

Abstract
Background
To prevent low back pain (LBP) from developing into a prolonged disabling condition, clinical guidelines advocate early stage assessment, risk‐screening, and tailored interventions. Occupational health services recommend guideline‐oriented biopsychosocial screening and individualized assessment and management. However, it is not known whether training a limited number of health care professionals improves the management process. The primary objective of this study is to investigate whether training in the biopsychosocial practice model is effective in reducing disability. Furthermore, we aim to evaluate health‐economic impacts of the training intervention in comparison to usual medical care.
Methods
The occupational health service units will be allocated into a training or control arm in a two‐arm cluster randomized controlled design. The training of occupational physiotherapists and physicians will include the assessment of pain‐related psychosocial factors using the STarT Back Tool and the short version of the Örebro Musculoskeletal Pain Screening Questionnaire, the use of an evidence‐based patient education booklet as part of the management of LBP, and tailored individualized management of LBP according to risk stratification. The control units will receive no training. The study population will include patients aged 18–65 with nonspecific LBP. The primary outcome is a patient‐reported Oswestry Disability Index from baseline to 12 months. By estimating group differences over time, we aim to evaluate the effectiveness of the training intervention in comparison to usual medical care, and to undertake an economic evaluation using individual patients' health care records (participant‐level data) and the participating units' registries (cluster‐level data). In addition, through interviews and questionnaires, we will explore the health care professionals' conceptions of the adoption of, the barriers to, and the facilitators of the implementation of the practice model.
Discussion
The evaluation of training in the guideline‐oriented biopsychosocial management of LBP in occupational health services is justified because LBP represents an enormous burden in terms of work disability.
Keywords: biopsychosocial approach, cluster randomized controlled study, implementation research, low back pain, occupational health services, Örebro musculoskeletal pain screening questionnaire, risk stratification, STarT Back tool
1. BACKGROUND
Low back pain (LBP) is a complex condition in which biological, psychological, and social factors impact on both the experience of back pain and its associated disability. 1 According to the Finnish Occupational Health Care Act (1383/2001; http://www.finlex.fi/en/laki/kaannokset/2001/20011383), all employers are obliged to arrange occupational health services (OHS) for their employees. The main objectives of OHS in Finland are to prevent work‐related illnesses and accidents; raise the level of health and safety at work and in the work environment; maintain and improve the health, work ability, and functional capacity of employees at different stages of their working careers; and promote the functioning of the working community. Therefore, work‐related health is prioritized, often meaning that all the primary health care needs of the workers are covered. Routine Finnish OHS care is provided not in the workplaces but externally by public or private organizations. In 2018, the coverage of OHS in Finland was about 90% of employees. 2
Early assessment and tailored interventions seem to promote a more efficient secondary preventive approach to prolonged disabling LBP. 3 , 4 The National Institute for Health and Care Excellence (NICE) guidelines recommend targeted interventions according to LBP risk stratification, such as patient information, group exercise, manual therapy, or a combined physical and psychosocial program. 5 The STarT Back tool (SBT) is a brief questionnaire to identify patients' risk of persistent disabling pain (low, medium, or high risk) in order to match treatments according to the risk subgroup. 6 A randomized controlled trial showed risk‐based stratification using SBT to be cost effective in primary health care. 7 Another questionnaire on the risk evaluation of chronic pain is the Örebro Musculoskeletal Pain Screening Questionnaire (ÖMPSQ). 8 The short version of ÖMPSQ (ÖMPSQ‐short) was developed from the original 25‐item longer version and was shown to be valid in both clinics and research. 9 The ÖMPSQ and ÖMPSQ‐short capture a range of biopsychosocial (BPS) factors that are known predictors of a poor outcome, thus enabling the identification of workers at a higher risk of work disability. 8 , 10 The SBT and ÖMSPQ‐short have been translated into and validated in Finnish. 11 , 12
The Lancet LBP series recommends active treatments that address both physical and psychosocial risk factors and focus on improvement in function among triage patients who do not have serious or specific pathology. 13 Some of its key messages are that LBP should be managed in primary care and that a BPS framework should guide this management. 13 In the context of physiotherapy, psychologically informed physiotherapy seeks to address both the physical and psychological risk factors of people with LBP. 14 , 15 Psychologically informed physiotherapy aims to combine physical therapy practice with cognitive‐behavioral approaches originally developed to treat psychological conditions. 15
In Finland, it is suggested that LBP should be managed according to biomedical findings and pain duration and that psychosocial factors be taken into account as risk factors for prolonged pain within the BPS framework. 16 , 17 However, no tools or methods are provided to support health care professionals (HCPs) in the management of psychosocial problems or to identify early individual risk factors. BPS training interventions for HCPs could potentially help facilitate and improve the delivery of guideline‐orientated care. The primary objective of this two‐arm cluster randomized study is to investigate the effectiveness of a guideline‐oriented BPS training intervention of HCPs, in comparison to usual medical care, in reducing patient‐reported, LBP‐related disability in OHS. The second objective is to undertake an economic evaluation of the training intervention based on patients' health care records and the participating units' registries. The third objective is to explore the training process from the perspective of the HCPs. The study will also explore the adoption and implementation of the guideline‐oriented practice model in the participating OHS units.
2. METHODS/DESIGN
2.1. Study setting and cluster allocation
Units of Finnish major private and public OHS companies will be invited to participate. The units that consent to participate will be randomized by a statistician (J.R.) who is not aware of the characteristics of the units into training or control arms using a random number generator. The first author (J.K.) will then notify the OHS providers of their allocation, but he will not be involved in patient recruitment or data analysis. All the selected training units will attend the same training sessions and start patient recruitment at the same time. Randomization will be stratified by OHS provider type (public companies combined) to minimize selection bias, as described in Figure 1. The number of units interested in participating is 27 (Figure 1, Table 1). Within each OHS unit randomized for training, the employer will select voluntary HCPs (occupational health physiotherapists and physicians) for the training, based on their motivation and willingness to learn more about the BPS approach. The training will be provided free of charge. The aim is that at least one physiotherapist and one physician from each unit will participate. No BPS training or material will be offered to any HCPs of the control units, which will continue to deliver their usual care.
