

Abstract
Objectives.
To examine the association between individual, neighborhood, and school-level influences on individual screen time among adolescents and young adults (AYAs) in the National Longitudinal Study of Adolescent to Adult Health.
Methods.
We classified screen time continuously as self-reported total hours per week of television, videos, and video/computer games at baseline and categorical as extended screen time (≥ 14 hours per week). We fit cross-classified multilevel models (CCMM) and examined the individual-, school- and neighborhood-level demographic and socioeconomic factors associated with screen time. Models were fit using MLwiN with Bayesian estimation procedures.
Results.
AYAs reported an average of 22.8 (SD=19.4) and 21.9 (SD=20.3) hours of screen time, respectively. At the individual level, younger age, male sex, Black/multiracial race, receipt of public assistance, and lower parental education were associated with higher screen time. At the school level, being out of session (i.e., school and national holidays including summer), having a higher proportion of non-White students, and having a lower proportion of parents with a college education were associated with higher individual screen time.
Conclusions.
We found that individual-level factors most influence youth screen time, with smaller contributions from school factors.
Introduction
Over the past few decades, there has been a drastic increase in the engagement of sedentary activities among adolescents ages 10–24 years1, in particular through increased screen time during discretionary periods of the day such as watching television and playing computer games while sitting, reclining, or lying.2 This increase has paralleled the rising rates of obesity and is a critical factor underlying the obesity epidemic.3 In fact, studies of both children and adults show that greater time spent in discretionary (e.g., watching television) and nondiscretionary sedentary activities (e.g., completing homework) is associated with an increased risk of obesity and chronic disease outcomes.4–7 Sedentary behaviors involve little movement and, therefore, result in low levels of energy expenditure [1.0–1.5 metabolic equivalent units].8,9 Sedentary behaviors, which can be done in a variety of postures, including reclining/lying, sitting, and standing, are increasingly acknowledged as distinct from a lack of physical activity.10 For instance, an adolescent who runs track for 60 minutes daily, but also sits at school 8 hours per day is considered both physically active and sedentary.10 Moreover, there is no “gold standard” for sedentary behavior assessment; self-reported measures provide information on the behavioral context that is not available from objective measures.11 Prevalence of sedentary behavior differs depending on the assessment tool;11 however, it is estimated that adolescents in the U.S. ages 6–19 spend approximately 6 to 8 hours per day in sedentary behavior, including general sitting and screen time (e.g., television viewing and computer use).12
Among adolescents, screen time while sitting, reclining, or lying is an important contributor to sedentary behavior, but can also be modified as targets for public health. Moreover, recent studies indicate that youth, on average, spend up to 3 or more hours daily watching television, and may engage in 5.5 to 8.5 hours of sedentary activities every day outside of school.13 These findings are of special concern, because adolescence is a critical period for developing health habits that may continue into adulthood,14 and such high levels of sedentary behavior have stimulated efforts to reduce adolescents’ sedentary time.
Greater screen time is significantly associated with poorer physical and mental health outcomes.15,16 In terms of physical health effects, excessive screen time is associated with risk factors for cardiovascular disease such as obesity, high blood pressure, insulin resistance, and dyslipidemia.16 Other physical health consequences include poor sleep and impaired vision. Mental health effects of excessive screen time include depressive symptoms, internalizing and externalizing behavior, and inattention.15,16
Data conflict with each other as to whether there are differences in time spent in sedentary behavior by socioeconomic status, sex, or race/ethnicity.4,17,18 The available evidence from prospective and cross-sectional studies suggest that sedentary behavior differs between boys and girls3,19 and may increase5,20,21 or decrease22 during adolescence. Although findings are mixed, there appears to be more support for an increase in sedentary behavior as youth age.3 Studies also indicate that there are children who maintain high levels of sedentary behavior during adolescence,5 and there are those who engage in low amounts of sedentary activities (< 2 hours/day of screen time).23,24 Prior studies examining screen time specifically in adolescence have found that boys compared to girls,25 Black compared to White race,26,27 and lower-income versus higher-income households28 report more screen time.
