

Summary:
Burnout in medicine has become a national epidemic, affecting greater than one third of physicians, and yet physicians, departments, and institutions remain ill equipped to address it. Burnout is a syndrome characterized by emotional exhaustion, depersonalization, and a reduced sense of accomplishment that occurs as a response to one’s environment. We have a moral and ethical imperative to address physician burnout, as it has immense implications within healthcare. Solutions have historically focused on changing the behavior of the individual, but research has demonstrated that long-lasting change is brought about by intervening at the organizational level, which requires that leadership champion these efforts. Departmental and hospital leadership play a critical role in addressing the drivers of burnout. Here, we outline evidence-based strategies to combat physician burnout at both the individual and organizational levels and review what has been explored within the field of plastic surgery.
Happiness is when what you think, what you say, and what you do are in harmony.
—Mahatma Gandhi1
THE PROBLEM
Burnout in medicine has become a national epidemic, and yet physicians, departments, and institutions remain ill equipped to address it.2 The term “burnout” was first used in 1974 to describe the exhaustion observed in people in “healing professions.”3 Maslach4 further conceptualized burnout as a syndrome characterized by emotional exhaustion, depersonalization, and a reduced sense of accomplishment at work. The 6 major contributing factors to burnout include work overload, lack of autonomy or control, insufficient reward, breakdown of community, lack of fairness, and a mismatch between the values of the employer and employee (Table 1). The impact of each on an individual’s experience of burnout can be measured using the Maslach Burnout Inventory.4
Table 1.
Maslach’s Areas of Work Life
| Maslach’s Areas of Work Life |
|---|
| Workload |
| Control |
| Reward |
| Community |
| Fairness |
| Values |
The struggle of burnout is widespread. Greater than one third of physicians and surgeons are estimated to have high levels of burnout, with symptoms of burnout evident even among trainees and students.5,6 A systematic review and meta-analysis found that 27% of medical students screened positive for depression and 11% reported suicidal ideation during medical school.7 Similarly, 28% of residents screened positive for depression and 60% for burnout.8 Though faring slightly better than other surgical specialties, plastic surgeons are not immune to this phenomenon with a reported rate of burnout ranging between 30% and 37%.5,9,10 Factors that increase rates of burnout among plastic surgeons include middle age, subspecialty practice including microsurgery or aesthetic surgery, greater than 70 hours worked per week, greater than 2 nights of call per week, junior academic rank, and nonsalaried compensation.11,12 Among aesthetic surgeons, the growing demands of the marketplace and patient expectations may contribute to burnout.13 Factors that are protective against burnout among plastic surgeons include being in practice for over 15 years, serving as a program director, and being over the age of 60.10
A 2020 cross-sectional study of plastic surgery residents reported a rate of burnout of nearly 60%.14 Risk factors include dissatisfaction with plastic surgery as a career, feeling uninvolved in program decisions, excessive call, dissatisfaction with income, and dissatisfaction with his or her role in the operating room.14,15 Training in a program with fewer than 6 residents, having fewer than 2 weeks of vacation per year, and working greater than 80 hours per week were also found to increase the rate of burnout.16 Work hour reform alone, however, is insufficient to reduce levels of burnout, as levels remain high even after ACGME-mandated work hour restrictions, highlighting the multifaceted nature of the problem.
