

Abstract
The fetal circulatory system bypasses the lungs and liver with three shunts. The foramen ovale allows the transfer of the blood from the right to the left atrium, and the ductus arteriosus permits the transfer of the blood from the pulmonary artery to the aorta. The ductus venosus is the continuation of the umbilical vein, allowing a large part of the oxygenated blood from the placenta to join the supradiaphragmatic inferior vena cava, bypassing the fetal liver and directly connecting the right atrium. These structures are named after the physicians who are thought to have discovered them. The foramen ovale and the ductus arteriosus are called the “foramen Botalli” and the “ductus Botalli,” after Leonardo Botallo (1530–c. 1587). The ductus venosus is styled “ductus Arantii” after Giulio Cesare Arantius (1530–1589). However, these eponyms have been incorrectly applied as these structures were, in fact, discovered by others earlier. Indeed, the foramen ovale and the ductus arteriosus were described by Galen of Pergamon centuries earlier (c. 129–210 AD). He understood that these structures were peculiar to the fetal heart and that they undergo closure after birth. The ductus venosus was first described by Andreas Vesalius (1514–1564) 3 years before Arantius. Therefore, the current anatomical nomenclature of the fetal cardiac shunts is historically inappropriate.
Keywords: Andreas Vesalius, ductus arteriosus Botalli, ductus venosus Arantii, foramen botalli, Gabriele Falloppio, Galen of Pergamon, Giovanni Battista Carcano Leone, Giulio Cesare Arantius, Leonardo Botallo
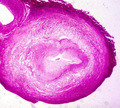
Spontaneous closure of ductus arteriosus, becoming ligamentum arteriosum. Histological cross‐section of the closing ductus arteriosus in a male new‐born, 15 days old, with pulmonary atresia, ventricular septal defect, and ductus‐dependent pulmonary blood supply. Note: The almost occluded ductal lumen by intimal proliferation. Weigert‐Van Gieson stain original magnification ×5.
1. THE THREE CARDIAC SHUNTS
It is well‐known that the fetal lungs and liver are not fully functional during pregnancy and that these organs are bypassed by three shunts (Figure 1). The foramen ovale allows the venous blood to flow from the right atrium to the left atrium and thereby to the systemic circulation. The ductus arteriosus diverts the blood from the pulmonary artery to the aorta, whereas the ductus venosus connects the umbilical vein to the inferior vena cava bypassing the portal vein and the liver. These shunts close shortly after birth when the newborn begins to breathe and the lungs are perfused. At this point, the muscular and endothelial components of the ductus arteriosus degenerate and undergo proliferation, apoptosis, and fibrous repair obstruction (Figure 2). The ductus venosus persists a little longer but becomes non‐functional once the umbilical cord is severed. The ductus venosus closes during the first week of infancy and becomes the ligamentum venosum. When, in the new‐born, the blood returns to the left atrium the foramen ovale closes somewhat like a door from left to right. It can take weeks for definitive closure and in approximately 30% of the population this does not occur, giving rise to foramen ovale patency (Figure 3).
FIGURE 1.
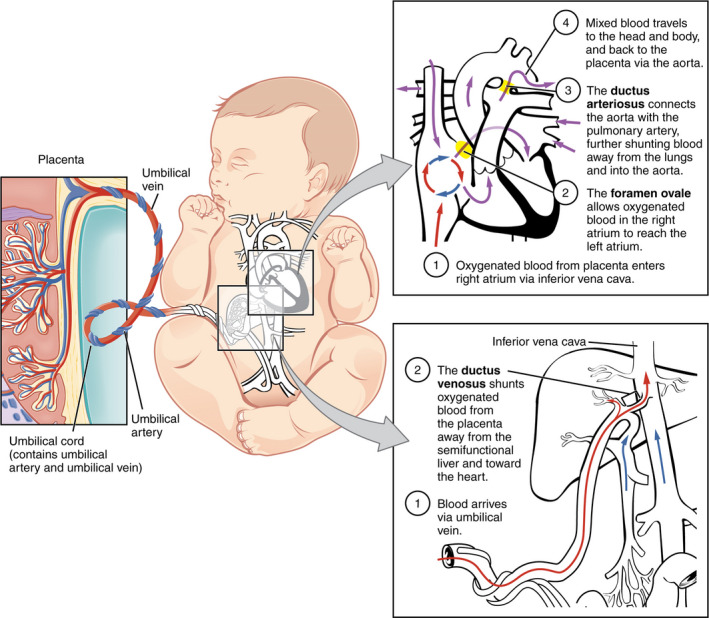
The fetal circulatory system includes three shunts to divert blood from undeveloped and partially functioning organs, as well as blood supply to and from the placenta (Source: Anatomy & Physiology, Connexions Web site. http://cnx.org/content/col11496/1.6/, June 19, 2013. Author: OpenStax College)
FIGURE 2.