Population-level studies indicate that, on average, utilizing geographic and contextual indicators may be a more robust, realistic indicator of health outcomes at multiple levels and predictions than individual-level indicators alone, and that projections from these predictions can inform policy and target interventions at the level that will have the most significant impact. Prior studies have examined school contexts or neighborhood contexts and their relation to adolescent screen time; however, there is a paucity of research examining both school and neighborhood factors and weighing their relative importance. At the school level, the availability of extracurricular activities (such as sports), students’ perceptions of fair teachers, and feeling safe at school were found to be associated with lower levels of screen time.29,30 At the neighborhood level, access to outdoor activities, favorable perceived aesthetics, and low social neighborhood disorder were associated with lower levels of screen time.30–32 However, these studies did not account for both school and neighborhood factors related to screen time. Understanding the social determinants of adolescent health and how these may affect later adult health is a priority in the field of adolescent health.33,34 The latest adaptation of the conceptual model on adolescent health defines adolescent health at three levels: current health problems of AYAs; health risks for health problems in AYA, adulthood, or the next generation; and social determinants of health among AYAs.33,34
This study fills an important gap in the literature and extends previous findings by examining the individual, school, and neighborhood contributions to screen time in adolescence (and if these adolescent contributions persist into young adulthood as an exploratory aim) using a large representative sample of US adolescents from the National Longitudinal Study of Adolescent to Adult Health (Add Health). Understanding the relative influence of these factors can help inform the development of targeted interventions to reduce screen time among youth. Our approach drills down beyond individual-level screen time which may mask true overarching interacting mechanisms of school and neighborhood influences on screen time. Specifically, this study used cross-classified multilevel models (CCMM) in disentangling the role of two critical influences on adolescent screen time: schools and neighborhoods.
Methods
Data and Study Design
We used data from the National Longitudinal Study of Adolescent to Adult Health (Add Health), a nationally representative cohort of youth in the U.S. that has been followed from adolescence through adulthood to identify social, behavioral, and biological determinants of health across the life course.35 Further details about the Add Health study design, coordinated by the Carolina Population Center, can be found elsewhere.35 The University of North Carolina Institutional Review Board approved all Add Health study procedures. This secondary analysis was conducted using deidentified data obtained under an Add Health Restricted-Use Data Contract at the University of California, San Francisco.
Participants
A total of 20,745 adolescents in grades 7–12 (aged 11–21 years) participated in Wave I (1994–1995). Follow-up of participants occurred in 1996 (Wave II), from 2001–2002 (Wave III), and from 2007–2009 (Wave IV) when participants were aged 12–22, 18–26, and 24–32 years, respectively. Between 71% and 76% of the baseline cohort completed study interviews at each follow-up assessment. A total of 80.3% (N=15,701) of adolescents from Wave I provided information in Wave IV, and further details of the Wave I-IV study designs are provided elsewhere.36 Due to exclusions clarified below, our final analytic sample consisted of 18,642 participants in Wave I and 4,195 participants in Wave IV.
Screen Time
Described in detail elsewhere, Add Health surveys employed a standard activity recall.35 The screen time measure included self-reported total hours per week of television, videos, and video/computer games at baseline (Wave I) and have been published previously.37–40 The self-reported hours per week of television watching question has demonstrated moderate test-test reliability and was negatively associated with moderate-to-vigorous intensity physical activity as measured by an accelerometer.41 For this analysis, we measured screen time in two ways: continuously as hours per week and categorical as less than or equal to 14 hours per week (this threshold denotes recommendations of 2 or less hours of screen time per day).42 Additionally, in order to support the validity of our linear regression estimates provided below, we have carefully examined the distribution screen time in our analytic sample and found that is normally distributed.