FIGURE 1.
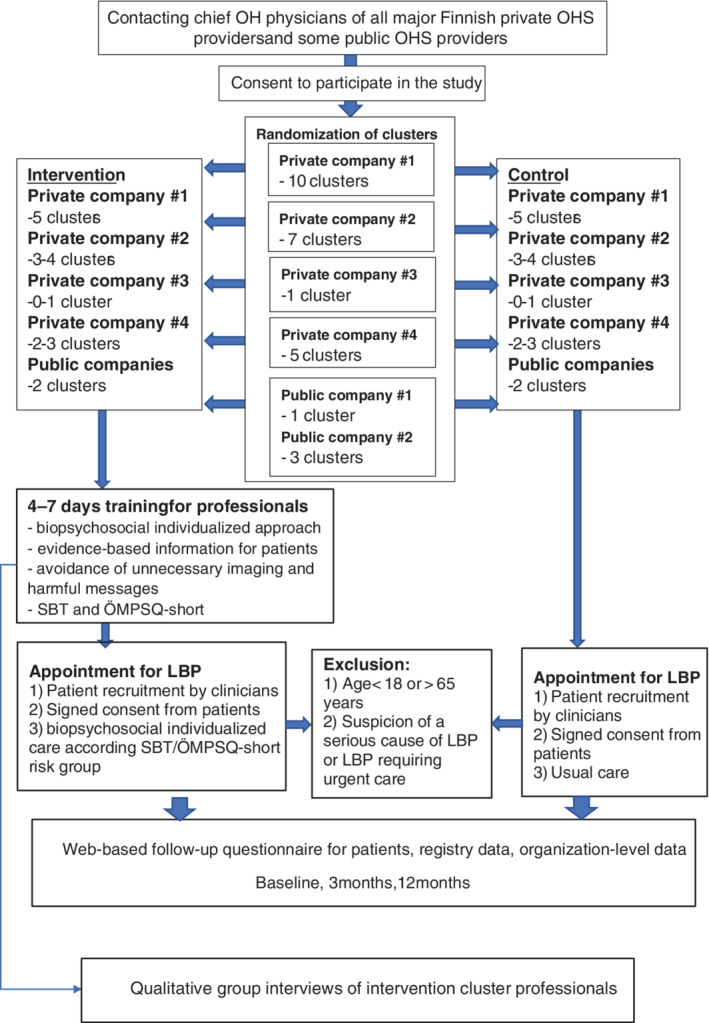
Flowchart of the study. OHS, occupational health services; LBP, low back pain; SBT, STarT Back Tool; ÖMPSQ‐short, short version of the Örebro Musculoskeletal Pain Screening Questionnaire
TABLE 1.
Characteristics of the units of private and public occupational health service (OHS) companies (n = 27) that have indicated interest in participating in the trial (number of occupational health customers, and occupational health physicians, physiotherapists, and psychologists)
| Code of service provider | Running code | Geographical location in Finland | Number of occupational health customers | Number of occupational health physicians | Number of occupational health physiotherapists | Number of OH psychologists |
|---|---|---|---|---|---|---|
| Private company #1 | 1 | Northern | 1000 | 1 | 1 | 0 |
| 2 | Eastern | 1200 | 1 | 2 | 0 | |
| 3 | Northern | 1200 | 1 | 1 | 0 | |
| 4 | Northern | 2400 | 1 | 1 | 0 | |
| 5 | Southern | 3500 | 1 | 1 | 0 | |
| 6 | Western | 6000 | 1 | 2 | 0 | |
| 7 | Northern | 600 | 1 | 1 | 0 | |
| 8 | Northern | 3000 | 1 | 1 | 0 | |
| 9 | Western | 3800 | 1 | 1 | 0 | |
| 10 | Southern | 4200 | 1 | 1 | 0 | |
| Private company #2 | 1 | Southern | 14 400 | 89 | 4 | 7 |
| 2 | Southern | 15 500 | 215 | 5 | 4 | |
| 3 | Eastern | 10 300 | 68 | 4 | 3 | |
| 4 | Western | 3400 | 9 | 2 | 1 | |
| 5 | Eastern | 7200 | 74 | 3 | 2 | |
| 6 | Northern | 13 200 | 16 | 5 | 2 | |
| 7 | Western | 17 400 | 178 | 8 | 6 | |
| Private company #3 | 1 | Northern | 1100 | 1 | 1 | 0 |
| Private company #4 | 1 | Eastern | 13 100 | 9 | 3 | 4 |
| 2 | Southern | 19 900 | 2 | 0 | 0 | |
| 3 | Northern | 33 600 | 49 | 11 | 8 | |
| 4 | Western | 29 400 | 11 | 9 | 2 | |
| 5 | Eastern | 5900 | 7 | 5 | 0 | |
| Public company #1 | 1 | Western | 26 500 | 15 | 10 | 6 |
| Public company #2 | 1 | Northern | 12 500 | 15 | 6 | 3 |
| 2 | Northern | 2300 | 3 | 1 | 1 | |
| 3 | Northern | 9000 | 5 | 3 | 2 |
The study has been approved by the Ethics Committee of the University Hospital of Oulu, Finland (79/2017), and will be conducted in accordance with the Declaration of Helsinki.
2.2. Patient recruitment and eligibility criteria
All occupational health physicians and physiotherapists from the participating training and control units will invite consecutive eligible patients to participate in the study as part of their normal practice. The HCP will identify the eligible patients in their normal appointments and inform them of the study, give them an information sheet, and ask if they are willing to give their consent (Figure 1). Patient consent forms will be posted to the research nurse every 2 weeks from each unit.