Spontaneous closure of ductus arteriosus, becoming ligamentum arteriosum. Histological cross‐section of the closing ductus arteriosus in a male new‐born, 15 days old, with pulmonary atresia, ventricular septal defect, and ductus‐dependent pulmonary blood supply. Note: The almost occluded ductal lumen by intimal proliferation. Weigert‐Van Gieson stain original magnification ×5
FIGURE 3.
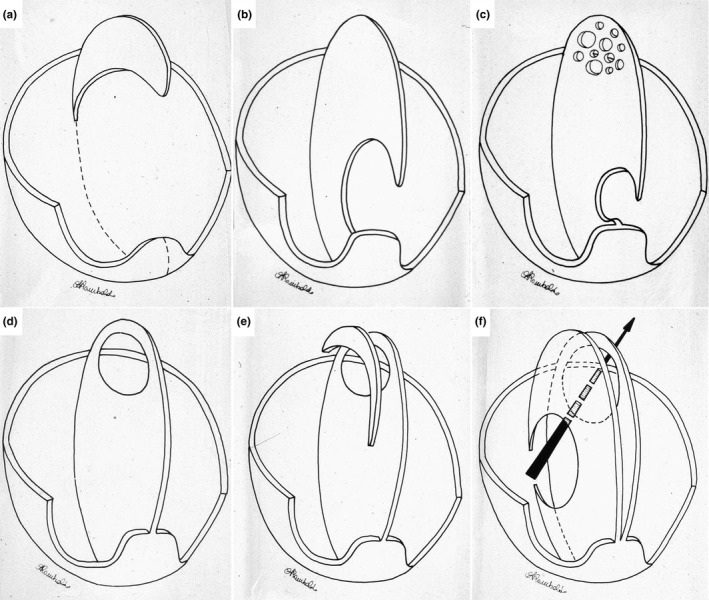
Formation of the atrial septum during development. (a) Appearance of the septum primum. (b) Expansion of the septum primum to leave the ostium primum as a communication between the right and left atrium. (c) Starting of the ostium secundum by spotty apoptosis. (d) Definitive closure of the ostium primum, which leaves the ostium secundum as the only communication between the two atria. (e) Appearance of the septum secundum. (f) Complete covering of the ostium secundum by the septum secundum leaving patency from right to left (foramen ovale). Image from: Thiene G. and Frescura C. Cardiopatie congenite in Calì A. and Fiore‐Donati L. (Eds.) Anatomia Patologica generale e applicata. Uses; 1988; 1: 799
These structures are termed after the physicians who are traditionally considered their discoverers. The foramen ovale is called “foramen Botalli” and the ductus arteriosus is named “ductus Botalli,” after the Italian Renaissance physician Leonardo Botallo (1530–c. 1587). The ductus venosus is named “ductus Arantii” after the Italian anatomist Giulio Cesare Arantius (1530–1589). However, these eponyms are inappropriate because other physicians had previously described these structures. We wonder whether the current anatomical nomenclature of the fetal cardiac shunts should be revised. In the medical historical literature, there are some contributions that have already highlighted that these cardiac shunts have inappropriate eponyms (Franklin, 1941; Fransson, 1999; Tozzo et al., 2020). However, the present paper is the first to cover the entire history of these eponyms. In particular, the classic and Renaissance sources are integrally quoted, thus demonstrating in detail to whom should be attributed the discovery of each of the three cardiac shunts.
2. FORAMEN OVALE
Leonardo Botallo was an Italian physician who spent most of his life at the French court (Tozzo et al., 2020). As mentioned, he is credited for having discovered the foramen ovale and the ductus arteriosus. However, Botallo observed the foramen ovale in the adult and not fetal heart, and he did not mention the ductus arteriosus in his original works (Tozzo et al., 2020).
