

Abstract
Objective
Flexible fibreoptic intubation is challenging in paediatric patients. Very few studies have compared fibreoptic intubation via oral and nasal routes in children. We hypothesised that the total time to a successful fibreoptic-guided tracheal intubation would be faster through the nasal route when compared to the oral route.
Methods
Sixty children aged 6–12 years were randomised to receive fibreoptic tracheal intubation through oral (group FOI) or nasal route (group FNI). We measured the time to glottic view and total time to successful tracheal intubation. The number of attempts needed, first attempt and overall success rate, external manoeuvres needed to obtain an adequate laryngeal view, subjective assessment of ease of intubation and complications, if any, were also recorded.
Results
The time to glottic view (76.26±.7 s vs. 46.33±16.9 s; p=0.001) and total intubation time (4.55±1.07 min vs. 3.05±0.60 min; p<0.0001) were significantly higher in the FOI group as compared to the FNI group. An overall success rate was 100% in the FNI group and 96.6% in the FOI group. The haemodynamic parameters (mean heart rate and blood pressures) changes were comparable in the two groups at all time intervals. The subjective assessment of ease of intubation was comparable in the two groups (p=0.21). Complications were minor and self-limiting.
Conclusion
Intubation guided by a nasal flexible fibreoptic bronchoscope is easier and faster when compared to oral intubation in children aged 6–12 years with normal airway, and it should be preferred for intubation in children requiring fibreoptic intubation.
Keywords: Anaesthesia general, child, fibreoptic bronchoscopy, glottis, intubation, intratracheal
Introduction
Flexible fibreoptic bronchoscope (FFB)-guided intubation has been considered as the gold standard for the management of difficult airway (DA) cases in both adults and paediatric patients (1–5). The children have an increased incidence of difficult laryngoscopy and are prone to rapid decrease in oxygen saturation due to higher rates of oxygen consumption (5–7). The advantages of FFB for managing DA scenarios include a more extensive range of view within the tracheobronchial tree along with the ability to navigate past any malformations of the airway with a high degree of safety and excellent patient tolerance. So, it is important that all paediatric anaesthesiologists possess the technical expertise in FFB-guided intubation (8, 9).
The technique of performing fibreoptic intubation in children can be a challenging task due to various anatomical and physiological differences as compared to adults (7, 10). Furthermore, intubation with FFB is technically difficult in children due to smaller fiberscopes with a reduced field of vision, decreased range of tip angulation and delicate insertion cord (11).
Despite airway management being an important concern in children, and FFB being an important component of the armamentarium for the management of DA, astoundingly, there are very limited prospective randomised trials on fibreoptic intubation in children with regard to evaluation of the preferred route (oral versus nasal). Also, these two routes have not been compared with regard to time required for intubation, ease of insertion and other complications in children of aged 6–12 years.
We hypothesised that the time to successful fibreoptic-guided tracheal intubation would be faster with the nasal route than the oral route in children aged 6–12 years.
Methods
The study was conducted in a tertiary care hospital in Delhi, after obtaining clearance from the hospital ethics committee (IEC/VMMC/SJH/Thesis/November-2014/424) and written informed consent from parents/legal guardians of the children. Assent was also taken from children >7 years of age.
Sixty elective surgical, ASA Grades 1 and 2 patients of both sexes in the age group 6–12 years weighing >20 kgs requiring endotracheal general anaesthesia were randomly assigned into two equal groups using the sealed envelope technique. Group FOI underwent fibreoptic-guided oral intubation, while group FNI underwent fibreoptic-guided nasal intubation. Patients with anticipated DA, tonsillar/adenoid hyperplasia, congenital airway anomalies, coagulation defects, history of a recent upper respiratory tract infection or those posted for upper airway surgery were excluded from the study.
