

Abstract
Little is known about the relationship between gut dysbiosis, inflammation, and adverse outcomes in patients with chronic kidney disease. We examined the association of microbial diversity with all-cause mortality in hemodialysis patients. The gut microbiota was assessed by 16S ribosomal RNA gene sequencing. During a median follow-up of 2.1 years, the adjusted risk of death among patients with higher diversity (above median) was 74% lower than that among patients with lower diversity (below median). We then compared the microbial composition between nonsurvivors and survivors in a matched case-control study. We observed significantly lower microbial diversity and higher proinflammatory cytokines among nonsurvivors than survivors. Specifically, the relative abundance of Succinivibrio and Anaerostipes, two short-chain fatty acid-producing bacteria, was markedly reduced in nonsurvivors. Thus, a unique gut microbial composition is associated with an increased risk of mortality among hemodialysis patients and may be used to identify subjects with a poor prognosis.
Subject terms: Applied microbiology, Clinical microbiology
Introduction
Patients with end-stage kidney disease (ESKD) receiving dialysis have a significantly reduced life expectancy compared to the general population1. Both cardiovascular (CV) and non-CV mortality risks are equally increased2. Identifying factors that are associated with this higher risk is important in the care of patients with ESKD. Observational studies among patients on dialysis have pointed out several predictors for the greater mortality risk, including older age and the high prevalence of comorbidities, especially diabetes mellitus (DM) and cardiovascular diseases (CVD) (traditional risk factors)3, as well as malnutrition, inflammation, and accumulation of uremic solutes (nontraditional risk factors)4–6.
A growing number of studies have shown that the gut microbiota is crucial for protecting against pathogens and maintaining normal immune and metabolic homeostasis7. The healthy human gastrointestinal tract harbors a highly diverse population of microorganisms. In contrast, uremia alters the normal composition and function of the gut microbiota, commonly referred to as gut dysbiosis8. Gut dysbiosis promotes local and systemic inflammation that leads to various pathological consequences. Accumulating evidence also indicates that gut-derived uremic toxins are involved in the pathogenesis of CVD in ESKD9.
Gut dysbiosis is characterized by loss of diversity and imbalance in composition. High α-diversity, a measure of bacterial richness and evenness, is often associated with better health status10. The association of lower microbial diversity with poor survival has been described in patients undergoing allogeneic hematopoietic-cell transplantation and in patients hospitalized for chronic obstructive pulmonary disease11,12. We have recently demonstrated that malnutrition and inflammation are correlated with a significant decrease in gut microbial diversity in patients with ESKD13,14. However, it is unclear whether decreased gut microbial diversity is associated with adverse outcomes in ESKD. The aim of this study was to explore whether gut dysbiosis can predict the risk of death in an observational ESKD cohort. Furthermore, we examined the gut microbiota profile among nonsurvivors and survivors in a matched case-control study.
Results
Patient characteristics
A total of 109 patients were enrolled in the study. Overall, the mean age was 68.4 ± 10.4 years, with 57 men and 52 women; 49.5% had DM (n = 54), and 45.9% had CVD (n = 50). The dialysis vintage was 8.0 (4.6–11.0) years. Across the 109 fecal samples, the total number of merged reads was 17,520,918, and after filtering steps, 11,968,852 reads were considered for analysis. Patients were stratified into higher-diversity and lower-diversity groups by the median Simpson index to evaluate the association between gut microbial diversity and mortality. We found that patients with lower diversity were more likely to have a higher prevalence of CVD and other comorbidities and had a significantly lower subjective global assessment (SGA) score, Physical Activity Scale for the Elderly (PASE) score, and plasma intact parathyroid hormone but significantly higher inflammatory markers, including interleukin-6 (IL-6) and tumor necrosis factor-α (TNF-α) (Table 1). Microbial diversity, expressed as the Simpson index, was significantly correlated with several baseline variables, including body mass index (BMI) (rs = 0.252, P = 0.008), SGA score (rs = 0.263 P = 0.008), PASE score (rs = 0.309, P = 0.004), IL-6 (rs = −0.293, P = 0.002), and TNF-α (rs = −0.264, P = 0.011) (Fig. 1). The correlations remained significant after adjustment for age, sex, and the Charlson comorbidity index, as determined by Spearman’s partial correlation analyses. The gut microbial composition among patients with higher and lower microbial diversity at the phylum and genus levels are shown in Supplementary Fig. 1.
Table 1.
Baseline characteristics of patients according to the median Simpson index.