Botallo described the foramen ovale in an adult in a brief note entitled Vena arteriarum nutrix,a nullo antea notata published in 1564, at the end of his work De catarrho (Botallo, 1564). This note was republished twice, in 1640 and in 1641, under the title De Via sanguinis a dextro in sinistrum cordis ventriculum Leonardi Bottalli,sententia promulgata Parisiis anno salutis 1564, edited by Cecilius Folius (1615–1650) (Folius, 1639). Folius was a Venetian physician who, some years before, found a patent foramen ovale (PFO) in an adult cadaver. He immediately reached the conclusion that it was a normal structure and that the blood passed in all cases through the route he had observed (Folius, 1639; Kasten, 1954). This was exactly the same opinion that Botallo advanced in 1564. Finally, the Leiden anatomist Johann Van Horne (1621–1670) edited Botallo's Opera omnia in 1660 (Botallo, 1660). Here, under a section entitled “Anatomical observations,” Van Horne reported the note published by Botallo at the end of De catharro.
At the time of Botallo, pulmonary circulation was still not fully understood. Galen of Pergamon (c. 129–210 AD) postulated that the passage of blood from the right to the left part of the heart was through “invisible pores” in the interventricular septum and the existence of these pores remained a sort of dogma for centuries. In 1559, Matteo Realdo Colombo (1516–1559), professor of anatomy in Padua, Pisa, and Rome, first demonstrated that the passage of blood from the right ventricle to the left was carried out through the lungs, rejecting Galenic dogma and establishing the new pathway of the so‐called “small circulation” (Colombo, 1559; Elmaghawry et al., 2014). Colombo experimentally demonstrated this new model also by the vivisection of dogs: “I believe that the venous artery [pulmonary vein] has been made to carry blood mixed with air in the lungs to the left ventricle of the heart.This matter is true,very true:indeed,you will find this artery always full of blood,both by dissecting cadavers and vivisecting animals” (Colombo, 1559). Before Colombo, the Arab physician Ibn al‐Nafis (1213–1288) and the Spanish theologian Michael Servetus (1511–1553) had already advanced the hypothesis of a pulmonary blood transit from the right to the left atrium in 1242 and 1553, respectively. Some medical history scholars have advanced that, on the examination of the manuscripts from Servetus, Vesalius, and Colombo, they seemed to contain verbatim translations of the quoted passage from Ibn al‐Nafis’ commentary (Loukas et al., 2008). As far as Servetus, the description of pulmonary circulation was published inside a theological treatise, namely the Christianismi restitutio, which was considered heretical by both Catholics and Calvinists. Servetus and his books were burned at the stake in Geneva in 1553 and therefore his discovery was not divulged. In any case, Servetus did not describe the modern pulmonary circuit as the new text implied (Izquierdo, 1937). Colombo was the first to demonstrate, by in vivo dissection of the pulmonary veins in dog, that blood and not air was coming out (Ongaro, 1971).
However, Colombo's discovery was not immediately accepted by the medical community since many still believed in Galen's dogma, while others advanced alternative views.
Botallo observed a PFO in an adult cadaver and believed he had found the real pathway of blood from the right to the left part of the heart. He based his assumption on both adult animal and human dissections. Indeed, while dissecting a calf heart, he had found a fairly large foramen, which he called “ductus” or “channel,” leading directly into the left auricle, just above the coronary vein. Then, he found the same structure in other animals, as well as in man: “I began to dissect the heart of a calf,in which I discovered […] a channel […] near the right auricle […] that leads directly […] to the left auricle.[…] This pathway which I discovered is quite large and clearly visible in calves,pigs and dogs.In man instead it is a bit smaller” (Botallo, 1564). It is important to underline that fetal communication between the right and left atrium may appear as a channel or ductus in ungulates such as cow and pig, whereas in rodents and primates it appears as a foramen. Botallo considered this “ductus,” therefore, to be the nutrient vessel of the arteries and the “vital spirits.” It was believed, that the arterial blood contained also this kind of “air” (called pneuma) responsible for several physiological or psychic functions.
Botallo observed the persistence of this hole which might occur in adult mammals, representing a disorder that could have severe consequences. This condition is now called PFO (Figure 4) and it is present in 20–25% of the population (Hara et al., 2005), although its persistence and the mechanism which accounts for it are not entirely clear (Schneider, 2012).
FIGURE 4.
