

Summary
Celiac disease is a multi-factorial chronic inflammatory intestinal disease, characterized by malabsorption resulting from mucosal injury after ingestion of wheat gluten or related rye and barley proteins. Inappropriate T-cell-mediated immune response against ingested gluten in genetically predisposed people, leads to characteristic histological lesions, as villous atrophy and intraepithelial lymphocytosis. Nevertheless, celiac disease is a comprehensive diagnosis with clinical, serological and genetic characteristics integrated with histological features. Biopsy of duodenal mucosa remains the gold standard in the diagnosis of celiac disease with the recognition of the spectrum of histological changes and classification of mucosa damage based on updated Corazza-Villanacci system. Appropriate differential diagnosis evaluation and clinical context also for the diagnosis of complications is, moreover, needed for correct histological features interpretation and clinical management.
Key words: celiac disease, sprue, small bowel, gluten
Introduction
Celiac disease (CD) is an immune-mediated inflammatory disorder of the small intestine occurring in genetically predisposed individuals when exposed to gluten 1. CD can occur at any age, from early childhood to elderly, with two peaks of onset, one shortly after weaning with gluten in the first 2 years of life and the other during the second or third decade of life with a preference for females (male/female ratio 1:2). The disease has a variable incidence, with a worldwide prevalence of about 1:100; in Europe is estimated between 0.3 and 1.2% 2,3. A correct diagnosis of CD requires a precise reconstruction of a puzzle, whose pieces are represented by the clinical, serological, genetic and histological aspects. The evaluation of all these factors, apart from genetics, must take place while the patient is still on a diet containing gluten, since a gluten-free diet changes the clinical, serological and histological pattern, making it impossible to recognize the characteristic aspects of disease. Nonetheless, CD still represents an under-recognized condition, due to heterogeneous symptoms and/or poor disease awareness, and the occurrence of diagnostic delay ranging from 4 to 13 years has been reported by some authors 4-9.
Clinical and laboratory aspects
The diagnosis of CD can be very challenging, since symptoms can significantly vary from patient to patient and this variability has been compared, not surprisingly, to a chameleon 10. In 2011, the Oslo Classification ranked the clinical presentation of CD in classical, non classical, subclinical and refractory 11. The gold standard for CD diagnosis is represented by the combination of both mucosal changes and positivity of serological tests 12,13.
Serologic markers
A major role in the diagnostic process of CD is played by serology, which allows identification of the subjects who should undergo intestinal biopsy; the following are the most important tests and their relative significance:
IgA class antitransglutaminase antibodies (tTGA) are the tests with the highest sensitivity for CD (98%) with specificity estimated at around 90%. High titles of IgA class tTGA (> 5 times the cut-off) are almost always the expression of CD;
IgA class antiendomysial antibodies (EMA), this test has a lower sensitivity compared to IgA class tTGA (90% vs. 98%), but shows an almost absolute specificity for CD;
IgA class antigliadin antibodies (AGA) are now an obsolete test with levels of sensitivity and specificity significantly lower than tTGA and EMA, and the search for their presence is useful only in early childhood (children aged < 2 years); since they are the first antibodies to appear, they show a higher sensitivity than other tests in this age group. Regard to the IgG class of antibodies, their use should be restricted to patients with selective IgA deficiency, because only in this subgroup of patients the response is indicative for CD.
Genetic testing
CD is closely associated with histocompatibility antigens (HLA) DQ2 and DQ8. Practically all CD patients are positive for one or both of these HLAs or for a fraction of the heterodimer, but genetic testing is never diagnostically significant since at least 30% of the general population present the same HLAs as coeliac patients.
The genetic test should be performed in cases where there is a discrepancy between serology and histology and in 1st degree relatives to assess the genetic predisposition to CD.
The main clinical significance of genetic testing is to exclude a diagnosis of CD in the absence of HLA-DQ2 (and its fractions) and -DQ8 in cases of diagnostic doubt and predisposition to CD in family members of coeliac patients in the absence of HLADQ2 (and fractions) and -DQ8 14,15.
Approach to duodenal biopsy
The biopsies that the pathologist receives nowadays are all performed by endoscopic examination, which, in addition to the duodenum, makes it possible to explore other districts of the gastro-intestinal tract. The following are some points which require a close working relationship between the endoscopist, the endoscopy-room nurse, the pathology laboratory technician and the pathologist 16.
Site of the biopsy
Biopsy by endoscopy should be performed in the bulb (in particular this site in children) and second duodenal portion; the recommendation in this field are at least 4 biopsies, 2 for each of sites mentioned above 17-19.
Orientation of the biopsy sample
Biopsy orientation is a crucial event for a proper histological assessment. We suggest the use of acetate cellulose filters previously cut and in this setting it is fundamental a strict relationship between endoscopist-nurse-technicians and pathologist. The endoscopist can place each mucosal sample in a straight line and with proximal-to-distal orientation onto the cellulose acetate filter with a “clarinet beak-shaped cut” (Bio-Optica). Such a filter allows a perfect adherence of biopsies and, being chemically inert and not reactive with fixative or processing chemicals, it does not alter the quality of histological sections at all. As the embedding phase starts, the filters are 90 degrees-rotated by technician, in order to ensure the best trans-sectional cut. The above described procedure is time- and money-sparing, allowing a significant improvement of diagnostic accuracy.
Stains
The “old mistress” haematoxylin-eosin is sufficient to assess all the necessary morphological elements (one or two sections can be used, if needed, for immunohistochemical assessment, generally for CD3 immunostain which is useful for a correct count of T lymphocytes) 20.
Histopathological aspects of normal and pathological duodenal mucosa
NORMAL INTESTINAL MUCOSA
Villi: digitiform appearance with the ratio between the height of the villi and of the crypts always in favor of the villus (3:1 or more).
Intra-epithelial lymphocytic infiltrate: the number of intraepithelial lymphocytes (T lymphocytes; IEL) is subject to individual variability. The majority of normal subjects have less than 25 lymphocytes per 100 epithelial cells; based on the experiences of Hayat and Veress 21,22 a count of IEL over 25/100 epithelial cells is considered pathological. The intraepithelial lymphocyte count is very important and should always be done, especially in the initial lesions, using anti-CD3 antibodies.
Glandular crypts: the crypts are comprehensive of epithelial cells, endocrine cells, goblet cells and Paneth cells; mitosis are in general 1 for any crypt.
Lamina propria: plasma cells, eosinophils, histiocytes, mast cells and lymphocytes are normally found in the lamina propria. Neutrophils are generally absent, except in cases of active duodenitis with possible gastric metaplasia closely related to Helicobacter pylori infection; eosinophils must never be more than 5 per field at 40× 20.