Covariates
SES was obtained at the individual, school, and neighborhood level. At the individual-level, SES was determined based on parental education and receipt of public assistance. We used socioeconomic data from the caregiver interview to capture receipt of public assistance (1=mother currently receiving public assistance, such as welfare; 0=not) and highest level of parental education (or the youth interview if the caregiver did not provide this information). We preferentially used caregivers’ responses when available because they were more likely to be accurate regarding the household’s economic status and educational background. At the school-level, we created a continuous measure of school-level SES by aggregating individual-level data. Use of individual-level data was required as information about school-level SES was not directly available. To be consistent with tract-level sociodemographic from the census, we calculated the proportion of students within each school whose mother had received public assistance, the percent of students with at least one parent with a college degree, and the percent of students who self-reported as White. At the neighborhood level, we used data from the 1990 Census to create a neighborhood-level SES measure indicating the proportion of residents within each neighborhood who had received public assistance or had a college degree. Adjusted models included the following individual-level covariates: age (continuous), sex (male=0; female=1), and self-reported race/ethnicity (1=non-Hispanic White; 2=non-Hispanic Black; 3=Asian; 4=Hispanic; 5=Other; 6=Multiracial). We also adjusted for the percentage of students in either the school or the neighborhood who were White.
Measures of SES (parent education and receipt of public assistance) were derived from caregiver interviews when available and youth interviews only if the parent did not provide information. We preferentially used caregivers’ responses when they were available because they were more likely to be accurate regarding the household’s economic status and educational background. Our final analytic sample, 87% of respondents had information on public assistance from the caregiver interview while 13% was from the youth interview due to no caregiver information. Similarly, parental education was available from the caregiver interview for 87% of respondents and 13% came from the youth interview. This is similar to the entire Wave 1 Add Health sample, of which 85% of participants had a caregiver participate.36
Statistical Analysis
We performed a series of regression models to examine 1) the between-level variation (random effects) in adolescent screen time as well as 2) the individual-, school- and neighborhood-level demographic and SES factors associated with adolescent screen time. Adolescent screen time at Wave I was modeled continuously using linear regression and extended screen time using logistic regression. Models were fit using MLwiN (version 3.00; Birmingham, UK) via STATA’s runmlwin command. MLwiN uses Bayesian estimation procedures using Markov Chain Monte Carlo (MCMC) methods with non-informative priors and a Metropolis-Hastings sampling algorithm, allowing for the simultaneous modeling of non-hierarchically nested contexts.43–46
To parse out the effects of individual-, neighborhood-, and school-level contributions on screen time, we ran linear regression models with model-building proceeding in a number of steps. We first examined the independent contributions of neighborhood and school contexts on the outcome using two-level hierarchical null (or unconditional) models. These models were fit by including individuals nested within either the school- or neighborhood-level. Next, school and neighborhood contexts were examined simultaneously by allowing for cross-classification of the two contexts. Subsequent models incorporated this cross-classification of school and neighborhood and the adjustment for other predictors via the following model equation. Continuous screen time outcome (denoted y) for an adolescent in the study (denoted i) nested in a given school (denoted j) and neighborhood (denoted k) was modeled as:
with the following fixed effect parameters: β0 refers to the overall mean screen time y across all schools and neighborhoods, βxi refers to the vector of individual-level covariates, βxij refers to the vector of school-level covariates, and βxik refers to the vector of neighborhood-level covariates. Random effect parameters included the following: e0i(jk) refers to the individual-level random effect variance parameter for the adolescent within the combination of school j and neighborhood k, where u0j is the variance at the school-level and u0k is the variance at the neighborhood-level.
A series of four adjusted cross-classified models were fitted. Model 1 adjusted for individual-level predictors including age, gender, race/ethnicity, parental education, parental receipt of public assistance, and school being currently in session at the time of interview. Model 2 included individual-level predictors as well as the following school-level predictors: percentage of students of White race, percentage of students whose parents receive public assistance, and percentage of students whose parents have a college degree. Model 3 included individual predictors plus neighborhood-level predictors from the Census using Census tracts: percentage of residents who are of White race, percentage of residents receiving public assistance, and percentage of residents with a college degree. Model 4 presents the fully-adjusted model, which included all individual-, school-, and neighborhood-level predictors.
