

Abstract
Introduction and Objectives:
Diabetic foot is the most common complication among 50% diabetic patients. Evidence exists that with the self-care, the incidence of foot ulcers and toe amputation can be decreased significantly. Hence, the current study was planned to assess knowledge and foot care practice among diabetic patients attending primary care centre in Saudi Arabia.
Methodology:
This prospective cross-sectional study was conducted at a Primary Care Center in Security Forces Hospital of Riyadh. Consecutive sampling was used to enrol 350 diabetic patients. Information on demographics, knowledge and practice of footcare was collected through standardized and pre-tested self-administered questionnaire. Data were entered and analysed using SPSS V 22.0 software.
Results:
Out of 350 patients aged 18 years and more, 170 (46.7%) belonged to age group of 46-60 years; mostly males (n = 185, 53.9%). The foot complications were absent among 57.9% patients, 35.5% having numbness, 4.3% having a history of healed ulcer and 2.3% reported toe amputation. More than 65% patients were certain about their knowledge regarding foot self-care. There was no statistically significant difference in the knowledge among males and females. The practice of self-care of feet was statistically significantly different among males and females regarding self-inspection of feet on regular basis as well as daily moisturizing of their feet.
Conclusions:
Both knowledge and practice levels were low among diabetic patients which needs to be strengthened through regular counselling sessions. There is a pressing need to spread awareness on this important aspect of morbidity and mortality which can be addressed with minimal resources.
Keywords: Diabetes mellitus, knowledge, practice, self care
Introduction
The global prevalence of Diabetes Mellitus (DM) has been estimated to increase by 7.7% affecting 439 million by 2030[1] and 642 million by 2040[2]; with current burden of affecting more than 400 million adults in 2014 with a predilection for old people (>65 years).[3] The multifaceted disease has been attributed to sedentary lifestyles, urbanisation and ageing.[4,5] The most common complication among 50% of diabetic patients is diabetic foot[6,7] and attributing to 80% of all non-traumatic lower limb amputations.[8]
The major etiological factors in diabetic foot abnormalities development are mechanical stress, neuropathy and angiopathy.[9] Sensory neuropathy results in reduction of sensation making foot more prone to trauma eventually leading to skin breakdown and foot ulcer formation. It is estimated globally that foot ulcers have an incidence of 8%-17% among diabetic patients.[10] Diabetic Foot has been as the foot of diabetic patients with ulceration, infection and/or destruction of the deep tissues, associated with neurological abnormalities and various degrees of peripheral vascular disease in the lower limb.[11]
A recent meta-analysis estimated the global burden of diabetic foot ulcer (DFU), to be 6.3% with higher predilection among males, and DM type 2 patients.[12] Global prevalence is estimated highest among North Americans natives (13%).[7] The prevalence rate varied from 3% in Oceania, 7.2% in Africa, 5.1% in Europe, 1.5% in Australia and 5.5% in Asia.[7] The prevalence was reportedly higher in countries like Canada and Belgium. Among Asian countries, India alone accounted for 11.6% of DFU.[7]
Saudi Arabia accounts for being the second highest country in Middle East[13] for diabetic patients with varying prevalence of DFU ranging from 26%-61.8% as per studies conducted in the past.[14,15] It is estimated that this multifaceted disease accounts for 5% of total deaths in Saudi Arabia.[16] A registry based data of Saudi estimated foot complications among 3.3% of diabetic patients with majority having foot ulcer.[17] The foot ulcer is often succeeded by complications and deterioration of quality of life. Along with this, it adds to hospital expenditure as well with nearly 35% of all hospital admissions attributing to this in diabetic specialized clinics.[18] Globally studies conducted on cost factor in diabetic foot treatment in US, European countries like France, Belgium; have shown massive direct and indirect expenditure for treatment of DFUs.[19,20,21,22] A recent study conducted in India showed expenses of US$1960 for the treatment of DFUs.[23] Burden in terms of cost of treatment is seen in UAE as well owing to faster rise in prevalence of DM as compared to rest of world and middle east region.[13]
However, these complications can be curbed in diabetic foot with proper preventive measures and prophylaxis care. The Diabetes Committee of the American Orthopaedic Foot and Ankle Society have developed guidelines for prophylactic foot care which includes timely screening, patient education and treatment.[24] Lacunae have been witnessed in patients awareness and education levels about early detection and self- management. Saudi Arabia with the second highest incidence of DM in middle east and seventh highest in the world faces an alarming situation. In the past few studies have been conducted in middle east, sparsity of literature required the need of further research. With this Background, the current study will assess knowledge and foot care practice in diabetic patients attending primary care centre in Saudi Arabia.