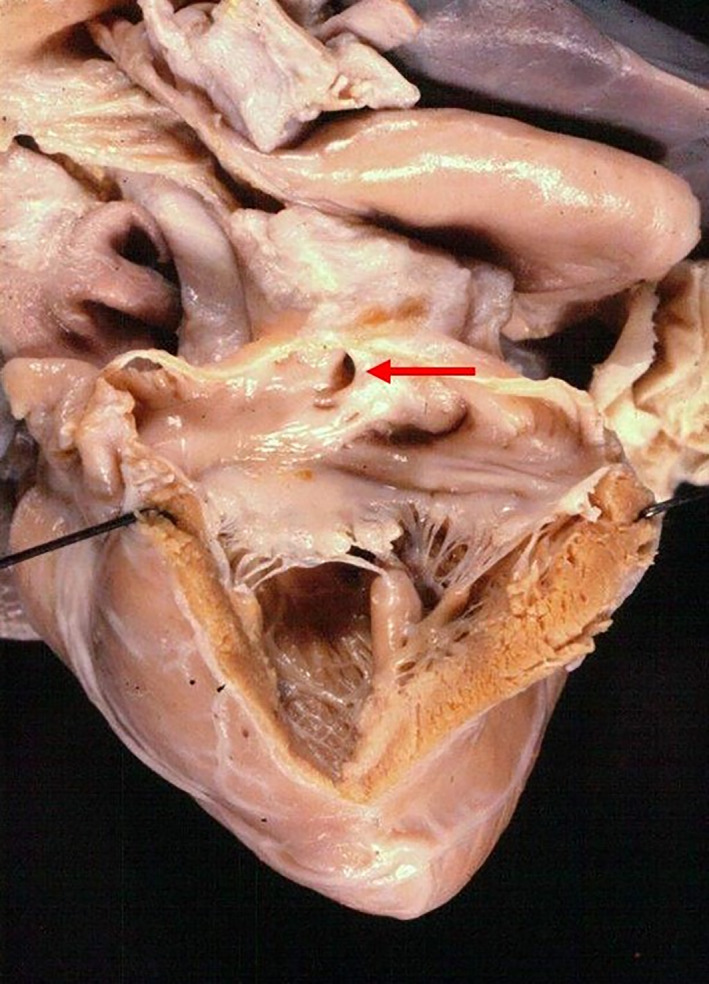
The patent foramen ovale in a heart specimen seen from the left atrium (red arrow)
One of the first descriptions of PFO, with a remarkable interpretation of its pathophysiology, can be found in the Giovanni Battista Morgagni (1682–1771) De sedibus et causis morborum per anatomen indagatis (Morgagni, 1761), where Morgagni reported the clinical history of a “girl,who was sick since birth and died at the age of 16.” At autopsy, Morgagni found that “the heart was small […] the right ventricle had the shape of the left one […] the foramen ovale was patent […] the sigmoid pulmonary valves were cartilaginous with a small orifice.” He understood that the PFO was present at birth and that “the livid skin was due to blood stagnation and to the existence of foramen ovale,the valve of which was pushed from right to left” (Morgagni, 1761; Zampieri et al., 2016). Thus, for the first time in medical literature, Morgagni was describing a case of pulmonary valve stenosis with atrial septal defect. He surmised that the valve defect was present at birth and that the cyanosis of the girl was due to right to left shunt at the level of foramen ovale which remained patent.
Therefore, in anatomical nomenclature the term “foramen Botalli” should be used for designating the PFO (even if Botallo did not understand that it was persistence of fetal shunt), while the fetal foramen ovale should be named “foramen Galeni,” given that Galen of Pergamon described it for the first time in the fetus (Franklin, 1941). In his De usu partium (On the usefulness of parts), Galen described both the foramen ovale and the ductus arteriosus, even if the passages are difficult to interpret. However, he understood that these structures were peculiar to the fetal heart, because in the fetus there was no respiration through the lungs, and that they closed after birth (Tallmadge, 1968). He stated that “[The nature] opens the great artery [i.e.aorta] in the thick and solid vessels of the lungs [i.e.the pulmonary arteries] and it opens the vena cava in the thin and lax vessels of the lungs [i.e.pulmonary veins].” The first part of this sentence seems clear to refer to the ductus arteriosus whereas the second part is more difficult to interpret. However, a few lines after Galen stated that “The adult heart can draw from the lungs the blood mixed with air through that opening which has only two valves [i.e.,the bicuspid mitral valve between the left atrium and the left ventricle] and which leads into the left chamber of the heart.But in the foetus,this chamber actually receives the blood from the vena cava through a certain anastomosis which is of a remarkable size” (Singer, 1968). That this anastomosis was described as of “remarkable size” confirms that he was observing the foramen ovale. Finally, he was perfectly aware that these “anastomoses” close after birth: “Nature,as dries out during time the vein connecting the navel with the liver […] transforming it in a structure similar to a cord,in the same way it changes in the new‐born the anastomoses of cardiac vessels.” The first part of this quotation seems to indicate that Galen observed also the ductus venosus, being aware that it closed after birth. However, this is the only passage in Galen's extant works where this structure seems to be mentioned. Moreover, the passage is too short and not clear enough to be considered as the first real description of the ductus venosus. The ductus arteriosus and the foramen ovale were, instead, clearly described by Galen, so that their discovery deserves to be ascribed to him.