For linear regression models predicting continuous screen time we report parameter estimates (β) and 95% credible intervals (CI) for fixed effects, in which parameter estimates (95% CI) for intercepts while variance estimates (95% CI) and intra-class correlations (ICC) are reported for random effects. ICCs allow for comparison of variance parameters across contextual levels and are interpreted as the percent of variance attributable to a given level. For logistic models predicting extended screen time (≥14 hours), we present odds ratios (OR) and 95% credible intervals for fixed effects, parameter estimates (95% CI) for intercepts, and variance estimates (95% CI) and ICC for random effects.47 Predictors at the school- or neighborhood-level were calculated as the effect on screen time for a 10% change in the predictor. We evaluated model fit using the Deviance Information Criterion (DIC) which refers to the model complexity and “badness of fit” with higher DIC values indicate a poorer fitting model.45
Results
A total of 18,642 adolescents were included in Wave I from 128 schools and 2,285 neighborhoods. At Wave IV, 14,195 young adults participated in the survey. Table 1 presents descriptive statistics on individuals in the total sample at baseline in Wave 1 and at follow-up in Wave IV. Average age in adolescence (Wave I) was 15.6 years (SD=1.7) and 29.0 years (SD=1.7) in young adulthood (Wave IV).48 In adolescence, 59% reported more than 14 hours of screen time per week, with an average of 22.8 hours per week (SD=20.3). Average screen time in young adulthood was 21.9 hours per week (SD=19.4). Parent SES was relatively high, as only 9.5% of adolescents’ parents were currently receiving public assistance and only 13% had less than a high school education.
Table 1.
Descriptive Characteristics of Participants in adolescence at Wave I (1994–1995; N=18,642) and young adulthood at Wave IV (2007–2009; N=14,195) of the National Longitudinal Study of Adolescent to Adult Health.
| Participant Characteristic | Wave I | Wave IV |
|---|---|---|
| N (%) | ||
| Individual-Level | (N=18,642) | (N=14,195) |
| Age (years), mean (SD) | 15.6 (1.7) | 29.0 (1.7) |
| Gender | ||
| Male | 9,264 (49.7) | 6,672 (47.0) |
| Female | 9,378 (50.3) | 4,523 (53.0) |
| Race/Ethnicity | ||
| White | 9,436 (50.6) | 7,513 (52.9) |
| Black | 3,853 (20.7) | 2,905 (20.5) |
| Asian | 1,189 (6.4) | 788 (5.6) |
| Hispanic | 3,118 (16.7) | 2,229 (15.7) |
| Other | 268 (1.4) | 179 (1.3) |
| Multiracial | 778 (4.1) | 581 (4.1) |
| Parental Education (Wave I) | ||
| Less than high school | 2,378 (12.7) | 1,697 (12.0) |
| High school graduate / GED | 4,875 (26.1) | 3,687 (26.0) |
| Some college | 5,474 (29.3) | 4,227 (29.8) |
| College graduate or beyond | 5,915 (31.7) | 4,584 (32.3) |
| Parent Receipt of Public Assistance (Wave I) | ||
| No | 16,860 (90.4) | 12,939 (91.2) |
| Yes | 1,782 (9.5) | 1,256 (8.9) |
| School currently in session during interview | ||
| No | 11,570 (62.1) | N/A |
| Yes | 7,072 (37.9) | N/A |
| Screen Time (Hours per week), mean (SD) | 22.8 (20.3) | 21.9 (19.4) |
| Screen Time | ||
| <14 hours per week | 7,632 (40.9) | 5,740 (40.4) |
| ≥14 hours per week | 11,010 (59.1) | 8,455 (59.6) |
| Mean (SD) |
||
| School-Level | (N=128 schools) | (N=128 schools) |
| School Size | 145.6 (160.9) | 110.9 (119.2) |
| Percent White Race | 47.5 (25.5) | 47.5 (25.5) |
| Percent on Public Assistance | 10.4 (9.4) | 10.4 (9.4) |
| Percent Parent with College Degree | 31.7 (16.9) | 31.7 (16.9) |
| Neighborhood-Level (Census Tract) | (N=2,285 neighborhoods) | (N=1,940 neighborhoods) |
| Neighborhood Size, mean (SD) | 8.15 (20.4) | 7.32 (17.2) |
| Percent White Race | 66.3 (33.0) | 66.8 (32.7) |
| Percent of Residents on Public Assistance | 10.8 (10.0) | 10.6 (9.7) |
| Percent of Residents with College Degree | 23.5 (14.6) | 23.7 (14.6) |
Figure 1 presents the variance estimates for null models predicting continuous screen time in adolescence (Wave I) and young adulthood (Wave IV), including hierarchical school-only and neighborhood-only models as well as the null CCMM with both school and neighborhood contexts. The results of the CCMM accounting for both school and neighborhood suggest that the between-level variation in screen time is driven almost exclusively by school-level variation with neighborhood-level variation being relatively small in Wave I and completely negligible in Wave IV compared to the contribution of the school.