We have a moral and ethical imperative to address physician burnout, which contributes to alcohol and substance abuse, career dissatisfaction, depression, and even suicide.9,17,18 Although the lifetime rate of depression is similar among physicians to that of the general population, the rate of suicide is disproportionately higher, ranging from 1.1 to 3.4 times the rate of the general population in male physicians and 2.5 to 5.7 times in female physicians.3 A staggering 300–400 physicians are lost to suicide annually.19
Physician burnout also has considerable implications in healthcare delivery. As burnout progresses, work performance is affected to the detriment of patient care, leading to decreased quality of care, patient satisfaction, and productivity and increased medical errors and physician turnover.6,20 This applies to resident physicians as well, who report more self-perceived errors.21 There is also business rationale to institutional investment in reducing burnout, as increased productivity, decreased turnover, and fewer malpractice suits ultimately lowers costs.19,20
Given the significant and costly effects of physician burnout, a substantial amount of research has been conducted to explore how burnout can be mitigated. However, investigation into the prevention and reduction of burnout has traditionally focused on interventions by the individual. Individual-based interventions that have been shown to promote wellness include stress management, self-care, communication skills training, facilitated small group discussion, gratitude interventions, and professional coaching.22–24 The focus of these interventions is often the cultivation of skills such as resiliency, mindfulness, and reflection.19,25 For trainees, peer mentoring, professional development coaching, exercise, discussion of imposter syndrome, and access to healthy foods and self-care resources such as primary care physicians and dentists have been shown to support well-being.19,26–28 Although individual-based interventions can help to promote positive attitudes, bolster confidence, and decrease depersonalization, they do not necessarily result in decreased levels of burnout.19,20 As such, these efforts have been criticized as misguided and even victim-blaming, as research has demonstrated that burnout is a response to the environment, necessitating greater focus on organization-directed interventions to reduce burnout.20
The causes of burnout have been well studied.4 Here, we outline evidence-based strategies to combat physician burnout on both the individual and organizational levels and report what has been explored within the field of plastic surgery. Following PRISMA guidelines, a PubMed search was performed using the following search terms: “burnout” AND “plastic surgery” AND “intervention,” which resulted in 36 English references. Abstracts were reviewed and unrelated references were excluded, resulting in 14 remaining references. An additional 46 references were included after review of the bibliography (Fig. 1).
Fig. 1.
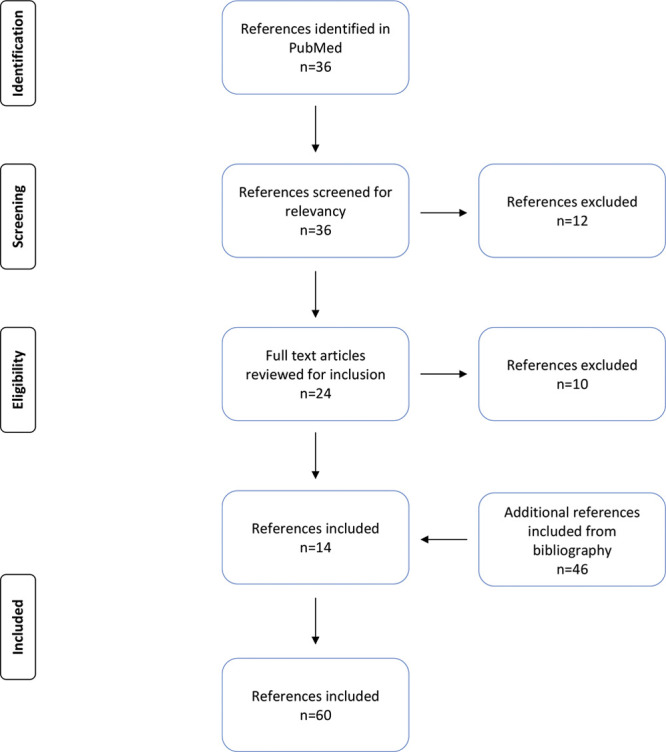
Flow diagram of references.
ORGANIZATIONAL LEADERSHIP
The role of organizational leadership on tackling burnout is paramount. Leadership qualities, attributes, and management styles have a direct impact on physician satisfaction and burnout. Transformational qualities and skills such as mentorship, coaching, instilling pride, discussing values and purpose, praising accomplishments, and identifying individual needs and talents result in the highest rates of physician satisfaction.29,30 Notably, these are skills that can be learned. To effect long-lasting and meaningful reductions in burnout, it is necessary and crucial for organizational leadership to demonstrate a commitment to creating a culture of wellness, model change, and address the problem of burnout at the systemic and organizational level.
Effective organization-directed interventions target key drivers in the workplace: workload and job demands, efficiency and resources, control and flexibility, work-life integration, social support and community at work, alignment of individual and organizational cultures and values, and meaning in work.20 Interventions to address burnout at the organizational level and also within the context of plastic surgery are reviewed.