All the patients underwent a detailed pre-anaesthetic evaluation with relevant investigations and airway examinations. Bilateral nostrils were checked for patency. Standard fasting guidelines were followed. Oral midazolam was administered to all patients 30 minutes prior to the procedure in the dose of 0.05 mg kg−1. An eutectic mixture of local anaesthetic cream was applied to proposed site of intravenous (IV) cannulation 45–60 min prior to the procedure. In the operating room, electrocardiogram (ECG), non-invasive blood pressure and pulse oximetry (SpO2) were attached, and baseline parameters were recorded. The same monitor was used to measure the blood pressure (BP) and heart rate (HR) in both groups. Ventilation was controlled to normocapnia throughout the study period. All the patients were nebulised with 4 mL of 2% lignocaine, and IV glycopyrrolate 0.01 mg kg−1 was administered 15 min prior to the procedure. One drop of xylometazoline 0.05% was instilled in both the nostrils.
Intubation was performed by two anaesthesiologists who had an experience of at least 10 mannequin and 10 paediatric FFB-guided intubations. A PVC Portex cuffed ETT of appropriate size, lubricated with 2% lignocaine gel was loaded over a paediatric FFB (Karl Storz, Tuttlingen, Germany) with a diameter of 3.5 mm. All the FFB-guided intubations were performed under general anaesthesia with preserved spontaneous respiration until the airway was secured.
After preoxygenation, anaesthesia was induced with IV fentanyl 2 μg kg−1 and propofol 2–3 mg kg−1. Following loss of verbal response, the bag-mask ventilation was attempted. If it was deemed difficult, the patient was excluded from further study. Following induction, nasopharyngeal airway of an appropriate size was inserted. The depth of anaesthesia was maintained with 2%–3% sevoflurane in 100% oxygen (titrated to achieve a MAC of 1–1.3) using a closed anaesthesia circuit connected to the nasopharyngeal airway. In the FOI group, the scope was advanced using the Ovasappian airway of appropriate size. The FFB was manoeuvred towards and into the glottis, and once carina was visible, the ETT was advanced over the scope into the glottic opening. In the FNI group, the FFB was advanced through the more patent nostril and manoeuvred to guide the FFB and ETT into the trachea. The successful placement of the ETT was confirmed with the appearance of a regular square waves capnogram. A maximum of two attempts was allowed before declaring the procedure as failure. The total time for intubation comprised of the sum of all individual attempts. The procedure was halted whenever the saturation fell <90% and positive pressure ventilation was instituted using 100% oxygen. In the event of failure, the intubation was achieved with direct laryngoscopy. Following intubation, injection vecuronium 0.01 mg kg−1 was administered for muscle relaxation, and anaesthesia was continued with sevoflurane in oxygen to achieve a MAC of 1. At the end of surgery, neostigmine and glycopyrrolate were administered, and trachea was extubated following return of adequate respiratory efforts and consciousness. We recorded time taken for glottic view (time from the introduction of FFB till first visualisation of the glottis), total intubation time (time from the introduction of FFB into the nasal/oral cavity till the appearance of five capnographic waves), subjective assessment of ease of insertion, graded on a 3-point scale (easy, difficult and impossible) and the number of attempts (an attempt was defined as insertion of the FOB inside the nostril/mouth till its complete withdrawal). Ease of insertion was rated to evaluate subjective difficulty after intubation attempts based on actions necessary during intubation. Intubation was graded as ‘easy’ if straightforward without any need for modification of the usual technique. It was labelled as ‘difficult’ if following initial attempt, external manoeuvres were required to optimise the laryngeal view. ‘Impossible’ intubation implied the inability to secure airway despite use of external manoeuvres. We also noted the first attempt and overall success rate, haemodynamic parameters [heart rate (HR), systolic blood pressure (SBP), diastolic blood pressure (DBP) and mean arterial pressure (MAP)] at baseline, after induction, at the time of glottic view and 1 minute after intubation. Need for external manoeuvres (jaw thrust during the fibreoptic bronchoscopy and tongue traction, neck flexion/extension, optimal external laryngeal manipulation and ETT rotation at the level of glottis during ETT insertion) was also recorded in the two groups. Complications such as intubation failure, desaturation (lowest SPO2 <90%), mucosal bleeding, laryngospasm (clinical evidence of the inability to ventilate during or after procedure) and blood staining of ETT on extubation.