Figure 1.
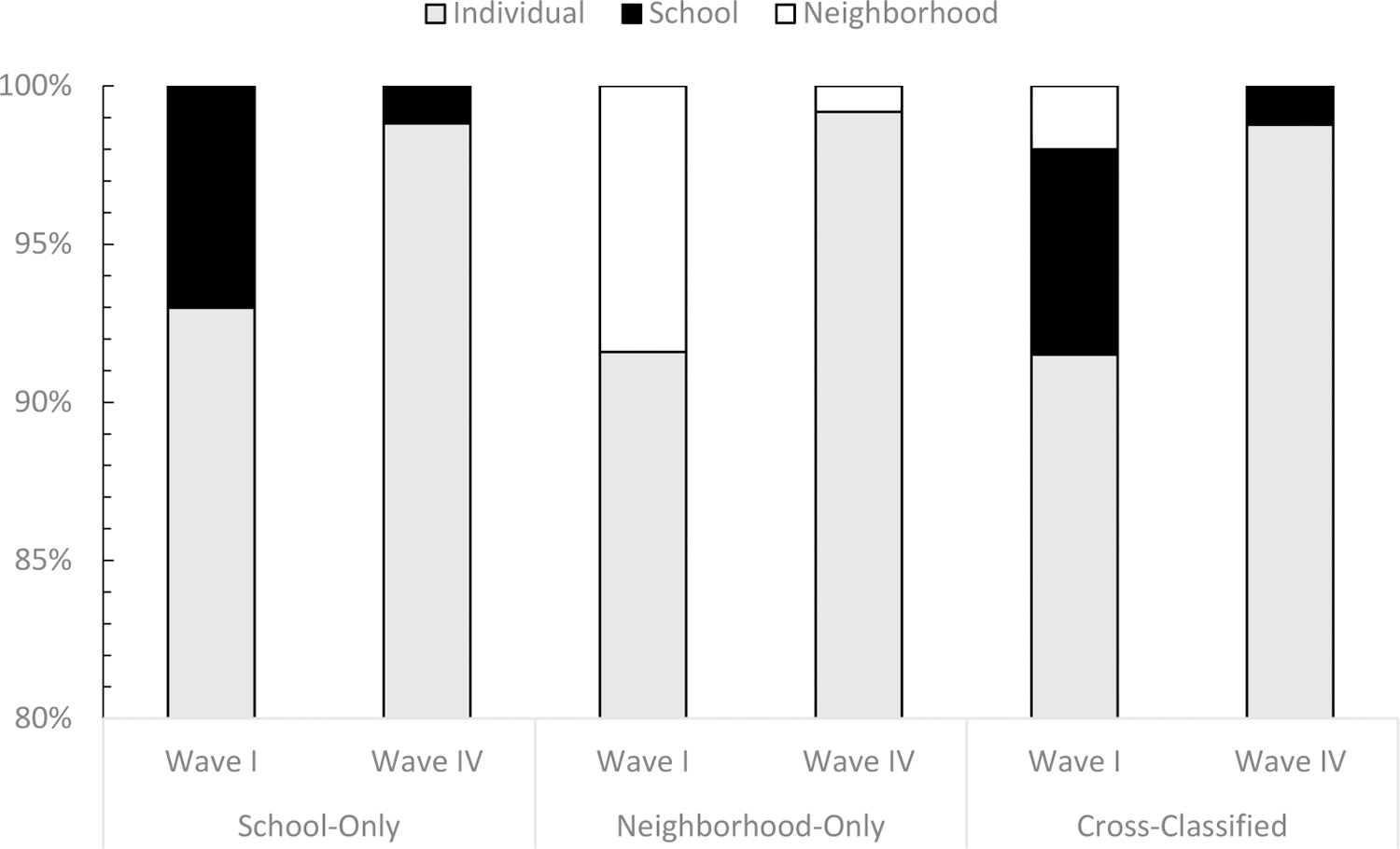
Intra-class correlation estimates from null multilevel models predicting past week screen time during adolescence and young adulthood in the National Longitudinal Study of Adolescent to Adult Health, Wave I, 1994–1995 (N=18,642) and Wave IV, 2007–2009 (N=14,195).
Table 2 shows the series of adjusted cross-classified models predicting continuous screen time among adolescents at Wave I. In the model adjusting only for individual factors (Model 1), the random effects for individual-, school-, and neighborhood-levels were 96%, 3% and 1%, respectively. These indicate that the majority of variation in screen time is due to individual variation, with a small percentage attributable to the school and a negligible percentage to the neighborhood. When school-level predictors were added to the model (Model 2), the school-level variance decreased to 2% attributable to school while the neighborhood variance remained stable with 1% of the variance being attributable to the neighborhood. Model 3 introduces neighborhood predictors into the individual-only model, and variance contributions of the school and neighborhood were similar to Model 1 (3% and 1%, respectively). In the fully-adjusted CCMM (Model 4) accounting for individual, school, and neighborhood-level predictors, ICCs for the school and neighborhood were virtually unchanged with 2% of the variability due to school and only 1% to neighborhood. Comparing the variance parameters from the fully-adjusted model (Table 2, Model 4) to the null model (Figure 1, Cross-Classified Wave I), adjusting for individual, school and neighborhood predictors attenuated the variance contributions for both the school (from 7% null to 2% fully-adjusted) and neighborhood (from 2% to 1%).
Table 2.
Linear cross-classified multilevel models (CCMM) predicting past week screen time (hours) in adolescence from individual-, school- and neighborhood-level factors in the National Longitudinal Study of Adolescent to Adult Health, Wave I, 1994–1995 (N=18,642).