ORGANIZATIONAL INTERVENTIONS
Workload, Job Demands, Efficiency, and Resources
High workload intensity, characterized by excessive hours, nights on call, and patients seen in the office per week is an often-cited contributing factor to burnout. This is true of plastic surgeons as well, as those who work more hours, take more call, and have less vacation time have higher rates of burnout.11,12,16 Moreover, inefficiency or underutilization of resources resulting in increased clerical work or mundane tasks is also significantly associated with the symptoms of burnout. Additionally, electronic health records (EHRs) have increased regulatory requirements without improvement in patient engagement, workflow, or usability.2,3,31
Strategies that target the problem of excessive workload at the systemic level include modifications to work processes, shortened shifts or rotation lengths, and duty hour requirements.31 Other factors to consider include productivity targets, method of compensation, quality of support staff, utilization of scribes and advanced practice providers, processes for scheduling and ordering, and optimization of the EHR.20 The use of scribes in a plastic surgery practice was shown to decrease physician workload and costs while improving operational efficiency.32 There is also growing demand for telemedicine, for which plastic surgery consultation is quite amenable and has been well received by patients. Telemedicine can potentially promote delivery of specialized care, facilitate multidisciplinary collaboration, and decrease costs; however, implementation remains a challenge and further investigation is warranted in regards to effect on workload and efficiency.33,34
Resident clinical workload has quantifiably increased in the last 3 decades with little change in the resident workforce.35–37 This includes the number and acuity of the patients on a census, the rate of patient turnover, the location of patients within the hospital, and the number of admissions, discharges, total operations, operating room hours, clinic visits, hours worked, and days on call per week. This may be especially important in smaller programs where rates of burnout are higher.16 Despite this, an estimated 23% of resident’s on-duty time is spent on noneducational activities.35 Programs should eliminate the tasks that increase residents’ workload at the expense of education and consider optimizing the role of physician extenders and streamlining EHR and other workflow processes.31,35,38
Control, Flexibility, and Work-life Integration
Lack of control over one’s schedule is one of the most significant drivers of burnout.20,39 Among physicians working for the Kaiser healthcare system, lack of control and autonomy in the workplace was the single most important predictor of burnout.40 It has been suggested that physician happiness is not related to the workload itself, but to the perceived ability to manage it.41
Flexibility to adjust work effort, work hour distribution, and start times gives physicians influence over their schedule.20 This applies to residents as well, as higher rates of resident disengagement and burnout have been reported for plastic surgery residents not involved in program decisions that impact them.14 Residents should be able to make scheduling requests, be provided accommodations within the hospital for overnight call, and have progression of clinical autonomy.38 Attention should also be given to policies regarding the call schedule, vacation time, sick leave, child care, maternity and paternity leave, and cross coverage, as work-life interference may be more directly related to burnout than the work itself.20
A time-banking system, which administers credit for extra time rendered in service, can encourage a work culture of flexibility and collaboration. A pilot study conducted at Stanford University rewarded unacknowledged time spent on teaching, service and clinical activities with practical rewards to improve work-life integration.42 Support services offered enhanced time at work (grant-writing, laboratory management, and public speaking) and also at home (house cleaning, laundry, and meal delivery). The program significantly increased faculty wellness and institutional satisfaction, prompting initiation of a similar program for residents.