Statistical analysis
A statistical analysis was performed using the IBM Statistical Packages for the Social Sciences software version 20 for Windows (IBM SPSS Corp.; Armonk, NY, USA). Categorical data (the incidence of failed intubations, number of episodes of desaturation, trauma caused and need for external manoeuvres) were compared using the Chi-squared test and Fisher’s exact test. Our primary outcome was the total intubation time. In a previous study evaluating a cohort of paediatric FFB-guided oral intubation cases found the mean (SD) intubation time of 40 s (12). Considering a mean difference of 10 s (considering the FFB-guided nasal intubation will take 25% less time) and standard deviation of 11 s in both the groups, 26 patients were required per group with a power of 90% and an α error of 0.05. We decided to recruit 30 patients in each group to account for failures and dropouts. A p-value >0.05 was used to reject the null hypothesis for the primary outcome.
Results
Eighty patients were assessed for eligibility to be included in the study, out of which 20 were excluded, and 60 were randomised and analysed (Figure 1). The morphometric parameters (age, sex, weight and ASA grading) were comparable in the two groups (Table 1). The time to glottic view (76.26±48.7 s vs. 46.33±16.9 s; p=0.001) and total intubation time (4.55±1.07 min vs. 3.05±0.60 min; p<0.0001) were significantly higher in the FOI group as compared to the FNI group (Table 1, Figure 2 and 3).
Figure 1.

Consort diagram
Table 1.
Patient characteristics and laryngoscopy and intubation parameters in the two groups
| Parameter | Group FOI | FNI | p |
|---|---|---|---|
|
| |||
| Age | |||
| 6–9 years | 17/30 | 17/30 | |
| 10–12 years | 13/30 | 13/30 | 1 |
| Gender (M/F) | 22/8 | 23/7 | 0.76 |
| Weight (kg) | 28.4 (9.2) | 25.47 (4) | 0.115 |
| ASA (I/II) | 30/0 | 30/0 | |
| First-attempt success rate | 86.6% | 96.6% | 0.18 |
| Time to glottic view (s) | |||
| Mean (SD, 95% CI) | 76.3 (48.7,17.45) | 46.33 (16.9,5.59) | |
| Median (IQR) | 60 (30,120) | 40 (30,60) | 0.001 |
| Total intubation time (min) | |||
| Mean (SD, 95% CI) | 4.55 (1.07,0.38) | 3.05 (0.60,0.24) | |
| Median (IQR) | 4.5 (4,5) | 3.05 (3,3.5) | <0.0001 |
FOI: fibreoptic oral intubation; FNI: fibreoptic nasal intubation; M: male; F: female; ASA PS: Americal society of Anaesthesiologists physical status; SD: standard deviation; IQR: interquartile range
Figure 2.

Box-and-whisker plots illustrating time to glottic view (in seconds) with FOI and FNI. The inner horizontal line within the box represents the median time for the glottic view, and the outer horizontal lines of the box represent the 25th and 75th quartiles. The horizontal lines of the whiskers represent the 95% confidence intervals
Figure 3.
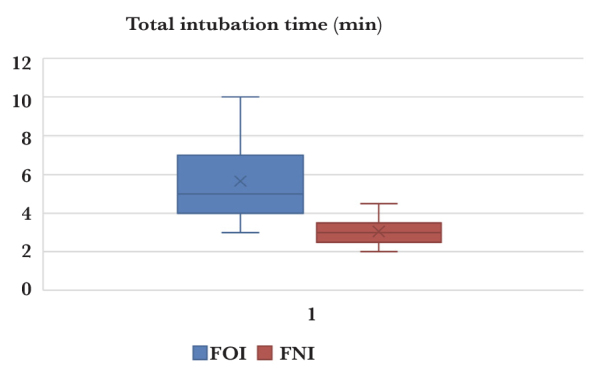
Box-and-whisker plots illustrating total intubation time (in minutes) with FOI and FNI. The inner horizontal line within the box represents the median time for the glottic view, and the outer horizontal lines of the box represent the 25th and 75th quartiles. The horizontal lines of the whiskers represent the 95% confidence intervals
Baseline haemodynamic parameters and oxygen saturation were comparable in the two groups (Figure 4). There was a statistically significant fall in HR, SBP, DBP and MAP in both the groups as compared to baseline at all time intervals. However, the mean HR and blood pressure (SBP, DBP and MAP) changes were comparable in the two groups at all time intervals (Figure 1). The oxygen saturation showed a significant decline as compared to baseline in the FOI group in comparison to the FNI group at the time of intubation (p=0.028) but was comparable at other times. The subjective assessment of ease of intubation was comparable in the two groups (p=0.21) (Table 2). One patient in FNI and 4 patients in FOI were difficult to intubate. One patient in the FOI group was labelled as impossible to intubate. An overall success rate was 100% in the FNI group and 96.6% in the FOI group, while the first-attempt success rate was 96.6% in the FNI group and 86.6% in the FOI group (p=0.18) (Table 2). One patient in the FOI group could not be intubated in two attempts and was considered failure. Need for manoeuvres during the fibreoptic bronchoscopy and ETT insertion were comparable in the two groups (p=0.3 and 0.4) (Table 2). Complications (Table 2) included desaturation in 1 patient from the FOI group and self-limiting mucosal bleeding in 3 patients in the FNI group, and they were comparable in the two groups (p=0.25). No patient developed laryngospasm or airway trauma in either group.