| Parameter | Lower diversity (n = 54) | Higher diversity (n = 55) | P Value |
|---|---|---|---|
| Age (years) | 69 ± 11 | 68 ± 10 | 0.486 |
| Male sex, n (%) | 32 (59.3%) | 25 (45.5%) | 0.149 |
| DM, n (%) | 29 (53.7%) | 25 (45.5%) | 0.389 |
| CVD, n (%) | 32 (59.3%) | 18 (32.7%) | 0.005 |
| Charlson comorbidity index | |||
| 1–2 | 1 (1.9%) | 0 (0.0%) | |
| 3–4 | 5 (9.3%) | 15 (27.3%)a | 0.035 |
| ≥5 | 48 (88.9%) | 40 (72.7%)a | |
| Dialysis vintage (years) | 7.5 (4.8–12.0) | 8.0 (4.0–11.0) | 0.752 |
| Dialysis access type | |||
| Arteriovenous fistula | 47 (87.0%) | 49 (89.1%) | |
| Arteriovenous graft | 6 (11.1%) | 6 (10.9%) | 0.597 |
| Central venous catheter | 1 (1.9%) | 0 (0.0%) | |
| BMI (kg/m2) | 23.2 ± 3.5 | 24.5 ± 3.4 | 0.053 |
| FTI (kg/m2) | 8.9 ± 4.1 | 10.2 ± 3.9 | 0.098 |
| LTI (kg/m2) | 13.3 ± 3.6 | 13.7 ± 2.7 | 0.596 |
| BF (%) | 27.8 ± 10.9 | 30.1 ± 9.3 | 0.230 |
| Overhydration (%) | 4.1 (−3.2–9.7) | 4.5 (−2.5–10.9) | 0.445 |
| SGA score | 6.0 (5.0–7.0) | 6.0 (6.0–7.0) | 0.007 |
| PASE score | 32 (9–59) | 58 (35–86) | 0.002 |
| Medication | |||
| PPI, n (%) | 5 (9.4%) | 5 (9.1%) | 0.951 |
| Calcium carbonate, n (%) | 40 (75.5%) | 49 (89.1%) | 0.063 |
| CCB, n (%) | 26 (49.1%) | 25 (45.5%) | 0.708 |
| β-blocker, n (%) | 24 (45.3%) | 27 (49.1%) | 0.692 |
| RAASi, n (%) | 20 (37.7%) | 16 (29.1%) | 0.341 |
| Dietary intake (servings/day) | |||
| Vegetables | 2.4 (1.5–3.3) | 2.2 (1.6–3.1) | 0.867 |
| Fruits | 0.9 (0.3–1.1) | 0.6 (0.3–1.4) | 0.904 |
| Meat | 0.9 (0.4–1.3) | 0.7 (0.4–1.3) | 0.699 |
| Laboratory parameters | |||
| Kt/V | 1.7 ± 0.4 | 1.7 ± 0.3 | 0.740 |
| nPNA (g/kg/day) | 1.2 ± 0.2 | 1.1 ± 0.3 | 0.755 |
| Albumin (g/dl) | 3.9 ± 0.3 | 4.0 ± 0.4 | 0.536 |
| Fasting glucose (mg/dl) | 115 (96–150) | 109 (100–140) | 0.587 |
| Total cholesterol (mg/dl) | 153 (136–191) | 157 (138–179) | 0.901 |
| LDL (mg/dl) | 86 (66–106) | 90 (73–106) | 0.248 |
| Triglycerides (mg/dl) | 102 (70–177) | 101 (70–151) | 0.513 |
| Calcium (mmol/l) | 9.3 ± 0.8 | 9.3 ± 0.9 | 0.753 |
| Phosphorus (mg/dl) | 5.1 ± 1.4 | 5.3 ± 1.2 | 0.296 |
| iPTH (pg/ml) | 257 (107–425) | 398 (187–605) | 0.034 |
| CRP (mg/dl) | 0.32 (0.17–0.85) | 0.23 (0.14–0.61) | 0.154 |
| IL-6 (pg/ml) | 12.38 (6.35–18.91) | 6.46 (4.07–11.83) | 0.002 |
| TNF-α (pg/ml) | 5.02 (1.86–10.76) | 2.57 (0.68–5.89) | 0.009 |
BF body fat, BMI body mass index, CCB calcium channel blocker, CRP C-reactive protein, CVD cardiovascular disease, DM diabetes mellitus, FTI fat tissue index, IL-6 interleukin-6, iPTH intact parathyroid hormone, LDL low-density lipoprotein, LTI lean tissue index, nPNA normalized protein nitrogen appearance, PASE the Physical Activity Scale for the Elderly, PPI proton pump inhibitor, RAASi renin-angiotensin-aldosterone system inhibitor, SGA subjective global assessment; TNF-α tumor necrosis factor-α.
aP < 0.05 between the lower-diversity and the higher-diversity group by the Bonferroni post hoc test.
Fig. 1. Factors associated with the Simpson index.

Univariate analysis of the correlation of the Simpson index with a BMI, b SGA score, c PASE score, d IL-6, and e TNF-α. Natural logarithmic transformation of IL-6 and TNF-α was used to normalize the distributions for univariate analyses. BMI body mass index, IL-6 interleukin-6, PASE the Physical Activity Scale for the Elderly, SGA subjective global assessment, TNF-α tumor necrosis factor-α.
Association between microbial diversity and survival
During a median follow-up of 2.1 years, 15 (13.8%) patients died. The majority of deaths were due to non-CV causes (n = 11), whereas 4 patients died of CVD. The most common causes of non-CV death were infections (n = 5) and malignancies (n = 2). Kaplan–Meier analysis showed that the risk of death was significantly greater in patients with lower diversity (n = 54) than in those with higher diversity (n = 55) (P = 0.015) (Fig. 2). The estimated overall survival was 94.5% for the higher-diversity group and 77.8% for the lower-diversity group. Cox proportional hazards analyses for overall survival are shown in Table 2. Microbial diversity at baseline was significantly associated with the risk of death from any cause. Specifically, patients with higher diversity had 74% risk reduction for mortality compared with their lower-diversity counterparts in age-, sex-, and comorbidity-adjusted models (adjusted hazard ratio, 0.26; 95% confidence interval, 0.07–0.95, P = 0.041).
Fig. 2. Kaplan–Meier analysis curves.
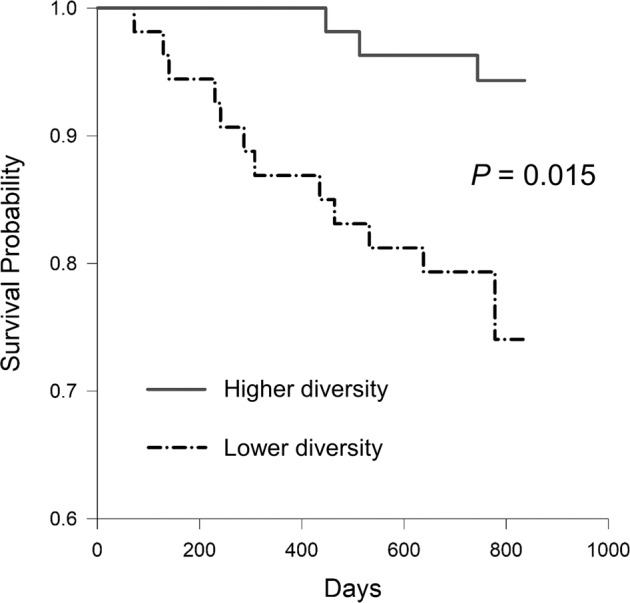
Hemodialysis patients were stratified by the median of the Simpson index to assess the unadjusted risks for all-cause mortality.
Table 2.
Multivariable Cox regression analysis for the relative risk of all-cause mortality calculated for a Simpson index below or above the median.
| Unadjusted | Model 1 | Model 2 | |
|---|---|---|---|
| HR (95% CI) | HR (95% CI) | HR (95% CI) | |
| Simpson index by median | |||
| Lower | 1.0 | 1.0 | 1.0 |
| Higher | 0.24 (0.07–0.84) | 0.24 (0.07–0.87) | 0.26 (0.07–0.95) |
| P value | 0.026 | 0.030 | 0.041 |
CI confidence interval, HR hazard ratio.
Model 1 was adjusted for age and sex.
Model 2 was adjusted for age, sex, and the Charlson comorbidity index.