PATHOLOGICAL INTESTINAL MUCOSA
The histological diagnosis of CD consists of an integrated assessment of the following elementary lesions:
Increased intraepithelial T-lymphocytes: a value of 25 T-lymphocytes/100 enterocytes is considered a pathological condition also called “lymphocytosis”.
Crypt hyperplasia: extension of the regenerative epithelial crypts associated with presence of more than 1 mitosis per crypt.
Villous atrophy: decrease in villous height, alteration of normal crypt/villous ratio (3:1) until total disappearance of villi. This assessment requires proper orientation of the biopsies.
None of these elementary lesions is specific for CD; the diagnosis of CD is based on the identification of histological alterations accompanied by clinical and serological consistent data. On the basis of the presence of one or more of these elementary lesions the histopathology of CD is subdivided into different diagnostic categories according to the Marsh classification 23.
TYPE 1 OR INFILTRATIVE LESION
Villi within normal morphological limits (normal villous/crypt ratio 3:1);
increased number of IEL (greater than 25/100 epithelial cells).
TYPE 2 OR HYPERPLASTIC LESION
Villi architecturally within normal morphological limits (like type 1);
increased number of IEL (greater than 25/100 epithelial cells) (like type 1);
hyperplasia of the glandular elements (regenerative aspects highlighted by the reduced mucinous activity and increased number of mitoses).
TYPE 3 OR DESTRUCTIVE LESION
Varying degrees of villous atrophy associated with hyperplasia of glandular crypts;
surface enterocytes with reduced height, irregular brush border and sometimes cytoplasmic vacuoles;
increased number of IEL (like type 1 and 2 lesions).
A combination of the three factors described above with adeguate clinical informations (i.e. anamnesis and serological/genetic data) is consistent with a CD diagnosis. This classification is universally recognized for the diagnosis of CD, and extensively validated; the only point worthy of observation and critical analysis is that mild, moderate or severe atrophy (total villous flattening) are all grouped together in a single category: the type 3 lesion.
A modification to this classification has been proposed by Oberhuber et al. 24 who divided the Marsh type 3 lesion into three subgroups:
3a mild villous atrophy and pathological increase of IEL;
3b moderate villous atrophy and pathological increase of IEL;
3c total villous atrophy and pathological increase of IEL.
Along the same lines, and in an attempt to simplify and standardize the work of pathologists and facilitate the relationship between pathologists and clinicians, a new version of the histological classification has recently been proposed by Corazza and Villanacci 25,26; in particular, the lesions that characterize CD have been divided into two categories: non-atrophic (grade A) and atrophic (grade B).
Grade A lesions are characterized by normal villi but with a pathological increase in IEL.
Grade B lesions are further subdivided into:
Grade B1 in which the villus/crypt ratio is less than 3:1 and pathological increase of IEL is present;
Grade B2 in which the villi are no longer identifiable and pathological increase of IEL is present.
Recently a simplified classification with only two entities was proposed 27 (Tab. I).
Table I.
Comparison of Marsh - Corazza-Villanacci - Villanacci classification schemes.
| Marsh mod. Oberhuber | Corazza-Villanacci | Villanacci | |
|---|---|---|---|
| Lesions | Diagnostic Criteria | Lesions | Lesions |
|
Type I lesion infiltrative |
No architectural changes (villous/cript ratio preserved) Increased IELs count (> 25/100 epithelial cells) |
Grade A lesion not atrophic No architectural changes (villous/cript ratio preserved) Increased IELs count (> 25/100 epithelial cells) |
A Non atrophic type No architectural changes (villous/cript ratio preserved) Increased IELs count (> 25/100 epithelial cells) |
|
Type II lesion hyperplastic |
No architectural changes (villous/cript ratio preserved) Crypt hyperplasia (mitoses > 1/crypt) Increased IELs count (> 25/100 epithelial cells) |
||
|
Type III A lesion destructive |
Villous atrophy (mild degree) Crypt hyperplasia (mitoses > 1/crypt) Increased IELs count (> 25/100 epithelial cells) |
Grade B1 lesion partial atrophy Villous atrophy (mild-moderate degree) Crypt hyperplasia (mitoses > 1/crypt) Increased IELs count (> 25/100 epithelial cells) |
B Atrophic type Villous atrophy (mild-moderate-severe degree) Crypt hyperplasia (mitoses > 1/crypt) Increased IELs count (> 25/100 epithelial cells) |
|
Type III B lesion destructive |
Villous atrophy (moderate degree) Crypt hyperplasia (mitoses > 1/crypt) Increased IELs count (> 25/100 epithelial cells) |
||
|
Type III C lesion destructive |
Villous atrophy (severe degree) Crypt hyperplasia (mitoses > 1/crypt) Increased IELs count (> 25/100 epithelial cells) |
Grade B2 lesion total atrophy Villous atrophy (severe degree) Crypt hyperplasia (mitoses > 1/crypt) Increased IELs count (> 25/100 epithelial cells |
|
Immunohistochemistry
One of the key points in the CD diagnosis is the number of IEL, which are CD3 and CD8 positive T lymphocytes; in pathological conditions, their number should be more than 25 lymphocytes per 100 epithelial cells. The counts can be performed reasonably well on the normal and irreplaceable hematoxylin-eosin but we suggest, especially in the initial forms, that an immunohistochemical assessment should always be carried out with monoclonal CD3 antibodies which often allows for a more accurate evaluation of T lymphocytes (Fig. 1) 28-31.
Figure 1.
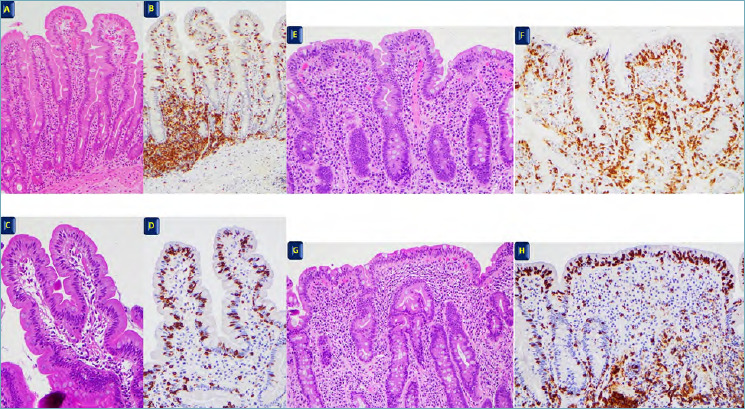
(A-B): normal duodenal mucosa; villous/crypt ratio over 3:1; number of T lymphocytes < 25 x 100 epithelial cells. (A) H&E x 10, (B) CD3 immunostain x 10. (C-D): Type 1 - Grade A lesion; normal villi but with pathological increase of T lymhocytes > 25 x 100 epithelail cells. (C) H&E x 20, (D) CD3 immunostain x 20. (E-F): mild to moderate villous atrophy Type 3A-3B - Grade B1 with pathological increase of T lymphocytes. (E) H&E x 20, (F) CD3 immunostain x 20. (G-H): severe villous atrophy Type 3C - Grade B2 with pathological increase of T lymphocytes. (G) H&E x 20, (H) CD3 immunostain x 20.