Aim
To evaluate the level of knowledge and practice towards foot self-care among diabetic patients attending primary care center in Security Forces Hospital, Riyadh, Saudi Arabia.
Objectives:
- To assess the knowledge level about foot self-care among diabetic patients.
- To assess foot self-care practice among diabetic patients.
- To compare the level of knowledge about foot self-care between males and females.
Methodology
This prospective crossectional study was conducted from year 2018 To 2019 among diabetic patients attending Primary Care Center at Security Forces Hospital in Riyadh. All the patients above 18 years of age diagnosed with Type 1 or Type 2 diabetes who provided their consent were included in the study.
The Raosoft calculator was used to estimate the sample size by assuming the target population to be more than 20,000 subjects using a confidence level of 95%, and a margin of error of 5%, the minimum sample size required for this study was 350. We used convenience sampling technique, which is a type of non-probability sampling to achieve our sample size.
We used a validated and reliable self-administered questionnaire that evaluated the knowledge and practice of foot self-care among diabetic patients. The questionnaire was translated to Arabic and back-translated to English. This process was repeated until a satisfactory version of the questionnaire was reached. The questionnaire was pre-tested among 20 patients before the start of actual survey. This helped to establish the reliability and flow of questions.
A hard-copy of this self- administered questionnaire was distributed to the subjects in waiting areas in the Primary Care Center for final data collection. It took about 15 minutes on an average to fill the questionnaire. In case of doubt or non-clarity regarding the question, the author facilitated the participant for filling the form.
The collected data was entered and analyzed using SPSS v. 22.0 software. Descriptive analysis of numerical data was carried out to express it as mean (standard deviation). Categorical variables were expressed as numbers and their percentages. Analytical analysis was done by using Chi square test of significance to study the relationship between categorical variables. P value less than or equal to 0.05 was considered to be statistically significant.
Ethical consideration
The ethical clearance of the study was obtained from the Research Ethics Committee at Security Forces Hospital, Riyadh, before starting the study. It was assured to keep all the collected information to be confidential. And would be used only for research purpose.
Results
The number of patients enrolled in the study was 350. Out of them, 158 (46.1%) were females. The information on type of diabetes was available for 276 patients, out of which, 55.1% (n = 152) were type 1 diabetic. Nearly 98.8% (n = 338) patients out of 342 who had information on the duration of diabetes, were suffering from the same for less than or equal to 10 years [Table 1].
Table 1.
Demographic characteristics of the diabetic patients (N=350)
| Characteristic | Number | Percent | |
|---|---|---|---|
| Age (years) (N=349) | 18–30 | 37 | 10.6 |
| 31–45 | 65 | 18.6 | |
| 46–60 | 170 | 48.7 | |
| 61–75 | 77 | 22.1 | |
| Gender (N=343) | Females | 158 | 46.1 |
| Males | 185 | 53.9 | |
| Type of diabetes (N=276) | Type 1 | 152 | 55.1 |
| Type 2 | 124 | 44.9 | |
| Duration of diabetes (N=342) | less than or equal 10 years | 338 | 98.8 |
| More than 10 years | 4 | 1.2 | |
| Type of treatment for diabetes (N=348) | Diet/oral agent | 192 | 55.2 |
| Insulin oral agent | 90 | 25.8 | |
| Insulin | 66 | 19.0 | |
| Foot complication among diabetic patients (N=349) | Numbness | 124 | 35.5 |
| History of healed ulcer One toe amputation | 15 8 | 4.3 2.3 | |
| None | 202 | 57.9 | |
| Status of HBA1c (N=340) | Controlled | 194 | 57.1 |
| Uncontrolled | 146 | 42.9 |
Majority of the diabetics were following the treatment regimen including diet and/or oral agent. Nearly 35.5% (n = 124) patients had complication of foot numbness, followed by 4.3% (n = 15) having history of healed ulcers. Around 2.3% (n = 8) patients have had one toe amputation. [Figure 1].
Figure 1.