Figure 4.

Haemodynamic parameters (HR and MAP) changes in the two groups
Table 2.
Ease of intubation, complications and use of external manoeuvres
| Parameter | Group FOI | FNI | p |
|---|---|---|---|
|
| |||
| Ease of intubation (1/2/3) | 25/4/1 | 29/1/0 | 0.213 |
| Complications (desaturation/bleeding/laryngospasm/failure) | 1/0/0/1 | 0/3/0/0 | 0.25 |
| Use of external manoeuvre (jaw thrust) during the FFB insertion | 10 | 8 | 0.40 |
| Number of external manoeuvres during the ETT threading (0/1/2/3 or more) | 2/16/6/6 | 15/14/1/0 | 0.30 |
FOI: fibreoptic oral intubation; FNI: fibreoptic nasal intubation; ETT: endotracheal tube
Discussion
The present study documented shorter times to glottic view and total intubation times for FFB-guided nasal route as compared to the oral route for intubation in children aged 6–12 years.
The shorter time in the FNI group can be attributed to the straighter route to larynx via the nasal route. This approach is anatomically favourable as the laryngeal aperture is more easily seen with the fiberscope as it courses past the nasopharynx with less obstruction by the tongue. The results of our study are in concordance with a study by Jagannathan et al. (12) who also compared oral and nasal FFB-guided intubation in children aged <2 years. They had also reported a faster intubation times with the nasal route and concluded that the FFB intubation through the nasal route may be easier for inexperienced clinicians. However, the total intubation times in our study were more than previously reported in all patients, despite a relatively similar glottic view times (13). This suggests that the main difficulty lied in the threading of the ETT because we had used PVC tubes, which are stiffer than soft latex ETT (as reported in previous studies) and were more difficult to railroad over the FFB (12). The difficulty is conceivably greater with the oral route due to more acute angulation. Also, Xue et al. (13) reported the use of muscle relaxant in their study, which would provide better intubation conditions than in a spontaneously breathing child and may have facilitated faster intubation.
In our study, all the intubations were performed by anaesthesiologists who were experienced in adult as well as paediatric FFB-guided intubations. However, the operators in study by Jagannathan et al. (12) (>150 adult and >40 paediatric intubations/operator) were probably more experienced in FFB-guided intubation than our operators (10 mannequin intubations and 10 clinical intubations). It has been shown that the skill in fibreoptic intubation can be learnt after 10 tracheal intubations in anaesthetised patients with normal airways (14). However, the specific learning curve for paediatric FOB has not been documented in literature, and this can be an area suitable for further research.
In a previous randomised trial, Xue et al. (13) investigated the effect of FNI and FOI on haemodynamic responses and demonstrated that there was a significant rise in the HR and arterial pressures during the procedure and following intubation in both groups as compared to baseline. However, in our study, the HR and blood pressures fell from baseline before intubation, which can be attributed to the effect of premedication and induction agents. The lower blood pressures throughout the study period as compared to baseline in our study were probably due to the use of sevoflurane that is known to suppress sympathoadrenal activity and causes milder hemodynamic changes during tracheal intubation along with more stable plasma catecholamine levels as compared to that of isoflurane (15). Xue et al. (13) administered isoflurane to the study subjects, and furthermore, there was a lack of standardisation of depth of anaesthesia in their study, whereas we ensured an adequate depth throughout the study period by maintaining a MAC of 1–1.3. The MAC value at the time of intubation in all the patients.