All patients aged 18–65 presenting to the involved OHS units with nonspecific LBP with or without radicular pain will be eligible. Exclusion criteria include suspicion of a serious underlying cause of LBP or requirement of urgent care. Participation in the study, including consultations, will not incur direct costs to the patients, as their employers will cover the costs as part of OHS. Patients will not be reimbursed for participation in the study.
3. INTERVENTION
3.1. Professional‐level biopsychosocial training
The training will consist of in‐house workshops and web‐based material for the HCPs designed to enhance adherence to the guideline‐oriented BPS approach for LBP care, to provide evidence‐based information to patients (supported by a patient education booklet), and to avoid unnecessary imaging and harmful messages. An initial 4‐day training course will be delivered by a senior pain psychologist, (Prof. Steven Linton) and a physiotherapist with extensive experience in BPS management of LBP (Kasper Ussing), assisted by other members of the research team (J.K., M.L., R.H., M.P.). The training will comprise a mix of lectures, communications workshops, and live patient demonstrations with a focus on BPS management, followed by a clinical reasoning process. The lectures will focus on developing a BPS understanding of LBP. This includes considering the potential role of emotional, cognitive, and social factors, as well as physical/structural factors. The importance of addressing maladaptive coping strategies, movement, and pain behaviors will also be integrated into the training. The communication workshops will include role‐plays in validating communication, as well as management of patients demanding referral for imaging. The patient demonstrations will target individualized management of complex cases of chronic LBP, in order to demonstrate how the above‐mentioned factors can be addressed in the clinical encounter (Table 2). The training will be delivered mostly in English.
TABLE 2.
Contents of initial 4‐day training
| Duration of training | Trainer | Content |
|---|---|---|
| 4 h 30 min | Steven Linton and Kasper Ussing | Biopsychosocial approach, risk factors for prolonged pain (psychosocial, physical, lifestyle factors) |
| 1 h 45 min | Kasper Ussing | Patient interviews and clinical assessment of behavioral responses to pain |
| 1 h | Steven Linton | Fear‐avoidance, graded activation, and exposure in vivo |
| 1 h | Kasper Ussing | Key management principles of LBP |
| 1 h | Kasper Ussing | Clinical reasoning including triage, management planning |
| 1 h | Jaro Karppinen | Imaging |
| 30 m | Jaro Karppinen | Patient education booklet |
| 1 h | Maija Paukkunen | Work‐related interventions |
| 8 h 45 min | Kasper Ussing | Patient demonstrations and discussions |
| 1 h 45 min | Kasper Ussing | Case studies, discussion |
| 1 h | Kasper Ussing | Q&A, discussions |
| 1 h | Riikka Holopainen and Mikko Lausmaa | Communication skills with practical training |
Abbreviation: LBP, low back pain.
The HCPs will be trained to use SBT systematically and to make individualized care plans for all LBP patients according to their risk profiles. They will be trained to evaluate the BPS factors salient for each LBP patient, which will include training in the use of the ÖMPSQ‐short. The HCPs will be encouraged to provide their patients with an education booklet, which is based on the BPS model and delivers evidence‐based information on the etiology of LBP and appropriate imaging. The booklet has been translated into Finnish and validated. 18 A 3‐day booster session will be held 6–12 months after the initial training. Table 3 shows the contents of the booster training session. The HCPs will also be asked to read related articles and take notes on the barriers to and facilitators of implementation, and to prepare to discuss successful and unsuccessful patient cases between the training sessions.
TABLE 3.
Contents of 3‐day booster training
| Duration of training | Trainer | Content |
|---|---|---|
| 2 h | Kasper Ussing | Q&As after initial training, recap of key principles, obstacles in implementation of biopsychosocial approach encountered by participants |
| 6 h 45 min | Kasper Ussing and Mikko Lausmaa | Patient demonstrations |
| 2 h 45 min | Kasper Ussing | Clinical reasoning, discussions |
| 2 h | Kasper Ussing | Therapeutic alliance, changing negative beliefs |
| 1 h 45 min | Kasper Ussing | Pain behaviors and movement patterns |
| 1 h | Kasper Ussing | Making sense of pain, individualized pain explanation |
| 1 h 15 min | Riikka Holopainen and Mikko Lausmaa | Communication skills, validating communication with practical training |
| 1 h | Jaro Karppinen, Riikka Holopainen, and Mikko Lausmaa | Planning of implementation in each unit |
Approximately 4–6 months after the initial workshop, a second brief (1–2 hours) workshop will be offered at least once to all units to explain the process of the study and the management principles. In addition to the HCPs participating in the initial 4‐day training workshop, those who did not participate in the first workshop will also be invited. Additional training by two experienced physiotherapist researchers (M.L. and R.H.) will be offered to the participating physiotherapists, and all participating HCPs will be assigned a web‐based platform with additional materials (such as articles and videos on the topic) and a discussion forum. We will also deliver a written educational package to support the HCPs who received training, to enable them to share their ideas on the BPS approach and the use of the questionnaires, booklet, and so on, with other HCPs delivering treatment to LBP patients in the participating units who did not participate in the training (occupational health physicians, physiotherapists, and other HCPs such as nurses and psychologists). The participating professionals will be encouraged to teach the principles of the BPS approach to other HCPs within their units.
3.2. Patient‐level intervention
All the LBP patients consenting to participate in the study will be encouraged to accept the new patient education booklet. The booklet Understanding Low Back Pain was developed in Australia and aims to address both clinician and patient barriers to appropriate care, 19 in particular the overuse of imaging. The booklet helps screen patients for possible serious pathology, facilitates patient communication, education, and reassurance (including information on imaging issues), and provides a customized patient management plan. It has been translated into Finnish and undergone preliminarily evaluation in Finnish primary health care. 18
We will encourage the HCPs to classify the patients into low‐, moderate‐, or high‐risk groups during the first OHS visit, based on the SBT. 20 The occupational health physicians will initially plan the individual treatment process. Figure 2 describes the evaluation and treatment process according to risk classification. Low‐risk patients will be given advice on pain medication, if needed, the patient education booklet, and education on the BPS nature of pain and advice on staying active, including work as well as self‐management strategies. Medium‐risk patients will receive similar treatment to those in the low‐risk group. In addition, the physicians will refer the patient to a physiotherapist, who will evaluate and address the patients' specific pain‐related fears and functional limitations. We will encourage active, individualized, and BPS‐oriented physiotherapy management, aiming for gradual functional restoration linked to the patients' goals, reduction of movement‐related fear, and coaching in healthy lifestyle‐behaviors. The patients will typically be allowed to contact the occupational health physiotherapist up to three times for each musculoskeletal condition over 1 year. Some employers may also have contracts that allow further physiotherapy appointments, and the patients involved in this study will be treated according to the content of these contracts.