Of course, Galen was observing these structures in apes, not in humans, but he attributed them to man, which are, in this case, identical to the apes’. Moreover, it is remarkable that he perfectly understood that fetal shunts closed after birth, a knowledge which would be rediscovered only by Renaissance anatomists.
3. DUCTUS ARTERIOSUS
Regarding the ductus arteriosus, also the eponym “ductus Botalli” is wrong because Botallo never described this structure either in fetal or in adult hearts. In Botallo's De catarrho there is no mention of the ductus arteriosus, nor in 1640, 1641 or 1660 re‐editions of Botallo's De via sanguinis. The incorrect attribution most probably originated from a misunderstanding of Van Horne's edition of Botallo's Opera Omnia. Van Horne inserted a plate where there was depicted both the “foramen ovale” and the “ductus arteriosus” (called “canalis à pulmonali arteria tendens in aortam”). In the footnote, Van Horne referred, probably ironically, to Botallo's claim: “Immediately he exclaimed with Archimedes eureka,but celebrated the triumph before the victory” (Botallo, 1660; Franklin, 1941; Obladen, 2011). Later authors, without grasping the irony of this footnote, wrongly attributed the figure in Van Horne edition to Botallo himself, who thus became famous and inadvertently made his way into the nomina anatomica at the Basel conference in 1895 (Kopsch & Knese, 1957).
Therefore, this anatomical eponym should be corrected. As already shown, in fact, Galen first described the ductus arteriosus, but before him, also Aristotle (384/383‐322 BC) seems to have described this structure. Aristotle believed that the human heart was composed of three, rather than four, chambers. Most probably, he did not recognize the right atrium, seeing it as a dilatation of the vena cava (Shaw, 1972; Van Praagh & Van Praagh, 1983). In his Historia animalium (History of Animals), Aristotle mentioned three principal connections between heart and lungs, each one from the three heart chambers. He stated that: “All of them,even the two small ones,have a connection with the lungs,and this is quite clearly visible in respect of one of them” (Shaw, 1972).
It is possible that he was describing the pulmonary arteries as connecting the right ventricle to the lungs and the pulmonary veins as connecting the left atrium to the lungs, while the structure connecting the left ventricle to the lungs could be a still pervious ductus arteriosus, because there is no other possible “vessel” that could be observed. This interpretation is based on the hypothesis that Aristotle could have dissected some human fetuses, because in other parts of his anatomical treatises he described features typical of the fetal body, ascribing them to the adult one, such as the lobulated kidneys (Shaw, 1972). At that time, the dissection of cadavers of human adult was taboo whereas fetuses might have been more accessible to anatomical investigation. However, Aristotle's possible observation of the ductus arteriosus is too imprecise to deserve full historical priority. Moreover, he did not return back to this observation in any other of his works.
During Botallo's time, Galen's description was confirmed by Gabriele Falloppio (1523–1562), professor of Anatomy at the University of Padua. Falloppio, born in Modena, studied medicine at Padua and Ferrara universities. He was appointed as professor of botany at the University of Ferrara (1547), then of Anatomy at the University of Pisa (1548), and finally as professor of Anatomy, Surgery, and Botany at the University of Padua in 1551, where he remained until his death. At that time, he was probably the most important anatomist internationally and the medical school of the University of Padua had a great reputation in anatomical studies. In 1561, he published his Observationes anatomicae, in which the ductus arteriosus is mentioned for the first time since Galen, though he added almost no new information compared to Galen's original description (Falloppio, 1561) noting only that the vessel was of large calibre (Franklin, 1941). Falloppio declared that he was surprised that no other anatomist other than Galen had observed this “ductus” and, in particular, criticized Andreas Vesalius (1514–1564), his predecessor at the chair of Anatomy in Padua, for having omitted to note this “large ductus” which was easily observed connecting the right ventricle to the aorta in fetuses and became “dry” after birth (Falloppio, 1561).
