

Summary
The emergence of COVID-19, caused by novel Coronavirus SARS-CoV-2, became a pandemic in just 10 weeks. Without effective medications or vaccines available, authorities turned toward mitigation measures such as use of face masks, school’s closings, shelter-in-place, telework and social distancing. People found refuge on the internet and social media apps; however, there was a proliferation of instant messaging containing hoaxed, deliberate misleading information: fake news messaging (FNM). The aim of this study was to assess FNM through content analysis and to discriminate them in a proposed taxonomy structure. A sample of convenience of messages, memes, tweets or cartoons in several languages was selected from the most popular social media outlets, i.e. Facebook, WhatsApp, Twitter etc. More than 300 FNM were identified. Descriptive statistics were used for highlighting potential relationships between variables. Content analysis determined that FNM could be divided into Health- and non-health-related types. There are several sub-types considering, but not limited to, religious beliefs, politics, economy, nutrition, behaviors, prevention of the infection, the origin of the disease and conspiracy theories. The parallel FNM pandemic affected the response from an already debilitated public health system through the confusion created in the community and the erosion in the credibility of genuine media. Public health practitioners had to face people’s unpredictable behaviors, panic, tensions with the communities and, in some cases, a hostile climate toward frontline workers. Public health practitioners must adjust ongoing and future health promotion and education interventions including plans to neutralize fake news messages.
Keywords: community health promotion, health education, health literacy, public health, global health
INTRODUCTION
‘The problem with the Internet is that it gives you everything - reliable material and crazy material. So the problem becomes, how do you discriminate?’ Umberto Eco
The fulminant emergence and dissemination of COVID-19, caused by novel Coronavirus SARS-CoV-2, became a pandemic in just ten weeks with at least 2 million confirmed cases, 100 thousand deaths, and an unknown number of asymptomatic carriers. These numbers have gone up severalfold until today. Without structurally competent health systems (Metzl et al., 2020), effective medications or a vaccine, authorities turned toward mitigation measures such as school’s closings, shelter-in-place, telework and social distancing. People found refuge on the internet and social media apps becoming their fundamental sources for information; however, this enkindled the proliferation of instant messaging containing hoaxed, exploitative, deliberate misleading information: fake news messaging (FNM). As the virus was quickly spreading out across the globe, Dr Tedros Adhanom Ghebreyesus the World Health Organization (WHO) Director General warned at the Munich security conference ‘we’re not just fighting an epidemic; we’re fighting an infodemic’ (WHO, 2020), in other words, a pandemic of fake news.
COVID-19 fake news proliferation
The fertile grounds for the briskly proliferation of fake news is situated in the co-existence and interaction of two domains: technology and health literacy. Indeed, WHO’s Director General reckoned that fake news spreads as fast and easily as the virus, making it just as dangerous (WHO, 2020). In the case of technology, evidence available has shown that cyborg accounts, trolls and bots networks, disguised as legitimate individuals, are used to spread malware and unsolicited polarizing content to promote discord and erode the trust of the communities and the credibility in the legitimate health authorities (Broniatowski et al., 2018). Others have openly created false claims about the use of a future COVID-19 vaccine as the vehicle for quantum-dot spyware through a nanochip (Biohackinfo.com, 2020). This disinformation was purposely used by political apparatchik to promote a negationist, conspiracy-based agenda (Fredericks, 2020).
By the same token, false rumors, misinformation/disinformation, fake news are diffused (and unconsciously endorsed) through social media significantly farther, faster, deeper, more broadly, reaching more people than true rumors. False rumors can reach out up to six times faster the same number of individuals than true rumors (Vosoughi et al., 2018). Recent evidence demonstrated that COVID-19-related false or fake news can be moved from one platform to another very fast using shortcuts or tunnels, a.k.a. ‘wormhole’ engineering. Social media platforms then would have to lengthen the pathways to increasing chances for timely detection and neutralization of misinformation/disinformation (Velasquez et al., 2020).
Potential effects of COVID-19 fake news
There are several potential effects of the propagation of FNM on the health of the individuals during the pandemic. The exposure to torrents of information, correct or misleading, either in traditional sources or social media (Riehm et al., 2020) plus the loss of trust in the health systems (Barua et al., 2020) contribute to the generation of patterns of anxiety, psychological distress and depression resulting in compulsive behaviors like binge shopping or hoarding (Lopes et al., 2020; Zhang et al., 2020), or to the aggravation of pre-existing mental health problems (Chatterjee et al., 2020). Another dangerous effect is the life threatening behavior of some people, induced by public figures and/or by politicians’ misleading information, to use toxic substances as ‘cures’ not properly cleared, i.e. the use of disinfectants, chloroquine phosphate (Waldrop et al., 2020) or the self-prescribed off-label use of medications (Cuan-Baltasar et al., 2020; Gerard et al., 2020).
