

Summary
Several oncoplastic techniques have been proposed for subareolar breast cancer, some of which may require contralateral operation for symmetry, or more than one operation for delayed reconstruction of the nipple-areola complex (NAC). We herein developed a simple and effective oncoplastic approach following central quadrantectomy, aiming to achieve the following: (1) preservation of breast shape and contour for patients who are not accepting of a notably smaller breast or bilateral operation; (2) single procedure with advantages of single anesthetic and the ability to reconstruct a breast that has not yet been affected by radiation; (3) no autologous grafts with disadvantage of an extra donor site; (4) creation of natural neo-NAC with only incision within the region of the areola complex; and (5) maintaining long-term nipple projection. In this technique, the medial and lateral peri-areolar flap was advanced and rotated to restore partial neo-NAC, and to fill the defect after central tumor and NAC resection. The whole neo-NAC margin was created using the “round block” technique. Additionally, the nipple reconstruction was performed at the mitten of the neo-areola area using the C-V nipple flaps with an internal strut of rolled dermal grafts harvested from excised skin during the round block procedures. Lastly, a purse-string suture is placed in the outer skin margin for control of areola diameter and project. Six patients with central tumors of the breast were treated in this easily achieved approach. Patient satisfaction was noted as high, and the cosmetic results were evaluated as good to excellent.
INTRODUCTION
Simple closure of defects after central tumor and nipple-areola complex (NAC) resection gave cosmetic outcomes so poor that mastectomy was traditionally considered.1,2 Several oncoplastic techniques have been proposed for patients with subareolar breast cancer, some of which may require more than one operation.3–5
There are also immediate breast and NAC reconstruction techniques using volume displacement or replacement, such as latissimus dorsi myocutaneous flap, anterior intercostal artery perforator flap, keyhole-shaped flap, and Grisotti’s flap.6–9 However, these approaches require recruitment of additional tissue in the used flaps. To overcome these problems, we developed an immediate neo-NAC reconstruction technique aiming to improve the cosmesis after central lumpectomy. Our technique involved double opposing rotational peri-areolar flaps, C-V nipple flap10 with inner dermal core, and the “round block” procedure.11
PATIENTS AND METHODS
Six patients with subareolar breast cancer, aged 36–76 years, were treated with breast-conserving and NAC resection followed by immediate neo-NAC reconstruction. Axillary lymph node dissection was performed if indicated. All patients underwent preoperative imaging examination, and surface markers were applied for location and range of breast tumor.
Suitability
This technique can be used for small-volume breasts with minimal or little ptosis.
Surgical Strategy
The surgical strategy is composed of central quadrantectomy, including NAC and tumor, 2 medial and lateral peri-areolar flaps, a C-V flap, and the round block procedures. Figure 1 shows detailed schematic stages I–VI of the developed neo-NAC reconstruction technique. Stage I (preoperative design): An eccentric ellipse is drawn around the proposed central quadrantectomy area with 2 “crab claw shaped” peri-areolar flaps (b) and the NAC located in the inferior pole. The ellipse is extended superiorly to encompass the neo-NAC position with the neo-nipple located on the edge of remaining local skin after nipple-areolar excision. A parallel hemi-circumferential ring is marked around the upper half of ellipse outline for the round block procedures. Stage II and III: Perform central quadrantectomy, including NAC and tumor, with a column of tissue from the subcutaneous layer down to the pectoral, then bring the defect together with 2 or 3 layers of glandular suture using the purse-string technique to obtain a central projection of the mammary cone.12,13 The operation is continued with management of designed 2 medial and lateral peri-areolar flaps. The medial and lateral borders of the flap are performed extending from the medial and lateral margins of the neo-NAC to give a “crab claw” shaped appearance skin and subcutaneous tissue flap. Stage IV and V: The flaps are advanced and rotated in opposite directions toward each other to cover the large part of defect after central quadrantectomy, and the opposite poles are closed in a hemi-circumferential fashion. Flap edges are sutured with interrupted, nonabsorbable sutures. In this way, the lower portion of neo-NAC is created simultaneously. The skin between the 2 rings around the upper portion of neo-NAC is carefully de-epithelialized during the round block procedures. The dermal graft harvested from de-epithelialization is rolled tightly and held in place with a 3/0 Vicryl suture so that a cylindrical central pillar of the nipple reconstruction (d) is formed. The designed C-V flap is elevated from the underlying subcutaneous tissue, and the donor sites are closed with interrupted nonabsorbable sutures. The “V” flaps are rolled and sutured together in a ying-yang fashion, and the cylindrical compacted graft is placed in its erect position into the trough formed by the V flaps so that the core volume of nipple is augmented with axial rigidity. The C flap is folded over and sutured to the V flaps to complete the nipple reconstruction.14,15 Stage VI: Lastly, the round skin defects along the edge of the NAC are closed by a continuous running stitch technique using purse-string sutures for control of neo-areola diameter, shape, and project.16 Figure 2 shows the surgical procedure intraoperatively.
