toward FDA approval for a COVID-19 indication. Too many drugs are being tested in humans as antiviral agents without prior evaluation in cell culture. Additional modifications of repurposed nucleoside antiviral agents, with similar backbones found to be effective herein, could potentially offer improved potency and therapeutic options to reduce the global burden of COVID-19.
Supplementary Material
ACKNOWLEDGMENTS
This work was supported in part by NIH grant RO1-AI-141327 and Center for AIDS NIH grant P30-AI-050409.
We thank James Kohler for critical review of the paper.
Footnotes
Supplemental material is available online only.
REFERENCES
- 1.Bai Z, Gong Y, Tian X, Cao Y, Liu W, Li J. 2020. The rapid assessment and early warning models for COVID-19. Virol Sin 35:272–279. doi: 10.1007/s12250-020-00219-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Li H, Liu SM, Yu XH, Tang SL, Tang CK. 2020. Coronavirus disease 2019 (COVID-19): current status and future perspective. Int J Antimicrob Agents 55:105951. doi: 10.1016/j.ijantimicag.2020.105951. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Rajapakse N, Dixit D. 2020. Human and novel coronavirus infections in children: a review. Paediatr Int Child Health 25:1–20. doi: 10.1080/20469047.2020.1781356. [DOI] [PubMed] [Google Scholar]
- 4.Pruijssers AJ, Denison MR. 2019. Nucleoside analogues for the treatment of coronavirus infections. Curr Opin Virol 35:57–62. doi: 10.1016/j.coviro.2019.04.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Schinazi RF, Chu CK, Peck A, McMillan A, Mathis R, Cannon D, Jeong LS, Beach JW, Choi WB, Yeola S. 1992. Activities of the four optical isomers of 2',3'-dideoxy-3'-thiacytidine (BCH-189) against human immunodeficiency virus type 1 in human lymphocytes. Antimicrob Agents Chemother 36:672–676. doi: 10.1128/aac.36.3.672. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Lopatin U. 2019. Drugs in the pipeline for HBV. Clin Liver Dis 23:535–555. doi: 10.1016/j.cld.2019.04.006. [DOI] [PubMed] [Google Scholar]
- 7.Bhatia HK, Singh H, Grewal N, Natt NK. 2014. Sofosbuvir: a novel treatment option for chronic hepatitis C infection. J Pharmacol Pharmacother 5:278–284. doi: 10.4103/0976-500X.142464. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Schinazi RF. 2003. Emtricitabine: a viewpoint. Drugs 63:2425–2426. doi: 10.2165/00003495-200363220-00004. [DOI] [Google Scholar]
- 9.Pierra C, Amador A, Benzaria S, Cretton-Scott E, D'Amours M, Mao J, Mathieu S, Moussa A, Bridges EG, Standring DN, Sommadossi JP, Storer R, Gosselin G. 2006. Synthesis and pharmacokinetics of valopicitabine (NM283), an efficient prodrug of the potent anti-HCV agent 2'-C-methylcytidine. J Med Chem 49:6614–6620. doi: 10.1021/jm0603623. [DOI] [PubMed] [Google Scholar]
- 10.Bradshaw CW, Sakamuri S, Liu D. 16 June 2016. Mononucleotides having a bioreversible disulfide group. Patent WO2016094677.
- 11.Mengshetti S, Zhou L, Sari O, De Schutter C, Zhang H, Cho JH, Tao S, Bassit LC, Verma K, Domaoal RA, Ehteshami M, Jiang Y, Ovadia R, Kasthuri M, Ollinger Russell O, McBrayer T, Whitaker T, Pattassery J, Pascual ML, Uher L, Lin BY, Lee S, Amblard F, Coats SJ, Schinazi RF. 2019. Discovery of a series of 2'-α-fluoro,2'-β-bromo-ribonucleosides and their phosphoramidate prodrugs as potent pan-genotypic inhibitors of hepatitis C virus. J Med Chem 62:1859–1874. doi: 10.1021/acs.jmedchem.8b01300. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Zhou S, Mahmoud S, Liu P, Zhou L, Ehteshami M, Bassit L, Tao S, Domaoal RA, Sari O, Schutter C, Amiralaei S, Khalil A, Ollinger Russell O, McBrayer T, Whitaker T, Abou-Taleb N, Amblard F, Coats SJ, Schinazi RF. 2017. 2'-Chloro,2'-fluoro ribonucleotide prodrugs with potent pan-genotypic activity against hepatitis C virus replication in culture. J Med Chem 60:5424–5437. doi: 10.1021/acs.jmedchem.7b00067. [DOI] [PubMed] [Google Scholar]