Additionally, people tend to viralize unfiltered content through social media because they might not be proficient enough in the health literacy and/or critical thinking skills necessary to manage the decision-making process of sharing or not a given health-related content. It is recognized that both functional and cognitive skills are required to self-manage (Rademakers and Heijmans, 2018). As an example, in March 2020, WhatsApp tested adding a search function in the beta version of the Android app that enables people to go online and fact-check the messages they receive; therefore, helping to prevent or avoid the distribution of false messages (Singh, 2020). Although a final decision as to have it as a standard feature has not been made yet, it would help to filter-out messages appealing to emotions and/or carrying misinformation to help preserve the health and safety of the community (US DHHS, 2015).
Justification, aim and research question
Previous studies have analyzed the speed and characteristics of the diffusion of fake news messages (FNMs), some others performed public health-related content analysis focused on specific areas: Corporate social responsibility (Pulker et al., 2018), diabetes (Wilbur et al., 2017), public health and safety (Sutherland, 2016) or public policy (Zardo and Collie, 2014). To our knowledge, there are no studies performing a content analysis of COVID-19 FNMs in a global context. Therefore, to fill this gap, the aims of this study were to assess the content of a sample of convenience of publicly available COVID-19 related FNM in social media platforms and to classify them in a proposed taxonomy structure. Messages would be organized based on their language, perceived intention, number of words and other variables deemed relevant.
METHODOLOGY
Study design
An exploratory, structured, cross-sectional content analysis study was performed on a purposive, non-probabilistic sample of convenience of publicly available messages accessible to the researchers through international personal and professional networks’ media outlets. The messages were shared by the peers through any the most popular digital platforms, i.e. Facebook, WhatsApp, Twitter, YouTube etc., and then identified and flagged as COVID-19 FNM over the period comprised between 1 February and 31 March 2020.
These messages were written in several languages and included a wide-arrange of texts, pictures, illustrations, cartoons, memes or tweets, either alone or in combination. The unit of analysis was the COVID-19-related information, the knowledge, or the ideas included in the messages and the language and country of origin when it was possible to trace that information back to the source. The authors decided against the utilization of any social media/web search engines or message mining algorithms because they reinforce existing biases, do not account for the validity of methods for online FNM distribution, or the sources of the messages are not open to scrutiny, verification of accuracy or trustworthiness (Pennycook and Rand, 2019).
Information in languages other than English were directly translated by the authors when it was written in Spanish, Italian, French and/or Portuguese due to their language proficiency and fluency. In the case of other languages, whenever an English version of the message was not available, the Google Translate® app for Android and compatible with an auto-focus camera and dual-core processor was used for its translation and counter translation to verify/check for translation accuracy.
Study protocol
The COVID-19-related information, knowledge or ideas were extracted and subsequently registered using a non-validated coding frame data collection matrix tool designed in MS Excel®. Themes were identified and variables were defined for data collection: (i) Given title; (ii) Language; (iii) Country of origin; (iv) Number of Words; (v) Graphic in nature; (vi) Video embedded; (vii) Website or social media links or hashtags embedded; (viii) Main theme category; (ix) Purpose; (x) Outlet of publication/distribution; (xi) Target; (xii) Misinformation or disinformation type; (xiii) Key words; and (xiv) Reach (when available).
Coding and interrater reliability
Data were systematically collected and registered by each of the authors. A basic set of code words was adopted using selective reduction into manageable content themes and categories integrated by either one single word, a small set of words or short phrases. Problems or disagreements related to the coding process were solved by consensus between the authors. To test for appropriate interrater reliability, both authors coded 60 randomly selected messages from the sample of messages using the random number generation function in MS Excel® (RANDBETWEEN). To prevent volatility or unwanted changes in the random number generation function, a pivot table referencing the cells containing the numbers between 1 and 342 was organized. Coders graded the coding done by the other and results were compared using a grader reliability matrix. The Krippendorff’s (KALPHA) nominal binary alpha coefficient (Krippendorff, 2004) was calculated at 0.925 using Hayes’ SPSS macro file (Hayes and Krippendorff, 2007) in IBM SPSS Statistics® version 26.
Statistical analysis
Due to the exploratory nature of this study, descriptive statistics were used to illustrate the summaries of the data collected and to highlight potential relationships between the variables. Graphic analysis was included where deemed appropriate. Results are presented as tables and figures. Statistical analyses, tables and figures were conducted using MS Excel® for MS Windows 10®.