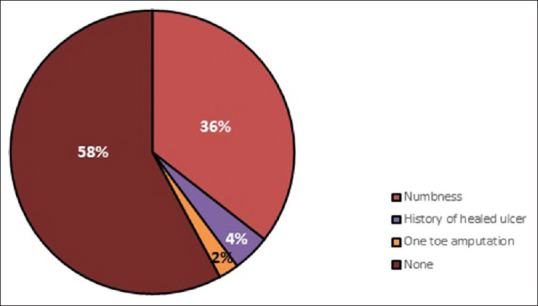
Diabetic Foot Complications Among Patients (N = 349)
The diabetic patients were having varied responses in relation to the knowledge regarding foot self-care. Majority of the patients (more than 65%) were certain about their knowledge regarding foot self-care. However, 34.3% (n = 120) patients were either having no idea or perceived it to be false about looking after their feet because they may not feel a minor injury to their feet. Similar was the case with knowledge about not smoking (n = 113, 32.3%) as it causes poor circulation which affects feet. A similar number (n = 119, 34.0%) either did not have knowledge or perceived it to be a false claim about looking after their feet because they are more prone to flat foot. One hundred thirty (37.1%) patients had similar perception as above about the fact that they have to look after their feet because they may get a foot ulcer. [Table 2].
Table 2.
Knowledge about self-practice of foot care among diabetes patients
| Knowledge indicator | Response | |
|---|---|---|
| True | False/don’t know | |
| Look after their feet because they may not feel a minor injury to their feet | 230 (65.7%) | 120 (34.3%) |
| Look after their feet because wounds and infection may not heal quickly | 270 (77.1%) | 80 (22.9%) |
| Look after their feet because they may get a foot ulcer | 220 (62.9%) | 130 (37.1%) |
| Do not smoke because smoking causes poor circulation and affects the feet | 237 (67.7) | 113 (32.3%) |
| Look after their feet because they are more prone to flat foot | 231 (66.0%) | 119 (34.0%) |
| Take medication regularly because they are liable to get DM complication | 309 (88.3%) | 41 (11.7%) |
Only 98 (28.0%) patients practiced the self-examination or inspection of their feet on a regular basis. Around 20.9% (n = 73) patients reported that they never practice the careful drying between the toes after washing their feet. Around 17.7% (n = 62) patients never continuously wore the cotton socks. Two hundred one patients (57.6%) would at times walk outside barefoot. The regular cutting of sex toenails every 2 weeks was being practiced by 199 (56.9%) patients [Table 3]. The difference in knowledge about foot self-care was not statistically significantly different among males and females [Table 4].
Table 3.
Practice of self-care of foot among diabetes patients
| Practice indicator | Response | ||
|---|---|---|---|
| Always | Rarely/sometimes | Never | |
| Do you examine/inspect your feet on a regular basis? | 98 (28.0%) | 214 (61.1%) | 38 (10.9%) |
| Do you check your shoes before you put them on? | 132 (37.7%) | 195 (55.7%) | 23 (6.6%) |
| Do you walk outside barefoot? | 21 (6.0%) | 201 (57.6%) | 127 (36.4%) |
| Do you wash your feet with warm water daily? | 117 (33.4%) | 187 (53.4%) | 46 (13.1%) |
| Do you carefully dry between toes after washing your feet? | 84 (24.0%) | 193 (55.1%) | 73 (20.9%) |
| Do you moisturize your feet daily? | 99 (28.3%) | 207 (59.1%) | 44 (12.6%) |
| Do you continuously wear cotton socks? | 83 (23.7%) | 205 (58.6%) | 62 (17.7%) |
| Do you cut your Sex toenails every 2 weeks? | 199 (56.9%) | 137 (39.1%) | 14 (4.0%) |
Table 4.
Comparison of knowledge regarding self-foot care among male and female diabetic patients
| Knowledge indicator | Total | Males | Females | Chi square Pvalue |
|---|---|---|---|---|
| Look after their feet because they may not feel a minor injury to their feet | ||||
| False/don’t know | 117 (34.1%) | 61 (52.1%) | 56 (47.9%) | 0.649 |
| True | 226 (65.9%) | 124 (54.9%) | 102 (45.1%) | |
| Look after their feet because wounds and infection may not heal quickly | ||||
| False/don’t know | 79 (23.0%) | 45 (57.0%) | 34 (43.0%) | 0.607 |
| True | 264 (77.0%) | 140 (53.0%) | 124 (47.0%) | |
| Look after their feet because they may get a foot ulcer | ||||
| False/don’t know | 126 (36.7%) | 65 (51.6%) | 61 (48.4%) | 0.574 |
| True | 217 (63.3%) | 120 (55.3%) | 97 (44.7%) | |
| Do not smoke because smoking causes poor circulation and affects the feet | ||||
| False/don’t know | 108 (31.5%) | 57 (52.8%) | 51 (47.2%) | 0.816 |
| True | 235 (68.5%) | 128 (54.5%) | 107 (45.5%) | |
| Look after their feet because they are more prone to flat foot | ||||
| False/don’t know | 117 (34.1%) | 67 (57.3%) | 50 (42.7%) | 0.219 |
| True | 226 (65.9%) | 118 (52.2%) | 108 (47.8%) | |
| Take medication regularly because they are liable to get DM complication | ||||
| False/don’t know | 41 (12.0%) | 22 (53.7%) | 19 (46.3%) | 1.000 |
| True | 302 (88.0%) | 163 (54.0%) | 139 (46.0%) |
The practice of self-care of feet was statistically significantly different among males and females regarding self-inspection of feet on regular basis as well as daily moisturizing of their feet. Where in the majority of males (n = 61, 63.5%) always (n = 96, 28.0%) performed the former, the daily moisturizing was more prevalent among females (n = 66, 67.3%) out of those who claimed to have performed it always (n = 98, 28.6%) as their routine of foot-self-care practice. [Table 5].