Non celiac gluten sensitivity (NCGS)
Non-celiac gluten sensitivity (NCGS) is “a clinical entity induced by the ingestion of gluten leading to intestinal and/or extraintestinal symptoms that improve once the gluten-containing foodstuff is removed from the diet, and CD and wheat allergy have been excluded” 32. The histologic characteristics of NCGS are still under investigation, ranging from normal histology to a slight increase in the number of T lymphocytes in the superficial epithelium of villi. Some authors described a normal number of T lymphocytes but a peculiar disposition of this cells in small “cluster” of 3-4 elements in the superficial epithelium, as well as the linear disposition in the deeper part of the mucosa together with an increased number of eosinophils (> 5/HPF) in lamina propria. Further studies are needed to assess these findings as specific for NCGS 33 (Fig. 2).
Figure 2.
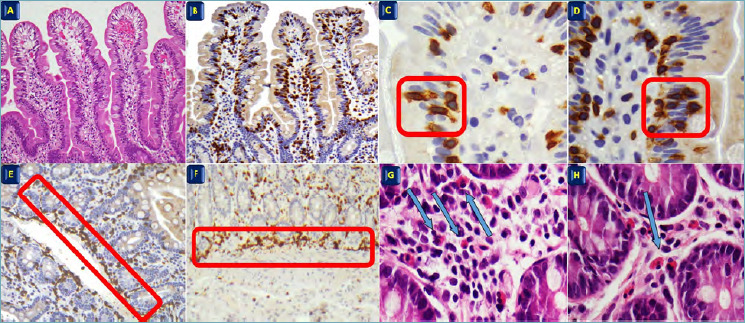
(A-B): normal villi; T lymphocytes < 25 x 100 epithelial cells. (A) H&E x 10, (B) CD3 immunostain x 10. (C-D): cluster of T Lymphocytes in the superficial epithelium. (C-D) CD3 immunostain x 60 red rectangle. (E-F): linear disposition of T lymphocytes in the deeper part of the mucosa. CD3 immunostain x 4 red rectangle. (G-H): eosinophils in lamina propria.
Differential diagnosis
CD shares its duodenal histopathologic features with a large variety of intestinal disorders. Thus, a correct diagnosis may be reached only by an integrated evaluation of clinical manifestations, laboratory and HLA tests and endoscopic findings, as well as histopathologic findings. Main conditions with histologic changes that can overlap with CD and some tips for differential diagnosis are summarized in Table II.
Table II.
Major CD non-neoplastic mimickers and histopathologic features useful for differential diagnosis.
| Mimicker | Increased IELs | Villous atrophy | Histopathologic tips for differential diagnosis |
|---|---|---|---|
| Infectious diseases | |||
| Parasitic infestation | Rare (in children) | Rare (in children) | Identification of parasites (e.g. Giardia); increased eosinophils in lamina propria |
| HP-positive gastritis and peptic duodenitis | Possible | Possible, mild (if present) | Foveolar metaplasia of the duodenum; increased plasma cells in lamina propria; neutrophilic infiltration in lamina propria and epithelium; changes more prominent in the bulbus; HP in gastric biopsies |
| Tropical sprue | Yes | Yes, usually low-grade | Extensive ileal involvement |
| Bacterial overgrowth | Yes | Possible | Mild lesions |
| Whipple disease | Rare | Yes | PAS-positive macrophages in lamina propria |
| Viral gastroenteritis or post-infectious changes | Yes | Possible, variable grade | Mucosal recovery after infection resolution |
| Drugs | |||
| NSAIDs | Possible | Rare, patchy, mild | Erosions, neutrophilic infiltration in lamina propria |
| Antineoplastic and immune modulatory drugs (including immune checkpoint inhibitors) | Rare | Possible | Crypt architectural distortion; neutrophilic infiltration in lamina propria; foci of crypt apoptosis; involvement of other gastrointestinal tracts (gastritis, colitis) |
| ARBs use (Olmesartan and others) | Possible | Frequent, variable grade | Neutrophilic infiltration in lamina propria; deposition of subepithelial collagen, foci of crypt apoptosis |
| Other immune-inflammatory conditions | |||
| Collagenous sprue | Yes | Frequent, variable grade | Deposition of subepithelial collagen |
| Immunodeficiencies (including CVID) | Yes | Possible, variable grade | Depletion of plasma cells in lamina propria, follicular lymphoid hyperplasia; concomitant giardiasis |
| Autoimmune enteropathy | Possible (celiac pattern) | Yes, variable grade | Neutrophilic infiltration in lamina propria; crypt apoptosis; reduction in goblet and Paneth cells; diffuse involvement of other gastrointestinal tracts (gastritis, enteritis, colitis) |
| Crohn’s disease and ulcerative colitis-associated duodenitis | Rare | Rare, patchy (if present) | Erosions/ulcerations, neutrophilic inflammation; crypt distortion; microgranulomas; basal plasmacytosis; ileal and colonic involvement |
| Eosinophilic gastroenteritis and food protein-sensitive enteropathies (including gluten-sensitive enteropathy) | Possible | Possible, usually not severe | Increased eosinophils in lamina propria; involvement of other gastrointestinal tracts (enteritis and colitis) |
Legend: ARB: angiotension receptor blocker; CVID: common variable immunodeficiencies; HP: Helicobacter pylori; IEL: intraepithelial lymphocyte; NSAID: non-steroidal anti-inflammatory drug; PAS: periodic acid Schiff.
Common entities characterized by intraepithelial lymphocytosis without villous atrophy include several medications, Helicobacter pylori gastritis, duodenal parasitic infestations, and autoimmune conditions. Potential confounders which typically cause villous atrophy comprise olmesartan and other angiotensin receptor blockers, various immunomodulatory drugs, common variable immunodeficiency, autoimmune enteropathy, Whipple disease and tropical sprue 1,34.