4. DUCTUS VENOSUS
A few years after the publication of Falloppio, another Italian anatomist, Giulio Cesare Arantius (1530–1589), described in greater detail both the foramen ovale and the ductus arteriosus in his De humano fetus libellus of 1564 (Arantius, 1564). Arantius, who graduated in medicine at Bologna University, Italy, was one of the distinguished anatomists of his generation. He also studied at the University of Padua and then became Lecturer in Medicine and Surgery at the University of Bologna in 1557. In 1570, he was able to separate the two fields, surgery and anatomy, so that each would have its own Chair. He was the first lecturer at the University of Bologna to hold a separate Chair of Anatomy and held both positions until his death in 1589 (Gurunluoglu et al., 2011). It is important to note that, 10 years after the publication of Arantius, Giovanni Battista Carcano Leone (1536–1606), a pupil of Falloppio in Padua and then professor of Anatomy at Pavia University, published the Anatomici libri duo. In the first part, entitled De cordis vasorum in foetu unione, he described both the foramen ovale and the ductus arteriosus with more accuracy than Falloppio or Arantius (Scarpa, 1813). In particular, Carcano corrected Falloppio, who stated that the ductus arteriosus was placed just above the base of the heart, while the real seat is placed further above the heart, and more precisely “in the curvature of the aorta,where it reclines on the left side of dorsal vertebrae” (Carcano Leone, 1574). Then, he corrected Arantius, who believed that both the foramen ovale and ductus arteriosus were provided with “semilunar valves.” He stated instead that: “By opening the arteriosus canal [ductus arteriosus] all along its length,no valvular apparatus might be noted,neither in the aorta side,nor in the side of the pulmonary artery” (Carcano Leone, 1574). After the publication of Carcano, Arantius published a second edition of his work, in which he corrected his description according to Carcano's notes (Scarpa, 1813).
However, in Arantius’ De humano fetus libellu there was an additional achievement, missing in Galen, Falloppio, and Carcano, namely the account of the ductus venosus. This publication, therefore, described all the three fetal cardiac conduits. Because of this, the ductus venosus is also called “ductus Arantii.” In Chapter XIV, on “The connection between the vessels of heart and liver,” Arantius declared that regarding the connection between vena cava—which was considered as the right atrium—and the left chamber of the heart (foramen ovale), and about the connection between the pulmonary artery and aorta (ductus arteriosus), nothing could be added to what Galen had already described. However, Arantius added another observation “worthy to be mentioned,” namely a connection between the umbilical vein and the vena cava, which existed in the fetus and dried‐out after birth (Arantius, 1564).
Albrecht von Haller (1708–1777) in his Elementa physiologiae corporis humani (1764–1766) was the first to attribute the discovery of ductus venosus to Arantius and after him, the eponym “ductus venosus Arantii” became popular in the German literature (Franklin, 1941) and in the clinical setting. Subsequently. this eponym was included in the 1895 Basel Anatomical Nomenclature (His, 1895), and finally in the International Anatomical Terminology of 1989 (Kachlík et al., 2008) which is the subtitle of the 1989 edition of the Terminologia Anatomica, generated by the International Anatomical Nomenclature Committee of the International Federation of Associations of Anatomists.
However, this structure should not be named “ductus Arantii” because it was already described in 1561, even if only published in 1564, by Andreas Vesalius in his Anatomicarum Gabrielis Falloppii Observationum Examen (Vesalius, 1564). In this book, Vesalius replied to Falloppio's criticisms found in the Observationem anatomicae, where Falloppio blamed Vesalius, “prince of anatomists,” for having omitted the observation of the ductus arteriosus (Vesalius, 1564). Vesalius first answered Falloppio by admitting that he was not fully convinced of the existence of ductus arteriosus by his observations on the human fetus. At the same time, he was able to take a step further, by describing a structure noted neither by Galen nor by Falloppio, namely, the ductus venosus; he observed that the umbilical vein joined the portal vein. From the posterior portion of this trunk, a branch passed up to enter the vena cava on its anterior aspect (Franklin, 1941; Vesalius, 1564). Therefore, given that Vesalius described the ductus venosus 3 years before Arantius, even if the publication is of the same year as Arantius’ (1564), also this eponym should be changed, and styled as “ductus venosus Vesalii.”