FIGURE 2.

Infographic of evaluation and treatment process of low back pain patients. LBP, low back pain; OH, occupational health; OHS, occupational health services; PT, physiotherapist
High‐risk patients will receive similar treatment protocol to medium‐risk patients but with an emphasis on exploring and integrating the management of psychosocial factors, and with as short a delay in access to physiotherapy as possible, preferably by a physiotherapist who has participated in the full training (Figure 2). In the case of high‐risk patients, an occupational health psychologist will be consulted if needed. The extent to which the training provided to the HCPs within the unit results in the adoption of the BPS approach by the HCPs treating each patient will be assessed by auditing their notes of the first appointment. We will measure adherence to the intervention and the extent to which therapy was carried out as intended, using self‐reported questionnaires and interviews of health care providers and by reviewing the patient records using a checklist of different components relevant in the BPS approach. We will also measure the quality of delivery and exposure to the intervention from the patient record data at the end of the study. Any possible adverse events will be reported in subsequent publications.
3.3. Control intervention
In the control OHS units, the HCP will not receive BPS training and thus the LBP patients will receive care according to the usual care pathways of the respective unit. The management of patients with LBP in Finnish OHS is typically biomedically focused. Bed rest is avoided, and active exercise is recommended. Physicians typically prescribe pain medication and sick leaves for their patients. They refer patients to physiotherapy on the basis of their own appraisal. 16 Physician appointments for acute or sub‐acute LBP patients mostly last 15–20 minutes, and psychosocial factors are not systematically evaluated. Physiotherapy, in most cases, is not based on risk‐stratification, and physiotherapists are not confident about their skills to treat psychosocial issues. Psychosocial issues are considered more systematically among patients with prolonged pain and work disability. 17 Only physicians (not physiotherapists) are allowed to refer patients for medical imaging. Radiographs are available for all occupational health physicians, while magnetic resonance imaging (MRI) mainly requires a referral from a specialized physician in primary care or a secondary care consultation.
The unit leaders will be contacted to explain the course of the study and the data collection. The participating HCPs will be informed of the study and reminded every 1–2 months about the recruitment of patients.
3.4. Primary outcome measure
The primary outcome will be patient‐reported back‐related disability (Oswestry Disability Index, ODI) over 12 months. 21
3.5. Secondary outcome measures
Patient‐reported pain‐related disability: Roland Morris and PROMIS PF‐20 (Patient‐Reported Outcomes Measurement Information System, a 20‐item physical functioning short form) over 12 months. 22 , 23
Patient reported‐pain intensity: Back and leg pain intensity over 12 months.
Patient‐reported health‐related quality of life: EQ‐5D (EuroQol five dimensions) from baseline to 12‐month follow‐up. 24 , 26
LBP‐related sick leave days: over 12 months.
Direct and indirect costs will be measured over the 12‐month follow‐up period, and will include the following:
Direct costs: Occupational health physician, physiotherapist, nurse, and other health care clinician visits (e.g., psychologist), imaging due to LBP (radiographs/MRI/CT [computer tomography]), pain medication, and spine surgery and other invasive procedure rates from patient records held by the OHS providers.
Indirect costs: LBP‐related sick leave days (also includes short sick leaves) from patient records held by the OHS providers.
Details on prescription medicine reimbursements will be collected from questionnaires administered to the patients. For the costs of visits to publicly provided health care, we intend to use the information that the Finnish Institute for Health and Welfare (THL in Finnish) gathers from Finnish hospitals, available from the Care Register for Health Care (CRHC).
HCPs (physiotherapists and physicians): The beliefs and attitudes toward using the Back Pain Beliefs Questionnaire, Attitudes to Back Pain Scale, and Musculoskeletal Practitioners' Questionnaires, before and after the training. 26
HCPs (physiotherapists, physicians, and nurses): Conceptions concerning the integration of training into practice, including barriers and facilitators to implementation using a qualitative group interview in active units 1 year after the booster training. The facilitators of and barriers to successful implementation and sustainability at the organizational level will be evaluated using a qualitative focus group (OHS developers and clinical champions) interview in active units 3 years after the booster training.
3.6. Sample size
The sample size needed for the trial was calculated according to the primary outcome measure (ODI) at 12 months. With a conservative estimate for the intraclass correlation coefficient of 0.05 and alpha set at 0.05, a total of 162 patients from 27 clusters (units), with an estimate of 6 patients from each, will have 80% power to detect at least a 4‐point difference in ODI (0–50 scale) between the groups, assuming an SD of 8 out of 50 points. 27 This would equate to a 20% difference in groups at 1 year if the mean ODI in the control group was projected to be 20 points. With an expected attrition rate of 30%, the adjusted sample size requirement is thus 192 patients. Toward the end of the recruitment, we will aim to monitor the true intraclass coefficient in our data 28 in order to evaluate the accuracy of the a priori assumption.
3.7. Data collection
The baseline and follow‐up surveys at 3 months and 1 year will use web‐based questionnaires. The research nurse will email the patients (from both the intervention and control units) the baseline questionnaire link after receiving their signed consent. The research nurse will resend the link 3 weeks later if no response is received. Thereafter, in the case of no response, she will re‐send the link twice more. Patient enrolment has ended but data collection is ongoing. The patients' questionnaires include descriptive data and the validated disability and quality‐of‐life questions listed in Table 4.