Additional analyses for microbial diversity with risk of CV events and infection-related hospitalizations are shown in Supplementary Table 1. There were 24 CV events, including nonfatal myocardial infarction (n = 10), nonfatal stroke (n = 3), hospitalization for congestive heart failure (n = 7), and CV death (n = 4). Twenty-eight subjects experienced an infection event requiring hospitalization, consisting of pulmonary infection (n = 13), genitourinary infection (n = 2), gastrointestinal or hepatobiliary infection (n = 2), skin and soft tissue infection (n = 4), bloodstream infection or sepsis (n = 4), and other infections (n = 3). We found that higher microbial diversity was associated with a significantly lower risk of CV events (adjusted hazard ratio, 0.36; 95% confidence interval, 0.15–0.88, P = 0.026). However, there was no significant association between microbial diversity and the risk of infection (adjusted hazard ratio, 0.71; 95% confidence interval, 0.33–1.52, P = 0.374).
Characteristics of nonsurvivors and survivors
In general, nonsurvivors (n = 15) were older than survivors (n = 94) (Table 3). Otherwise, the two groups were similar regarding sex, the prevalence of DM and preexisting CVD, dialysis vintage, physical activity, and nutritional status, including the SGA score, BMI, and serum albumin. In addition, there was no significant difference in the use of medications known to affect the gut microbiota, as well as dietary consumption patterns of vegetables, fruits, or meat between the two groups. We observed that nonsurvivors had significantly lower levels of total cholesterol and low-density lipoprotein cholesterol but significantly higher levels of IL-6 and TNF-α than survivors. Moreover, a significantly lower proportion of nonsurvivors used arteriovenous fistula as vascular access compared to survivors.
Table 3.
Baseline characteristics of patients according to mortality status before matching.
| Characteristic | Dead (n = 15) | Alive (n = 94) | P Value |
|---|---|---|---|
| Age (years) | 74 ± 10 | 68 ± 10 | 0.031 |
| Male sex, n (%) | 7 (46.7%) | 50 (53.2%) | 0.638 |
| DM, n (%) | 6 (40.0%) | 48 (51.1%) | 0.426 |
| CVD, n (%) | 9 (60.0%) | 41 (43.6%) | 0.237 |
| Charlson comorbidity index | |||
| 1–2 | 0 (0.0%) | 1 (1.1%) | |
| 3–4 | 0 (0.0%) | 20 (21.3%) | 0.126 |
| ≥5 | 15 (100.0%) | 73 (77.7%) | |
| Dialysis vintage (years) | 7.0 (6.0–9.0) | 8.0 (4.1–11.1) | 0.747 |
| Dialysis access type | |||
| Arteriovenous fistula | 10 (66.7%) | 86 (91.5%) | |
| Arteriovenous graft | 4 (26.7%) | 8 (8.5%) | 0.004 |
| Central venous catheter | 1 (6.7%) | 0 (0.0%) | |
| BMI (kg/m2) | 22.6 ± 3.3 | 24.0 ± 3.5 | 0.146 |
| FTI (kg/m2) | 8.7 ± 4.7 | 9.7 ± 3.9 | 0.363 |
| LTI (kg/m2) | 13.4 ± 3.0 | 13.5 ± 3.2 | 0.886 |
| BF (%) | 27.2 ± 12.5 | 29.2 ± 9.8 | 0.469 |
| Overhydration (%) | 5.8 (−5.4–12.4) | 4.1 (−2.6–10.0) | 0.829 |
| SGA score | 5.5 (5.0–7.0) | 6.0 (6.0–7.0) | 0.082 |
| PASE score | 9 (0–68) | 51 (23–67) | 0.080 |
| Medication | |||
| PPI, n (%) | 1 (7.1%) | 9 (9.6%) | 0.770 |
| Calcium carbonate, n (%) | 10 (71.4%) | 79 (84.0%) | 0.248 |
| CCB, n (%) | 6 (42.9%) | 45 (47.9%) | 0.726 |
| β-blocker, n (%) | 7 (50.0%) | 44 (46.8%) | 0.823 |
| RAASi, n (%) | 4 (28.6%) | 32 (34.0%) | 0.685 |
| Dietary intake (servings/day) | |||
| Vegetables | 1.8 (0.4–2.7) | 2.3 (1.6–3.3) | 0.059 |
| Fruits | 0.7 (0.2–1.0) | 0.7 (0.3–1.2) | 0.559 |
| Meat | 0.6 (0.0–1.3) | 0.7 (0.4–1.3) | 0.353 |
| Laboratory parameters | |||
| Kt/V | 1.6 ± 0.6 | 1.8 ± 0.3 | 0.142 |
| nPNA (g/kg/day) | 1.1 ± 0.2 | 1.2 ± 0.3 | 0.164 |
| Albumin (g/dl) | 3.8 ± 0.3 | 4.0 ± 0.4 | 0.148 |
| Fasting glucose (mg/dl) | 112 (97–147) | 109 (99–147) | 0.847 |
| Total cholesterol (mg/dl) | 135 (124–152) | 158 (143–186) | 0.012 |
| LDL (mg/dl) | 74 (63–87) | 90 (72–111) | 0.016 |
| Triglycerides (mg/dl) | 88 (58–192) | 106 (75–154) | 0.305 |
| Calcium (mmol/l) | 9.2 ± 0.8 | 9.3 ± 0.8 | 0.544 |
| Phosphorus (mg/dl) | 4.9 ± 1.5 | 5.3 ± 1.3 | 0.389 |
| iPTH (pg/ml) | 183 (25–467) | 345 (179–517) | 0.249 |
| CRP (mg/dl) | 0.30 (0.14–0.88) | 0.27 (0.15–0.62) | 0.556 |
| IL-6 (pg/ml) | 16.87 (11.57–34.59) | 7.15 (4.90–14.67) | 0.002 |
| TNF-α (pg/ml) | 7.15 (1.86–18.67) | 3.40 (1.27–6.54) | 0.040 |
BF body fat, BMI body mass index, CCB calcium channel blocker, CRP C-reactive protein, CVD cardiovascular disease, DM diabetes mellitus, FTI fat tissue index, IL-6 interleukin-6, iPTH intact parathyroid hormone, LDL low-density lipoprotein, LTI lean tissue index, nPNA normalized protein nitrogen appearance, PASE the Physical Activity Scale for the Elderly, PPI proton pump inhibitor, RAASi renin-angiotensin-aldosterone system inhibitor, SGA subjective global assessment, TNF-α tumor necrosis factor-α.
Gut microbial composition according to mortality status after matching
We then conducted a case-control study for the comparison of microbial composition according to mortality status. Fourteen nonsurvivors were matched to 56 survivors (1:4 matching) by age (±5 years) and sex according to a prespecified statistical plan (Table 4). One nonsurvivor was excluded from the analysis because there were no available matches from the survivors who satisfied the age matching criteria. The distribution of baseline characteristics before and after matching was relatively consistent among the two groups except for a higher SGA score in survivors.
Table 4.