Social Support and Community at Work
Social support is a key factor to prevent burnout and improve health and happiness. The quality and quantity of social relationships affect mental and physical health through behavioral, psychosocial, and physiologic pathways. A longitudinal study involving nearly 7000 people over a 9-year period found that those with more social ties had greater lifespans independent of socioeconomic status, smoking, drinking, or exercise.43 It is postulated that strong social support dampens the negative effects of the stress response by reducing cortisol levels, which may explain why those with more social relationships live longer and have greater cognitive function into old age.44 Social belonging has also been shown to play an important role in resident well-being and retention, highlighting the importance of building community and enhancing relationships within the work environment.45
Mentorship has been demonstrated to cultivate professional relationships, build camaraderie, promote professional development, and increase job satisfaction.46 Other interventions to decrease isolation and build community include social events, celebration of shared accomplishments, team building exercises, faculty and resident retreats, and optimization of shared workspaces.19
Residency programs fulfill an important role in community building and have a responsibility to create opportunities for resident relationships to form and strengthen. At Brigham and Women’s Hospital, such opportunities are offered not only in the form of class dinners and holiday parties, but also through longitudinal peer discussion groups, bringing together those with similar research or career interests.47 Opportunities to encourage faculty and resident engagement should also be provided. In a cross-sectional study, weekly rounds with senior surgeons and frequent staff meetings to discuss complex cases or interpersonal issues were protective against burnout in plastic surgery residents.48
Alignment of Individual and Organizational Cultures, Values, and Meaning in Work
Competing interests between an organization and its individual employees play a significant role in burnout. Healthcare organizations must clearly articulate their values and mission so that leadership can model and embody these values, using them to guide decision-making at the local level.20,30 These include prioritizing patient care over profit and trusting physicians to act in accordance with patient’s best interests. Recognition of accomplishments, appreciation of hard work, and alignment of individual talents to specific needs can help to cultivate a culture of mutual respect, appreciation, and teamwork.
Meaning and purpose are incredibly important to physician satisfaction and can be strengthened through professional development and opportunities to focus on personal interests. The degree to which faculty spend time on work they find most meaningful is directly related to burnout. Physicians who spend at least 20% of their professional effort on what they find most meaningful had a 50% reduction in their rate of burnout compared to those who spent less time.49
Residency programs must also support and educate residents in a manner that cultivates meaning and purpose. Quality of hours worked is more important than number in regard to resident perceptions on wellness and burnout. This requires a paradigm shift, especially in surgical specialties, as the experiential or immersion method of learning associated with the historical apprenticeship model is no longer appropriate. Graduate medical education should seek to develop a curriculum based on the competencies by which trainees are evaluated, requiring that education is organized and goal-oriented, incorporating objective-driven lectures, skills training laboratories, and deliberate practice in the operating room utilizing adult learning theory.35,50
Residencies should also create an environment that fosters psychological safety, including support in handling moral distress, swift response to concerns regarding unprofessional conduct, and access to mental health services.19,20,38 Shame-based learning, such as verbal abuse, mocking, exclusion, public embarrassment, and intimidation, is not conducive to learning. Shame reactions are described as sentinel emotional events, having devastating consequences resulting in social isolation, disengagement from learning, impaired wellness, unprofessional behavior, and impaired empathy.51 A survey of Canadian plastic surgery programs revealed that a majority of residents experienced shaming in the operating room resulting in loss of confidence, professional isolation, poor job performance, and depression.52 Trainees learn and perform best from surgical educators who promote a culture of respect, accountability, and collegiality.53
Increasing clinical demands and malpractice costs in the face of diminishing reimbursement and state budget cuts to higher education have made it difficult for academic plastic surgeons to prioritize resident education.50,54 Academic plastic surgeons feel that departments and institutions are unsupportive of educational effort, and it has been shown that academic faculty are largely uncompensated for the time they spend teaching.55,56 Institutions must support, incentivize, and reward faculty participation in resident education. Implementation of an educational value unit resulted in significantly increased faculty contribution to targeted educational activities such as conference attendance and completion of resident evaluations in an academic emergency medicine department.57 Such a system could easily be tailored to the specific needs and goals of a department.
ENACTING CHANGE
The individual physician cannot combat burnout alone. Long-lasting change is the result of the effort put forth by organizational leadership that acknowledges the influence of the local work environment on burnout and recognizes the responsibility they share in mitigating and preventing burnout (Table 2).3,19,20
Table 2.