Table 5.
Comparison of practice regarding self-foot care among male and female diabetic patients
| Practice indicator | Total | Males | Females | Chi square Pvalue |
|---|---|---|---|---|
| Do you examine/inspect your feet on a regular basis? | ||||
| Always | 96 (28.0%) | 61 (63.5%) | 35 (36.5%) | 0.031 |
| Sometimes/Rarely | 211 (61.5%) | 102 (48.3%) | 109 (51.7%) | |
| Never | 36 (10.5%) | 22 (61.1%) | 14 (38.9%) | |
| Do you check your shoes before you put them on? | ||||
| Always | 129 (37.6%) | 66 (51.2%) | 63 (48.8%) | 0.629 |
| Sometimes/Rarely | 191 (55.7%) | 105 (55.0%) | 86 (45.0%) | |
| Never | 23 (6.7%) | 14 (60.9%) | 9 (39.1%) | |
| Do you walk outside barefoot? | ||||
| Always | 20 (5.8%) | 12 (60.0%) | 8 (40.0%) | 0.530 |
| Sometimes/Rarely | 197 (57.6%) | 101 (51.3%) | 96 (48.7%) | |
| Never | 125 (36.5%) | 71 (56.8%) | 54 (43.2%) | |
| Do you wash your feet with warm water daily? | ||||
| Always | 115 (33.5%) | 57 (49.6%) | 58 (50.4%) | 0.436 |
| Sometimes/Rarely | 184 (53.6%) | 105 (57.1%) | 79 (42.9%) | |
| Never | 44 (12.8%) | 23 (52.3%) | 21 (47.7%) | |
| Do you carefully dry between toes after washing your feet? | ||||
| Always | 82 (23.9%) | 49 (59.8%) | 33 (40.2%) | 0.298 |
| Sometimes/Rarely | 191 (55.7%) | 103 (53.9%) | 88 (46.1%) | |
| Never | 70 (20.4%) | 33 (47.1%) | 37 (52.9%) | |
| Do you moisturize your feet daily? | ||||
| Always | 98 (28.6%) | 32 (32.7%) | 66 (67.3%) | 0.000 |
| Sometimes/Rarely | 205 (59.8%) | 124 (60.5%) | 81 (39.5%) | |
| Never | 40 (11.7%) | 29 (72.5%) | 11 (27.5%) | |
| Do you continuously wear cotton socks? | ||||
| Always | 81 (23.6%) | 43 (53.1%) | 38 (46.9%) | 0.084 |
| Sometimes/Rarely | 202 (58.9%) | 117 (57.9%) | 85 (42.1%) | |
| Never | 60 (17.5%) | 25 (41.7%) | 35 (58.3%) | |
| Do you cut your Sex toenails every 2 weeks? | ||||
| Always | 195 (56.9%) | 101 (51.8%) | 94 (48.2%) | 0.553 |
| Sometimes/Rarely | 134 (39.1%) | 75 (56.0%) | 59 (44.0%) | |
| Never | 14 (4.1%) | 9 (64.3%) | 5 (35.7%) |
*Figures in bold indicate significant pvalue<0.05
Discussion
The current study was conducted among 350 diabetic patients in ABC settings, Saudi Arabia with majority being type I diabetic patients and male patients (53.9%). The information acquired regarding duration of diabetes showed patient being affected by disease for less than or almost equivalent to ten years in majority of cases (98.8%). Around more than 50% of patients were adhering to treatment regimen of diet restriction along with oral agents. These findings are coherent with previous literature in terms of males being majorly diabetic patients.[25,26,27] However, majority of the studies exhibited oral agent as the treatment option among patients with diet regime being followed barely in some as compared to the present study.[25,26]
Further, our study participants were majorly type I diabetic patients which is contrary to previous studies where majority of patients are suffering from type II diabetes.[18,25,26,27,28] The duration of disease also differed in our study as compared to other studies with majority suffering from diabetes for less than or equal to ten years. However, a study conducted in Malaysia stated diabetes in majority of the patients for less than or equal to 10 years (53.5%).[29] The current study exhibited controlled HBA1c status in majority of patients (57.1%) whereas studies especially conducted in middle east have shown uncontrolled status among participants.[25,26,27,28]
The foot complications were absent in majority of diabetic patients enrolled in study with 57.9% exhibiting absence of foot complication and 35.5% having numbness, 4.3% having history of healed ulcer and 2.3% reporting toe amputation. Previous studies conducted in middle east exhibited a varied pattern. A study conducted in Jordan exhibited numbness as a major complication (57%) rather foot ulcer.[26] Another study conducted by Mehmood MK et al. exhibited foot complication in majority of patients (60.9%).[27]