Baseline characteristics of patients according to mortality status after matching.
| Characteristic | Dead (n = 14) | Alive (n = 56) | P Value |
|---|---|---|---|
| Age (years) | 73 ± 9 | 71 ± 9 | 0.419 |
| Male sex, n (%) | 7 (50.0%) | 28 (50.0%) | 1.000 |
| DM, n (%) | 6 (42.9%) | 32 (57.1%) | 0.337 |
| CVD, n (%) | 9 (64.3%) | 28 (50.0%) | 0.338 |
| Charlson comorbidity index | |||
| 1–2 | 0 (0.0%) | 0 (0.0%) | |
| 3–4 | 0 (0.0%) | 8 (14.3%) | 0.133 |
| ≥5 | 14 (100.0%) | 48 (85.7%) | |
| Dialysis vintage (years) | 7.0 (5.5–9.8) | 8.0 (4.0–11.3) | 0.797 |
| Dialysis access type | |||
| Arteriovenous fistula | 9 (64.3%) | 51 (91.1%) | |
| Arteriovenous graft | 4 (28.6%) | 5 (8.9%) | 0.015 |
| Central venous catheter | 1 (7.1%) | 0 (0.0%) | |
| BMI (kg/m2) | 22.4 ± 3.3 | 23.9 ± 3.5 | 0.134 |
| FTI (kg/m2) | 8.3 ± 4.5 | 9.6 ± 4.3 | 0.300 |
| LTI (kg/m2) | 13.6 ± 3.1 | 13.3 ± 3.4 | 0.813 |
| BF (%) | 26.1 ± 12.3 | 28.9 ± 10.7 | 0.405 |
| Overhydration (%) | 6.6 (−5.1–13.2) | 6.1 (−0.9–10.0) | 0.912 |
| SGA score | 5.0 (5.0–6.5) | 6.0 (6.0–7.0) | 0.032 |
| PASE score | 17 (2–73) | 54 (22–71) | 0.204 |
| Medication | |||
| PPI, n (%) | 1 (7.7%) | 4 (7.1%) | 0.945 |
| Calcium carbonate, n (%) | 9 (69.2%) | 45 (80.4%) | 0.381 |
| CCB, n (%) | 6 (46.2%) | 28 (50.0%) | 0.803 |
| β-blocker, n (%) | 7 (53.8%) | 26 (46.4%) | 0.630 |
| RAASi, n (%) | 4 (30.8%) | 21 (37.5%) | 0.649 |
| Dietary intake (servings/day) | |||
| Vegetables | 1.9 (0.3–2.7) | 2.3 (1.8–3.2) | 0.083 |
| Fruits | 0.7 (0.2–1.0) | 0.6 (0.3–1.2) | 0.497 |
| Meat | 0.6 (0.0–1.3) | 0.7 (0.4–1.2) | 0.696 |
| Laboratory parameters | |||
| Kt/V | 1.6 ± 0.6 | 1.8 ± 0.3 | 0.128 |
| nPNA (g/kg/day) | 1.1 ± 0.2 | 1.2 ± 0.3 | 0.095 |
| Albumin (g/dl) | 3.8 ± 0.3 | 4.0 ± 0.3 | 0.202 |
| Fasting glucose (mg/dl) | 115 (100–157) | 111 (101–156) | 0.877 |
| Total cholesterol (mg/dl) | 138 (122–155) | 157 (144–187) | 0.033 |
| LDL (mg/dl) | 75 (68–87) | 89 (69–111) | 0.053 |
| Triglycerides (mg/dl) | 89 (59–193) | 101 (68–153) | 0.681 |
| Calcium (mmol/l) | 9.1 ± 0.8 | 9.4 ± 0.9 | 0.354 |
| Phosphorus (mg/dl) | 4.9 ± 1.5 | 5.1 ± 1.3 | 0.503 |
| iPTH (pg/ml) | 166 (24–494) | 295 (185–577) | 0.154 |
| CRP (mg/dl) | 0.36 (0.14–1.07) | 0.26 (0.15–0.59) | 0.436 |
| IL-6 (pg/ml) | 17.50 (10.59–34.95) | 6.86 (5.06–14.76) | 0.006 |
| TNF-α (pg/ml) | 7.07 (1.71–24.07) | 2.53 (0.50–5.06) | 0.026 |
BF body fat, BMI body mass index, CCB calcium channel blocker, CRP C-reactive protein, CVD cardiovascular disease, DM diabetes mellitus, FTI fat tissue index, IL-6 interleukin-6, iPTH intact parathyroid hormone, LDL low-density lipoprotein, LTI lean tissue index, nPNA normalized protein nitrogen appearance, PASE the Physical Activity Scale for the Elderly, PPI proton pump inhibitor, RAASi renin-angiotensin-aldosterone system inhibitor, SGA subjective global assessment, TNF-α tumor necrosis factor-α.
Overall, the relative abundance of bacterial taxa at the phylum level did not reveal significant differences between the groups. The majority of the taxa (displayed as the median relative abundance) among the two groups belonged to Bacteroidetes (59.3% and 61.7% for survivors and nonsurvivors, respectively, P = 0.860), followed by Firmicutes (26.3% and 23.2% for survivors and nonsurvivors, respectively, P = 0.895) and Proteobacteria (6.9% and 7.0% for survivors and nonsurvivors, respectively, P = 1.000). In addition, the Firmicutes/Bacteroidetes ratio did not differ between the two groups (0.45 and 0.35 for survivors and nonsurvivors, respectively, P = 0.941). At the genus level, there was no significant difference in distribution according to the enterotypes between the two groups. The Bacteroides enterotype was predominant among the two groups (83.9% and 71.4% for survivors and nonsurvivors, respectively), followed by the Prevotella enterotype (16.1% and 21.4% for survivors and nonsurvivors, respectively). Mean relative abundances of all genera in survivors versus nonsurvivors are shown in Supplementary Table 2.
α-Diversity analysis revealed significant differences between groups. Nonsurvivors had significantly lower values for the Simpson index (P = 0.007) and the Shannon index (P = 0.028) (Fig. 3). The difference in microbial composition (β-diversity) between the two groups was insignificant (P = 0.482) (Supplementary Fig. 2). LEfSe analysis showed 32 discriminating taxon features between the two groups across different taxonomic levels (Fig. 4). At the genus level, Parabacteroides, Succinivibrio, and Anaerostipes were enriched in survivors. Their relative abundance with respect to mortality status is depicted in Fig. 5. In contrast, nonsurvivors demonstrated a higher expression of Oscillospira, Achromobacter, Agrobacterium, PSB_M_3, Lactobacillus, vadinCA02, Alloscardovia, Anoxybacillus, Devosia, and Yersinia.