The British physician William Harvey (1578–1657), who graduated in Padua in 1602, discovered and described systemic blood circulation in his famous Exercitatio anatomica de motu cordis et sanguinis in animalibus of 1628 (Harvey, 1628). In Chapter VI he also described the fetal circulation, the foramen ovale, and the ductus arteriosus. First, he stated that: “[…] in the embryo,while the lungs are idle and devoid of activity or movement,as though they did not exist,Nature uses the two ventricles of the heart as one for the transmission of the blood.And the condition of the embryo that has lungs,but is not as yet making use of them,is similar to that of the animals that has no lungs at all” (Harvey, 1628). The foramen ovale is described as follows: “[…] in the embryo the blood must continuously be passing through this opening (oval in shape) from the vena cava into the vein‐like artery,and thence into the left auricle of the heart.On the other hand,once it has so entered,it can never flow back again” (Harvey, 1628). The ductus arteriosus was “The other union […] of the artery‐like vein (which occurs after that vein has left the right ventricle and is dividing into two branches).It is a sort of third trunk added to these two,an artery‐like channel […] leading obliquely from this point to the great artery and perforating into it.Hence,in the dissection of embryos there appear […] to be two aortae […] arising from the heart.[…] Hence […] in the embryo there is a continuous transference of blood by this route from the right ventricle to the great artery,during contraction of the heart” (Harvey, 1628). Interestingly, Harvey mentioned also Botallo, noting that he wrongly believed he had have found a “new passage of the blood from vena cava to the left ventricle of the heart” (Harvey, 1628). Oddly enough, he did not mention the ductus venosus, probably because he was not interested in this structure, given that his focus was on the circulatory movements of blood.
5. CONCLUSIONS
The historical eponyms of the three fetal conduits are not named according to the original discoverers. In particular, the foramen ovale in the fetus should be named as “foramen Galeni,” while the traditional eponym “foramen Botalli” should refer only to the foramen ovale which remains patent in the adult. The ductus arteriosus should be called “ductus Galeni” and the ductus venosus “ductus Vesalii.” As written in Mark Gospel (12:17): “Give Caesar what belongs to Caesar.”
CONFLICT OF INTEREST
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
ACKNOWLEDGMENTS
We thank Dr. Carla Frescura curator of the congenital heart disease collection of our institute for having stimulated us to write this paper and to provide fig. 2 and 3. This study is supported by the Registry for Cardio‐Cerebrovascular Pathology, Veneto Region, Venice, Italy, and by the Ministry of Health, target project RF‐2013‐02356762 "The genetics of sudden cardiac death in athletes and implication for risk prevention" Azienda Ospedaliera di Padova—University of Padua, Italy.
Zampieri F, Thiene G, Basso C, Zanatta A. The three fetal shunts: A story of wrong eponyms J. Anat.2021;238:1028–1035. 10.1111/joa.13357
REFERENCES
- Arantius, G.C. (1564) De humano foetus libellous. Leiden: Ex officina Felicis Lopes de Haro. [Google Scholar]
- Botallo, L. (1564) De catarrho. Paris: Bernardinum Turrisanum. [Google Scholar]
- Botallo, L. (1660) Opera omnia medica et chirurgica. Haec postrema editione a mendis repurgata, methodice disposita, paragraphis distincta, notis marginalibus, et authorum testimoniis aucta, hinc inde annotationibus illustrata, prodeunt e musaeo Joannis van Horne. Lugduni Batavorum: Ex officina Danielis et Abrahami a Gaasbeeck. [Google Scholar]
- Carcano Leone, G.B. (1574) Anatomici libri duo. Ticini: Apud Hieronimum Bartholum. [Google Scholar]
- Colombo, R. (1559) De re anatomica. Venetiis: Ex typographia Nicolai Beuilacquae. [Google Scholar]
- Elmaghawry, M. , Zanatta, A. & Zampieri, F. (2014) The discovery of pulmonary circulation from Imhotep to William Harvey. Global Cardiology Science and Practice, 2, 103–116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Falloppio, G. (1561) Observationes anatomicae. Venezia: (Grazioso Percacino) per Marcantonio Olmo. [Google Scholar]