Several medications, including nonsteroidal anti-inflammatory drugs (NSAIDs), immunomodulatory and antineoplastic drugs, can mimic CD histologically; however, villous atrophy is seldom described in these cases. In addition, use of NSAIDs has been reported to usually cause mucosal erosions/ulcerations with inflammatory infiltrate composed with plasma cells and neutrophils 35, while crypt architectural distortion, neutrophilic infiltration, ischemic changes, villous blunting, epithelial cell apoptosis in crypts and neutrophilic cryptitis were occasionally described in individuals treated with checkpoint inhibitors or kinase inhibitors 36,37. Olmesartan, an angiotensin II receptor blocker, was proved to cause partial to complete villous atrophy and increased IEL, thus mimicking CD histology 38.
Helicobacter pylori (HP) infection may determinate an epithelial lymphocytosis generally with minimal villous changes. Foveolar gastric metaplasia and marked neutrophilic infiltration in epithelium and/or lamina propria may help in distinguishing HP-related peptic duodenitis from microscopic alterations of CD 39. Although intestinal parasitic organisms may show every CD histopathologic hallmark, a high number of eosinophils in lamina propria should prompt the pathologist to search for the presence of parasites. Giardiasis, caused by Giardia lamblia, is one of the most common intestinal parasitic disease. Giardia can be easily identified in duodenal biopsy samples as a pear-shaped organism with two paired nuclei, located in lumen, adjacent to the epithelium. It usually does not determine significant histologic lesions, even if villous blunting, intraepithelial lymphocytosis and/or crypt hyperplasia are rarely observed in children 40. Nevertheless, the presence of villous atrophy in association with signs of parasitic infections should hint the possibility of an underlying CD 41.
Food protein-sensitive enteropathies can also reproduce CD histologic abnormalities, but they tend to be transient or to respond to dietary allergen withdrawal. In duodenal biopsies from patients with pernicious anemia, partial villous blunting and mucosal chronic inflammatory infiltration may be detected, along with the more typical epithelial megaloblastic changes 42.
Collagenous sprue is a rare malabsorption condition which is often misdiagnosed as CD; however, the identification of a thick subepithelial collagen type I band with inflammatory cells and capillaries entrapped may lead to a correct diagnosis 43,44. A significant, albeit variable, fraction of cases is associated with CD and may be treated with combinations of a gluten-free diet and immunosuppressive therapy.
Common variable immunodeficiency (CVID) enteropathy may mimic CD. Nevertheless, two distinguishing features, usually absent in CD individuals, may be found in duodenal samples of CVID patients: depletion in plasma cells (present in about two-third of cases) and follicular lymphoid hyperplasia 45. Furthermore, pathologists should always search for a coexisting Giardia lamblia infection, as it was reported in 23% of cases by Malamut et al. 46. In a minority of CVID patients, villous atrophy is gluten-sensitive 47.
Autoimmune enteropathy, a disease characterized by small intestinal mucosal atrophy and circulating autoantibodies towards enterocytes and/or goblet cells, may show an active enteritis pattern, characterized by expansion of the lamina propria by mixed inflammation with neutrophil infiltrates, or a CD-like pattern 48-50. Foci of apoptotic epithelial cells and reduction in goblet and Paneth cells may rarely be observed. Importantly, biopsies from other gastrointestinal sites often show histologic abnormalities and may aid for diagnosis.
Lastly, it should be remembered that forms of idiopathic villous atrophy (villous atrophy or sprue of unknown aetiology) may cause diagnostic challenges. Some of these patients have spontaneous histological recovery and are associated with excellent survival, whereas others show persistent villous atrophy, with or without associated lymphoproliferative disorders 51.
Complications of CD
Refractory celiac disease (RCD)
RCD a condition characterized by prolonged villous atrophy in duodenal biopsies of a CD patient, along with malabsorption symptoms, despite a strict adherence to gluten-free diet (GFD) over a minimum period of 12 months 52,53. Other causes of persistent villous atrophy or slow-to-respond CD must be carefully excluded before making a diagnosis of RCD. Endoscopic abnormalities such as mucosal erosions, ulcerations (ulcerative duodeno-jejunitis) or strictures may be observed.
It is a rare CD complication with a variable incidence and prevalence. A systematic review by Rowinski and Christensen54 showed a cumulative incidence of 1-4% over 10 years and a prevalence of 0.31%-0.38% in CD patients, while a study based on a cohort of celiac individuals in Austria reported an incidence over 25 years of 2.6% 55. Globally, RCD incidence seems to be decreasing during the last 20 years, probably because of increased awareness, stricter adherence to GFD and greater availability of gluten-free products 55,56. Mean age at RCD diagnosis has been reported to be abound 63 years. Generally, the median time between the diagnosis of CD and the diagnosis of RCD is 21 months, although rare cases of RCD primarily diagnosed at the time of first presentation of malabsorption symptoms have been described 57.
Two types of RCD have been recognized on the bases of their clinical, histologic and molecular features. Type I RCD is characterized by an usual immunophenotype of IEL (i.e. retained expression of surface CD3, CD8 and CD103) and absence of a monoclonal T cell receptor (TCR) gene rearrangement, whereas type II RCD is marked by an aberrant intraepithelial lymphocyte immunophenotype (i.e. > 50% of intraepithelial T cells lacking CD8 by immunohistochemistry on formalin-fixed paraffin-embedded sections and/or >20-25% CD45+ T cells lacking surface CD3 on flow cytometry), and a monoclonal TCR gene rearrangement 54. TCR gene rearrangement clonal analysis by multiple polymerase chain reaction may be efficiently performed also on formalin-fixed paraffin-embedded tissues. As samples from duodenal mucosa from normal, CD or RCD type I patients may occasionally show TCR-β or TCR-γ clonality, the diagnosis and typing of RCD should be only made by a gastroenterologist after an integrated evaluation of clinical information, histology, intraepithelial lymphocyte immunophenotype (by immunohistochemistry or flow cytometry) and clonal analysis 58,59. Flow cytometry seems to be better than CD8 immunohistochemistry in differential diagnosis between type I and II RCD. However, a recent study found that immunohistochemical expression of a NK biomarker, NKp46, on T-cell surface, may help in distinguishing RCD type II (NKp46-positive) from RCD type I, usually showing no or few NKp46-positive T-cells 60. Histology of RCD type I may be indistinguishable from untreated responsive CD; however, a collagenous sprue-type pattern and basal plasmocytosis are rarely noted in RCD type I. Making a correct diagnosis is of pivotal importance because type I and type II RCD have very different prognosis, therapy response and rate of development of lymphoproliferative malignancies. RCD type I has 5-year survival rates up to 95%, response rate to corticosteroids of 90% and rates of developing enteropathy-associated T-cell lymphoma (EATL) 5 year after RCD diagnosis lower than 14%; on the other hand, RCD type II has a 5-year survival of 58%, lower response rate to corticosteroids and higher rates of developing EATL 54,61.
