

Supplemental Digital Content is available in the text.
Keywords: cerebral microbleed, extracorporeal membrane oxygenation, macrohemorrhage
Abstract
Objectives:
Current studies lack robust information on the prevalence and associated factors of cerebral microbleeds in patients who underwent extracorporeal membrane oxygenation.
Design:
Retrospective analysis.
Setting:
We reviewed patients who underwent (extracorporeal membrane oxygenation) and subsequent brain autopsy with gross and microscopic examinations from January 2009 to December 2018 from a single tertiary center.
Patients:
Twenty-five extracorporeal membrane oxygenation patients (median age, 53 yr; interquartile range, 36–61 yr; 17 women and 8 men) underwent brain autopsy.
Interventions:
Descriptive analysis of neuropathologic findings. Cerebral microbleed was defined as a small focus (< 10 mm diameter) of accumulation of blood product in the brain tissue. Macrohemorrhage was defined as any of the grossly identifiable epidural, subdural, subarachnoid, or intraparenchymal hemorrhages larger than 10 mm.
Measurement and Main Results:
Of 25 (22 venoarterial extracorporeal membrane oxygenation; three venovenous extracorporeal membrane oxygenation), 15 patients (60%) were found to have cerebral microbleeds, whereas 13 (52%) had macrohemorrhages, of whom five (20%) had both. Overall, 92% of brains demonstrated the presence of either cerebral microbleeds or macrohemorrhages after extracorporeal membrane oxygenation support. Of the patients with cerebral microbleeds, lobar cerebral microbleeds (80%) occurred more frequently than deep cerebral microbleeds (60%), with 40% of patients having both types. The cases of macrohemorrhages consisted of one epidural (8%), two subdural (15%), and 10 subarachnoid hemorrhages (77%). In univariate analyses, the presence of macrohemorrhages was significantly associated with the presence of cerebral microbleeds (p = 0.03) with odds ratio of 0.13 (CI, 0.02–0.82). Age, sex, extracorporeal membrane oxygenation duration, extracorporeal membrane oxygenation type, use of aspirin or dialysis during extracorporeal membrane oxygenation support, bloodstream infections, hemoglobin, platelets, and coagulopathy profiles were not associated with cerebral microbleeds.
Conclusions:
In patients with postmortem neuropathologic evaluation, 92% sustained acute cerebral microbleeds or macrohemorrhages after extracorporeal membrane oxygenation support. Cerebral microbleeds were commonly present in the majority of extracorporeal membrane oxygenation nonsurvivors. Further research is necessary to study the long-term sequelae, such as cognitive outcome of extracorporeal membrane oxygenation-associated cerebral microbleeds in extracorporeal membrane oxygenation survivors.
Intracranial hemorrhage, namely intraparenchymal hemorrhage, subarachnoid hemorrhage, and subdural hematoma, is a well-described complication of patients on extracorporeal membrane oxygenation (ECMO) with rates of 2–21% (1). However, there are sparse data on cerebral microbleeds (CMBs) in ECMO with prior studies only being at the case-report level (2–4). CMB is one of the phenotypes of cerebral small vessel disease, which also includes lacunar infarct, enlarged perivascular space, punctate infarcts, cortical superficial siderosis, and white matter disease (5). CMBs are particular concerning, as they have been reported to be associated with future hemorrhagic stroke, ischemic stroke, worse cognitive deterioration, and dementia in the general population, in addition to having a high prevalence of CMBs in patients with other forms of cardiac devices with continuous blood flow, such as the left ventricular assist device (6, 7).
Although CMBs can readily be detected by gradient-echo T2-weighted or susceptibility weighted imaging of MRI, the ECMO circuit serves as a barrier for MRI imaging, thereby preventing detection of CMBs in people during ECMO support. Furthermore, CT imaging of the head generally cannot detect CMBs. Although performing transcranial Doppler and electroencephalogram have been explored in ECMO patients to identify emboli or to assist with neuroprognostication respectively, they are not expected to discover CMBs (8). Thus, we investigated primarily the prevalence of CMBs at the time of autopsy in people who were on ECMO and secondarily the risk factors associated with their presence.