Solutions to Burnout: Considerations on an Individual and Organization Level
| Solutions to Burnout | ||
|---|---|---|
| Considerations on an Individual Level | Considerations on an Organizational Level | |
| Workload, job demands, efficiency, and resources | ♦ Stress management ♦ Self-care ♦ Exercise ♦ Gratitude Interventions ♦ Professional coaching (mindfulness, resiliency) |
♦ Shortened shifts ♦ Productivity targets ♦ Method of compensation ♦ Modifications to work processes and flow ♦ Optimization of EHR ♦ Quality of support staff ♦ Use of scribes and APPs |
| Control, flexibility, and work-life integration | ♦ Organizational skills ♦ Personal efficiency ♦ Personal factors that may affect work-life |
♦ Flexibility over start times and work hour distribution ♦ Policies regarding scheduling requests, cross coverage, vacation, sick leave, maternity and paternity leave ♦ Time-banking system ♦ Access to self-care resources |
| Social support and community | ♦ Communication skills training ♦ Facilitated small group discussion |
♦ Social events ♦ Team building and retreats ♦ Optimization of shared workspaces |
| Alignment of cultures and values and meaning in work | ♦ Mentorship | ♦ Professional development ♦ Educational value unit |
To begin to effect change within an organization, leadership must recognize the problem of burnout, recognize the role they play in its prevention, and be open and willing to commit to change.
A team of invested stakeholders and physicians are assembled to perform a needs assessment and prioritize what they see as the major drivers of their burnout.
Solutions that target their specific key drivers of burnout are developed and implemented.
Outcomes and impact on burnout are measured so that modifications for improvement can be made.
This process should be implemented at both the organizational level to support academic faculty and at the programmatic level to support resident physicians.19 At a time when the rate of burnout among physicians was increasing nationally Mayo Clinic reduced burnout by 7% over 2 years despite already having a rate of burnout lower than the national average by following such a model.20 To accomplish this they utilized the Listen-Act-Develop model, an empirically validated model for physician engagement and a tool to better understand specific drivers of burnout and empower physicians to develop and implement targeted solutions. The CEO met with department chairs and staff in various formats, including town hall meetings, radio broadcasts, video interviews, and face-to-face meetings to identify departments with higher-than-average rates of burnout. A team of physicians and administrators then met with these department chairs, as well as departmental focus groups, to identify local challenges and drivers of burnout and devise-specific solutions, with follow-up surveys demonstrating a significant decrease in burnout.58
A similar model can be applied to residency training programs to better understand the drivers of resident burnout and implement solutions.19 This may also help to foster communication, transparency, and clarification of the issues that hinder resident well-being, as program directors may be unaware or have difficulty understanding the scope of issues, despite wanting to improve wellness among residents. The development and implementation of a wellness curriculum may also be a useful adjunct in promoting a culture of wellness.59,60 Further research is necessary to elucidate the approach that plastic and reconstructive surgery departments, private practices, and residency programs can take to most effectively reduce burnout and promote wellness within their respective organizations.
CONCLUSIONS
Burnout has detrimental effects on physicians, their loved ones, and their patients. The problem is pervasive and affects greater than one third of physicians, including plastic surgeons. Burnout has historically been treated as an individual problem, but research has demonstrated that fixing the problem of burnout is a shared responsibility. Departmental and hospital leadership play a critical role in addressing the drivers of burnout and implementing change to achieve meaningful, long-lasting reductions in burnout and improve physician engagement. Further research is required to continue to address the specific drivers of burnout for plastic surgeons and plastic surgery trainees.
Footnotes
Published online 16 February 2021.
Disclosure: The authors have no financial interest to declare in relation to the content of this article.
REFERENCES
- 1.Smith D. Happiness: The Art of Living with Peace, Confidence, and Joy. 2nd ed. Columbus, Ohio: White Pine Mountain; 2014. [Google Scholar]
- 2.Khansa I, Janis JE. A growing epidemic: plastic surgeons and burnout—a literature review. Plast Reconstr Surg. 2019;144:298e–305e. [DOI] [PubMed] [Google Scholar]
- 3.Rothenberger DA. Physician burnout and well-being: a systematic review and framework for action. Dis Colon Rectum. 2017;60:567–576. [DOI] [PubMed] [Google Scholar]
- 4.Maslach C, Schaufeli WB, Leiter MP. Job burnout. Annu Rev Psychol. 2001;52:397–422. [DOI] [PubMed] [Google Scholar]
- 5.Kane L. Medscape plastic surgeon lifestyle, happiness & burnout report 2019. Available at: https://www.medscape.com/slideshow/2019-lifestyle-burnout-depression-6011056. Accessed July 31, 2020.