Lymphoproliferative malignancies
CD individuals, especially those with longstanding disease, have a relative risk of developing extra-nodal non-Hodgkin lymphoma around 3-4 times higher than general population 60.
EATL is an aggressive malignancy complicating CD, commonly involving jejunum and ileum and characterized by markedly atypical malignant cells, densely infiltrating both the epithelium, which typically shows severe villous atrophy, and the lamina propria, extending below muscularis mucosae. Neoplastic cells are positive for CD3 and CD103, negative for CD5 and CD4, express CD8 variably, contain cytotoxic granule-associated proteins and harbor a clonal rearrangement of TCRγ and/or TCRβ genes 61.
EATL should be distinguished from monomorphic epitheliotrophic intestinal T-cell lymphoma (MEITL), composed of monomorphic, not significantly atypical, small- to medium-sized T cells, immunoreactive for CD3, CD8, CD56, CD103, and TIA1 and negative for CD5, CD4, CD30. Neoplastic T cells infiltrate both the lamina propria and the epithelium, causing partial or severe villous atrophy. Although the latest WHO classification of lymphoid neoplasms denied any association of MEITL with CD, it was recently described in two CD patients 62. Both EATL and MEITL have an ominous prognosis, with a reported 5-year survival rate lower than 20% 63 (Fig. 3).
Figure 3.
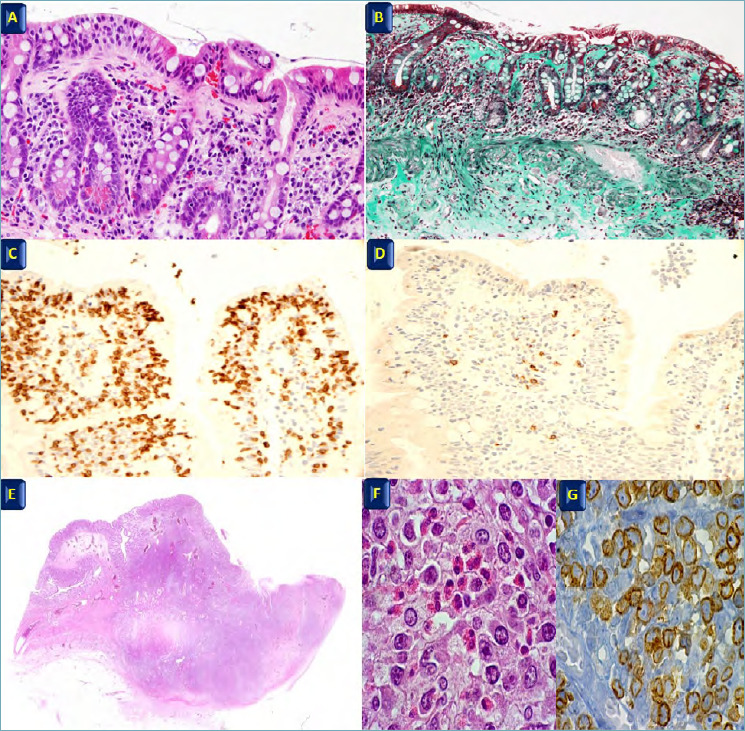
(A-B): collagenous sprue; pathological increase in the thickness of the connective tissue band under the superficial epithelium > 10 mμ; (A) H&E x 20; (B) Trichrome stain x 20. (C-D): refractory celiac disease; pathological increase of T lymphocytes CD3 positive (C) negativity for CD8 (D). C-D x 20. (E-F): enteropathy type T cell lymphoma; (E) x 4, (F) H&E x 40; (G) CD3 immunostain x 40.
Small bowel carcinoma (SBC)
Patients with CD have an increased risk of developing SBC. CD-associated SBC was shown to arise after a median CD duration of 17 months in patients with a median age of 53 years and to predominantly involve the jejunum. CD-associated SBCs harbor mismatch repair deficiency more frequently in comparison with Crohn’s disease-associated or sporadic SBCs 64,65. In addition, they often showed a high number of tumor infiltrating lymphocytes and a subset of them has a medullary-type histology 66. Importantly, they usually display a relatively indolent behavior. SBC in CD patients is rarely associated with adjacent preinvasive neoplastic/dysplastic lesions, which, like their invasive components, usually express nuclear β-catenin, while retaining mismatch repair protein expression. Recently, Giuffrida and colleagues found that CD-associated SBCs are often infiltrated by PD-1-positive T-cells and show expression of PD-L1 in neoplastic/immune cells (combined positive score ≥ 1) in more than one third of cases 67.
Liver complications
Some CD patients may have altered liver function tests and/or develop a wide spectrum of liver diseases, encompassing cryptogenic hepatitis, steatohepatitis, cirrhosis, as well as liver autoimmune disorders 68.
Conclusion
CD is a very common disorder affecting most people in the silent form. Many of these patients are identified through screening of at-risk groups or after malabsorption symptoms onset, rarely for disease-associated complications. CD diagnosis and its differential diagnosis is made from integrations between typical histological findings and clinical, serological and immunological features. Corazza-Villanacci System is a helpful method to assess mucosal damage and and the response to gluten-free diet in patient follow-up.