Globally, awareness level regarding foot care in diabetes has been found to be poor among previous studies[23,25,30,31,32,33]. However, the current study on the contrary had more than 65% of patients certain about their knowledge regarding foot care. Around 63% patients had the knowledge of looking after their feet as they feared getting a foot ulcer or the fear of wounds and infections not getting healed among 77.1% patients. Diabetes being a metabolic syndrome is a multifaceted disease linked with various risk factors like hypertension, obesity, smoking etc., Smoking, an addictive habit, is again a predisposing factor for foot related problems in diabetes.[25] However, the current study exhibited poor knowledge among patients regarding the same with 32.3% of them not having any knowledge of same.
Previous literature exhibits poor knowledge of diabetic foot care among patients with more than 20% of patients examining their feet only while having some problem.[34] Another study reiterated the same with 61.8% of the patients having poor diabetic foot care.[29] The knowledge and practices of foot care varies globally with some regions showing satisfactory knowledge but limited practises and some showing both poor knowledge as well as poor practises. In the current study, discrepancy was seen between patient's knowledge and practises with only 28% practising self-examination or feet inspection on regular basis.
Such kind of discrepancy between knowledge and practice was similar to two previous studies conducted in Jordan. These findings are contrast to findings from UK,[33] Iran,[30] Netherlands,[35] India[36] and USA[37] where inadequate knowledge of self-foot-care among diabetic patients was seen. However, the previous studies conducted could justify their result with statistical significant association between knowledge of foot care and education status. However, the current study is unable to elucidate those aspects due to absence of information regarding socioeconomic status of patients.
As discussed earlier, the practise pattern was poor among diabetic patients in the current study with only 28% inspecting feet on a regular basis, 33.4% patients washing feet daily with warm water, 24% of them drying between toes after washing and 28.3% moisturising feet daily. In a study conducted in Iraq, the correct measure that majority of the patients knew and practised was washing their feet daily (76% patients).[28] They attributed this practise due to religious reasons and not diabetic care. However, drying the feet after washing was done only in about 30% of patients which is concurrent to our findings.
The daily washing feet ritual exhibited higher percentages among studies conducted in Saudi Arabia[14] and Pakistan[32] which is again attributed to Islamic ritual. However, a study conducted in Malaysia by Muhammad-Lutfi et al. depicted coherent findings as ours with the majority being unaware that foot should be washed by a warm water, the temperature should be checked before washing feet, or using moisturizer on feet is good.[29] In another study in Iran by Kafaie et al., the majority were unaware nor did they practise washing their feet daily or inspected foot daily or used any moisturiser.[38] However, the patients in the current study majorly cut their toenails frequently (56.9%). Influence of education and educational programs had a positive impact on knowledge and practise among patients as cited in previous studies conducted in Tanzania, India and Saudi Arabia.[39,40,41] The current study was limited in this aspect as they were unable to elucidate these socioeconomic gradients and their impact on knowledge, awareness and practise among patients.
In the current study, no significant difference in knowledge about foot self-care was observed among males and females. A study reported significantly higher diabetic foot care knowledge score in women[33] compared to men whereas a study conducted in Malaysia exhibited higher knowledge about foot self-care among men.[29] However, the difference in behaviour has been attributed to sociocultural beliefs and educational status.
In the current study, the practice of self-care of feet was statistically significantly different among males and females regarding self-inspection of feet on regular basis (p value = 0.031) as well as daily moisturizing of their feet (p value = 0.000). The majority of males (n = 61, 63.5%) always (n = 96, 28.0%) performed the former, the daily moisturizing was more prevalent among females (n = 66, 67.3%) out of those who claimed to have performed it always (n = 98, 28.6%) as their routine of foot-self-care practice.
