
Figure 2.
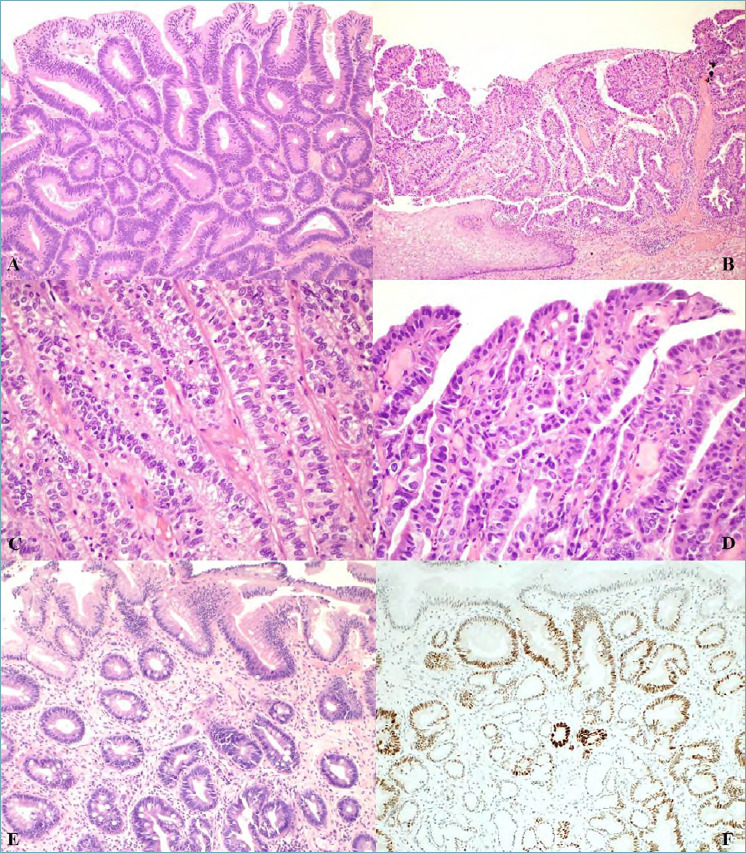
(A) Intestinal type low grade dysplasia in Barrett’s oesophagus showing scanty architectural distortion and mild to moderate cytological atypia; hyperchromatic nuclei with irregular contours, nuclear overlapping and crowding are seen (magnification x20). (B) Intestinal type high grade dysplasia in Barrett’s oesophagus showing both architectural abnormality and severe cytological atypia adjacent to squamous epithelium (magnification x10). (C) Foveolar type low grade dysplasia in Barrett’s oesophagus with closely packed glands with a single layer of columnar cells with no interspersed goblet cells, round/oval basal nuclei with little stratification or pleomorphism and vesicular nuclei (magnification x20). (D) Foveolar type high grade dysplasia with enlarged cells with greater pleomorphism, loss of polarity and increased mitoses (magnification x20). (E) Crypt dysplasia: dysplasia is confined to the crypt with surface epithelium maturation (magnification x20). (F) p53 immunostained section of crypt dysplasia showing p53 nuclear accumulation in the crypt areas of dysplastic epithelium but not in the surface epitheium.