TABLE 4.
Content of follow‐up questionnaires for patients with low back pain (LBP)
| Domain | Measures | Time point (months) |
|---|---|---|
| Descriptive data | ||
| Age and gender | 0 | |
| Occupation | 0 | |
| Weight and height | 0 | |
| Country of birth | 0 | |
| Pregnancy | 3, 12 | |
| Lifestyle | ||
| Leisure‐time physical activity | 0 | |
| Smoking | 0, 12 | |
| Comorbidity |
Diabetes, rheumatoid arthritis, ankylosing spondylitis, osteoarthritis, depression, fibromyalgia, inflammatory bowel disease, muscle disease |
0 |
|
Stratification questionnaires Back pain |
STarT Back Tool (SBT) Short version of Örebro Musculoskeletal Pain Screening Questionnaire (ÖMPSQ) |
0, 12 0, 12 |
| Previous back pain episode of at least 2 weeks' duration |
0 |
|
| Previous (lifetime) physician consultations related to back pain | 0 | |
| Frequency of LBP during past 3 months | 0, 3, 12 | |
| NRS (Numeral Rating Scale) of LBP intensity during past week | 0, 3, 12 | |
| NRS of back‐related leg pain intensity during past week | 0, 3, 12 | |
| Work status | ||
| Employment/unemployment/pension/student/unpaid work at home/other | 0 | |
| LBP‐related sick leave during past 3 months | 0, 3 | |
| LBP‐related sick leave during past 9 months | 12 | |
| LBP‐related part‐time sick leave during past 3 months | 0, 3 | |
| LBP‐related part‐time sick leave during past 9 months | 12 | |
| Work changes due to LBP | 0, 3, 12 | |
| Use of health care resources | ||
| Physician consultations during past 3 months | 0, 3 | |
| Physician consultations during past year | 12 | |
| Physiotherapist consultations during past 3 months | 0, 3 | |
| Physiotherapist consultations during past year | 12 | |
| Nurse consultations during past 3 months | 0, 3 | |
| Nurse consultations during past year | 12 | |
| Other health care clinician consultation (eg, psychologist, occupational therapist) during past 3 months | 0, 3 | |
| Other health care clinician consultation (eg, psychologist, occupational therapist) during past year | 12 | |
| Imaging due to back pain (X‐ray/magnetic resonance imaging/computed tomography) during past year | 0, 12 | |
| Imaging due to back pain (X‐ray/magnetic resonance imaging/computed tomography) during past 3 months | 3 | |
| Referral for imaging examinations (X‐ray/magnetic resonance imaging/computed tomography) due to back pain | 0, 3, 12 | |
| Medication | Over‐the‐counter pain medication during past week | 0, 3,12 |
| Prescription pain medication (paracetamol/anti‐inflammatory/mild opioid/strong opioid/others) | 0, 3, 12 | |
| Surgery | Spine operation |
12 |
| Patient satisfaction | ||
| With information related to pain explanation | 0, 3, 12 | |
| With self‐efficacy | 0, 3, 12 | |
| With health care provider's skills | 0, 3, 12 | |
| With being heard and understood in terms of symptoms | 0, 3, 12 | |
| Pain‐related disability | ||
| PROMIS PF‐20 (Patient‐Reported Outcomes Measurement Information System, 20‐item physical functioning short form) a | 0, 3, 12 | |
| Oswestry Disability Index b | 0, 3, 12 | |
| Roland Morris Disability Questionnaire c | 0, 12 | |
| Beliefs | ||
| FABQ (Fear Avoidance Beliefs Questionnaire) d | 0, 12 | |
| PSEQ (Pain Self‐Efficacy Questionnaire) e | 0, 12 | |
| BBQ (Back Beliefs Questionnaire) f | 0, 3 | |
| Depressive symptoms | DEPS (Depression Scale) | 0 |
| Work ability | ||
| Current work ability compared with lifetime best (0–10) g | 0, 3, 12 | |
| Work ability in relation to demands of job | 0, 12 | |
| Estimated work impairment due to disease | 0, 12 | |
| Own prognosis of work ability 2 years from now | 0, 12 | |
| Health‐related quality of life | EQ‐5D (EuroQol five dimensions) h | 0, 3, 12 |
Clinician‐level data will be collected using the web‐based questionnaire described in Table 5. The questionnaire will be sent via email after the study information is provided. All physicians and physiotherapists from both the training and control units who have consented to the study will receive the questionnaire to assess their baseline demographic characteristics and beliefs about LBP. Through the group interviews of the training units, we will explore the HCP conceptions of the adoption as well as the barriers to and facilitators of the implementation of the BPS practice model.
TABLE 5.
Clinician‐level data collection from questionnaires at baseline
| Domain | Measures |
|---|---|
| Descriptive data | |
| Gender | |
| Occupation (physician/physiotherapist/nurse/other) | |
| Clinical work experience | |
| OHS unit in which HCP works | |
| Proportion of patients with LBP of all consultations | |
| Attitudes and beliefs | |
| Back Pain Beliefs Questionnaire a | |
| ABS‐mp (Attitudes to Back Pain Scale, for musculoskeletal practitioners) b | |
| Routines and satisfaction | |
| Use of patient education leaflet | |
| Use of risk stratification tool in practice (eg, STarT Back Tool) | |
| Satisfaction with treatment | |
| Level of confidence in their own skills |
Organizational‐level data on health care utilization and imaging due to LBP will be collected retrospectively from the participating intervention and control units with the help of their registry administration and will contain no identifiable patient information (Table 6).
TABLE 6.
Monthly organizational‐level data collection from participating occupational health services (OHS) units from 2016 to 2019
| Domain | Measures |
|---|---|
| Organizational | Number of appointments with occupational health physicians, physiotherapists, nurses, other HCPs according to ICD‐10M40‐M54 diagnoses |
| Lumbar spine imaging examinations (radiographs/magnetic resonance imaging/computed tomography) | |
| Secondary care consultations due to LBP | |
| Number of sick leave episodes and days according to ICD10 M40‐M54 |
Abbreviations: HCP, health care professional; LBP, low back pain.