The current study exhibited fair knowledge but poor practises conduct among diabetic patients regarding foot care. Even though the current study illustrated the knowledge, awareness and practises among diabetic patients along with gender segregation, the current study had certain limitations. The unavailability of socioeconomic factors like education, income restricted the causative explanation of certain findings as illustrated in previous studies. Further, risk factors associated with diabetes could have been explored better.
The results of this study should be useful as they will provide an insight not only for clinicians and nurses but importantly for primary care physicians As the primary care physicians are the primary contact point of majority patients with the healthcare, awareness about the patient's knowledge and practise level of diabetic foot would definitely equip them for promoting self-care among their diabetic patients. Secondly, the primary care physicians would get ware of the specific lacunae areas in patient's knowledge and practices, which would help them to reinforce the desired behaviour of selfcare among them.
The lacunae pointed out in the knowledge and practise regarding diabetic foot care can aid in building new guidelines for spreading awareness and policies regarding those aspects.[42] These guidelines can focus on conducting awareness and educational programs for the diabetic patient's first contact with healthcare, door to door campaigns, promotional activities enhancing the importance of self-foot-care, etc.[43] Key points of the study:
Out of 350 diabetic patients, 35.5% had numbness, 4.3% with the history of healed ulcer and 2.3% reported toe amputation.
About 65% of patients were certain about their knowledge regarding foot care due to various reasons. Around 63% patients had the knowledge of looking after their feet as they feared of getting a foot ulcer. Another 77% knew that their wounds and infections would not get healed if proper care was not taken.
The practise pattern was poor among diabetic patients in the current study with only 28% inspecting feet on a regular basis, 33.4% patients washing feet daily with warm water, 24% of them drying between toes after washing, and 28.3% moisturising feet daily.
No significant difference in knowledge about foot self-care was observed among males and females. However, the practice of self-care of feet was statistically significantly different among males and females regarding self-inspection of feet on regular basis as well as daily moisturizing of their feet.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient (s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgemaents
Authors acknowledge all primary authors of the included studies for their assistance and academic support.
References
- 1.Shaw JE, Sicree RA, Zimmet PZ. Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Res Clin Pract. 2010;87:4–14. doi: 10.1016/j.diabres.2009.10.007. [DOI] [PubMed] [Google Scholar]
- 2.World Health Organization (WHO) Global Report on Diabetes. Geneva, Switzerland: WHO; 2016. [Google Scholar]
- 3.Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence of diabetes: Estimates for the year 2000 and projections for 2030. Diabetes Care. 2004;27:1047–53. doi: 10.2337/diacare.27.5.1047. [DOI] [PubMed] [Google Scholar]
- 4.International Federation of Diabetes (IDF), 2017. About Diabetes [online] Available from: http://idf.org/about-diabetes/what-is-diabetes .
- 5.Global Report on Diabetes. Geneva, Switzerland: WHO; 2017. World Health Organization (WHO) [Google Scholar]
- 6.Boulton AJ, Vileikyte L, Ragnarson-Tennvall G, Apelqvist J. The global burden of diabetic foot disease. Lancet. 2005;366:1719–24. doi: 10.1016/S0140-6736(05)67698-2. [DOI] [PubMed] [Google Scholar]
- 7.Zhang P, Lu J, Jing Y, Tang S, Zhu D, Bi Y. Global epidemiology of diabetic foot ulceration: A systematic review and meta-analysis. Ann Med. 2017;49:106–16. doi: 10.1080/07853890.2016.1231932. [DOI] [PubMed] [Google Scholar]
- 8.Carmona GA, Hoffmeyer P, Herrmann FR, Vaucher J, Tschopp O, Lacraz A, et al. Major lower limb amputations in the elderly observed over ten years: The role of diabetes and peripheral arterial disease. Diabetes Metab. 2005;31:449–54. doi: 10.1016/s1262-3636(07)70215-x. [DOI] [PubMed] [Google Scholar]