Fig. 3. Comparison of different metrics of α-diversity between nonsurvivors and survivors after matching.

a Simpson index, b Shannon index. P values were obtained using the Mann–Whitney U test.
Fig. 4. Cladogram showing differentially abundant taxa of the gut microbiota.

a Differential taxon features at the genus level identified by LEfSe according to nonsurvivors and survivors after matching (LDA score >2). b Red and green bars represent taxon features with significantly higher expression in nonsurvivors and survivors, respectively. LDA linear discriminant analysis, LEfSe linear discriminant analysis effect size.
Fig. 5. Relative abundance of the gut microbiota at the genus level between nonsurvivors and survivors after matching.

Parabacteroides, Succinivibrio, and Anaerostipes were enriched in survivors compared with nonsurvivors. P < 0.05 using the Mann–Whitney U test.
Discussion
CKD, a growing public health concern, substantially increases the risk of mortality1,2. We observed that lower gut microbial diversity was associated with higher mortality in patients with ESKD on maintenance hemodialysis. On average, survivors demonstrated higher microbial diversity than nonsurvivors. The observed associations are consistent with the notion that diversity is an important feature of a healthy microbiota10. Moreover, our results extend beyond microbial diversity to provide evidence that a distinct gut microbial composition may have a significant role in ESKD patient outcomes. Specifically, we found that the relative abundance of Succinivibrio and Anaerostipes, two short-chain fatty acid (SCFA)-producing bacteria15,16, was markedly reduced in nonsurvivors compared with survivors, suggesting that specific taxonomic configurations of the human gut microbiota may reflect health-associated changes that are linked to increased mortality.
Changes in the normal or healthy composition of the intestinal microbiota, referred to as gut dysbiosis, could be defined as the expansion of pathogens, loss of beneficial microbes, and/or reduced microbial diversity17. Decreased gut microbial diversity has been reported in a myriad of both intestinal and extraintestinal disorders, such as inflammatory bowel disease, obesity, hypertension, DM, and CKD18–22. Our results corroborate previous findings by showing that patients with ESKD with lower diversity were more likely to have preexisting CVD and higher Charlson comorbidity index scores. Notably, although a more diverse microbial community is often considered to constitute a healthier host–microbiome relationship, recent metabolomics studies have demonstrated that certain gut-derived uremic toxins are strongly and positively correlated with intestinal microbial diversity in cohorts of healthy individuals23,24. Thus, large-scale and integrated omics studies are required to expand our understanding of the complex interactions between microbial diversity and host health in the context of CKD.
The association of lower microbial diversity with poor survival may be due, in part, to a higher risk of developing CVD and infectious complications. Gut microbial diversity has been shown to be inversely associated with blood pressure and arterial stiffness20,25. Although correlations have not been shown between coronary artery disease and heart failure with gut microbiota, recent studies have identified relevant microbial metabolic pathways consistent across several study cohorts, in particular the production of trimethylamine N-oxide, secondary bile acids, and SCFAs26. Gut dysbiosis can also be reasonably presumed to increase the risk of infection. Taur et al.27 observed that a decline in intestinal microbial diversity with domination of a single bacterial taxon predicted subsequent bloodstream infections in patients undergoing allogeneic hematopoietic stem cell transplantation. Similar findings have been described by Kato et al.28. They showed that loss of microbial diversity was associated with increasing episodes of bloodstream infections among patients undergoing liver transplantation. We observed a significant association of lower microbial diversity with CV events, but not with infection-related hospitalizations. The reasons for the discrepancy of the findings between CVD and infection may be explained by lower incidence of bloodstream infections in the present study.
Inflammation may be the mediator linking gut dysbiosis with adverse outcomes in ESKD. Chronic low-grade inflammation is a hallmark of patients with CKD, but its etiology remains obscure. Our findings of the association between lower microbial diversity and inflammation in ESKD are consistent with the results of previous studies and strongly support the notion that gut dysbiosis is involved in the development of chronic inflammation in CKD29–31. Beyond microbial diversity, we identified significant taxon differences between nonsurvivors and survivors, with a higher expression of two SCFA-producing bacteria, Succinivibrio and Anaerostipes, in the survivor group. SCFAs have been shown to have a wide range of impacts on host physiology, including anti-inflammatory effects and the maintenance of gut integrity32. The gut microbiota plays an essential role in the development of the host immune system. The immune system in return has evolved largely to maintain its symbiotic relationship with the highly diverse microbiota33. However, the disruption of this homeostasis in the presence of a uremic environment may hamper the anti-inflammatory responses by the gut microbiota.
Our study has several limitations. First, given the nature of observational studies, our results do not support causal relationships. Second, fecal samples were collected at baseline only. However, microbial diversity may decrease over time in patients with ESKD with poor survival and reach a minimum value around the time of an event. Therefore, a higher baseline microbial diversity would only bias the study results toward the null hypothesis. Third, although we excluded patients who had used antibiotics in the 3 months prior to enrollment, the long-term effect of antibiotic administration on gut microbiota could not be excluded34. Fourth, we only investigated the correlation between gut microbiota and clinical outcomes in this study. Further research will be required to determine if functional characteristics of the microbiome in CKD may be as important as or more important than the contribution of any specific taxa. Fifth, the sample size and death number of our study were relatively small, precluding further adjustment for relevant covariates in multivariate analyses and the ability to conduct subgroup analyses to investigate the effect of gut microbiota on death from different causes. Finally, the study cohort was older, with longer dialysis vintage, and with higher prevalence of diabetes and CVD than have been reported in other studies35,36. Thus, the findings may not be generalizable to the overall hemodialysis population.
In conclusion, in this study, we show that gut microbial diversity and composition are strongly correlated with all-cause mortality in ESKD patients receiving maintenance hemodialysis. Our findings also suggest that inflammation may be involved in the pathogenesis of gut dysbiosis with poor survival. Future studies with larger sample sizes and longer follow-up durations are needed to validate our observations and to investigate whether interventions for specific microbial targets may modify the outcomes for hemodialysis patients.
Methods
Study design and patient population
This was a prospective cohort study conducted in the outpatient dialysis unit of Taipei Tzu Chi Hospital, Taiwan. The study design and patients were previously described13,14. Briefly, 250 patients with ESKD undergoing hemodialysis three times weekly for at least 3 months were assessed for eligibility for inclusion from November 2017 to February 2018. Patients were excluded if they had active malignancies or liver cirrhosis or had used antibiotics in the 3 months prior to enrollment. Information on participant demographics and comorbidities was obtained from interviews and medical record reviews at the time of enrollment. DM was defined by self-reported history or use of oral antidiabetic agents or insulin. The presence of CVD was defined as coronary artery disease, as documented by coronary angiography or a history of myocardial infarction, class III or IV congestive heart failure, or a cerebrovascular accident. This study was conducted in accordance with the Declaration of Helsinki and was approved by the institutional review board of Taipei Tzu Chi Hospital (07-X01-002). All participants provided written informed consent.