Fig. 1.
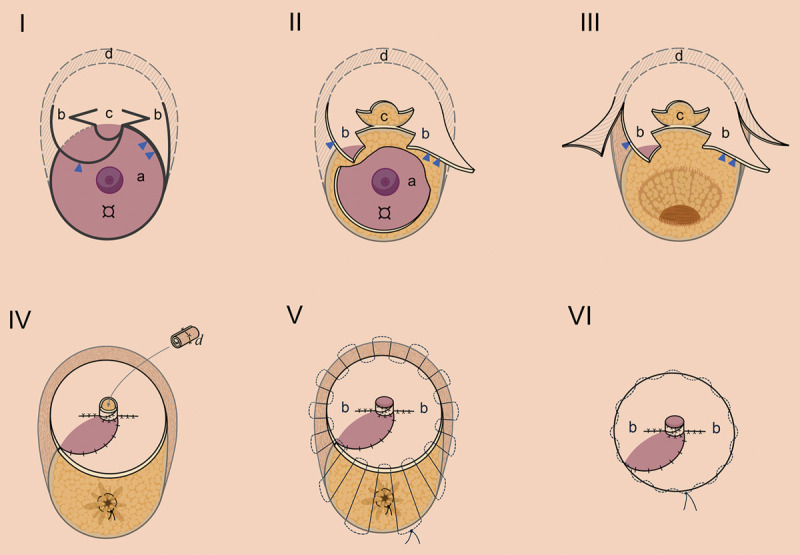
Schematic of the authors’ technique, stages I–VI. (I) Preoperative design. For illustration purpose, (a) shows proposed removal area with tumor involving the lower subareolar region and NAC; only the partial upper portion of areola is preserved (arrow head). (b) Arrows denoting 2 “crab foot shaped” medial (arrow head) and lateral (double arrow heads) peri-areolar flaps. (c) A V-C nipple flap. (d) The area of de-epithelialized or excised skin at the edge of neo-NAC. “¤” indicates tumor. (II) Central lumpectomy and flaps’ elevation. (III) NAC and tumor were removed together with central lumpectomy cavity and area of V-C and peri-areolar flaps. (IV) Appearance of advancement of glandular tissue and flaps that were mobilized and sutured to fill the central breast while creating neo-NAC. The edge of the neo-NAC was epithelialized and packed into the neo-nipple. (V) Reduction of the diameter of the outer skin margin using a purse-string suture. (VI) Final result following closure of the skin incision.
Fig. 2.