Figures and tables
References
- 1.Robert ME, Crowe SE, Burgart L, et al. Statement on best practices in the use of pathology as a diagnostic tool for celiac disease: a guide for clinicians and pathologists. Am J Surg Pathol 2018;42:e44-e58. https://doi.org/10.1097/PAS.0000000000001107 10.1097/PAS.0000000000001107 [DOI] [PubMed] [Google Scholar]
- 2.Volta U, Caio G, Stanghellini V, et al. Non-celiac gluten sensitivity: questions still to be answered despite increased awarness. Cell Mol Immunol 2013;10:383-92. https://doi.org/10.1038/cmi.2013.28 10.1038/cmi.2013.28 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Caio G, Volta U, Sapone A, et al. Celiac disease: a comprehensive current review. BMC Medicine 2019;17:142-62. https://doi.org/10.1186/s12916-019-1380-z 10.1186/s12916-019-1380-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ludvigsson JF, Rubio-Tapia A, van Dyke CT, et al. Increasing incidence of celiac disease in a North American population. Am J Gastroenterol 2013:108:818-24. https://doi.org/10.1038/ajg.2013.60 10.1038/ajg.2013.60 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Mustalahti K, Catassi C, Reunanen A, et al. The prevalence of celiac disease in Europe: results of a centralized, international mass screening project. Ann Med 2010;42:587-95. https://doi.org/10.3109/07853890.2010.505931 10.3109/07853890.2010.505931 [DOI] [PubMed] [Google Scholar]
- 6.Sanders DS, Patel D, Stephenson TJ, et al. A primary care cross-sectional study of undiagnosed adult coeliac disease. Eur J Gastroenterol Hepatol 2003;15:407-13. https://doi.org/10.1097/00042737-200304000-00012 10.1097/00042737-200304000-00012 [DOI] [PubMed] [Google Scholar]
- 7.Sanders DS, Hurlstone DP, Stokes RO, et al. Changing face of adult coeliac disease: experience of a single university hospital in South Yorkshire. Postgrad Med J 2002;78:31-3. https://doi.org/10.1136/pmj.78.915.31 10.1136/pmj.78.915.31 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.West J, Fleming KM, Tata LJ, et al. Incidence and prevalence of celiac disease and dermatitis herpetiformis in the UK over two decades: population-based study. Am J Gastroenterol 2014;109:757-68. https://doi.org/10.1038/ajg.2014.55 10.1038/ajg.2014.55 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Lo W, Sano K, Lebwohl B, et al. Changing presentation of adult celiac disease. Dig Dis Sci. 2003, 48:395-8. https://doi.org/10.1023/a:1021956200382 10.1023/a:1021956200382 [DOI] [PubMed] [Google Scholar]
- 10.Fasano A. Celiac disease: how to handle a clinical chamaleon. N Eng J Med 2003; 348:2568-70. https://doi.org/10.1056/NEJMe030050 10.1056/NEJMe030050 [DOI] [PubMed] [Google Scholar]
- 11.Ludviggson JF, Leffler DA, Bai JC, et al. The Oslo Classification for coeliac disease and related terms. Gut 2013;6:43-52. https://doi.org/10.1136/gutjnl-2011-301346 10.1136/gutjnl-2011-301346 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Caio G, Volta U, Sapone A, et al. Celiac disease: a comprehensive current review. BMC Medicine 2019;17:142-62. https://doi.org/10.1186/s12916-019-1380-z 10.1186/s12916-019-1380-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Ciacci C, Ciclitira P, Hadjivassiliou M, et al. The gluten-free diet and its current application in coeliac disease and dermatitis herpetiformis. United European Gastroenterol J. 2015;3:121-35. https://doi.org/10.1177/2050640614559263 10.1177/2050640614559263 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Volta U, Granityo A, Fiorini E, et al. Usefulness of antibodies to deamidated gliadin peptides in celiac disease diagnosis and follow up. Dig Dis Sci 2008;853:1582-8. https://doi.org/10.1007/s10620-007-0058-0 10.1007/s10620-007-0058-0 [DOI] [PubMed] [Google Scholar]
- 15.Volta U, Tovoli F, Piscaglia M, et al. Old and new serological testsfor celiac disease screening. EXP Rev Gastroenterol Hepatol 2010;4:31-5. https://doi.org/10.1586/egh.09.66 10.1586/egh.09.66 [DOI] [PubMed] [Google Scholar]
- 16.Serra S, Jani PA. An approach to duodenal biopsies. J Clin Pathol 2006;59:1133-50. https://doi.org/10.1136/jcp.2005.031260 10.1136/jcp.2005.031260 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Pais WP, Duerksen DR, Pettigrew NM, et al. How many duodenal biopsy specimens are required to make a diagnosis of celiac disease? Gastrointest Endosc 2008;67:1082-7. https://doi.org/10.1016/j.gie.2007.10.015 10.1016/j.gie.2007.10.015 [DOI] [PubMed] [Google Scholar]
- 18.Latorre M, Lagana SM, Freedberg DE, et al. Endoscopic biopsy technique in the diagnosis of celiac disease: one bite or two? Gastrointest Endosc 2015;81:1228-33. https://doi.org/10.1016/j.gie.2014.10.024 10.1016/j.gie.2014.10.024 [DOI] [PubMed] [Google Scholar]
- 19.De Leo L, Villanacci V, Ziberna F, et al. Immunohistologic analysis of the duodenal bulb: a new method for celiac disease diagnosis in children. Gastrointest Endosc. 2018;88:521-6. https://doi.org/10.1016/j.gie.2018.05.014 10.1016/j.gie.2018.05.014 [DOI] [PubMed] [Google Scholar]
- 20.Villanacci V, Ceppa P, Tavani E, et al. Coeliac disease: the histology report. Dig Liver Dis. 2011;43 Suppl 4:S385-95. https://doi.org/10.1016/S1590-8658(11)60594-X 10.1016/S1590-8658(11)60594-X [DOI] [PubMed] [Google Scholar]
- 21.Hayat M, Cairns A, Dixon MF, et al. Quantitation of intraepithelial lymphocytes in human duodenum: what is normal? J Clin Pathol 2002;55:393-4. https://doi.org/10.1136/jcp.55.5.393 10.1136/jcp.55.5.393 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Veress B, Franzen L, Bodin L, et al. Duodenal intraepithelial lymphocyte-count revisited. Scand J Gastroenterol 2004;39:138-44. https://doi.org/10.1080/00365520310007675 10.1080/00365520310007675 [DOI] [PubMed] [Google Scholar]
- 23.Marsh MN. Grains of truth: evolutionary changes in small intestinal mucosa in response to environmental antigen challenge. Gut 1990;31:111-4. https://doi.org/10.1136/gut.31.1.111 10.1136/gut.31.1.111 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Oberhuber G, Granditsch G, Vogelsang H. The histopathology of coeliac disease: time for a standardized report scheme for pathologists. Eur J Gastroenterol Hepatol 1999;11:1185-94. https://doi.org/10.1097/00042737-199910000-00019 10.1097/00042737-199910000-00019 [DOI] [PubMed] [Google Scholar]