Clinical data collection
Anthropometry and body composition measurements were performed 1 h after the mid-week hemodialysis session by trained nursing staff using standardized procedures. Body weight and height were measured with participants wearing indoor clothing without shoes using an autoanthropometer (Seca, Hamburg, Germany). BMI was calculated as weight in kilograms divided by height in meters squared (kg/m2). Body composition was assessed using a portable whole-body bioimpedance spectroscopy device, the body composition monitor (BCM, Fresenius Medical Care, Bad Homburg, Germany). The use of the BCM has been validated among healthy controls from the same ethnic background as the study population37. Lean tissue mass and fat tissue mass (fat mass and adipose water) based on a three-compartment model were derived from the impedance data and were expressed as the lean tissue index (lean tissue mass/height2) and fat tissue index (adipose tissue mass/height2), respectively38. Dietary data were collected using a modified short-form food frequency questionnaire39. Nutritional status was assessed with the 7-point SGA40. Both dietary and nutritional assessments were conducted by a registered dietitian. Physical activity was assessed by the PASE score, which has been validated in ESKD41.
Laboratory measurements
Blood was drawn after an 8-h fasting period, immediately before dialysis during the mid-week dialysis session. The serum albumin concentration was measured using the bromocresol green method. Plasma levels of IL-6 and TNF-α were measured using commercially available ELISA kits based on the manufacturer’s instructions (R&D Systems, Minneapolis, MN). Other laboratory measurements, including glucose, lipids, and electrolytes, were determined according to routine laboratory methods.
Outcome data collection
Mortality data including the cause of death were ascertained from official death certificates. Patients were censored at the time of transferring to other hemodialysis units, receiving kidney transplantation, or at the end of follow-up in February 2020.
Fecal sample collection
Fecal samples were obtained at home using a specimen collection kit and delivered to the laboratory (Germark Biotechnology, Taichung, Taiwan) within 24 h by refrigerated (4 °C) transportation. The samples were subsequently aliquoted, and a 200-mg subsample was immediately kept in InhibitEx buffer (Qiagen, Valencia, CA). DNA was extracted using the Qiagen DNA Mini Kit (Qiagen, Valencia, CA). The bacterial DNA concentration was measured with a NanoDrop ND-1000 (Thermo Scientific, Wilmington, DE).
16S ribosomal RNA gene sequencing and data processing
Amplification of genomic DNA was performed using bar-coded primers (341F and 805R) that targeted the V3–V4 regions of the bacterial 16S rRNA gene42. A paired-end library (insert size of 465 bp for each sample) was constructed with the TruSeq Nano DNA Library Prep kit (Illumina, San Diego, CA). Amplicons were sequenced on an Illumina MiSeq 2000 sequencer using a MiSeq Reagent Kit v3 (Illumina). To minimize batch effects, all samples were sequenced at the same time in the same research laboratory (Germark Biotechnology, Taichung, Taiwan). On a per-sample basis, paired-end reads were merged using USEARCH (v8.0.1623), setting 8 bp as the minimum overlap of read pairs43. Merged sequences were quality trimmed using Mothur (v1.35.1). Those reads that did not meet the quality criteria of a minimum quality score of 27 and sequence length shorter than 400 bp or longer than 550 bp for 16S amplicon reads were removed44. Chimeric sequences were identified and deleted by USEARCH (reference mode and 3% minimum divergence). Clustering of sequence reads into operational taxonomical units (OTUs) at 97% identity level was achieved using the UPARSE pipeline, and identified taxonomy was then aligned using the Greengenes reference database45,46.
Bioinformatic analyses
α-Diversity, a measure of the richness and evenness of taxa within each sample, was estimated by calculating the Simpson and Shannon indices with the R package phyloseq47. The Simpson and Shannon indices take into account the number of species present, as well as the relative abundance of each species, in a single indicator. β-Diversity, comparing the microbial community structures between groups, was calculated based on the Bray–Curtis distance matrices and displayed using principal coordinates analysis (PCoA) by the R package ade4, and the between-group inertia percentages were tested using the Monte-Carlo test with 1000 permutations to determine the P value of the ordination results48. Both the α-diversity and β-diversity were calculated at the OTU level without prior rarefaction49. OTU differences between groups were obtained using LEfSe, which uses the Kruskal–Wallis and Wilcoxon–Mann–Whitney tests to identify taxon features that differ in abundance between groups. Only taxa with an LDA score >2 and a significance of α < 0.05 were presented50. The results were plotted in a cladogram according to their phylogenetic relationship. The reference-based enterotype is predicted by the classifier trained from 278 MetaHIT samples51,52.
Statistical analyses
Categorical data are presented as frequencies and percentages and were compared by the chi-square test and Bonferroni post hoc test. Continuous data with or without a normal distribution are presented as the means ± standard deviations or medians and interquartile ranges and were compared by Student’s t test or the Mann–Whitney U test, respectively. Univariate correlations between the α-diversity and clinically relevant variables were assessed by Spearman’s correlation analyses. Because there is a lack of a definite cut-off value for α-diversity, we divided the patients into two groups according to the median diversity value calculated by using the Simpson index for comparing the mortality risk. The association between α-diversity and all-cause mortality was examined by using the Kaplan–Meier method and log-rank test. Cox proportional hazards modeling was applied to estimate the risk of death. The proportional hazards assumption was visually inspected by log–log survival curves. Because the event rate was relatively low, we avoided overfitting the model by selecting three clinically relevant covariates (age, sex, and Charlson comorbidity index) in adjusted models. Two-tailed P values <0.05 were considered statistically significant. All statistical analyses were carried out using the Statistical Package for the Social Sciences software, version 20.0 (SPSS Inc., Chicago, IL).
Reporting summary
Further information on experimental design is available in the Nature Research Reporting Summary linked to this article.
Supplementary information
Acknowledgements
This project was supported by grants from Research Projects MOST 105-2314-B-303-014-MY3, MOST 107-2314-B-303-021, MOST 108-2314-B-303-002-MY3, and MOST 108-2314-B-303-004-MY3, the Ministry of Science and Technology, Taiwan; and Research Projects TCRD-TPE-106-RT-5, TCRD-TPE-108-15, TCRD-TPE-108-19, TCMF-EP 108-06, and TCAS-108-02, Taipei Tzu Chi Hospital, Taiwan.