Moreover, there was no intubation response following intubation probably due to an adequate topicalisation of the airway (nebulisation and lignocaine spray in the oropharynx) prior to FFB-provided adequate blunting of upper airway, glottic and infra-glottic reflexes. Xue et al. (13) had employed only pharyngeal lignocaine sprays, which are unlikely to obtund the glottic and infra-glottic reflexes and thus reported haemodynamic response to intubation, especially following the railroading of the ETT into the trachea.
There was an episode of transient desaturation (SpO2 fell to 85%) in 1 patient in the FOI group. This occurred due to the longer time required for the ETT insertion. Rest of the patients in both the groups had their SpO2 values in the range of 92%–100% during FOI. In a study on fibreoptic nasotracheal intubation in adult patients with normal airways under deep inhalational anaesthesia by Smith et al. (16) 30% of their patients suffered desaturation (SpO2<90%), while it fell to below 80% in 8% (5/60) of their patients. They had concluded that the high incidence of oxygen desaturation in their study was due to unanticipated difficult intubation encountered during the cases that prolonged the intubation period and lead to desaturation. The incidence is lower in our study as patients with a potential DA were excluded from the study.
We had also compared the two techniques for ease of intubation. In FOI group, the procedure was easy in 86.7% patients and difficult in 10%. In 1 patient, the procedure was declared impossible due to ab inability to secure the airway using FFB in two attempts, and intubation was achieved by direct laryngoscopy. In the FNI group, the ETT was successfully inserted in all except 1 patient in first attempt and the procedure was considered easy in 96.6% of patients. One patient in the FNI group required two attempts and was labelled as difficult to intubate, but there were no failures. The increased difficulty with the oral route is due to difficulty in centralising the scope in the mouth and acute angulation at the level of oropharynx during the insertion of FFB and the threading of ETT (17). A similar difficulty in passing an ETT over the orally inserted FFB was reported in a study by Schwartz et al. (18) in 80% of their patients due to the tube impinging over the right arytenoid cartilage. Katsnelson et al. (19) in their mannequin study found that right arytenoid cartilage was the main site which hinders the passage of an ETT over an orally inserted FFB. They also described epiglottis to be the main site which obstructs the passage of an ETT during fibreoptic nasal intubation. They found the same results clinically, when oral and nasal FFB-guided intubations were carried out in patients. The authors speculated that differences in the sites of obstruction in the two routes result from differences in the alignment of oral, pharyngeal and laryngeal axes in the two routes. It has been suggested that during the railroading of the ETT over the fibreoptic scope, its bevel should be oriented upwards for nasal intubation and downwards for oral intubation to facilitate its placement into the trachea because of different sites of obstruction (20). We rotated the ETT during its passage only in cases where resistance was encountered. Jagannathan et al. (12) had appropriately oriented the ETT bevel beforehand in all patients, which may partly account for their shorter intubation times. In our patients, the difficulty in threading the ETT was managed with neck flexion, jaw thrust and ETT rotation at the level of glottis as appropriate.
Airway complications were few and did not result in any sequel. The main problem with nasotracheal fibreoptic intubation is bleeding, which can make intubation difficult (21). While 3 patients of the FNI group experienced intranasal mucosal bleeding which was self-limiting, 1 patient in the FOI group developed transient desaturation during the ETT threading, which was technically difficult and prolonged. The saturation level immediately improved and came back to baseline levels with initiation of 100% oxygen and positive pressure ventilation through the ETT. This is despite the use of para-oxygenation through the nasopharyngeal insufflation of oxygen. None of the patient suffered apnoea or coughing. Intubation conditions using sevoflurane have been reported as good in spontaneously breathing patients without any hypoxemic episodes (22). The optimal anaesthetic depth should be maintained and monitored to avoid apnoea, as well as retching and coughing on the scope in these cases to achieve safe and smooth intubation.