- 9.Rahman S. Diabetic Foot Ulcer. Predisposing factors and Management. BMJ. 2006;332:407–10. [Google Scholar]
- 10.Crawford F, Inkster M, Kleijnen J, Fahey T. Predicting foot ulcers in patients with diabetes: A systematic review and meta-analysis. Q J Med. 2007;100:65–86. doi: 10.1093/qjmed/hcl140. [DOI] [PubMed] [Google Scholar]
- 11.Liapis CD, Balzer K, Benedetti-Valentini F, Fernandes e Fernandes J, editors. Vascular Surgery. Berlin, Heidelberg: European Manual of Medicine Springer; 2007. Diabetic Foot. [Google Scholar]
- 12.Veves A, Uccioli L, Manes C, Van Acker K, Komninou H, Philippides P, et al. Comparison of risk factors for foot problems in diabetic patients attending teaching hospitals in four different European states. Diabet Med. 1994;11:709–13. doi: 10.1111/j.1464-5491.1994.tb00338.x. [DOI] [PubMed] [Google Scholar]
- 13.Abdulaziz Al Dawish M, Alwin Robert A, Braham R, Abdallah Al Hayek A, Al Saeed A, Ahmed Ahmed R, et al. Diabetes mellitus in Saudi Arabia: A review of the recent literature. Curr Diabetes Rev. 2016;12:359–68. doi: 10.2174/1573399811666150724095130. [DOI] [PubMed] [Google Scholar]
- 14.Al-Hariri M, Al-Enazi A, Alshammari D, Bahamdan A, AL-Khtani S, Al-Abdulwahab A. Descriptive study on the knowledge, attitudes and practices regarding the diabetic foot. J Taibah Univ Med Sci. 2017;17:1–5. doi: 10.1016/j.jtumed.2017.02.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Goweda R. Assessment of knowledge and practices of diabetic patients regarding diabetic foot care, in Makkah, Saudi Arabia. J Fam Med Health Care. 2017;3:17–22. [Google Scholar]
- 16.World Health Organization – Diabetes Country Profiles. 2016 [Google Scholar]
- 17.Abdulghani HM, AlRajeh AS, AlSalman BH, AlTurki LS, AlNajashi NS, Irshad M, et al. Prevalence of diabetic comorbidities and knowledge and practices of foot care among diabetic patients: A cross-sectional study. Diabetes Metab Syndr Obes. 2018;11:417–25. doi: 10.2147/DMSO.S171526. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Alshammari ZJ, Alsaid LA, Parameaswari PJ, Alzahrani AA. Attitude and knowledge about foot care among diabetic patients in Riyadh, Saudi Arabia. J Family Med Prim Care. 2019;8:2089–94. doi: 10.4103/jfmpc.jfmpc_248_19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Ragnarson Tennvall G, Apelqvist J. Healtheconomic consequences of diabetic foot lesions. Clin Infect Dis. 2004;39:132–9. doi: 10.1086/383275. [DOI] [PubMed] [Google Scholar]
- 20.Prompers L, Huijberts M, Schaper N, Apelqvist J, Bakker K, Edmonds M, et al. Resource utilisation and costs associated with the treatment of DFUs. Prospective data from the Eurodiale Study. Diabetologia. 2008;51:1826–34. doi: 10.1007/s00125-008-1089-6. [DOI] [PubMed] [Google Scholar]
- 21.Girod I, Valensi P, Laforet C, Moreau-Defarges T, Guillon P, Baron F. An economic evaluation of the cost of DFUs: Results of a retrospective study on 239 patients. Diabetes Metabol. 2003;29:269–77. doi: 10.1016/s1262-3636(07)70036-8. [DOI] [PubMed] [Google Scholar]
- 22.Van Acker K, Oleen-Burkey M, De Decker L, Vanmaele R, Van Schil P, Matricali G, et al. Cost and resource utilization for prevention and treatment of foot lesions in a diabetic foot clinic in Belgium. Diabetes Res Clin Pract. 2000;50:87–95. doi: 10.1016/s0168-8227(00)00157-1. [DOI] [PubMed] [Google Scholar]
- 23.Ghosh P, Valia R. Burden of DFUs in India: Evidence Landscape from Published Literature. Value Health. 2017;20:9. [Google Scholar]
- 24.Pinzur MS, Slovenkai MP, Trepman E, Shields NN Diabetes Committee of American Orthopaedic Foot and Ankle Society. Guidelines for diabetic foot care: Recommendations endorsed by the Diabetes Committee of the American Orthopaedic Foot and Ankle Society. Foot Ankle Int. 2005;26:113–9. doi: 10.1177/107110070502600112. [DOI] [PubMed] [Google Scholar]
- 25.Qadi MA, Al Zahrani HA. Foot care knowledge and practice among diabetic patients attending primary health care centers in Jeddah City. J King Abdulaziz Univ Med Sci. 2011;98:1–34. [Google Scholar]
- 26.Al-Qaddah RM, Al Eyadeh A, Abu-Qamar ME, Younes N, Al-Ryalat D, Haddad F. Knowledge and practice of foot care among diabetics at King Hussein Medical Center, Jordan. Jordan Med J. 2016;102:1–0. [Google Scholar]