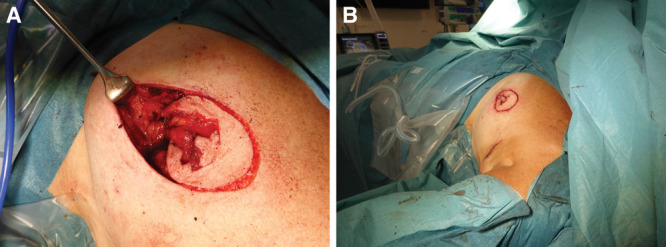
Details of the surgical procedure intraoperatively. A 64-year-old patient with subareolar invasive ductal carcinoma (IDC) and ductal carcinoma in situ (DCIS), 2.0 cm in size. A, a central lumpectomy cavity after removal of NAC and tumor together; medial and lateral peri-areolar flaps, V-C flap, and the area of de-epithelized at edge of areola are shown. (B) Immediate postoperative appearance of the reconstructed neo-NAC after closure of the skin incision.
RESULTS
With this novel approach, we successfully achieved satisfactory results for 6 patients. All central breast cancers were completely excised with negative margins. The neo-NAC positions were well centered, and the neo-nipple remained conspicuous (Fig. 3). (See figure 1, Supplemental Digital Content 1, which displays a 52-year-old woman with a right subareolar breast cancer (grade 3 DCIS, 2.0 cm) who elected to have central lumpectomy, NAC resection, and immediate breast reconstruction. The patient’s clinical result is shown at 3 months after radiation therapy. http://links.lww.com/PRSGO/B571.) (See figure 2, Supplemental Digital Content 2, which displays the same patient as in Fig. 2: Preoperative (A) and 3 months postoperative (B) picture of NAC reconstruction demonstrating good NAC symmetry. Although the left breast is smaller, its contour and natural shape have been preserved. http://links.lww.com/PRSGO/B572.) (See figure 3, Supplemental Digital Content 3, which displays a 75-year-old woman with a left subareolar breast cancer (IDC and DCIS, 2.5 cm in size) who elected to have central lumpectomy, NAC resection, and immediate neo-NAC reconstruction. The patient’s clinical result is shown at 6 months after radiation therapy. http://links.lww.com/PRSGO/B573.)
Fig. 3.

The same patient as in Figure 2: lateral image of neo-NAC was obtained after 3 months, demonstrating good nipple and areolar projection.
The patients were well pleased with the cosmetic results that were maintained over the long term. But notably, the breast of one 52-year-old patient showed mild central depression deformities after postoperative radiation, and the breast of one 73-year-old patient had small surface necrosis at the edge between the peri-areolar flaps, which delayed wound healing.
DISCUSSION
The surgical options for NAC involved central tumors include simple or modified ellipse excisions, round block purse-string excisions with poor cosmetic outcomes, volume displacement, and volume replacement techniques with more ideal cosmetic outcomes. Patients with large ptotic breasts are good candidates for volume displacement procedures, such as wedge excision and Grisotti flap. The procedure is usually bilateral for symmetry.17 Volume replacement techniques using local flap to correct partial breast defects and restore NAC are preferable in patients with smaller, non-ptotic breasts. However, these sophisticated approaches require recruitment of additional tissue in the used flaps, which increases the risk of adjacent tissue distortion, resulting in alteration of the final breast contour. Moreover, postoperative radiotherapy can result in retraction of scar outside the region of the NAC at breast and dislocate the neo-NAC position.8,9 Our approach fulfilled patients’ desire to have a one-stage procedure in which the double rotational peri-areolar flaps, C-V flap, and round block technique can create neo-NAC that has adequate long-term projection and provides satisfactory results. This technique is ideal for patients with small central breast cancers that involve the NAC or are located close to the NAC. It is also beneficial to operate on patients with larger subareolar tumors or Paget’s disease. However, one disadvantage of our technique is the high-riding of the neo-NAC location. Care should be taken in designing the neo-NAC position and areolar excision to avoid malposition.
CONCLUSION
We describe our new approach for immediate reconstruction of the NAC after central lumpectomy, with excellent results in patients who are not accepting of a notably smaller breast or bilateral operation.
ACKNOWLEDGMENT
The authors are thankful to Miss Eileen Huang for making illustrations.
Supplementary Material
Footnotes
Published online 16 February 2021.
Disclosure: The authors have no financial interest to declare in relation to the content of this article.