- 6.Shanafelt TD, Balch CM, Bechamps G, et al. Burnout and medical errors among American surgeons. Ann Surg. 2010;251:995–1000. [DOI] [PubMed] [Google Scholar]
- 7.Rotenstein LS, Ramos MA, Torre M, et al. Prevalence of depression, depressive symptoms, and suicidal ideation among medical students: a systematic review and meta-analysis. JAMA. 2016;316:2214–2236. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Mata DA, Ramos MA, Bansal N, et al. Prevalence of depression and depressive symptoms among resident physicians: a systematic review and meta-analysis. JAMA. 2015;314:2373–2383. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Streu R, Hansen J, Abrahamse P, et al. Professional burnout among US plastic surgeons: results of a national survey. Ann Plast Surg. 2014;72:346–350. [DOI] [PubMed] [Google Scholar]
- 10.Qureshi HA, Rawlani R, Mioton LM, et al. Burnout phenomenon in U.S. plastic surgeons: risk factors and impact on quality of life. Plast Reconstr Surg. 2015;135:619–626. [DOI] [PubMed] [Google Scholar]
- 11.Balch CM, Shanafelt TD, Sloan JA, et al. Distress and career satisfaction among 14 surgical specialties, comparing academic and private practice settings. Ann Surg. 2011;254:558–568. [DOI] [PubMed] [Google Scholar]
- 12.Ribeiro RVE, Martuscelli OJD, Vieira AC, et al. Prevalence of burnout among plastic surgeons and residents in plastic surgery: a systematic literature review and meta-analysis. Plast Reconstr Surg Glob Open. 2018;6:e1854. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Prendergast C, Ketteler E, Evans G. Burnout in the plastic surgeon: implications and interventions. Aesthet Surg J. 2017;37:363–368. [DOI] [PubMed] [Google Scholar]
- 14.Coombs DM, Lanni MA, Fosnot J, et al. Professional burnout in United States plastic surgery residents: is it a legitimate concern? Aesthet Surg J. 2020;40:802–810. [DOI] [PubMed] [Google Scholar]
- 15.Bin Dahmash A, Alhadlaq AS, Alhujayri AK, et al. Emotional intelligence and burnout in plastic surgery residents: is there a relationship? Plast Reconstr Surg Glob Open. 2019;7:e2057. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Hart AM, Crowley C, Janis JE, et al. Survey based assessment of burnout rates among US plastic surgery residents. Ann Plast Surg. 2020;85:215–220. [DOI] [PubMed] [Google Scholar]
- 17.Shanafelt TD, Balch CM, Dyrbye L, et al. Special report: suicidal ideation among American surgeons. Arch Surg. 2011;146:54–62. [DOI] [PubMed] [Google Scholar]
- 18.Oreskovich MR, Shanafelt T, Dyrbye LN, et al. The prevalence of substance use disorders in American physicians. Am J Addict. 2015;24:30–38. [DOI] [PubMed] [Google Scholar]
- 19.Sharp M, Burkart KM. Trainee wellness: why it matters, and how to promote it. Ann Am Thorac Soc. 2017;14:505–512. [DOI] [PubMed] [Google Scholar]
- 20.Shanafelt TD, Noseworthy JH. Executive leadership and physician well-being: nine organizational strategies to promote engagement and reduce burnout. Mayo Clin Proc. 2017;92:129–146. [DOI] [PubMed] [Google Scholar]
- 21.West CP, Tan AD, Habermann TM, et al. Association of resident fatigue and distress with perceived medical errors. JAMA. 2009;302:1294–1300. [DOI] [PubMed] [Google Scholar]
- 22.Rowe MM. Four-year longitudinal study of behavioral changes in coping with stress. Am J Health Behav. 2006;30:602–612. [DOI] [PubMed] [Google Scholar]
- 23.Emmons RA, McCullough ME. Counting blessings versus burdens: an experimental investigation of gratitude and subjective well-being in daily life. J Pers Soc Psychol. 2003;84:377–389. [DOI] [PubMed] [Google Scholar]