METHODS
This study used a retrospective approach for people on ECMO who were found to either have or not have CMBs at time of autopsy. Adult patients (age ≥18 yr) on ECMO between the years 2010 and 2018 at Johns Hopkins Hospital were identified by chart review of electronic medical records. Of these, only patients who underwent autopsy were selected for analysis. Gross and microscopic examinations of the brains were performed by neuropathologists with standardized procedures. Following 10 days of immersion fixation in 10% buffered formalin, the brains were examined grossly. Representative tissue sections from the cerebral cortex, basal ganglia, basal forebrain, thalamus, hippocampus, entorhinal cortex, amygdala, midbrain, pons, medulla, and cerebellum were processed routinely in paraffin, and sections were stained with hematoxylin-eosin. The definition of CMBs followed its neuroradiological and neuropathologic standard as accumulation of blood products less than 10 mm in greatest dimension in the brain tissue (Fig. 1) (9). The locations of the hemorrhages were categorized as deep or lobar, with the prior being defined as those in the basal ganglia, internal capsule, cerebellum, or brain stem, and the latter being defined as those in the cortical gray matter or subcortical white matter within the frontal, parietal, temporal, or occipital lobes.
Figure 1.
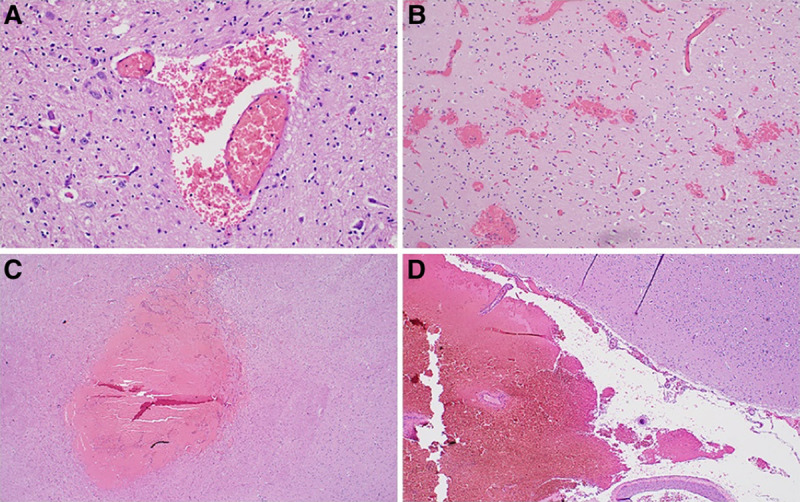
Manifestations of cerebral microbleeds in adult brains of patients who have received extracorporeal membrane oxygenation treatment. Cerebral microbleeds range from perivascular accumulation of blood cells (A), petechial hemorrhages (B), to small focus of bleeding (C) which require microscopic examination, in comparison with the subarachnoid hemorrhage (D) that is easily seen grossly.
The following 12 variables were hypothesized to be associated with CMBs based on clinical insight and literature review: presence of macrohemorrhages (subarachnoid hemorrhages, epidural hemorrhages, subdural hemorrhages, or intraparenchymal hemorrhages) at time of autopsy, age at time of ECMO, sex, ECMO duration, ECMO type, lowest hemoglobin value during ECMO, lowest platelet count during ECMO, highest international normalized ratio (INR) value during ECMO, highest activated partial thromboplastin time (aPTT) during ECMO, use of aspirin during ECMO, use of dialysis during ECMO, and bloodstream infection during ECMO (6, 10). The results of these variables were collected by reviewing electronic clinical records of each patient. All patients were on a continuous IV heparin drip during ECMO support. This study was approved by Johns Hopkins Institutional Review Board (IRB) and ethics committee (IRB: 19-01-09-01RD).
STATISTICAL ANALYSIS
Computing environment R (Foundation for Statistical Computing, Vienna, Austria) was used for statistical analysis. Because the data were not normally distributed for most of the variables, the median value and interquartile range (IQR) of each range were reported, rather than the mean and range. Univariate logistic regression models were created with the aforementioned independent variables and the dependent variable set as the presence of CMBs. p values less than 0.05 were considered to be statistically significant.