- 25.Corazza GR, Villanacci V. Coeliac disease. J Clin Pathol. 2005;58:573-4. https://doi.org/10.1136/jcp.2004.023978 10.1136/jcp.2004.023978 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Corazza GR, Villanacci V, Zambelli C, et al. Comparison of the Interobserver reproducibility with different histologic criteria used in celiac disease. Clin Gastroenterol Hepatol 2007;5:838-43. https://doi.org/10.1016/j.cgh.2007.03.019 10.1016/j.cgh.2007.03.019 [DOI] [PubMed] [Google Scholar]
- 27.Villanacci V. The histological classification of biopsy in celiac disease: time for a change? Dig Liver Dis 2015;47(1):2-3. https://doi.org/10.1016/j.dld.2014.09.022 10.1016/j.dld.2014.09.022 [DOI] [PubMed] [Google Scholar]
- 28.Shidrawi RG, Przemioslo R, Davies DR, et al. Pitfalls in diagnosing coeliac disease. J Clin Pathol 1994;47:693-4. https://doi.org/10.1136/jcp.47.8.693 10.1136/jcp.47.8.693 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Eigner W, Wrba F, Chott A, et al. Early recognition of possible pitfalls in histological diagnosis of celiac disease. Scand J Gastroenterol 2015;50:1088-93. https://doi.org/10.3109/00365521.2015.1017835 10.3109/00365521.2015.1017835 [DOI] [PubMed] [Google Scholar]
- 30.Freeman HJ. Pearls and pitfalls in the diagnosis of adult celiac disease. Can J Gastroenterol 2008;22:273-80. https://doi.org/10.1155/2008/905325 10.1155/2008/905325 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Ravelli A, Villanacci V. Tricks of the trade: how to avoid histological pitfalls in celiac disease. Pathol Res Pract 2012;208(4):197-202. https://doi.org/10.1016/j.prp.2012.01.008 10.1016/j.prp.2012.01.008 [DOI] [PubMed] [Google Scholar]
- 32.Fasano A, Sapone A, Zevallos V, et al. Nonceliac gluten sensitivity. Gastroenterology 2015;148:1195-204. https://doi.org/10.1053/j.gastro.2014.12.049 10.1053/j.gastro.2014.12.049 [DOI] [PubMed] [Google Scholar]
- 33.Zanini B, Villanacci V, Marullo M, et al. Duodenal histological features in suspected non-celiac gluten sensitivity: new insights into a still undefined condition. Virchows Arch 2018;473:229-34. https://doi.org/10.1007/s00428-018-2346-9 10.1007/s00428-018-2346-9 [DOI] [PubMed] [Google Scholar]
- 34.Dai Y, Zhang Q, Olofson AM, et al. Celiac disease: updates on pathology and differential diagnosis. Adv Anat Pathol 2019;26:292-312. https://doi.org/10.1097/PAP.0000000000000242 10.1097/PAP.0000000000000242 [DOI] [PubMed] [Google Scholar]
- 35.Bjarnason I, Zanelli G, Smith T, et al. Nonsteroidal antiinflammatory drug-induced intestinal inflammation in humans. Gastroenterology 1987;93:480-9. https://doi.org/10.1016/0016-5085(87)90909-7 10.1016/0016-5085(87)90909-7 [DOI] [PubMed] [Google Scholar]
- 36.Gonzalez RS, Salaria SN, Bohannon CD, et al. PD-1 inhibitor gastroenterocolitis: case series and appraisal of “immunomodulatory gastroenterocolitis”. Histopathology 2017;70:558-67. https://doi.org/10.1111/his.13118 10.1111/his.13118 [DOI] [PubMed] [Google Scholar]
- 37.Louie CY, DiMaio MA, Matsukuma KE, et al. Idelalisib-associated Enterocolitis: clinicopathologic features and distinction from other Enterocolitides. Am J Surg Pathol. 2015;39:1653-60. https://doi.org/10.1097/PAS.0000000000000525 10.1097/PAS.0000000000000525 [DOI] [PubMed] [Google Scholar]
- 38.Rubio-Tapia A, Herman ML, Ludvigsson JF, et al. Severe spruelike enteropathy associated with olmesartan. Mayo Clin Proc 2012;87:732-8. https://doi.org/10.1016/j.mayocp.2012.06.003 10.1016/j.mayocp.2012.06.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Ensari A. Gluten-sensitive enteropathy (celiac disease): controversies in diagnosis and classification. Arch Pathol Lab Med 2010;134:826-36. https://doi.org/10.1043/1543-2165-134.6.826 10.1043/1543-2165-134.6.826 [DOI] [PubMed] [Google Scholar]
- 40.Koot BG, ten Kate FJ, Juffrie M, et al. Does Giardia lamblia cause villous atrophy in children? A retrospective cohort study of the histological abnormalities in giardiasis. J Pediatr Gastroenterol Nutr 2009;49:304-8. https://doi.org/10.1097/MPG.0b013e31818de3c4 10.1097/MPG.0b013e31818de3c4 [DOI] [PubMed] [Google Scholar]
- 41.Hanevik K, Wik E, Langeland N, et al. Transient elevation of anti-transglutaminase and anti-endomysium antibodies in Giardia infection. Scand J Gastroenterol 2018;53:809-12. https://doi.org/10.1080/00365521.2018.1481522 10.1080/00365521.2018.1481522 [DOI] [PubMed] [Google Scholar]
- 42.Bianchi A, Chipman DW, Dreskin A, et al. Nutritional folic acid deficiency with megaloblastic changes in the small-bowel epithelium. N Engl J Med 1970;282:859-61. https://doi.org/10.1056/NEJM197004092821510 10.1056/NEJM197004092821510 [DOI] [PubMed] [Google Scholar]
- 43.Maguire AA, Greenson GK, Lauwers GY, et al. Collagenous sprue: a clinicopathologic study of 12 cases. Am J Surg Pathol 2009;33:1440-9. https://doi.org/10.1097/PAS.0b013e3181ae2545 10.1097/PAS.0b013e3181ae2545 [DOI] [PubMed] [Google Scholar]
- 44.Vakiani E, Arguelles-Grande C, Mansukhani MM, et al. Collagenous sprue is not always associated with dismal outcomes: a clinicopathological study of 19 patients. Mod Pathol 2010;23:12-26. https://doi.org/10.1038/modpathol.2009.151 10.1038/modpathol.2009.151 [DOI] [PubMed] [Google Scholar]
- 45.Daniels GA, Lederman HM, Maitra A, et al. Gastrointestinal tract pathology in patients with common variable immunodeficiency (CVID): a clinicopathologic study and review. Am J Surg Pathol 2007;31(12):1800-12. https://doi.org/10.1097/PAS.0b013e3180cab60c 10.1097/PAS.0b013e3180cab60c [DOI] [PubMed] [Google Scholar]
- 46.Malamut G, Verkarre V, Suarez F, et al. The enteropathy associated with common variable immunodeficiency: the delineated frontiers with celiac disease. Am J Gastroenterol 2010;105:2262-75. https://doi.org/10.1038/ajg.2010.214 10.1038/ajg.2010.214 [DOI] [PubMed] [Google Scholar]