- 24.Dyrbye LN, Shanafelt TD, Gill PR, et al. Effect of a professional coaching intervention on the well-being and distress of physicians: a pilot randomized clinical trial. JAMA Intern Med. 2019;179:1406–1414. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Goodman MJ, Schorling JB. A mindfulness course decreases burnout and improves well-being among healthcare providers. Int J Psychiatry Med. 2012;43:119–128. [DOI] [PubMed] [Google Scholar]
- 26.Weight CJ, Sellon JL, Lessard-Anderson CR, et al. Physical activity, quality of life, and burnout among physician trainees: the effect of a team-based, incentivized exercise program. Mayo Clin Proc. 2013;88:1435–1442. [DOI] [PubMed] [Google Scholar]
- 27.Webb J, Brightwell A, Sarkar P, et al. Peer mentoring for core medical trainees: uptake and impact. Postgrad Med J. 2015;91:188–192. [DOI] [PubMed] [Google Scholar]
- 28.Villwock JA, Sobin LB, Koester LA, et al. Impostor syndrome and burnout among American medical students: a pilot study. Int J Med Educ. 2016;7:364–369. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Menaker R, Bahn RS. How perceived physician leadership behavior affects physician satisfaction. Mayo Clin Proc. 2008;83:983–988. [DOI] [PubMed] [Google Scholar]
- 30.Shanafelt TD, Gorringe G, Menaker R, et al. Impact of organizational leadership on physician burnout and satisfaction. Mayo Clin Proc. 2015;90:432–440. [DOI] [PubMed] [Google Scholar]
- 31.Schumacher DJ, Slovin SR, Riebschleger MP, et al. Perspective: beyond counting hours: the importance of supervision, professionalism, transitions of care, and workload in residency training. Acad Med. 2012;87:883–888. [DOI] [PubMed] [Google Scholar]
- 32.Cho J, Sanchez K, Ganor O, et al. Utilizing a physician scribe in a pediatric plastic surgical practice: a time-driven activity-based costing study. Plast Reconstr Surg Glob Open. 2019;7:e2460. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Funderburk CD, Batulis NS, Zelones JT, et al. Innovations in the plastic surgery care pathway: using telemedicine for clinical efficiency and patient satisfaction. Plast Reconstr Surg. 2019;144:507–516. [DOI] [PubMed] [Google Scholar]
- 34.Vyas KS, Hambrick HR, Shakir A, et al. A systematic review of the use of telemedicine in plastic and reconstructive surgery and dermatology. Ann Plast Surg. 2017;78:736–768. [DOI] [PubMed] [Google Scholar]
- 35.Brasel KJ, Pierre AL, Weigelt JA. Resident work hours: what they are really doing. Arch Surg. 2004;139:490–493. [DOI] [PubMed] [Google Scholar]
- 36.Luce EA. Beyond working hours: part I. Genesis and current difficulties. Plast Reconstr Surg. 2012;129:1015–1021. [DOI] [PubMed] [Google Scholar]
- 37.Zelenock GB, Holmes MM, Campbell DA, Jr, et al. Quantitative increases in surgical house officer clinical activity as the basis for increased work loads in a university hospital. Surgery. 1992;112:235–242. [PubMed] [Google Scholar]
- 38.Jennings ML, Slavin SJ. Resident wellness matters: optimizing resident education and wellness through the learning environment. Acad Med. 2015;90:1246–1250. [DOI] [PubMed] [Google Scholar]
- 39.Shanafelt TD, West CP, Poland GA, et al. Principles to promote physician satisfaction and work-life balance. Minn Med. 2008;91:41–43. [PubMed] [Google Scholar]
- 40.Freeborn DK. Satisfaction, commitment, and psychological well-being among HMO physicians. West J Med. 2001;174:13–18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Eckleberry-Hunt J, Kirkpatrick H, Taku K, et al. Relation between physicians’ work lives and happiness. South Med J. 2016;109:207–212. [DOI] [PubMed] [Google Scholar]