RESULTS
Twenty-five patients (median age, 53 yr; IQR, 36–61 yr; 17 women and 8 men) who had undergone ECMO and subsequent autopsy with available brain tissue fixated in microscope slides were identified (Supplemental Table, Supplemental Digital Content 1, http://links.lww.com/CCX/A520). The median ECMO support time was 84 hours (IQR, 21–160 hr), and the autopsy interval from death was 24 hours (IQR, 14–37 hr). Twenty-two patients (88%) underwent venoarterial-ECMO (VA-ECMO) cannulation, whereas three (12%) underwent venovenous-ECMO (VV-ECMO). The most common indication for VA-ECMO was cardiogenic shock (40%), followed by cardiac arrest (32%). VV-ECMO was exclusively reserved for use in patients with acute respiratory distress syndrome. The median values of various hematologic laboratory values during ECMO were as follows: lowest hemoglobin 6.5 g/dL (IQR, 5.3–7.6 g/dL), lowest platelet 27,000 K/cu mm (IQR, 19,000–40,000 K/cu mm), highest INR 2.1 (IQR, 1.5–3.8), and highest aPTT 200 seconds (IQR, 76–200 s). During ECMO, eight patients (32%) were on aspirin therapy during ECMO support, seven patients (28%) required dialysis, and five patients (20%) were affected by acute bloodstream infections.
Of 25, 15 (60%) had CMBs, whereas 13 (52%) had macrohemorrhages, with a total of 23 (92%) having either or both types of hemorrhage (Supplemental Table, Supplemental Digital Content 1, http://links.lww.com/CCX/A520). Of the patients with CMBs, nine patients (60%) had deep hemorrhages, 12 patients (80%) had lobar hemorrhages, and six patients (40%) had both types. Of the patients with macrohemorrhages, there were one epidural (8%), two subdural (15%), and 10 subarachnoid hemorrhages (77%), but no large intraparenchymal hemorrhage. From the univariate logistic regression analysis, the presence of macrohemorrhages significantly associated with the presence of CMBs (p = 0.03) with odds ratio of 0.13 (CI, 0.02–0.82) (Table 1).
TABLE 1.
Univariate Logistic Regression Models for Cerebral Microbleeds
| Independent Variables | Beta | se | OR | p |
|---|---|---|---|---|
| Macrohemorrhage | –2.08 | 0.96 | 0.12 | 0.03 |
| Age at ECMO initiation (yr) | 0.01 | 0.02 | 1.01 | 0.79 |
| Sex | 0.37 | 0.98 | 1.45 | 0.70 |
| ECMO duration (hr) | 0.00 | 0.00 | 1.00 | 0.93 |
| ECMO type | 17.38 | 2,284.10 | 3.53 × 107 | 0.99 |
| Hemoglobin | 0.58 | 0.34 | 1.79 | 0.08 |
| Platelet | 0.02 | 0.02 | 1.02 | 0.30 |
| International normalized ratio | –0.27 | 0.25 | 0.76 | 0.29 |
| Activated partial thromboplastin time | 0.00 | 0.01 | 1.00 | 1.00 |
| Aspirin use | –1.39 | 0.90 | 0.25 | 0.13 |
| Dialysis | –1.87 | 0.99 | 0.15 | 0.06 |
| Bloodstream infection | 0.00 | 1.02 | 1.00 | 1.00 |
ECMO = extracorporeal membrane oxygenation, OR = odds ratio.
DISCUSSION
We hereby report the largest study conducted to date regarding the occurrence of CMBs in ECMO patients, which revealed that the majority of them had CMBs (60%) and at greater prevalence than macrohemorrhages (52%). The fact that the average interval from death to autopsy was 24 hours was not considered to influence the frequency of CMBs, as CMBs do not occur postmortem. It is important to note that 92% of ECMO nonsurvivors had acute hemorrhages in the CNS when their brains were examined after ECMO decannulation. It is also well known that intracranial macrohemorrhages and CMBs are strong predictors of long-term cognitive impairment in the general population (7). As the use of ECMO is increasing exponentially with a better understanding in ECMO-associated neurologic complications, future research should focus on the mechanism and risk factor of neurologic injury such as CMB and its impact on long-term neurologic outcome (10).
The univariate logistic regression model with the statistically significant independent variable revealed that the presence of macrohemorrhages was inversely associated with the presence of CMBs, likely related to their distinct mechanisms (5, 11). It is unclear as to why the presence of CMBs was protective of having macrohemorrhages. Although macrohemorrhages are most likely related to the use of anticoagulation and coagulopathy in ECMO, the mechanisms of CMBs may be associated with cerebral small vessel disease secondary to multiple risk factors such as refractory hypoxia, critical care illness, sepsis, and inflammation (2, 5, 10). However, it is also possible that these CMBs may have been present even before the ECMO cannulation. Despite the generally low platelet counts, elevated INRs, and elevated aPTTs of the patients, the presence of CMBs was not significantly associated with factors that commonly lead to increased hemorrhage, including lowest platelet count, highest INR or aPTT values, use of dialysis, or use of aspirin during ECMO. The presence of CMBs was also not significantly associated with the duration of ECMO. One prior study reported a 50% rate of neurologic events in ECMO patients, including subarachnoid hemorrhage, ischemic infarcts, hypoxic-ischemic encephalopathy, unexplained coma, and brain death (12). However, it is important to acknowledge that our model is limited by a small sample size, and overinterpretation should be avoided.