RESULTS
Geographic, linguistic and social media dimensions
A total of 342 COVID-19 FNMs were included in the final sample. We computed frequencies and proportions for the variables of interest. The messages were coming from all over the world (Figure 1). However, the biggest share of the sample was held by the USA (25.4%; n = 87). Immediately following, there was a group of western European countries with Spain in second place (11.4%; n = 39); the UK, third (7.6%; n = 26) and Italy, fourth (5.6%; n = 19) constituted half of the sample of messages. Immediately thereafter, a diverse group of countries completed three-quarters of the sample: In Latin America, Brazil (5.3%; n = 18), Colombia (4.7%; n = 16) and Mexico (3.5%; n = 12). In Asia, China and India (4.1%; n = 14) each, in Europe, France and Russia (2.3%; n = 8), respectively.
Fig. 1:

Geographical distribution of COVID-19 FNMs
The summary of the languages and social media sites used for sharing FNM are presented in Table 1. The language in which the fake news was written followed an even more concentrated pattern than the geographic location. English represented more than half of the sample of messages (52.6%; n = 180), followed by Spanish (28.4%; n = 97), Portuguese (5.0%; n = 17) and Italian (4.4%; n = 15). These four languages together accounted for 90% (n = 309) of the sample. Among other languages used were Chinese Mandarin, French, Arabic and German. Regarding social media platforms, Facebook was the one most frequently used for sharing the fake news (38.0%; n = 130), followed by Tweeter (16.7%; n = 57), WhatsApp (13.7%; n = 47) and YouTube (5.0%; n = 17). These four popular outlets concentrated almost 75% of the messages (n = 251). More structured and traditional media sites, such as Blogs, Newspapers, Magazines and News sites and channels were used a reference by another fifth of the messages (21.2%; n = 72).
Table 1:
COVID-19 FNMs language and social media sites
| Frequency (#) | Percent (%) | Cumulative percent (%) | |
|---|---|---|---|
| Language | |||
| English | 180 | 52.6 | 52.6 |
| Spanish | 97 | 28.4 | 81.0 |
| Portuguese | 17 | 5.0 | 86.0 |
| Italian | 15 | 4.4 | 90.4 |
| Chinese−Mandarin | 10 | 2.9 | 93.3 |
| French | 9 | 2.6 | 95.9 |
| Arabic | 4 | 1.2 | 97.1 |
| German | 4 | 1.2 | 98.2 |
| Other languages | 6 | 1.8 | 100.0 |
| Social media site | |||
| 130 | 38.0 | 38.0 | |
| Tweeter | 57 | 16.7 | 54.7 |
| 47 | 13.7 | 68.4 | |
| Blog | 40 | 11.7 | 80.1 |
| Newspaper | 18 | 5.3 | 85.4 |
| You Tube | 17 | 5.0 | 90.4 |
| News Site | 6 | 1.8 | 92.1 |
| Magazine | 5 | 1.5 | 93.6 |
| E-Bay | 4 | 1.2 | 94.7 |
| 3 | 0.9 | 95.6 | |
| News Channel | 3 | 0.9 | 96.5 |
| 2 | 0.6 | 97.1 | |
| Other Outlets | 10 | 2.9 | 100.0 |
Themes
FNM themes were divided into two clearly separated groups: health- and non-health-related types. The distribution of themes is shown in Figure 2. In general, there were several sub-types to consider, yet not limited to, religious beliefs, politics, economy, nutrition, behaviors (like hoarding), prevention of the infection, the origin of the disease, political propaganda, end of the world (Armageddon) and conspiracy theories.
Fig. 2:

COVID-19 fake prevention and treatment interventions messages
The ones that were Health-related, accounted for the majority (60.4%; n = 279) and included fake prevention, fake medicines and treatments, fake SARS-CoV-2 information, hoax or fake pandemic and anti-vaccine messages, and home remedies recommendations. The non-health-related group (39.6%; n = 183) included messages generating confusion, phishing/scams, conspiracy theories, political propaganda, pseudo-science and 5G theories along with anti-Bill Gates messages.
FNMs typology
In Table 2, the main characteristics of COVID-19 FNMs are presented. The mean number of words per message was 57; however, it came with a wide range (2 − 435) and a large variation (SD: 61.4). Half of the messages had 40 words or less (52.9%; n = 181). Most of the FNMs did not include a video embedded (82.2%; n = 281) nor were graphic in nature (52.3%; n = 179). The majority were considered as disinformation (59.6%; n = 204).