- 47.Biagi F, Bianchi PI, Zilli A, et al. The significance of duodenal mucosal atrophy in patients with common variable immunodeficiency: a clinical and histopathologic study. Am J Clin Pathol 2012;138:185-9. https://doi.org/10.1309/AJCPEIILH2C0WFYE 10.1309/AJCPEIILH2C0WFYE [DOI] [PubMed] [Google Scholar]
- 48.Akram S, Murray JA, Pardi DS, et al. Adult autoimmune enteropathy: Mayo Clinic Rochester experience. Clin Gastroenterol Hepatol 2007;5:1282-90. https://doi.org/10.1016/j.cgh.2007.05.013 10.1016/j.cgh.2007.05.013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Masia R, Peyton S, Lauwers GY, et al. Gastrointestinal biopsy findings of autoimmune enteropathy: a review of 25 cases. Am J Surg Pathol 2014;38:1319-29. https://doi.org/10.1097/PAS.0000000000000317 10.1097/PAS.0000000000000317 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Villanacci V, Lougaris V, Ravelli A, et al. Clinical manifestations and gastrointestinal pathology in 40 patients with autoimmune enteropathy. Clin Immunol 2019;207:10-17. https://doi.org/10.1016/j.clim.2019.07.001 10.1016/j.clim.2019.07.001 [DOI] [PubMed] [Google Scholar]
- 51.Schiepatti A, Sanders DS, Aziz I, et al. Clinical phenotype and mortality in patients with idiopathic small bowel villous atrophy: a dual-centre international study. Eur J Gastroenterol Hepatol 2020. Apr 10. Epub ahead of print. https://doi.org/10.1097/MEG.0000000000001726 10.1097/MEG.0000000000001726 [DOI] [PubMed] [Google Scholar]
- 52.Malamut G, Afchain P, Verkarre V, et al. Presentation and long-term follow-up of refractory celiac disease: comparison of type I with type II. Gastroenterology 2009;136:81-90. https://doi.org/10.1053/j.gastro.2008.09.069 10.1053/j.gastro.2008.09.069 [DOI] [PubMed] [Google Scholar]
- 53.Hujoel IA, Murray JA. Refractory celiac disease. Curr Gastroenterol Rep 2020;22:18. https://doi.org/10.1007/s11894-020-0756-8 10.1007/s11894-020-0756-8 [DOI] [PubMed] [Google Scholar]
- 54.Rowinski SA, Christensen E. Epidemiologic and therapeutic aspects of refractory coeliac disease - a systematic review. Dan Med J 2016;63(12). [PubMed] [Google Scholar]
- 55.Eigner W, Bashir K, Primas C, et al. Dynamics of occurrence of refractory coeliac disease and associated complications over 25 years. Aliment Pharmacol Ther 2017;45:364-72. https://doi.org/10.1111/apt.13867 10.1111/apt.13867 [DOI] [PubMed] [Google Scholar]
- 56.Hussein S, Gindin T, Lagana SM, et al. Clonal T cell receptor gene rearrangements in coeliac disease: implications for diagnosing refractory coeliac disease. J Clin Pathol 2018;71:825-31. https://doi.org/10.1136/jclinpath-2018-205023 10.1136/jclinpath-2018-205023 [DOI] [PubMed] [Google Scholar]
- 57.Celli R, Hui P, Triscott H, et al. Clinical insignficance of monoclonal t-cell populations and duodenal intraepithelial t-cell phenotypes in celiac and nonceliac patients. Am J Surg Pathol 2019;43:151-160. https://doi.org/10.1097/PAS.0000000000001172 10.1097/PAS.0000000000001172 [DOI] [PubMed] [Google Scholar]
- 58.Cheminant M, Bruneau J, Malamut G, et al. NKp46 is a diagnostic biomarker and may be a therapeutic target in gastrointestinal T-cell lymphoproliferative diseases: a CELAC study. Gut 2019;68:1396-1405. https://doi.org/10.1136/gutjnl-2018-317371 10.1136/gutjnl-2018-317371 [DOI] [PubMed] [Google Scholar]
- 59.Al-Toma A, Verbeek WH, Hadithi M, et al. Survival in refractory coeliac disease and enteropathy-associated T-cell lymphoma: retrospective evaluation of single-centre experience. Gut 2007;56:1373-8. https://doi.org/10.1136/gut.2006.114512 10.1136/gut.2006.114512 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.West J. Celiac disease and its complications: a time traveller’s perspective. Gastroenterology 2009;136:32-4. https://doi.org/10.1053/j.gastro.2008.11.026 10.1053/j.gastro.2008.11.026 [DOI] [PubMed] [Google Scholar]
- 61.Swerdlow SH, Campo E, Harris NL, et al. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues, revised. 4th ed. Vol. 2. Lyon: IARC; 2017. [Google Scholar]
- 62.Lenti MV, Biagi F, Lucioni M, et al. Two cases of monomorphic epitheliotropic intestinal T-cell lymphoma associated with coeliac disease. Scand J Gastroenterol 2019;54:965-8. https://doi.org/10.1080/00365521.2019.1647455 10.1080/00365521.2019.1647455 [DOI] [PubMed] [Google Scholar]
- 63.Nijeboer P, Malamut G, Mulder CJ, et al. Enteropathy-associated T-cell lymphoma: improving treatment strategies. Dig Dis 2015;33:231-5. https://doi.org/10.1159/000369542 10.1159/000369542 [DOI] [PubMed] [Google Scholar]
- 64.Potter DD, Murray JA, Donohue JH, Burgart LJ, Nagorney DM, van Heerden JA, Plevak MF, Zinsmeister AR, Thibodeau SN. The role of defective mismatch repair in small bowel adenocarcinoma in celiac disease. Cancer Res 2004;64(19):7073-7. [DOI] [PubMed] [Google Scholar]
- 65.Vanoli A, Di Sabatino A, Furlan D, et al. Small bowel carcinomas in coeliac or crohn’s disease: clinico-pathological, molecular, and prognostic features. A Study from the small bowel cancer italian consortium. J Crohns Colitis 2017;11:942-53. https://doi.org/10.1093/ecco-jcc/jjx031 10.1093/ecco-jcc/jjx031 [DOI] [PubMed] [Google Scholar]
- 66.Vanoli A, Di Sabatino A, Martino M, et al. Small bowel carcinomas in celiac or Crohn’s disease: distinctive histophenotypic, molecular and histogenetic patterns. Mod Pathol 2017;30:1453-66. https://doi.org/10.1038/modpathol.2017.40 10.1038/modpathol.2017.40 [DOI] [PubMed] [Google Scholar]
- 67.Giuffrida P, Arpa G, Grillo F, et al. PD-L1 in small bowel adenocarcinoma is associated with etiology and tumor-infiltrating lymphocytes, in addition to microsatellite instability. Mod Pathol 2020. Feb 17. https://doi.org/10.1038/s41379-020-0497-0 10.1038/s41379-020-0497-0 [DOI] [PubMed] [Google Scholar]
- 68.Majumdar K, Sakhuja P, Puri AS, et al. Coeliac disease and the liver: spectrum of liver histology, serology and treatment response at a tertiary referral centre. J Clin Pathol 2018;71:412-9. https://doi.org/10.1136/jclinpath-2017-204647 10.1136/jclinpath-2017-204647 [DOI] [PubMed] [Google Scholar]