3.8. Data analysis
We will use an external statistical expert for the data analysis. This analyst will be independent of the study group, that is, he/she will have no involvement in planning the study, recruiting patients, performing the randomization, delivering the intervention, or collecting the data. The expert will also apply the predetermined analysis plan strictly, as outlined in this protocol paper. Baseline characteristics at the unit and patient levels will be summarized using descriptive statistics. The effects of the intervention on primary and secondary outcomes at the patient level will be evaluated by estimating group differences (intervention vs control) over time, using three‐level linear and generalized linear mixed models with random effects for unit and time to allow for intraclass correlation at the unit and patient level, incorporating terms for the intervention group, time and intervention by time interaction, as well as for the variables that show an imbalance between groups at baseline. 34 , 35 Primary analysis will be performed with full intention to treat, using all available data at baseline, 3 months, and 12 months. As linear mixed models are a likelihood‐based estimation procedure, under the assumption of data missing at random, they can take the missing data into account based on the observed data. The estimates will be reported with the accompanying 95% confidence intervals and associated P‐values, using bootstrapped standard errors to account for departures from normality (Stata Version 16, StataCorp LLC, College Station, Texas). We plan to use methods that help gauge the validity of the health‐economic estimates. We will estimate the mean total health care costs using the available information from questionnaires and registry data, calculated as the number of appointments multiplied by estimates of the unit cost per item. The costs of the training will be considered in the analyses. 36 Finally, we will evaluate the need for presenting treatment effects among specific subgroups (according to, e.g., pain duration, radicular symptoms, and SBT risk stratification) in sensitivity analyses.
We will apply a mixed method approach to explore implementation processes and outcomes by triangulating (a) phenomenographic analysis 37 of semistructured group interviews of HCPs from each intervention unit to understand their conceptions of the adoption of the guideline‐oriented BPS model in clinical practice; (b) early phase barriers to and facilitators of the BPS approach by applying the theoretical domains framework 38 in the content analysis of HCPs' interviews and LBP‐related beliefs and attitudes questionnaires; (c) later phase organizational facilitators of and barriers to sustaining the BPS approach by applying the Consolidated Framework of Implementation Research (CFIR) 39 in the content analysis of the semistructured focus group interviews of clinical managers and clinical champions; (d) whether the intervention group more frequently attained goal behaviors for best praxis health care for LBP than the control groups (fewer referrals for imaging examinations, less prescription of pain medication, less consultation of secondary care, less use of spinal surgery, more use patient education leaflet and risk stratification tools).
Participant data will be stored on a secure database in accordance with the General Data Protection Regulations (2018). Personal information will be kept in secured facilities and replaced by ID codes for analyses. Published data from this study cannot be traced to a specific participant. Trial documentation and data will be archived for at least 10 years after completion of the trial.
4. DISCUSSION
Current clinical practice has failed to effectively manage LBP, and disability due to back pain has risen by more than 50% since 1990. 40 All major guidelines on the management of LBP recommend a BPS management approach 13 , 41 over higher risk biomedical approaches, but the translation of research findings into clinical practice is a widely recognized problem. Promising solutions for the rehabilitation of LBP include focused implementation of best practice, the redesign of clinical pathways, integrated health and occupational care, changes to payment systems and legislation, and public health and prevention strategies. 13 We are aware of one cluster randomized controlled trial in which primary care physicians and physiotherapists were trained together to provide cognitive patient education versus usual treatment for patients with LBP. The results did not support the addition of cognitive education to usual treatment. 42 According to a qualitative focus group interview, procedures in the recruitment of both providers and patients seem to be key factors, along with problems in standardization of the intervention. 43
In Finland, OHS plays an important role in the management of LBP among working‐age people. The effectiveness of patient education booklets, 44 , 45 and return‐to‐work interventions 46 have been previously evaluated among patients with LBP in Finnish OHS, but to our knowledge no guideline‐oriented BPS approach for patients with LBP has been widely used in Finnish OHS. We will be able to detect whether the training has led to the successful implementation of the BPS management process within individual units by examining a combination of organizational‐, professional‐, and patient‐level data. For patient‐level data, we will use the recommended outcome measurement instruments.
FUNDING
The study wass funded by the Finnish Work Environment Fund (#117139/2017); the Finnish Institute of Occupational Health; the Rokua Health and Rehabilitation Foundation; the Finnish Cultural Foundation; and the University of Oulu, Oulu, Finland. Bodies of the Finnish Work Environment Fund and the Finnish Institute of Occupational Health peer‐reviewed the study as part of the funding application. The funders did not influence the study design, data collection, data analysis, decision to publish, or preparation of the manuscript.
CONFLICT OF INTEREST
Anna Sofia Simula, Riikka Holopainen, Maija Paukkunen, Kasper Ussing, Mikko Lausmaa, Peter O'Sullivan, Katja Ryynänen, and Jaro Karppinen have received payments for talks or clinical workshops related to a biopsychosocial approach for LBP care from organizations or clinics outside of the current study. Neill Booth, Jouko Remes, Allan Abbott, Birgitta Öberg, Tomi Koski, Anne Smith, Steven J. Linton, and Antti Malmivaara have no competing interests.
AUTHOR CONTRIBUTIONS
Conceptualization: Jaro Karppinen, Neill Booth, Peter O'Sullivan, Antti Malmivaara
Formal Analysis: Jouko Remes, Anne Smith
Funding Acquisition: Jaro Karppinen
Writing ‐ original draft: Jaro Karppinen
Writing ‐ review and editing: Jaro Karppinen, Anna Sofia Simula, Riikka Holopainen, Mikko Lausmaa, Jouko Remes, Maija Paukkunen, Kasper Ussing, Neill Booth, Katja Ryynänen, Tomi Koski, Allan Abbott, Birgitta Öberg, Steven Linton, Anne Smith, Peter O'Sullivan, Antti Malmivaara.