Table 2:
Characteristics of COVID-19 FNMs
| Frequency (#) | Percent (%) | Cumulative percent (%) | |
|---|---|---|---|
| Number of words per message | |||
| 0-20 | 111 | 32.5 | 32.5 |
| 21-40 | 70 | 20.5 | 52.9 |
| 41-60 | 55 | 16.1 | 69.0 |
| 61-80 | 28 | 8.2 | 77.2 |
| 81-100 | 24 | 7.0 | 84.2 |
| 101-120 | 14 | 4.1 | 88.3 |
| 121-140 | 7 | 2.0 | 90.4 |
| 141-160 | 12 | 3.5 | 93.9 |
| 161-180 | 5 | 1.5 | 95.3 |
| 181-200 | 2 | 0.6 | 95.9 |
| >200 | 14 | 4.1 | 100.0 |
| Type of message | |||
| Disinformation | 204 | 59.6 | 59.6 |
| Misinformation | 138 | 40.4 | 100.0 |
| Mostly graphic | |||
| No | 179 | 52.3 | 52.3 |
| Yes | 163 | 47.7 | 100.0 |
| Video embedded | |||
| No | 281 | 82.2 | 82.2 |
| Yes | 61 | 17.8 | 100.0 |
Suspected intentions and links of FNM
Suspected intentions and links of COVID-19 FNMs are shown in Table 3. Two-thirds of the messages were suspected to have the negative intend of creating confusion in the community (40.1%; n = 137) or to disseminate conspiracy theories (27.2%; n = 93). Other sixth of the messages were suspected to try to help with prevention (9.9%; n = 34) or treatment (6.4%; n = 22) of COVID-19. Other perceived intentions were related to scam/phishing purposes, to promote sales of medicines or other products or even have a humoristic intention. More than half of the messages were clearly targeting science, prevention measures and vaccines as their objectives (61.1%; n = 209).
Table 3:
Suspected intentions and links of COVID-19 FNMs
| Frequency (#) | Percent (%) | Cumulative percent (%) | |
|---|---|---|---|
| Suspected intention | |||
| Confusion | 137 | 40.1 | 40.1 |
| Conspiracy theories | 93 | 27.2 | 67.3 |
| Help with prevention | 34 | 9.9 | 77.2 |
| Help with treatment | 22 | 6.4 | 83.6 |
| Phishing/scam/spam | 19 | 5.6 | 89.2 |
| Virus transmission | 12 | 3.5 | 92.7 |
| Sales of meds/products | 11 | 3.2 | 95.9 |
| Diagnostics | 2 | 0.6 | 96.5 |
| Humor | 2 | 0.6 | 97.1 |
| Other | 10 | 2.9 | 100.0 |
| Linked to | |||
| None/nothing | 159 | 46.5 | 46.5 |
| Website and social media | 83 | 24.3 | 70.8 |
| Website only | 51 | 14.9 | 85.7 |
| Hashtags | 26 | 7.6 | 93.3 |
| Government organizations | 6 | 1.8 | 95.0 |
| Tweeter | 5 | 1.5 | 96.5 |
| Phone number | 2 | 0.6 | 97.1 |
| Graphics | 2 | 0.6 | 97.7 |
| 1 | 0.3 | 98.0 | |
| Other | 7 | 2.0 | 100.0 |
| Against | |||
| Science | 176 | 51.5 | 51.5 |
| Prevention measures | 20 | 5.8 | 57.3 |
| USA | 14 | 4.1 | 61.4 |
| China | 13 | 3.8 | 65.2 |
| Covid information | 13 | 3.8 | 69.0 |
| Vaccines | 13 | 3.8 | 72.8 |
| Unicef | 12 | 3.5 | 76.3 |
| Politician | 11 | 3.2 | 79.5 |
| Technology | 11 | 3.2 | 82.7 |
| Treatment | 6 | 1.8 | 84.5 |
| Pharma | 4 | 1.2 | 85.7 |
| Celebrity | 3 | 0.9 | 86.5 |
| Governments | 3 | 0.9 | 87.4 |
| CDC | 2 | 0.6 | 88.0 |
| WHO | 2 | 0.6 | 88.6 |
| Diagnosis | 2 | 0.6 | 89.2 |
| Japan | 2 | 0.6 | 89.8 |
| Western Countries | 2 | 0.6 | 90.4 |
| Others | 33 | 9.6 | 100.0 |
The remaining 40% was scattered in messages against countries like the USA and other western countries, Japan or China; multilateral or national government organizations like UNICEF, WHO, CDC and the Military; politicians, celebrities and the pharma industry. A crosstabs analysis of countries, intentions and links was discarded due to the number of messages needed to have a meaningful analysis. Indeed, most messages were not including any links to other websites or social media platforms (46.5%; n = 159). The messages with some sort of linkages derived toward the combination of a website and a social media outlet (24.3%; n = 83); a website alone (14.9%; n = 51) or a social media outlet alone (9.1%; n = 31).
