

Editor
Postponing surgeries as a rapid response to SARS-CoV-2 pandemic was the clue to decrease disease spread in patients and health care professionals1,2. Non-urgent, non-cancer procedures were cancelled, and staff was reallocated to face the emergency, with most surgical departments closed or converted to COVID-19 medical wards3. Cancellation of elective operations creates a huge backlog of planned surgical patients, but no real data are currently available to assess the number of delayed operations and how this will be managed in the pandemic transition phase4,5.
We conducted a retrospective study to compare the surgical volume (defined as the number of procedures performed during the index period) and characteristics of patients undergoing surgery in the period January–March 2019 and 2020. Data were retrieved from the Operating Room Logs of all private and public hospitals in Tuscany (Italy), a region with a population of 3·73 millions and 322 intensive care beds (8,63/100 K inhabitants). We considered demographics, Charlson index, urgent or elective admission, mortality and return to operating room within 7 days. Other variables recorded were median time from diagnosis to surgery, operative time and total time spent in the operating room area. Differences between groups were assessed by non-parametric tests (χ2 and Kolmogorf-Smirnow). The statistical software Stata 14 SE was used for data analysis.
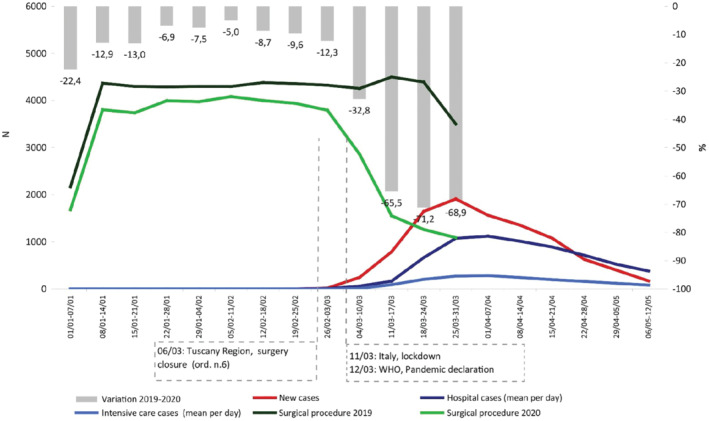
Between February 25th and May 19th, 9968 cases of Covid-19 were diagnosed and at the peak of the epidemic curve on April the 2nd, 91·3 per cent of the ICU beds (294) were used for SARS-CoV-2 patients. Regional government interrupted elective surgeries on March 6th, 1 week before WHO declaration of pandemic and Italian lockdown (Fig. 1). Between March 6th and 31th, a total of 4774 surgical procedures were performed, with a reduction of 68 per cent when compared to 2019 (14798). The reduction was higher for elective surgery (2796 vs. 11273) with a decrease of 75 per cent, while for urgent/emergency surgery the decrease was 30 per cent. Patients treated in 2020 were older (median age 67 vs. 63, p < 0·001) and the patients' rate with Charlson comorbidity index ≥2 was higher (36·4 per cent vs. 24·8 per cent). Admission to postoperative sub-intensive/intensive care was higher in 2020 (3·1 per cent vs. 2·8 per cent and 7·3 per cent vs. 6·2 per cent respectively). The median waiting time for elective surgery was shorter (6 vs. 23 days, p < 0·001). Median operative time and stay in the operating room area were both significantly higher (55 vs. 46 and 141 vs. 130 minutes respectively). Rate of patients with Clavien-Dindo 3b post-operative complications requiring a second procedure within 7 days was significant higher (5·8 per cent vs. 3·0 per cent, p < 0·001). Higher operative times and total operating room stay could be explained by the presence of SARS-CoV-2 related procedures.
Provision of surgical services will continue to be an essential aspect of our healthcare system throughout the pandemic, and surgical systems will have to adapt to a continuously changing situation. The results of our study provide important informations to define the impact of SARS-CoV-2 on elective surgery and set a benchmark to manage local planning and resource prioritization during the transition phase, ensuring quality standards and safety of patients and staff.
References
- 1. Di Marzo F, Sartelli M, Cennamo R, Toccafondi G, Coccolini F, La Torre Get al. Recommendations for General Surgery Activities in a Pandemic Scenario (SARS-CoV-2). Br J Surg 2020; 10.1002/bjs.11652 [Epub ahead of print]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Brindle ME, Gawande A. Managing COVID-19 in Surgical Systems. Ann Surg 2020; 10.1097/SLA.0000000000003923 [Epub ahead of print]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Torzilli G, Vigano L, Galvanin J, Castoro C, Quagliuolo V, Spinelli A, Zerbi A, Donadon M, Montorsi M; COVID-SURGE-ITA group . A Snapshot of Elective Oncological Surgery in Italy During COVID-19 Emergency: Pearls, Pitfalls, and Perspectives. Ann Surg 2020; 10.1097/SLA.0000000000004081 [Epub ahead of print]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. CovidSurg Collaborative, Nepogodiev D, Bhangu A. Elective surgery cancellations due to the COVID-19 pandemic: global predictive modelling to inform surgical recovery plans. Br J Surg 2020; 10.1002/bjs.11746. [Epub ahead of print]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Søreide K, Hallet J, Matthews JB, Schnitzbauer AA, Line PD, Lai PBSet al. Immediate and long-term impact of the COVID-19 pandemic on delivery of surgical services. Br J Surg 2020; 10.1002/bjs.11670 [Epub ahead of print]. [DOI] [PMC free article] [PubMed] [Google Scholar]