All authors have read and approved the final version of the manuscript.
Jaro Karppinen had full access to all of the data in this study and takes complete responsibility for the integrity of the data and the accuracy of the data analysis.
TRANSPARENCY STATEMENT
This manuscript is an honest, accurate, and transparent account of the study being reported. No important aspects of the study have been omitted. All discrepancies from the study are explained as planned and as registered.
Karppinen J, Simula AS, Holopainen R, et al. Evaluation of training in guideline‐oriented biopsychosocial management of low back pain in occupational health services: Protocol of a cluster randomized trial. Health Sci Rep. 2021;4:e251. 10.1002/hsr2.251
DATA AVAILABILITY STATEMENT
Patient data are not publicly available because this is an ongoing study. The research team is committed to full disclosure of the results of the trial. The results of the trial will be published in peer‐reviewed scientific journals and disseminated through both conventional and social media. Given the multitude of outcome parameters (both quantitative and qualitative), the results will be divided over several papers. The funder will take no role in the analysis or interpretation of trial results.
REFERENCES
- 1. Hartvigsen J, Hancock M, Kongsted A, et al. Underwood M for the lancet low back pain series working group. What is low back pain and why we need to pay attention. Lancet. 2018;391:2356‐2367. [DOI] [PubMed] [Google Scholar]
- 2. Takala E‐P, Leino T, Harjunpää K, et al. Työterveyshuollon toiminta ja laatu Suomessa 2018. Työterveyslaitos. 2019. [Google Scholar]
- 3. Burton AK, Balague F, Cardon G, et al. COST B13 working group on guidelines for prevention in low Back pain. Chapter 2. European guidelines for prevention in low back pain: November 2004. Eur Spine J. 2006;15(suppl 2):S136‐S168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Choi BK, Verbeek JH, Tam WW, Jiang JY. Exercises for prevention of recurrences of low‐back pain. Cochrane Database Syst Rev. 2010;1:CD006555. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Bernstein IA, Malik Q, Carville S, Ward S. Low back pain and sciatica: summary of NICE guidance. BMJ. 2017;356:i6748. [DOI] [PubMed] [Google Scholar]
- 6. Hill JC, Dunn KM, Lewis M, et al. A primary care back pain screening tool: identifying patient subgroups for initial treatment. Arthritis Rheum. 2008;59:632‐641. [DOI] [PubMed] [Google Scholar]
- 7. Hill JC, Whitehurst DG, Lewis M, et al. Comparison of stratified primary care management for low Back pain with current best practice (STarT Back): a randomised controlled trial. Lancet. 2011;378:1560‐1571. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Linton SJ, Boersma K, Clin J. Early identification of patients at risk of developing a persistent back problem: the predictive validity of the Örebro musculoskeletal pain questionnaire. Pain. 2003;19:80‐86. [DOI] [PubMed] [Google Scholar]
- 9. Linton S, Nicholas M, MacDonald S. Development of a short form of the Orebro musculoskeletal pain screening questionnaire. Spine (Phila Pa. 1976). 2011;36:1891‐1895. [DOI] [PubMed] [Google Scholar]
- 10. Karran EL, McAuley JH, Traeger AC, et al. Can screening instruments accurately determine poor outcome risk in adults with recent onset low back pain? A systematic review and meta‐analysis. BMC Med. 2017;15(1):13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Piironen S, Paananen M, Haapea M, et al. Transcultural adaption and psychometric properties of the STarT back screening tool among Finnish low back pain patients. Eur Spine J. 2016;25:287‐295. [DOI] [PubMed] [Google Scholar]
- 12. Ruokolainen O, Haapea M, Linton SJ, et al. Construct validity and reliability of Finnish version of Örebro musculoskeletal pain screening questionnaire. Scand J Pain. 2016;13:148‐153. [DOI] [PubMed] [Google Scholar]
- 13. Foster NE, Anema JR, Cherkin D, et al. Prevention and treatment of low back pain: evidence, challenges, and promising directions. Lancet. 2018;391:2368‐2383. [DOI] [PubMed] [Google Scholar]
- 14. Borrell‐Carrió F, Suchman AL, Epstein RM. The biopsychosocial model 25 years later: principles, practice, and scientific inquiry. Ann Fam Med. 2004;2:576‐582. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Main CJ, George SZ. Psychologically informed practice for management of low back pain: future directions in practice and research. Phys Ther. 2011;91:820‐824. [DOI] [PubMed] [Google Scholar]
- 16. Low Back Pain Current Care Guidelines . Working Group Set up by the Finnish Medical Society Duodecim and the Finnish Cardiac Society. Helsinki: The Finnish Medical Society Duodecim; 2017. https://www.kaypahoito.fi. [Google Scholar]
- 17. Recommendation by the Council for Choices in Health Care in Finland (COHERE Finland) . Biopsychosocial rehabilitation in prolonged or recurrent back pain. Recommendation 1.11.2018. Choices in health care; 2020. https://palveluvalikoima.fi/en/recommendations
- 18. Simula A‐S, Jenkins HJ, Holopainen R, et al. Transcultural adaption and preliminary evaluation of “understanding low back pain” patient education booklet. BMC Health Serv Res. 2019;19:1010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Jenkins HJ, Moloney NA, French SD, et al. Using behaviour change theory and preliminary testing to develop an implementation intervention to reduce imaging for low back pain. BMC Health Serv Res. 2018;18:734. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Simula A‐S, Ruokolainen O, Oura P, et al. Association of STarT Back tool and the short form of the Örebro musculoskeletal pain screening questionnaire with multidimensional risk factors. Sci Rep‐UK. 2020;10:290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Fairbank JC, Pynsent PB. The Oswestry index. Spine (Phila Pa 1976). 2000;25:2940‐2952. [DOI] [PubMed] [Google Scholar]