DISCUSSION
This study appears to be one of the first attempts to examine the content of fake news related to COVID-19 in a global context. Our findings illustrate the main characteristics of misinformation and disinformation and help to close some gaps in the existing body of literature.
Identified trends
Although the findings should be interpreted with caution, this study has several strengths. In first place, this study is of particular relevance to illustrate how FNM has been distributed globally and has used many of the most spoken languages in the world. According to Etnologue (Eberhard et al., 2020), English, for instance, is the most commonly used language in the world for business, travel, and international businesses; it is the most frequently learnt as a person’s second language, and the third when considering native speakers worldwide. Spanish, second in the order of languages used for FNM, is the second in number of native speakers, right after the Chinese Mandarin. Portuguese comes in third place for use of languages in misinformation/disinformation and in seventh place among the most spoken languages globally. Therefore, language selection for the design and distribution of the COVID-19-related infodemic is an essential component.
Second, this exploratory descriptive content analysis unveiled some trend in the themes involved and the social media platforms used for FNM distribution. The challenges are to transfer curated, current and easy to understand knowledge supported by evidence-based, best practices in the areas of disease prevention, early detection and diagnosis, and proper treatment to the people who need it most, at a pace better than the one fake news has (Chan et al., 2020). Additionally, purposive social media mining of these same themes becomes an essential tool to anticipate the onset of new efforts of distribution of misinformation/disinformation (Xie et al., 2020). Therefore, groups willingly distributing fake news use a global network-of-network dynamics that crossover and interconnect social media platforms, usually through back doors found in their structures, allowing them to jump between countries and languages (Johnson, 2019). In this context, our findings about the most frequently used digital platforms uphold the need for the use of computational social science tools (Ledford, 2020) to understand and maximize the effectiveness of new public health promotion and education interventions.
Third, this widespread distribution of FNMs about prevention, diagnosis, remedies, cures or treatments for COVID-19 on Facebook, Twitter and all the other social media outlets, often amplified by politicians and news media (Figure 3) has contributed to injuries and fatalities. This is where the elements of eHealth literacy come in play to understand individuals’ health information patterns of behavior, their skills to distinguish true from false information, and an opportunity to put digital health information to a good use to help our communities to make informed decisions (Xie et al., 2020).
Fig. 3:
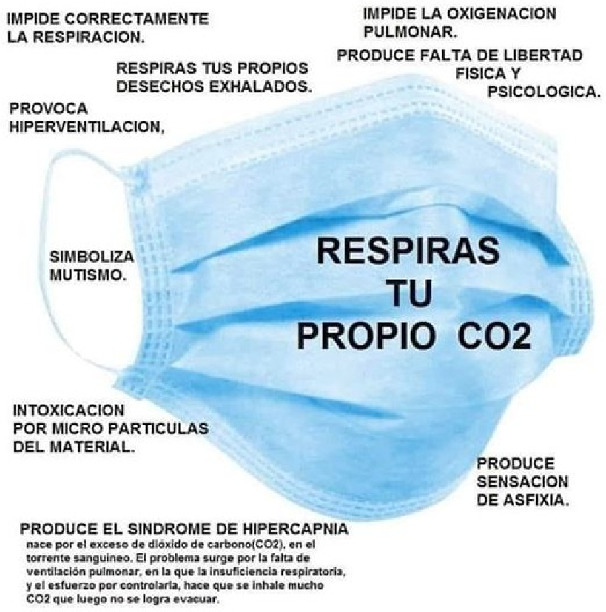
COVID-19 fake information about face masks in Spanish.
When we compared the list of countries with the highest frequency of publication of FNM (Figure 1) with the list of countries with most peer-reviewed publications in health literacy (Hernandez, 2013), some countries appear in both lists yet a valid correlation was not possible because of the heterogeneity and lack of uniformity in the measures and structures of this two different studies (Ratzan et al., 2013). Furthermore, research on health literacy has shown that more than one-third of the world population has difficulties in finding, understanding, evaluating and using information that is necessary to manage their health even when they live in developed countries (Van den Broucke, 2020).
Implications for public health promotion and education
There are a number of practical implications for public health promotion and education professionals. First, it is fundamental to advocate and enforce emergency policies at the systems’ level, would build up skills needed by practitioners in order to deliver more effective, faster and cost-effective responses to the misinformation/disinformation challenges. Second, practitioners must urge national, regional and local governments, health care public health leaders and decision makers to integrate and coordinate efforts to avoid missing key opportunities for prevention and early interventions. Lack of coordination limits drastically the levels and quality of care available, as an example, those aimed at solving behavioral health needs (Evans and Bufka, 2020). Third, securing policies that will warrant the timely provision of sufficient and adequate personal protection equipment in to first line responders, including their families and close relatives, during the COVID-19 pandemic (Chungtai et al., 2020).