This study has several limitations. First, the sample size is small at 25 patients, although it is thus far the highest among studies evaluating CMBs in ECMO patients. Second, the detection of further CMBs may have been limited by certain factors including ECMO duration that was too short in some patients or only a limited number of brain tissue slices being analyzed under the microscope for each patient. Third, the study lacked a control group. Future studies are needed to understand both the acute and chronic effects of CMBs on patient outcome.
CONCLUSIONS
A total of 92% of patients in our study sustained acute CMBs or macrohemorrhages after ECMO support. CMBs were commonly present in the majority of ECMO nonsurvivors. The routine practice of performing autopsies in ECMO nonsurvivors would be beneficial for deepening the understanding of neurologic and pathologic correlations related to CMBs. Further research is necessary to study the long-term sequelae, such as cognitive outcome of ECMO-associated CMBs in ECMO survivors.
Supplementary Material
Footnotes
Drs. Chen and Cho are cosenior authors.
Supplemental digital content is available for this article. Direct URL citations appear in the printed text and are provided in the HTML and PDF versions of this article on the journal’s website (http://journals.lww.com/ccxjournal).
The authors have disclosed that they do not have any potential conflicts of interest.
REFERENCES
- 1.Fletcher-Sandersjöö A, Thelin EP, Bartek J, Jr, et al. Incidence, outcome, and predictors of intracranial hemorrhage in adult patients on extracorporeal membrane oxygenation: A systematic and narrative review. Front Neurol. 2018; 9:548. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Gijs J, Lambert J, Meyfroidt G, et al. Cerebral microbleeds and intracerebral hemorrhage associated with veno-venous extracorporeal membrane oxygenation. Acta Neurol Belg. 2018; 118:513–515 [DOI] [PubMed] [Google Scholar]
- 3.Le Guennec L, Bertrand A, Laurent C, et al. Diffuse cerebral microbleeds after extracorporeal membrane oxygenation support. Am J Respir Crit Care Med. 2015; 191:594–596 [DOI] [PubMed] [Google Scholar]
- 4.Shah J, Armstrong MJ. Extracorporeal membrane oxygenation: Uncommon cause of corpus callosal microhemorrhage. Neurology. 2015; 84:630. [DOI] [PubMed] [Google Scholar]
- 5.Pantoni L. Cerebral small vessel disease: From pathogenesis and clinical characteristics to therapeutic challenges. Lancet Neurol. 2010; 9:689–701 [DOI] [PubMed] [Google Scholar]
- 6.Yoshioka D, Okazaki S, Toda K, et al. Prevalence of cerebral microbleeds in patients with continuous-flow left ventricular assist devices. J Am Heart Assoc. 2017; 6:e005955. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Akoudad S, Wolters FJ, Viswanathan A, et al. Association of cerebral microbleeds with cognitive decline and dementia. JAMA Neurol. 2016; 73:934–943 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Cho SM, Ziai W, Mayasi Y, et al. Noninvasive neurological monitoring in extracorporeal membrane oxygenation. ASAIO J. 2020; 66:388–393 [DOI] [PubMed] [Google Scholar]
- 9.Greenberg SM, Vernooij MW, Cordonnier C, et al. ; Microbleed Study Group. Cerebral microbleeds: A guide to detection and interpretation. Lancet Neurol. 2009; 8:165–174 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Cho SM, Farrokh S, Whitman G, et al. Neurocritical care for extracorporeal membrane oxygenation patients. Crit Care Med. 2019; 47:1773–1781 [DOI] [PubMed] [Google Scholar]
- 11.Greenberg SM, Nandigam RN, Delgado P, et al. Microbleeds versus macrobleeds: Evidence for distinct entities. Stroke. 2009; 40:2382–2386 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Mateen FJ, Muralidharan R, Shinohara RT, et al. Neurological injury in adults treated with extracorporeal membrane oxygenation. Arch Neurol. 2011; 68:1543–1549 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.