- Folius, C. (1639) Sanguinis a dextro in sinistrum cordis ventriculum defluentis facilis reperta via cui non vulgaris in lacteas nuper patefactas venas animadversio praeponitur. Venice: Apud Bertanos. [Google Scholar]
- Franklin, K.J. (1941) Ductus venosus (Arantii) and ductus arteriosus (Botalli). Bulletin of the History of Medicine, 9, 580–584. [Google Scholar]
- Fransson, S.G. (1999) The botallo mystery. Clinical Cardiology, 22, 434–436. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gurunluoglu, R. , Shafighi, M. , Gurunluoglu, A. & Cavdar, S. (2011) Giulio Cesare Aranzio (Arantius) (1530–89) in the Pageant of Anatomy and Surgery. Journal of Medical Biography, 19, 63–69. [DOI] [PubMed] [Google Scholar]
- Hara, H. , Virmani, R. , Ladich, E. , Mackey‐Bojack, S. , Titus, J. , Reisman, M. et al. (2005) Patent foramen ovale: current pathology, pathophysiology, and clinical status. Journal of the American College of Cardiology, 46, 1768–1776. [DOI] [PubMed] [Google Scholar]
- Harvey, W. (1628) Exercitatio anatomica de motu cordis et sanguinis in animalibus. Francofurti: Sumptibus Gulielmi Fitzeri. [Google Scholar]
- His, W. (1895) Die anatomische Nomenclatur. Nomina anatomica, Verzeichniss der von der anatomischen Gesellschaft auf ihrer IX. Versammlung in Basel angenommenen Namen. Leipzig: Veit. [Google Scholar]
- Izquierdo, J.J. (1937) A new and more correct version of the views of Servetus on the circulation of the blood. Bulletin of the History of Medicine, 5, 914–932. [Google Scholar]
- Kachlík, D. , Baca, V. , Bozdechova, I. , Cech, P. & Musil, V. (2008) Anatomical terminology and nomenclature: past, present and highlights. Surgical and Radiologic Anatomy, 30, 459–466. [DOI] [PubMed] [Google Scholar]
- Kasten, T.G. (1954) Caecilius Folius on the circulation. Bulletin of the History of Medicine, 28, 15–31. [PubMed] [Google Scholar]
- Kopsch, F. & Knese, K.‐H. (1957) Nomina anatomica. Vergleichende Übersicht der Basler, Jenaer und Pariser Nomenklatur, 5th edition. Stuttgart: Thieme. [Google Scholar]
- Loukas, M. , Lam, R. , Tubbs, R.S. , Shoja, M.M. & Apaydin, N. (2008) Ibn al‐Nafis (1210–1288): the first description of the pulmonary circulation. American Surgeon, 74, 440–442. [PubMed] [Google Scholar]
- Morgagni, G.B. (1761) De sedibus et causis morborum per anatomen indagatis. Venice: Ex Typographia Remondiniana. [Google Scholar]
- Obladen, M. (2011) History of the ductus arteriosus: 1. Anatomy and spontaneous closure. Neonatology, 99, 83–89. [DOI] [PubMed] [Google Scholar]
- Ongaro, G. (1971) La scoperta della circolazione polmonare e la diffusione della Christianismi Restitutio di Michele Serveto nel XVI secolo in Italia e nel Veneto. Episteme, 5, 3–44. [PubMed] [Google Scholar]
- Scarpa, A. (1813) Elogio storico di Giambattista Carcano Leone professore di notomia nella Università di Pavia. Milan: dalla Stamperia Reale. [Google Scholar]
- Schneider, D.J. (2012) The patent ductus arteriosus in term infants, children, and adults. Seminars in Perinatology, 36, 146–153. [DOI] [PubMed] [Google Scholar]
- Shaw, J.R. (1972) Models for cardiac structure and function in Aristotle. Journal of the History of Biology, 5, 355–388. [DOI] [PubMed] [Google Scholar]
- Singer, P.N. (1968) Galen’s system of physiology and medicine. Basel and New York: Karger. [Google Scholar]
- Tallmadge, M.M. (Ed.) (1968) Galen on the usefulness of the parts of the body, 2nd edition. Ithaca: Cornell University Press. [Google Scholar]
- Tozzo, P. , Zanatta, A. , D’Angiolella, G. , Caenazzo, L. & Zampieri, F. (2020) Leonardo Botallo (1530–1587) and his pioneering contributions to traumatology, cardiology and deontology. Journal of Medical Biography. 10.1177/0967772020940976 [DOI] [PubMed] [Google Scholar]
- Van Praagh, R. & Van Praagh, S. (1983) Aristotle, “triventricular” heart and the relevant early history of the cardiovascular system. Chest, 84, 462–466. [DOI] [PubMed] [Google Scholar]
- Vesalius, A. (1564) Anatomicarum Gabrielis Falloppii observationum examen. Venetiis: Apud F. de Franciscis senensem. [Google Scholar]
- Zampieri, F. , Zanatta, A. , Basso, C. & Thiene, G. (2016) Cardiovascular medicine in Morgagni’s De sedibus: dawn of cardiovascular pathology. Cardiovascular Pathology, 25, 443–452. [DOI] [PubMed] [Google Scholar]