Study limitations
The operators in the present study were experienced in fibreoptic intubations, and the results may thus not be applicable to untrained novices. Furthermore, the nature of the study did not permit us blinding of the allotted group. However, bias was avoided by having an independent assessor record the primary and secondary outcomes. Also, two different operators randomly performed the intubations to avoid subjective bias. Another limitation of the study is that children with normal airways were studied. Hence, the results may not be applicable to those with airway lesions or other airway abnormalities making the airway difficult. Nonetheless, even in these situations, the findings of the study would be relevant in making the decision regarding the appropriate approach to FFB-guided intubation.
Conclusion
Flexible fibreoptic bronchoscope-guided intubation is easier and faster when performed by nasal route as compared to orally acquired intubation in children aged 6–12 years with minimal complications. Hence, nasal fibreoptic intubation may be considered as the preferred technique for intubation in children requiring fibreoptic intubation.
Footnotes
Ethics Committee Approval: Ethics committee approval was received for this study from the ethics committee of VMMC and Safdarjung Hospital (25.11.2014).
Informed Consent: Written informed consent was obtained from parents/legal guardians of the children who participated in this study.
Peer-review: Externally peer-reviewed.
Author Contributions: Concept – K.S., U.G., A.G.; Design – K.S., U.G., A.G.; Supervision – U.G., D.B.; Resources – U.G., D.B.; Materials – U.G., D.B., A.G.; Data Collection and/or Processing – K.S., A.G.; Analysis and/or Interpretation – A.G., U.G., K.S.; Literature Search – A.G., K.S.; Writing Manuscript –A.G., K.S.; Critical Review – A.G., U.G., D.B.
Conflict of Interest: The authors have no conflicts of interest to declare.
Financial Disclosure: The authors declared that this study has received no financial support.
References
- 1.Benumof JL. Management of the difficult adult airway: with special emphasis on tracheal intubation. Anesthesiology. 1991;75:1087–110. doi: 10.1097/00000542-199112000-00021. [DOI] [PubMed] [Google Scholar]
- 2.Hasan MA, Black AE. A new technique for fibreoptic intubation in children. Anaesthesia. 1994;49:1031–3. doi: 10.1111/j.1365-2044.1994.tb04349.x. [DOI] [PubMed] [Google Scholar]
- 3.Okuyama M, Imai M, Fujisawa A, Kemmotsu O. Fiberoptic intubation under general anaesthesia for children with Goldenhar syndrome. Masui. 1994;43:1885–8. [PubMed] [Google Scholar]
- 4.Blanco G, Melman E, Cuairan V, Moyao D, Ortiz-Monasterio F. Fibreoptic nasal intubation in children with anticipated and unanticipated difficult intubation. Pediatric Anesth. 2001;11:49–53. doi: 10.1046/j.1460-9592.2001.00621.x. [DOI] [PubMed] [Google Scholar]
- 5.Sunder RA, Haile DT, Farrell PT, Sharma A. Pediatric airway management: current practices and future directions. Paediatr Anaesth. 2012;22:1008–15. doi: 10.1111/pan.12013. [DOI] [PubMed] [Google Scholar]
- 6.Litman RS, Fiadjoe JE, Stricker PA, Cote CJ. The pediatric airway. In: Cote CJ, Lerman J, Anderson JB, editors. A Practice of Anesthesia for Infants and Children. Philadelphia: Elsevier; 2013. pp. 269–70. [Google Scholar]
- 7.Duggan L, Jagannathan N. Unique airway issues in the pediatric population. In: Hung O, Murphy M, editors. Management of the Difficult and Failed Airway. New York: McGraw-Hill; 2012. [Google Scholar]
- 8.Sims C, vonUngern-Sternberg BS. The normal and the challenging pediatric airway. Paediatr Anaesth. 2012;22:521–6. doi: 10.1111/j.1460-9592.2012.03858.x. [DOI] [PubMed] [Google Scholar]