- 27.Mehmood MK, Parkar AZ, Mustafa NT, Mustafa SS, Makin MA, Alawadi F, et al. Diabetic foot self-care: Awareness and practice among type 2 diabetic patients in primary healthcare centers, Dubai Health Authority. Int J Community Med Public Health. 2019;6:1–7. [Google Scholar]
- 28.Saber HJ, Daoud AS. Knowledge and practice about the foot care and the prevalence of the neuropathy among a sample of type 2 diabetic patients in Erbil, Iraq. J Family Med Prim Care. 2018;7:967–74. doi: 10.4103/jfmpc.jfmpc_163_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Muhammad-Lutfi AR, Zaraihah MR, Anuar-Ramdhan IM. Knowledge and practice of diabetic foot care in an in-patient setting at a Tertiary Medical Center. Malays Orthop J. 2014;8:22–6. doi: 10.5704/MOJ.1411.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Khamseh ME, Vatankhah N, Baradaran HR. Knowledge and practice of foot care in Iranian people with type 2 diabetes. Int Wound J. 2007;4:298–302. doi: 10.1111/j.1742-481X.2007.00381.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Desalu O, Salawu F, Jimoh A, Adekoya A, Busari O, Olokoba A. Diabetic foot care: Self reported knowledge and practice among patients attending three tertiary hospital in Nigeria. Ghana Med J. 2011;45:60–5. doi: 10.4314/gmj.v45i2.68930. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Hasnain S, Sheikh NH. Knowledge and practices regarding foot care in diabetic patients visiting diabetic clinic in Jinnah Hospital, Lahore. J Pak Med Assoc. 2009;59:687–90. [PubMed] [Google Scholar]
- 33.Kim EJ, Han KS. Factors related to self-care behaviours among patients with diabetic foot ulcers. J Clin Nurs. 2020;29:1712–22. doi: 10.1111/jocn.15215. [DOI] [PubMed] [Google Scholar]
- 34.Goie TT, Naidoo M. Awareness of diabetic foot disease amongst patients with type 2 diabetes mellitus attending the chronic outpatients department at a regional hospital in Durban, South Africa. Afr J Prim Health Care Fam Med. 2016;2071:2928–36. doi: 10.4102/phcfm.v8i1.1170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Meijer JW, Links TP, Smit AJ, Groothoff JW, Eisma WH. Evaluation of a screening and prevention programme for diabetic foot complications. Prosthet Orthot Int. 2001;25:132–8. doi: 10.1080/03093640108726586. [DOI] [PubMed] [Google Scholar]
- 36.Chanda A, Ayyar V, Idiculla JM, Bantwal G. Perception of foot problems among diabetic patients: A cross sectional study. Int J Diab Dev Ctries. 2006;26:77–80. [Google Scholar]
- 37.Neil JA. Assessing foot care knowledge in a rural population with diabetes. Ostomy Wound Manage. 2002;48:50–6. [PubMed] [Google Scholar]
- 38.Kafaie P, Noorbala MT, Soheilikhah S, Rashidi M. Evaluation of patients’ education on foot self-care status in diabetic patients. Iran Red Crescent Med J. 2012;14:829–32. doi: 10.5812/ircmj.1138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Chiwanga FS, Njelekela MA. Diabetic foot: Prevalence, knowledge, and foot self-care practices among diabetic patients in dar es Salaam, Tanzania – A cross-sectional study. J Foot Ankle Res. 2015;8:20. doi: 10.1186/s13047-015-0080-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.George H, Rakesh P, Krishna M, Alex R, Abraham VJ, George K, et al. Foot care knowledge and practices and the prevalence of peripheral neuropathy among people with diabetes attending a secondary care rural hospital in Southern India. J Family Med Prim Care. 2013;2:27–32. doi: 10.4103/2249-4863.109938. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Al-Asmary AS, Mostafa OS, AL-Khaldi YM. Diabetic patients’ knowledge and practice regarding prevention of diabetic foot. Med J Cairo Univ. 2013;81:197–205. [Google Scholar]
- 42.Gupta M, Kaur M, Lakshmi PV, Prinja S, Singh T, Sirari T, et al. Social autopsy for identifying causes of adult mortality. PLoS One. 2018;13:e0198172. doi: 10.1371/journal.pone.0198172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Singh S, Jajoo S, Shukla S, Acharya S. Educating patients of diabetes mellitus for diabetic foot care. J Fam Med Prim Care. 2020;9:367–73. doi: 10.4103/jfmpc.jfmpc_861_19. [DOI] [PMC free article] [PubMed] [Google Scholar]