- 42.Fassiotto M, Simard C, Sandborg C, et al. An integrated career coaching and time-banking system promoting flexibility, wellness, and success: a pilot program at Stanford University School of Medicine. Acad Med. 2018;93:881–887. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Berkman LF, Syme SL. Social networks, host resistance, and mortality: a nine-year follow-up study of Alameda County residents. Am J Epidemiol. 1979;109:186–204. [DOI] [PubMed] [Google Scholar]
- 44.Hostinar CE, Gunnar MR. Social support can buffer against stress and shape brain activity. AJOB Neurosci. 2015;6:34–42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Salles A, Wright RC, Milam L, et al. Social belonging as a predictor of surgical resident well-being and attrition. J Surg Educ. 2019;76:370–377. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Janis JE, Barker JC. Medical student mentorship in plastic surgery: the mentor’s perspective. Plast Reconstr Surg. 2016;138:925e–935e. [DOI] [PubMed] [Google Scholar]
- 47.Berg DD, Divakaran S, Stern RM, et al. Fostering meaning in residency to curb the epidemic of resident burnout: recommendations from four chief medical residents. Acad Med. 2019;94:1675–1678. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Chaput B, Bertheuil N, Jacques J, et al. Professional burnout among plastic surgery residents: can it be prevented? Outcomes of a national survey. Ann Plast Surg. 2015;75:2–8. [DOI] [PubMed] [Google Scholar]
- 49.Shanafelt TD, West CP, Sloan JA, et al. Career fit and burnout among academic faculty. Arch Intern Med. 2009;169:990–995. [DOI] [PubMed] [Google Scholar]
- 50.Luce EA. Beyond working hours: part II. Incentive to improve. Plast Reconstr Surg. 2012;129:717e–720e. [DOI] [PubMed] [Google Scholar]
- 51.Bynum WE, IV, Artino AR, Jr, Uijtdehaage S, et al. Sentinel emotional events: the nature, triggers, and effects of shame experiences in medical residents. Acad Med. 2019;94:85–93. [DOI] [PubMed] [Google Scholar]
- 52.Boehm KS, McGuire C, Boudreau C, et al. The shame-blame game: is it still necessary? A national survey of shame-based teaching practice in Canadian plastic surgery programs. Plast Reconstr Surg Glob Open. 2019;7:e2152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Swendiman RA, Hoffman DI, Bruce AN, et al. Qualities and methods of highly effective surgical educators: a grounded theory model. J Surg Educ. 2019;76:1293–1302. [DOI] [PubMed] [Google Scholar]
- 54.Ruberg RL. Can academic plastic surgery survive? Ann Plast Surg. 2004;52:329–330. [DOI] [PubMed] [Google Scholar]
- 55.Sun HH, Pourtaheri N, Janis JE, et al. Do academic health care systems really value education? A survey of academic plastic surgeons. Plast Reconstr Surg Glob Open. 2018;6:e1948. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Shea S, Nickerson KG, Tenenbaum J, et al. Compensation to a department of medicine and its faculty members for the teaching of medical students and house staff. N Engl J Med. 1996;334:162–167. [DOI] [PubMed] [Google Scholar]
- 57.House J, Santen SA, Carney M, et al. Implementation of an Education Value Unit (EVU) system to recognize faculty contributions. West J Emerg Med. 2015;16:952–956. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Swensen S, Kabcenell A, Shanafelt T. Physician-organization collaboration reduces physician burnout and promotes engagement: the mayo clinic experience. J Healthc Manag. 2016;61:105–127. [PubMed] [Google Scholar]
- 59.Eckleberry-Hunt J, Van Dyke A, Lick D, et al. Changing the conversation from burnout to wellness: physician well-being in residency training programs. J Grad Med Educ. 2009;1:225–230. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Lefebvre D, Dong KA, Dance E, et al. Resident physician wellness curriculum: a study of efficacy and satisfaction. Cureus. 2019;11:e5314. [DOI] [PMC free article] [PubMed] [Google Scholar]