Our findings also suggest that some extremist movements are capitalizing the pandemic situation to disseminate harmful and hateful messages on social media, especially against immunization strategies to combat COVID-19 based on the heterogeneity of existing vaccination strategies, existing but in diverse phases of clinical trials (Pandey et al., 2020). In this point, it would be essential to capitalize on existing successful global vaccination campaigns such as the Global Polio Eradication Initiative (GPEI), supported by national governments, multilateral agencies like WHO, and private non-for-profit organizations like Rotary International and the Bill and Melinda Gates Foundation (Rahi and Sharma, 2020). Third, there is a definite need for access and analysis of data, to support, preferably in real-time, a quick evaluation and adjustment of ongoing public health promotion and education interventions in the middle of contention measures such as home confinement, shelter-in-place or social distancing (Pan et al., 2020).
Health promotion and education techniques to address FNM
There are multilayered risks to the health of the population inherent to the use of internet and social media outlets. In order to help reduce the spread of COVID-19 FNM and to protect health information, some strategies and techniques have been proposed. Initially, health promotion and education practitioners must be aware of the quality of the information they review and produce. Second, and in parallel, local, regional and national governments should implement directives regulating what health information is available to the public, this without censoring basic freedoms (Cuan-Baltazar et al., 2020).
Another strategy is to design and implement a health literacy and user empowerment campaigns with the support of traditional and social media outlets. The goal of this strategy is that users acquire the tools necessary to identify, process, share and amplify high-quality information, thus subsequently correcting any misinformation seen on social media (Vraga et al., 2020). In this same direction, another strategy consist in recovering the trust of the population and help them develop fact-checking capacities to filtering out perceptions heavily influenced by message contents that have little to do with facts (Krause et al., 2020).
Limitations of the study
The findings in this report are subject to some limitations. First, our sources of information were not curated nor standardized and were heavily exposed to processing or manipulations done by the originators of false rumors or FNMs. Second, the time period selected was arbitrary. It did not reflect any particular technical recommendation or timeline already described in the literature. Hence, our choice of time would not be replicable in other content analyses. Third, as our sample was not probabilistic in nature, the results of our study are not generalizable and respond only to the messages collected.
Last but not least, an important limitation in our study was related to the exploratory nature of the study and the lack of predefinition and validation of concept categories. Although it is recommended that researchers define a structure that accurately measures the combination of ideas/concepts/themes, especially if embedded in graphic environments, the method used to reduce the complexity into more simple and manageable units of analysis only allowed the use of descriptive statistics.
CONCLUSIONS AND RECOMMENDATIONS
The simultaneous COVID-19 pandemic and the fake news infodemic, affected the public health and health care responses from already debilitated systems and services that were caught isolated, underfinanced, unprepared and understaffed. This was worsened through the confusion created in the community by the avalanche of misinformation and disinformation related to COVID-19 and the resulting erosion in the credibility of genuine media and institutional channels. Some of this confusion was strategically created and propagated globally by groups with extremist political ideologies of all sorts or negationist, medical freedom, anti-vaccine agendas looking to take advantage of the crisis and sabotage any organized responses fueling anti-government sentiments.
On top of this already chaotic situation, there were diverse degrees of disconnection between local and national governments with their corresponding health authorities. Public health and health care practitioners, first-line responders, and hospital staff, clinical and non-clinical, had to face people’s unpredictable behaviors, panic, tensions and, in some cases, an open hostile climate.
Future directions
With these frantic scenarios in mind, health care, public health promotion and education practitioners must adjust current and future interventions with a plan to create and distribute curated, evidence-based content that would neutralize FNM swiftly and effectively. The plans have to include the creation and management of digital platforms communities that will deploy messages in strategic ways. As the time for production, distribution, and massive application of a safe and effective vaccine to prevent COVID-19 is approaching, we must anticipate and be prepared for the occurrence of new waves of false rumors, misinformation, disinformation and fake news coming from known perpetrators. It is essential and urgent to improve workforce capacities to understand current social, structural and political challenges in order to create high-impact solutions to the existing conundrums.
This study was designed to perform a content analysis of publicly available COVID-19 related FNM in social media platforms. This should the base for future research efforts that will explore more comprehensively the content and distribution of public health-related messages in the social media platforms, including but not limited to, the use of probabilistic samples, automated analysis and the inclusion of health and e-health literacy.
SUPPLEMENTARY MATERIAL
Supplementary material is available at Health Promotion International online.
FUNDING
This work was prepared with authors’ own resources. No external funding was used. Dr Atehortua and Ms Patino had no relevant financial and non-financial relationships.