- 13.Wang G, Deval J, Hong J, Dyatkina N, Prhavc M, Taylor J, Fung A, Jin Z, Stevens SK, Serebryany V, Liu J, Zhang Q, Tam Y, Chanda SM, Smith DB, Symons JA, Blatt LM, Beigelman L. 2015. Discovery of 4'-chloromethyl-2'-deoxy-3',5'-di-O-isobutyryl-2'-fluorocytidine (ALS-8176), a first-in-class RSV polymerase inhibitor for treatment of human respiratory syncytial virus infection. J Med Chem 58:1862–1878. doi: 10.1021/jm5017279. [DOI] [PubMed] [Google Scholar]
- 14.Boreko I, Pavlova NI, Zaĭtseva GV, Mikhaĭlopulo IA. 2001. Antiviral activity of 2'-deoxy-2'-fluoroguanosine against influenza and herpes simplex viruses in cultured cells. Vopr Virusol 46:40–42. (In Russian.) [PubMed] [Google Scholar]
- 15.Lo MK, Amblard F, Flint M, Chatterjee P, Kasthuri M, Li C, Russell O, Verma K, Bassit L, Schinazi RF, Nichol ST, Spiropoulou CF. 2020. Potent in vitro activity of β-D-4'-chloromethyl-2'-deoxy-2'-fluorocytidine against Nipah virus. Antiviral Res 175:104712. doi: 10.1016/j.antiviral.2020.104712. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Eldrup AB, Prhavc M, Brooks J, Bhat B, Prakash TP, Song Q, Bera S, Bhat N, Dande P, Cook PD, Bennett CF, Carroll SS, Ball RG, Bosserman M, Burlein C, Colwell LF, Fay JF, Flores OA, Getty K, LaFemina RL, Leone J, MacCoss M, McMasters DR, Tomassini JE, Von Langen D, Wolanski B, Olsen DB. 2004. Structure-activity relationship of heterobase-modified 2'-C-methyl ribonucleosides as inhibitors of hepatitis C virus RNA replication. J Med Chem 47:5284–5297. doi: 10.1021/jm040068f. [DOI] [PubMed] [Google Scholar]
- 17.Zandi K, Amblard F, Amichai S, Bassit L, Tao S, Jiang Y, Zhou L, Ollinger Russell O, Mengshetti S, Schinazi RF. 2019. Nucleoside analogs with antiviral activity against yellow fever virus. Antimicrob Agents Chemother 63:e00889-19. doi: 10.1128/AAC.00889-19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Siegel D, Hui HC, Doerffler E, Clarke MO, Chun K, Zhang L, Neville S, Carra E, Lew W, Ross B, Wang Q, Wolfe L, Jordan R, Soloveva V, Knox J, Perry J, Perron M, Stray KM, Barauskas O, Feng JY, Xu Y, Lee G, Rheingold AL, Ray AS, Bannister R, Strickley R, Swaminathan S, Lee WA, Bavari S, Cihlar T, Lo MK, Warren TK, Mackman RL. 2017. Discovery and synthesis of a phosphoramidate prodrug of a pyrrolo[2,1-f][triazin-4-amino] adenine C-nucleoside (GS-5734) for the treatment of Ebola and emerging viruses. J Med Chem 60:1648–1661. doi: 10.1021/acs.jmedchem.6b01594. [DOI] [PubMed] [Google Scholar]
- 19.Sheahan TP, Sims AC, Zhou S, Graham RL, Pruijssers AJ, Agostini ML, Leist SR, Schäfer A, Dinnon KH, Stevens LJ, Chappell JD, Lu X, Hughes TM, George AS, Hill CS, Montgomery SA, Brown AJ, Bluemling GR, Natchus MG, Saindane M, Kolykhalov AA, Painter G, Harcourt J, Tamin A, Thornburg NJ, Swanstrom R, Denison MR, Baric RS. 2020. An orally bioavailable broad-spectrum antiviral inhibits SARS-CoV-2 in human airway epithelial cell cultures and multiple coronaviruses in mice. Sci Transl Med 12:eabb5883. doi: 10.1126/scitranslmed.abb5883. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Cory AH, Owen TC, Barltrop JA, Cory JG. 1991. Use of an aqueous soluble tetrazolium/formazan assay for cell growth assays in culture. Cancer Commun 3:207–212. doi: 10.3727/095535491820873191. [DOI] [PubMed] [Google Scholar]
- 21.Gordon DE, Jang GM, Bouhaddou M, Xu J, Obernier K, White KM, O'Meara MJ, Rezelj VV, Guo JZ, Swaney DL, Tummino TA, Hüttenhain R, Kaake RM, Richards AL, Tutuncuoglu B, Foussard H, Batra J, Haas K, Modak M, Kim M, Haas P, Polacco BJ, Braberg H, Fabius JM, Eckhardt M, Soucheray M, Bennett MJ, Cakir M, McGregor MJ, Li Q, Meyer B, Roesch F, Vallet T, Mac Kain A, Miorin L, Moreno E, Naing ZZC, Zhou Y, Peng S, Shi Y, Zhang Z, Shen W, Kirby IT, Melnyk JE, Chorba JS, Lou K, Dai SA, Barrio-Hernandez I, Memon D, Hernandez-Armenta C, Lyu J, Mathy CJP, et al. 2020. A SARS-CoV-2 protein interaction map reveals targets for drug repurposing. Nature 583:459–468. doi: 10.1038/s41586-020-2286-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Wang M, Cao R, Zhang L, Yang X, Liu J, Xu M, Shi Z, Hu Z, Zhong W, Xiao G. 2020. Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro. Cell Res 30:269–271. doi: 10.1038/s41422-020-0282-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Stuyver LJ, Whitaker T, McBrayer TR, Hernandez-Santiago BI, Lostia S, Tharnish PM, Ramesh M, Chu CK, Jordan R, Shi J, Rachakonda S, Watanabe KA, Otto MJ, Schinazi RF. 2003. Ribonucleoside analogue that blocks replication of bovine viral diarrhea and hepatitis C viruses in culture. Antimicrob Agents Chemother 47:244–254. doi: 10.1128/aac.47.1.244-254.2003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Negishi K, Harada C, Ohara Y, Oohara K, Nitta N, Hayatsu H. 1983. N4-aminocytidine, a nucleoside analog that has an exceptionally high mutagenic activity. Nucleic Acids Res 11:5223–5233. doi: 10.1093/nar/11.15.5223. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Jácome R, Campillo-Balderas JA, Ponce de León S, Becerra A, Lazcano A. 2020. Sofosbuvir as a potential alternative to treat the SARS-CoV-2 epidemic. Sci Rep 10:9294. doi: 10.1038/s41598-020-66440-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Elfiky AA. 2020. Anti-HCV, nucleotide inhibitors, repurposing against COVID-19. Life Sci 248:117477. doi: 10.1016/j.lfs.2020.117477. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Eloy P, Solas C, Touret F, Mentré F, Malvy D, de Lamballerie X, Guedj J. 2020. Dose rationale for favipiravir use in patients infected with SARS-CoV-2. Clin Pharmacol Ther 108:188. doi: 10.1002/cpt.1877. [DOI] [PubMed] [Google Scholar]
- 28.Martinez MA. 2020. Clinical trials of repurposed antivirals for SARS-CoV-2. Antimicrob Agents Chemother 64:e01101-20. doi: 10.1128/AAC.01101-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Cinatl J, Michaelis M, Hoever G, Preiser W, Doerr HW. 2005. Development of antiviral therapy for severe acute respiratory syndrome. Antiviral Res 66:81–97. doi: 10.1016/j.antiviral.2005.03.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Al-Tawfiq JA, Momattin H, Dib J, Memish ZA. 2014. Ribavirin and interferon therapy in patients infected with the Middle East respiratory syndrome coronavirus: an observational study. Int J Infect Dis 20:42–46. doi: 10.1016/j.ijid.2013.12.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Dong L, Hu S, Gao J. 2020. Discovering drugs to treat coronavirus disease 2019 (COVID-19). Drug Discov Ther 14:58–60. doi: 10.5582/ddt.2020.01012. [DOI] [PubMed] [Google Scholar]
- 32.Del Amo J, Polo R, Moreno S, Díaz A, Martínez E, Arribas JR, Jarrín I, Hernán MA. 2020. Incidence and severity of COVID-19 in HIV-positive persons receiving antiretroviral therapy: a cohort study. Ann Intern Med 173:536–541. doi: 10.7326/M20-3689. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Pruijssers AJ, George AS, Schäfer A, Leist SR, Gralinksi LE, Dinnon KH, 3rd, Yount BL, Agostini ML, Stevens LJ, Chappell JD, Lu X, Hughes TM, Gully K, Martinez DR, Brown AJ, Graham RL, Perry JK, Du Pont V, Pitts J, Ma B, Babusis D, Murakami E, Feng JY, Bilello JP, Porter DP, Cihlar T, Baric RS, Denison MR, Sheahan TP. 2020. Remdesivir inhibits SARS-CoV-2 in human lung cells and chimeric SARS-CoV expressing the SARS-CoV-2 RNA polymerase in mice. Cell Rep 32:107940. doi: 10.1016/j.celrep.2020.107940. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Hoenen T, Groseth A, Feldmann H. 2019. Therapeutic strategies to target the Ebola virus life cycle. Nat Rev Microbiol 17:593–606. doi: 10.1038/s41579-019-0233-2. [DOI] [PubMed] [Google Scholar]
- 35.Paladugu S, Donato AA. 2020. Remdesivir improved time to recovery in adults hospitalized with COVID-19 and lower respiratory tract involvement. Ann Intern Med 173:JC4. doi: 10.7326/ACPJ202007210-005. [DOI] [PubMed] [Google Scholar]
- 36.Beigel JH, Tomashek KM, Dodd LE. 2020. Remdesivir for the treatment of Covid-19—preliminary report. Reply. N Engl J Med 383:994. doi: 10.1056/NEJMc2022236. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.