Related Digital Media are available in the full-text version of the article on www.PRSGlobalOpen.com
REFERENCES
- 1.Recht A, Connolly JL, Schnitt SJ, et al. Conservative surgery and radiation therapy for early breast cancer: Results, controversies, and unsolved problems. Semin Oncol. 1986;13:434–449. [PubMed] [Google Scholar]
- 2.Multon O, Bourgeois D, Validire P, et al. [Breast cancers with central localization: Conservative treatment by tumorectomy with ablation of the areolar plaque]. Presse Med. 1997;26:988–994. [PubMed] [Google Scholar]
- 3.Clough KB, Cuminet J, Fitoussi A, et al. Cosmetic sequelae after conservative treatment for breast cancer: Classification and results of surgical correction. Ann Plast Surg. 1998;41:471–481. [DOI] [PubMed] [Google Scholar]
- 4.Bajaj AK, Kon PS, Oberg KC, et al. Aesthetic outcomes in patients undergoing breast conservation therapy for the treatment of localized breast cancer. Plast Reconstr Surg. 2004;114:1442–1449. [DOI] [PubMed] [Google Scholar]
- 5.Horiguchi J, Koibuchi Y, Iijima K, et al. Local control by breast-conserving surgery with nipple resection. Anticancer Res. 2005;25:2957–2959. [PubMed] [Google Scholar]
- 6.de Lorenzi F. Oncoplastic surgery: The evolution of breast cancer treatment. Breast J. 2010;16(suppl 1):S20–S21. [DOI] [PubMed] [Google Scholar]
- 7.Zaha H, Hakazu O, Watanabe M, et al. Breast-conserving surgery using reduction mammoplasty. Jpn J Breast Cancer. 2008;23:211–5. [Google Scholar]
- 8.Berry MG, Fitoussi AD, Curnier A, et al. Oncoplastic breast surgery: A review and systematic approach. J Plast Reconstr Aesthet Surg. 2010;63:1233–1243. [DOI] [PubMed] [Google Scholar]
- 9.Kijima Y, Yoshinaka H, Shinden Y, et al. Oncoplastic breast surgery for centrally located breast cancer: A case series. Gland Surg. 2014;3:62–73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Jones G, Bostwick J, III. Nipple-areolar reconstruction. Operative Tech Plastic Reconstr Surg.1994;1:35–8. [Google Scholar]
- 11.Benelli L. A new periareolar mammaplasty: The “round block” technique. Aesthetic Plast Surg. 1990;14:93–100. [DOI] [PubMed] [Google Scholar]
- 12.Yang JD, Lee JW, Cho YK, et al. Surgical techniques for personalized oncoplastic surgery in breast cancer patients with small- to moderate-sized breasts (part 1): Volume displacement. J Breast Cancer. 2012;15:1–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Calhoun KE, Anderson BO. Oncoplastic surgery: Central quadrant techniques. In: Urban C, Rietjens M, eds. Oncoplastic and Reconstructive Breast Surgery. 1st ed. Milano: Springer; 2013;. Vol 12: 117–127. [Google Scholar]
- 14.Chia HL, Wong M, Tan BK. Nipple reconstruction with rolled dermal graft support. Arch Plast Surg. 2014;41:158–162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.de lorenzi F, Lohsiriwat V. Nipple and areola complex reconstruction. In: Urban C, Rietjens M, El-Tamer M, Sacchini V, eds. Oncoplastic and Reconstructive Breast Surgery. 2nd ed. Cham, Switzerland: Springer; 2019; Vol 55: 661–670. [Google Scholar]
- 16.Caterson SA, Singh M, Talbot SG, et al. Reconstruction of areolar projection using a purse-string suture technique. Plast Reconstr Surg Glob Open. 2015;3:e453. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Masetti R, Pirulli PG, Magno S, et al. Oncoplastic techniques in the conservative surgical treatment of breast cancer. Breast Cancer. 2000;7:276–280. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.