- 9.Weiss M, Engelhardt T. Proposal for the management of the unexpected difficult pediatric airway. Paediatr Anaesth. 2010;20:454–64. doi: 10.1111/j.1460-9592.2010.03284.x. [DOI] [PubMed] [Google Scholar]
- 10.Roth AG, Wheeler M, Stevenson GW, Hall SC. Comparison of a rigid laryngoscope with the ultrathin fibreoptic laryngoscope for tracheal intubation in infants. Can J Anaesth. 1994;41:1069–73. doi: 10.1007/BF03015656. [DOI] [PubMed] [Google Scholar]
- 11.Wheeler M, Roth AG, Dsida RM, Rae B, Seshadri R, Sullivan CL, et al. Teaching residents pediatric fiberoptic intubation of the trachea: traditional fiberscope with an eyepiece versus a video-assisted technique using a fiberscope with an integrated camera. Anesthesiology. 2004;101:842–6. doi: 10.1097/00000542-200410000-00007. [DOI] [PubMed] [Google Scholar]
- 12.Jagannathan N, Sequera-Ramos L, Sohn L, Huang A, Sawardekar A, Wasson N, et al. Randomized comparison of experts and trainees with nasal and oral fibreoptic intubation in children less than 2yr of age. Br J Anaesth. 2015;114:290–6. doi: 10.1093/bja/aeu370. [DOI] [PubMed] [Google Scholar]
- 13.Xue FS, Li CW, Liu KP, Sun HT, Zhang GH, Xu YC, et al. Circulatory Responses to Fiberoptic Intubation in Anesthetized Children: A Comparison of Oral and Nasal Routes. Anesth Analg. 2007;104:283–8. doi: 10.1213/01.ane.0000253032.09962.e5. [DOI] [PubMed] [Google Scholar]
- 14.Johnson C, Roberts JT. Clinical competence in the performance of fiberoptic laryngoscopy and endotracheal intubation: a study of resident instruction. J Clin Anesth. 1989;1:344–9. doi: 10.1016/0952-8180(89)90073-1. [DOI] [PubMed] [Google Scholar]
- 15.Tomiyasu S, Hara T, Morooka H, Shibata O, Sumikawa K. Hemodynamic and Catecholamine Responses to Tracheal Intubation during Inhalation of Isoflurane or Sevoflurane. Acta Med Nagasaki. 1996;41:76–9. [Google Scholar]
- 16.Smith M, Calder I, Cockard A, Isert P, Nicol ME. Oxygen saturation and cardiovascular changes during fibreoptic intubation under general anaesthesia. Anaesthesia. 1992;47:158–61. doi: 10.1111/j.1365-2044.1992.tb02019.x. [DOI] [PubMed] [Google Scholar]
- 17.Asai T, Shingu K. Difficulty in advancing a tracheal tube over a fibreoptic bronchoscope: incidence, causes and solutions. Br J Anaesth. 2004;92:870–81. doi: 10.1093/bja/aeh136. [DOI] [PubMed] [Google Scholar]
- 18.Schwartz D, Jhonson C, Roberts J. A maneuver to facilitate flexible fibreoptic intubation. Anesthesiology. 1989;71:470–1. doi: 10.1097/00000542-198909000-00038. [DOI] [PubMed] [Google Scholar]
- 19.Katsnelson T, Frost EAM, Farcon E, Goldiner PL. When the endotracheal tube will not pass over the flexible fibreoptic bronchoscope. Anesthesiology. 1992;76:151–2. doi: 10.1097/00000542-199201000-00030. [DOI] [PubMed] [Google Scholar]
- 20.Wheeler M, Dsida RM. UNDO your troubles with the tube: how to improve your success with endotracheal tube passage during fiberoptic intubation. Anesthesiology. 2006;104:378. doi: 10.1097/00000542-200602000-00031. [DOI] [PubMed] [Google Scholar]
- 21.Kim YC, Lee SH, Noh GJ, Cho SY, Yeom JH, Shin WJ, et al. Thermosoftening treatment of the nasotracheal tube before intubation can reduce epistaxis and nasal damage. Anesth Analg. 2000;91:698–701. doi: 10.1213/00000539-200009000-00038. [DOI] [PubMed] [Google Scholar]
- 22.Bonin M, Therre P, Albuisson E, Beaujard H, Barthelemyl I, Mondie JM, et al. Comparison of a propofol target-controlled infusion and inhalational sevoflurane for fibreoptic intubation under spontaneous ventilation. Acta Anaesth Scand. 2007;51:54–9. doi: 10.1111/j.1399-6576.2006.01186.x. [DOI] [PubMed] [Google Scholar]