CONFLICT OF INTEREST STATEMENT
None declared.
Supplementary Material
REFERENCES
- Barua Z., Barua S., Aktar S., Kabir N., Li M. (2020) Effects of misinformation on COVID-19 individual responses and recommendations for resilience of disastrous consequences of misinformation. Progress in Disaster Science, 8, 100119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Biohackinfo.com. (2020) Bill Gates Will Use Microchip Implants to Fight Coronavirus. Biohackinfo.Com. https://biohackinfo.com/news-bill-gates-id2020-vaccine-implant-covid-19-digital-certificates/ Last accessed on June 19th, 2020. [Google Scholar]
- Broniatowski D. A., Jamison A. M., Qi S. H., AlKulaib L., Chen T., Benton A. et al. (2018) Weaponized health communication: Twitter Bots and Russian Trolls amplify the vaccine debate. American Journal of Public Health, 108, 1378–1384. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chan A., Nickson C. P., Rudolph J. W., Lee A., Joynt G. M. (2020) Social media for rapid knowledge dissemination: early experience from the COVID-19 pandemic. Anaesthesia, 75, 1579–1582. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chatterjee S. S., Barikar C. M., Mukherjee A. (2020) Impact of COVID-19 pandemic on pre-existing mental health problems. Asian Journal of Psychiatry, 51, 102071. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chughtai A. A., Seale H., Islam M. S., Owais M., Macintyre C. R. (2020) Policies on the use of respiratory protection for hospital health workers to protect from coronavirus disease (COVID-19). International Journal of Nursing Studies, 105, 103567. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cuan-Baltazar J. Y., Muñoz-Perez M. J., Robledo-Vega C., Pérez-Zepeda M. F., Soto-Vega E. (2020) Misinformation of COVID-19 on the internet: infodemiology study. JMIR Public Health and Surveillance, 6, e18444. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eberhard D. M., Simons G. F., Fennig C. D. (eds) (2020) Ethnologue: Languages of the World, 23rd edn. SIL International, Dallas, TX. http://www.ethnologue.com. [Google Scholar]
- Evans A. C., Bufka L. F. (2020) The critical need for a population health approach: addressing the Nation’s Behavioral Health During the COVID-19 pandemic and beyond. Preventing Chronic Disease, 17, E79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fredericks B. (2020) Roger Stone: Bill Gates may have created coronavirus to microchip people. The New York Post. https://nypost.com/2020/04/13/roger-stone-bill-gates-may-have-created-coronavirus-to-microchip-people/
- Gérard A., Romani S., Fresse A., Viard D., Parassol N., Granvuillemin A. et al. (2020) “Off-label” use of hydroxychloroquine, azithromycin, lopinavir-ritonavir and chloroquine in COVID-19: a survey of cardiac adverse drug reactions by the French Network of Pharmacovigilance Centers. Therapies, 75, 371–379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hayes A. F., Krippendorff K. (2007) Answering the call for a standard reliability measure for coding data. Communication Methods and Measures, 1, 77–89. http://www.unc.edu/courses/2007fall/jomc/801/001/HayesAndKrippendorff.pdf (last accessed 15 June 2020). [Google Scholar]
- Hernandez L. M. (ed.) (2013) Health Literacy: Improving Health, Health Systems, and Health Policy around the World: Workshop Summary. National Academies Press, Washington DC. [PubMed] [Google Scholar]
- Johnson N. F., Leahy R., Restrepo N. J., Velasquez N., Zheng M., Manrique P. et al. (2019) Hidden resilience and adaptive dynamics of the global online hate ecology. Nature, 573, 261–265. [DOI] [PubMed] [Google Scholar]
- Krause N. M., Freiling I., Beets B., Brossard D. (2020) Fact-checking as risk communication: the multi-layered risk of misinformation in times of COVID-19. Journal of Risk Research, 23:7,8, 1052–1059, doi: 10.1080/13669877.2020.1756385. [Google Scholar]
- Krippendorff K. (2004) Content Analysis, an Introduction to Its Methodology, Vol. 11, 2nd edn. Sage Publications, Thousand Oaks, CA, pp. 211−–256.. [Google Scholar]
- Krippendorff K. (2004) Reliability in content analysis. Some common misconceptions and recommendations. Human Communication Research, 30, 411–433. [Google Scholar]
- Ledford H. (2020) How Facebook, Twitter and other data troves are revolutionizing social science. Nature, 582, 328–330. [DOI] [PubMed] [Google Scholar]
- Lopes B., Bortolon C., Jaspal R. (2020) Paranoia, hallucinations and compulsive buying during the early phase of the COVID-19 outbreak in the United Kingdom: a preliminary experimental study. Psychiatry Research, 293, 113455. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Metzl J. M., Maybank A., De Maio F. (2020) Responding to the COVID-19 pandemic. The need for a structurally competent health care system. JAMA, 324, 231–232. [DOI] [PubMed] [Google Scholar]