- 22. Rose M, Bjorner JB, Becker J, Fries JF, Ware JE. Evaluation of a preliminary physical function item bank supports the expected advantages of the patient‐reported outcomes measurement information system (PROMIS). J Clin Epidemiol. 2008;61:17‐33. [DOI] [PubMed] [Google Scholar]
- 23. Rose M, Bjorner JB, Gandek B, Bruce B, Fries JF, Ware JE Jr. The PROMIS physical function item bank was calibrated to a standardized metric and shown to improve measurement efficiency. J Clin Epidemiol. 2014;67:516‐526. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Rabin R, Gudex C, Selai C, Herdman M. From translation to version management: a history and review of methods for the cultural adaptation of the EuroQol five‐dimensional questionnaire. Value Health. 2014;17:70‐76. [DOI] [PubMed] [Google Scholar]
- 25. Brazier J, Jones N, Kind P. Testing the validity of the Euroqol and comparing it with the SF‐36 health survey questionnaire. Qual Life Res. 1993;2:169‐180. [DOI] [PubMed] [Google Scholar]
- 26. Georg J, Mackinnon A, Kong DC, Stewart K. Development and validation of the beliefs and behaviour questionnaire (BBQ). Patient Educ Couns. 2006;64:50‐60. [DOI] [PubMed] [Google Scholar]
- 27. Vibe Fersum K, O'Sullivan P, Skouen JS, Smith A, Kvåle A. Efficacy of classification‐based cognitive functional therapy in patients with non‐specific chronic low back pain: a randomized controlled trial. Eur J Pain. 2013;17:916‐928. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. van Breukelen GJ, Candel MJ. Calculating sample sizes for cluster randomized trials: we can keep it simple and efficient! Clin Epidemiol. 2012;65:1212‐1218. [DOI] [PubMed] [Google Scholar]
- 29. Roland MO, Morris RW. A study of the natural history of back pain. Part 1: Development of a reliable and sensitive measure of disability in low back pain. Spine. 1983;8:141‐4. [DOI] [PubMed] [Google Scholar]
- 30. Waddell G, Newton M, Henderson I, Somerville D, Main CJ. A Fear‐Avoidance Beliefs Questionnaire (FABQ) and the role of fear‐avoidance beliefs in chronic low back pain and disability. Pain. 1993;52:157–68. [DOI] [PubMed]
- 31. Nicholas MK. The pain self‐efficacy questionnaire: Taking pain into account. Eur J Pain. 2007;11:153‐63. [DOI] [PubMed]
- 32. Ilmarinen J, Tuomi K. Work ability of aging workers. Scand J Work Environ Health. 1992;18(Suppl 2):8‐10. [PubMed] [Google Scholar]
- 33. Pincus T, Vogel S, Santos R, Breen A, Foster N, Underwood M. The attitudes to back pain scale in musculoskeletal practitioners (ABS‐mp): the development and testing of a new questionnaire. Clin J Pain. 2006;22:378‐86. [DOI] [PubMed] [Google Scholar]
- 34. Vickers AJ, Altman DG. Analysing controlled trials with baseline and follow up measurements. BMJ. 2001;323:1123‐1124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Campbell MK, Piaggio G, Elbourne DR, Altman DG, CONSORT Group . Consort 2010 statement: extension to cluster randomised trials. BMJ. 2012;345:e5661. [DOI] [PubMed] [Google Scholar]
- 36. Ramsey SD, Willke RJ, Glick H, et al. Cost‐effectiveness analysis alongside clinical trials II – an ISPOR good research practices task force report. Value Health. 2015;18:161‐172. [DOI] [PubMed] [Google Scholar]
- 37. Åkerlind G. Variation and commonality in phenomenographic research methods. Higher Educ Res Dev. 2005;24:321‐334. [Google Scholar]
- 38. Atkins L, Francis J, Islam R, et al. A guide to using the theoretical domains framework of behavior change to investigate implementation problems. Implement Sci. 2017;12:77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci. 2009;4:50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Buchbinder R, van Tulder M, Öberg B, et al. Low back pain: a call for action. Lancet. 2018;391:2384‐2388. [DOI] [PubMed] [Google Scholar]
- 41. Koes B, van Tulder M, Lin CW, Macedo LG, McAuley J, Maher C. An updated overview of clinical guidelines for the management of nonspecific low back pain in primary care. Eur Spine J. 2010;19:2075‐2094. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Werner EL, Storheim K, Løchting I, Wisløff T, Grotle M. Cognitive patient education for low back pain in primary care: a cluster randomized controlled trial and cost‐effectiveness analysis. Spine (Phila Pa 1976). 2016;41:455‐462. [DOI] [PubMed] [Google Scholar]
- 43. Werner EL, Løchting I, Storheim K, Grotle M. A focus group study to understand biases and confounders in a cluster randomized controlled trial on low back pain in primary care in Norway. BMC Fam Pract. 2018;19:71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Rantonen J, Vehtari A, Karppinen J, et al. Face‐to‐face information in addition to a booklet versus a booklet alone for treating mild low‐back pain: a randomized controlled trial. Scand J Work Environ Health. 2014;40:156‐166. [DOI] [PubMed] [Google Scholar]
- 45. Rantonen J, Karppinen J, Vehtari A, et al. Cost‐effectiveness of providing patients with information on managing mild low‐back symptoms. A controlled trial in an occupational health setting. BMC Public Health. 2016;16:316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Viikari‐Juntura E, Kausto J, Shiri R, et al. Return to work after early part‐time sick leave due to musculoskeletal disorders: a randomized controlled trial. Scand J Work Environ Health. 2012;38:134‐143. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Patient data are not publicly available because this is an ongoing study. The research team is committed to full disclosure of the results of the trial. The results of the trial will be published in peer‐reviewed scientific journals and disseminated through both conventional and social media. Given the multitude of outcome parameters (both quantitative and qualitative), the results will be divided over several papers. The funder will take no role in the analysis or interpretation of trial results.