Author contributions
Research idea and study design: T.Y.L. and S.C.H.; data acquisition: T.Y.L.; data analysis/interpretation: T.Y.L., P.H.W., Y.T.L., and S.C.H.; statistical analysis: T.Y.L., P.H.W., Y.T.L., and S.C.H.; supervision or mentorship: S.C.H. Each author contributed important intellectual content during manuscript drafting or revision and accepts accountability for the overall work by ensuring that questions pertaining to the accuracy or integrity of any portion of the work are appropriately investigated and resolved.
Data availability
The datasets generated for this study can be found in NCBI with accession code PRJNA694038 (https://www.ncbi.nlm.nih.gov/bioproject/PRJNA694038).
Code availability
All code used to perform the analyses and generate the corresponding figures are publicly available at the Dryad Digital Repository (10.5061/dryad.k3j9kd55d).
Competing interests
The authors declare no competing interests.
Footnotes
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
The online version contains supplementary material available at 10.1038/s41522-021-00191-x.
References
- 1.United States Renal Data System. 2019 USRDS annual data report: epidemiology of kidney disease in the United States. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD (2019).
- 2.de Jager DJ, et al. Cardiovascular and noncardiovascular mortality among patients starting dialysis. JAMA. 2009;302:1782–1789. doi: 10.1001/jama.2009.1488. [DOI] [PubMed] [Google Scholar]
- 3.Nordio M, et al. Italian Dialysis and Transplantation Registry. Survival in patients treated by long-term dialysis compared with the general population. Am. J. Kidney Dis. 2012;59:819–828. doi: 10.1053/j.ajkd.2011.12.023. [DOI] [PubMed] [Google Scholar]
- 4.Lukowsky LR, Kheifets L, Arah OA, Nissenson AR, Kalantar-Zadeh K. Nutritional predictors of early mortality in incident hemodialysis patients. Int. Urol. Nephrol. 2014;46:129–140. doi: 10.1007/s11255-013-0459-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Barreto DV, et al. Plasma interleukin-6 is independently associated with mortality in both hemodialysis and pre-dialysis patients with chronic kidney disease. Kidney Int. 2010;77:550–556. doi: 10.1038/ki.2009.503. [DOI] [PubMed] [Google Scholar]
- 6.Liabeuf S, Cheddani L, Massy ZA. Uremic toxins and clinical outcomes: the impact of kidney transplantation. Toxins. 2018;10:E229. doi: 10.3390/toxins10060229. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ley RE, Peterson DA, Gordon JI. Ecological and evolutionary forces shaping microbial diversity in the human intestine. Cell. 2006;124:837–848. doi: 10.1016/j.cell.2006.02.017. [DOI] [PubMed] [Google Scholar]
- 8.Vaziri ND, et al. Chronic kidney disease alters intestinal microbial flora. Kidney Int. 2013;83:308–315. doi: 10.1038/ki.2012.345. [DOI] [PubMed] [Google Scholar]
- 9.Hung SC, Kuo KL, Wu CC, Tarng DC. Indoxyl sulfate: a novel cardiovascular risk factor in chronic kidney disease. J. Am. Heart Assoc. 2017;6:e005022. doi: 10.1161/JAHA.116.005022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Lloyd-Price J, Abu-Ali G, Huttenhower C. The healthy human microbiome. Genome Med. 2016;8:51. doi: 10.1186/s13073-016-0307-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Peled JU, et al. Microbiota as predictor of mortality in allogeneic hematopoietic-cell transplantation. N. Engl. J. Med. 2020;382:822–834. doi: 10.1056/NEJMoa1900623. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Leitao Filho FS, et al. Sputum microbiome is associated with 1-year mortality after chronic obstructive pulmonary disease hospitalizations. Am. J. Respir. Crit. Care. Med. 2019;199:1205–1213. doi: 10.1164/rccm.201806-1135OC. [DOI] [PubMed] [Google Scholar]
- 13.Lin, T. Y. & Hung, S. C. Association of subjective global assessment of nutritional status with gut microbiota in hemodialysis patients: a case–control study. Nephrol. Dial. Transplant. gfaa019, 10.1093/ndt/gfaa019 (2020). [DOI] [PubMed]
- 14.Lin TY, Wu PH, Lin YT, Hung SC. Characterization of gut microbiota composition in hemodialysis patients with normal weight obesity. J. Clin. Endocrinol. Metab. 2020;105:dgaa166. doi: 10.1210/clinem/dgaa166. [DOI] [PubMed] [Google Scholar]
- 15.Ticinesi A, et al. Aging gut microbiota at the cross-road between nutrition, physical frailty, and sarcopenia: Is there a gut-muscle axis? Nutrients. 2017;9:E1303. doi: 10.3390/nu9121303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Louis P, Flint HJ. Diversity, metabolism and microbial ecology of butyrate-producing bacteria from the human large intestine. FEMS Microbiol. Lett. 2009;294:1–8. doi: 10.1111/j.1574-6968.2009.01514.x. [DOI] [PubMed] [Google Scholar]
- 17.Petersen C, Round JL. Defining dysbiosis and its influence on host immunity and disease. Cell Microbiol. 2014;16:1024–1033. doi: 10.1111/cmi.12308. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Turnbaugh PJ, et al. A core gut microbiome in obese and lean twins. Nature. 2009;457:480–484. doi: 10.1038/nature07540. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Manichanh C, et al. Reduced diversity of faecal microbiota in Crohn’s disease revealed by a metagenomic approach. Gut. 2006;55:205–211. doi: 10.1136/gut.2005.073817. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Sun S, et al. Gut microbiota composition and blood pressure. Hypertension. 2019;73:998–1006. doi: 10.1161/HYPERTENSIONAHA.118.12109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Qin J, et al. A metagenome-wide association study of gut microbiota in type 2 diabetes. Nature. 2012;490:55–60. doi: 10.1038/nature11450. [DOI] [PubMed] [Google Scholar]
- 22.Wilkins LJ, Monga M, Miller AW. Defining dysbiosis for a cluster of chronic diseases. Sci. Rep. 2019;9:12918. doi: 10.1038/s41598-019-49452-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Pallister T, et al. Hippurate as a metabolomics marker of gut microbiome diversity: Modulation by diet and relationship to metabolic syndrome. Sci. Rep. 2017;7:13670. doi: 10.1038/s41598-017-13722-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Wilmanski T, et al. Blood metabolome predicts gut microbiome α-diversity in humans. Nat. Biotechnol. 2019;37:1217–1228. doi: 10.1038/s41587-019-0233-9. [DOI] [PubMed] [Google Scholar]