- Pan A., Liu L., Wang C., Guo H., Hao X., Wang Q. et al. (2020) Association of public health interventions with the epidemiology of the COVID-19 outbreak in Wuhan, China. JAMA, 323, 1915–1923. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pandey S. C., Pande V., Sati D., Upreti S., Samant M. (2020) Vaccination strategies to combat novel corona virus SARS-CoV-2. Life Sciences, 256, 117956. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pulker C. E., Trapp G. S. A., Scott J. A., Pollard C. M. (2018) Global supermarkets’ corporate social responsibility commitments to public health: a content analysis. Globalization and Health, 14, 121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rademakers J., Heijmans M. (2018) Beyond reading and understanding: health literacy as the capacity to act. International Journal of Environmental Research and Public Health, 15, 1676. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rahi M., Sharma A. (2020) Mass vaccination against COVID-19 may require replays of the polio vaccination drives. EClinicalMedicine, 25, p100501. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ratzan S. C., Weinberger M. B., Apfel F., Kocharian G. (2013) The digital health scorecard: a new health literacy metric for NCD prevention and care. Global Heart, 8, 171–179. [DOI] [PubMed] [Google Scholar]
- Riehm K. E., Holingue C., Kalb L. G., Bennett D., Kapteyn A., Jiang Q. et al. (2020) Associations between media exposure and mental distress among US adults at the beginning of the COVID-19 pandemic. American Journal of Preventive Medicine, 59, 630–638. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Singh M. (2020) WhatsApp tests New Feature to Fight Misinformation: Search the Web. TechCrunch. https://techcrunch.com/2020/03/21/whatsapp-search-web-coronavirus/ (last accessed 25 May 2020).
- Sutherland G., Kemp C., Studdert D. M. (2016) Mandatory responses to public health and safety recommendations issued by coroners: a content analysis. Australian and New Zealand Journal of Public Health, 40, 451–456. [DOI] [PubMed] [Google Scholar]
- U.S. Department of Health and Human Services, Office of Disease Prevention and Health Promotion. (2015) Health Literacy Online: A Guide to Simplifying the User Experience. Washington, DC. https://health.gov/healthliteracyonline/ (last accessed 25 May 2020).
- Van den Broucke S. (2020) Why health promotion matters to the COVID-19 pandemic, and vice versa. Health Promotion International, 35, 181–186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Velasquez N., Leahy N., Johnson Restrepo N., Lupu Y., Sear R., Gabriel N. (2020) Hate multiverse spreads malicious COVID-19 content online beyond individual platform control. arXiv: 2004.00673v2 [Physics.soc-ph]. https://arxiv.org/abs/2004.00673 (last accessed 5 June 2020). [Google Scholar]
- Vosoughi S., Roy D., Aral S. (2018) The spread of true and false news online. Science, 359, 1146–1151. [DOI] [PubMed] [Google Scholar]
- Vraga E. K., Tully M., Bode L. (2020) Empowering users to respond to misinformation about Covid-19. Media and Communication, 8, 475–479. [Google Scholar]
- Waldrop T., Alsup D., McLaughlin E. (2020) Fearing Coronavirus, Arizona Man Dies After Taking A Form of Chloroquine Used to Treat Aquariums. CNN.com, 25 March 2020. https://www.cnn.com/2020/03/23/health/arizonacoronavirus-chloroquine-death/index.html (last accessed 20 October 2020).
- Wilbur K., Berzou S., Meeds R. (2017) Framing diabetic public health information during Ramadan – a newspaper content analysis. Journal of International Medical Research, 45, 1750–1759. [DOI] [PMC free article] [PubMed] [Google Scholar]
- World Health Organization. (2020) Munich Security Conference. WHO Director-General Speech. Geneva, Switzerland. https://www.who.int/dg/speeches/detail/munich-security-conference (last accessed 28 June 2020).
- Xie B., He D., Mercer T., Wang Y., Wu D., Fleischmann K. R. et al. (2020) Global health crises are also information crises: a call to action. Journal of the Association for Information, Science and Technology, 2020;71:1419–1423. https://doi:10.1002/asi.24357 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zardo P., Collie A. (2014) Measuring use of research evidence in public health policy: a policy content analysis. BMC Public Health, 14, 496. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhang X., Lyu H., Luo J. (2020) Understanding the hoarding behaviors during the COVID-19 pandemic using large scale social media data. arXiv Preprint arXiv: 2010.07845. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.