- 25.Menni C, et al. Gut microbial diversity is associated with lower arterial stiffness in women. Eur. Heart J. 2018;39:2390–2397. doi: 10.1093/eurheartj/ehy226. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Trøseid M, Andersen GØ, Broch K, Hov JR. The gut microbiome in coronary artery disease and heart failure: Current knowledge and future directions. EBioMedicine. 2020;52:102649. doi: 10.1016/j.ebiom.2020.102649. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Taur Y, et al. Intestinal domination and the risk of bacteremia in patients undergoing allogeneic hematopoietic stem cell transplantation. Clin. Infect. Dis. 2012;55:905–914. doi: 10.1093/cid/cis580. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Kato K, et al. Longitudinal analysis of the intestinal microbiota in liver transplantation. Transplant. Direct. 2017;3:e144. doi: 10.1097/TXD.0000000000000661. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Meslier, V. et al. Mediterranean diet intervention in overweight and obese subjects lowers plasma cholesterol and causes changes in the gut microbiome and metabolome independently of energy intake. Gut69, 1258–1268 (2020). [DOI] [PMC free article] [PubMed]
- 30.Ott SJ, Schreiber S. Reduced microbial diversity in inflammatory bowel diseases. Gut. 2006;55:1207. [PMC free article] [PubMed] [Google Scholar]
- 31.Annavajhala MK, et al. Oral and gut microbial diversity and immune regulation in patients with HIV on antiretroviral therapy. mSphere. 2020;5:e00798–19. doi: 10.1128/mSphere.00798-19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Tan J, et al. The role of short-chain fatty acids in health and disease. Adv. Immunol. 2014;121:91–119. doi: 10.1016/B978-0-12-800100-4.00003-9. [DOI] [PubMed] [Google Scholar]
- 33.Belkaid Y, Hand TW. Role of the microbiota in immunity and inflammation. Cell. 2014;157:121–141. doi: 10.1016/j.cell.2014.03.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Rashid MU, et al. Determining the long-term effect of antibiotic administration on the human normal intestinal microbiota using culture and pyrosequencing methods. Clin. Infect. Dis. 2015;60:S77–S84. doi: 10.1093/cid/civ137. [DOI] [PubMed] [Google Scholar]
- 35.Marcelli D, et al. Body composition and survival in dialysis patients: results from an international cohort study. Clin. J. Am. Soc. Nephrol. 2015;10:1192–1200. doi: 10.2215/CJN.08550814. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Li P, et al. Plasma endothelin-1 and risk of death and hospitalization in patients undergoing maintenance hemodialysis. Clin. J. Am. Soc. Nephrol. 2020;15:784–793. doi: 10.2215/CJN.11130919. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Hung SC, et al. Volume overload correlates with cardiovascular risk factors in patients with chronic kidney disease. Kidney Int. 2014;85:703–709. doi: 10.1038/ki.2013.336. [DOI] [PubMed] [Google Scholar]
- 38.Chamney PW, et al. A whole-body model to distinguish excess fluid from the hydration of major body tissues. Am. J. Clin. Nutr. 2007;85:80–89. doi: 10.1093/ajcn/85.1.80. [DOI] [PubMed] [Google Scholar]
- 39.Huang YC, Lee MS, Pan WH, Wahlqvist ML. Validation of a simplified food frequency questionnaire as used in the Nutrition and Health Survey in Taiwan (NAHSIT) for the elderly. Asia Pac. J. Clin. Nutr. 2011;20:134–140. [PubMed] [Google Scholar]
- 40.de Mutsert R, et al. Netherlands Cooperative Study on the Adequacy of Dialysis-2 Study Group. Subjective global assessment of nutritional status is strongly associated with mortality in chronic dialysis patients. Am. J. Clin. Nutr. 2009;89:787–793. doi: 10.3945/ajcn.2008.26970. [DOI] [PubMed] [Google Scholar]
- 41.Johansen KL, et al. Validation of questionnaires to estimate physical activity and functioning in end-stage renal disease. Kidney Int. 2001;59:1121–1127. doi: 10.1046/j.1523-1755.2001.0590031121.x. [DOI] [PubMed] [Google Scholar]
- 42.Herlemann DP, et al. Transitions in bacterial communities along the 2000 km salinity gradient of the Baltic Sea. ISME J. 2011;5:1571–1579. doi: 10.1038/ismej.2011.41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Edgar RC. Search and clustering orders of magnitude faster than BLAST. Bioinformatics. 2010;26:2460–2461. doi: 10.1093/bioinformatics/btq461. [DOI] [PubMed] [Google Scholar]
- 44.Schloss PD, et al. Introducing mothur: open-source, platform-independent, community-supported software for describing and comparing microbial communities. Appl. Environ. Microbiol. 2009;75:7537–7541. doi: 10.1128/AEM.01541-09. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Edgar RC. UPARSE: highly accurate OTU sequences from microbial amplicon reads. Nat. Methods. 2013;10:996–998. doi: 10.1038/nmeth.2604. [DOI] [PubMed] [Google Scholar]
- 46.Quast C, et al. The SILVA ribosomal RNA gene database project: improved data processing and web-based tools. Nucleic Acids Res. 2013;41:D590–D596. doi: 10.1093/nar/gks1219. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.McMurdie PJ, Holmes S. phyloseq: an R package for reproducible interactive analysis and graphics of microbiome census data. PLoS ONE. 2013;8:e61217. doi: 10.1371/journal.pone.0061217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Dray S, Dufour AB. The ade4 package: Implementing the duality diagram for ecologists. J. Stat. Softw. 2007;22:1–20. doi: 10.18637/jss.v022.i04. [DOI] [Google Scholar]
- 49.McMurdie PJ, Holmes S. Waste not, want not: why rarefying microbiome data is inadmissible. PLOS Comput. Biol. 2014;10:e1003531. doi: 10.1371/journal.pcbi.1003531. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Segata N, et al. Metagenomic biomarker discovery and explanation. Genome Biol. 2011;12:R60. doi: 10.1186/gb-2011-12-6-r60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Le Chatelier E, et al. Richness of human gut microbiome correlates with metabolic markers. Nature. 2013;500:541–546. doi: 10.1038/nature12506. [DOI] [PubMed] [Google Scholar]
- 52.Costea PI, et al. Enterotypes in the landscape of gut microbial community composition. Nat. Microbiol. 2018;3:8–16. doi: 10.1038/s41564-017-0072-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The datasets generated for this study can be found in NCBI with accession code PRJNA694038 (https://www.ncbi.nlm.nih.gov/bioproject/PRJNA694038).
All code used to perform the analyses and generate the corresponding figures are publicly available at the Dryad Digital Repository (10.5061/dryad.k3j9kd55d).