| Model 1 Individual Predictors | Model 2 Individual and School Predictors | Model 3 Individual and Neighborhood Predictors | Model 4 Individual, School, and Neighborhood Predictors | |
|---|---|---|---|---|
| Fixed Effect Estimates | β (95% Credible Interval) | |||
| Intercept | 47.04 (43.66, 50.40) | 50.09 (45.5, 54.7) | 50.26 (46.03, 54.37) | 51.63 (46.95, 56.41) |
| Individual-Level | ||||
| Age (years) | −1.43 (−1.63, −1.23) | −1.36 (−1.55, −1.16) | −1.43 (−1.62, −1.22) | −1.37 (−1.57, −1.18) |
| Female Gender | −5.76 (−6.31, −5.19) | −5.75 (−6.31, −5.21) | −5.76 (−6.32, −5.21) | −5.76 (−6.34, −5.22) |
| Race/Ethnicity | ||||
| White | REF | REF | REF | REF |
| Black | 7.42 (6.45, 8.39) | 6.78 (5.84, 7.74) | 6.66 (5.65, 7.70) | 6.43 (5.39, 7.51) |
| Asian | 0.78 (−0.57, 2.15) | 0.31 (−1.08, 1.64) | 0.64 (−0.77, 2.01) | 0.22 (−1.19, 1.61) |
| Hispanic | 0.59 (−0.33, 1.61) | 0,03 (−1.00, 1.11) | 0.45 (−0.75, 1.51) | −0.03 (−1.12, 1.00) |
| Other | 3.67 (1.25, 6.19) | 3.17 (0.71, 5.64) | 3.42 (0.95, 5.86) | 3.05 (0.66, 5.47) |
| Multiracial | 3.19 (1.76, 4.65) | 2.90 (1.49, 4.33) | 3.00 (1.58, 4.42) | 2.81 (1.35, 4.26) |
| Parental Education | ||||
| Less than high school | REF | REF | REF | REF |
| High school graduate/GED | 1.47 (0.48, 2.49) | 1.59 (0.62, 2.59) | 1.53 (0.57 2.53) | 1.62 (0.60, 2.62) |
| Some college | 1.03 (0.04, 2.04) | 1.22 (0.21, 2.24) | 1.13 (0.10, 2.13) | 1.28 (0.24, 2.30) |
| College graduate or beyond | −0.89 (−1.89, 0.14) | −0.56 (−1.59, 0.45) | −0.66 (−1.71, 0.37) | −0.44 (−1.54, 0.61) |
| Parent Receipt of Public Assistance | 2.08 (1.11, 3.08) | 1.89 (0.90, 2.87) | 1.98 (0.99, 2.96) | 1.85 (0.86, 2.86) |
| School currently in session | −3.85 (−4.46, −3.26) | −3.91 (−4.50, −3.31) | −3.88 (−4.47, −3.28) | −3.94 (−4.53, −3.31) |
| School-Level* | ||||
| Percent White Race | −0.55 (−0.87, −0.25) | −0.46 (−0.79, −0.14) | ||
| Percent on Public Assistance | 0.73 (−0.34, 1.75) | 0.82 (−0.21, 1.85) | ||
| Parental College Degree | −0.67 (−1.13, −0.20) | −0.56 (−1.06, −0.08) | ||
| Neighborhood-Level* | ||||
| Percent White Race | −0.28 (−0.49, −0.06) | −0.17 (−0.39, 0.06) | ||
| Percent on Public Assistance | −0.10 (−0.82, 0.63) | −0.24 (−0.94, 0.48) | ||
| Percent with College Degree | −0.40 (−0.77, −0.02) | −0.30 (−0.70, 0.11) | ||
| Random Effect Estimates | Variance Parameter (95% Credible Interval) [ICC] | |||
| Individual | 365.4 (358.0, 373.1) [96%] | 365.1 (257.3, 372.7) [97%] | 365.3 (357.6, 373.0) [96%] | 365.2 (357.6, 372.7) [97%] |
| School | 13.22 (9.0, 18.4) [3%] | 7.50 (4.6, 11.2) [2%] | 11.3 (7.5, 16.0) [3%] | 7.6 (4.8, 11.3) [2%] |
| Neighborhood | 3.80 (1.4, 6.5) [1%] | 4.35 (2.1, 7.1) [1%] | 4.0 (1.9, 6.9) [1%] | 4.1 (1.4, 7.1) [1%] |
| Fit Statistics (DIC) | 163137 | 163124 | 163137 | 163126 |
ICC: intra-class correlation
DIC: deviance information criterion
School and neighborhood-level predictors are presented as estimate for a 10% change in the predictor
In the fully-adjusted CCMM (Table 2, Model 4), we found associations between continuous screen time and individual-level fixed effects for age, gender, race/ethnicity, and parental education. Being of older age and the female gender were associated with lower screen time while Black, Hispanic, and Multiracial adolescents reported more screen time than White adolescents. Receipt of public assistance was associated with higher screen time and parental education beyond high school but less than college was associated with more screen time compared to those whose parents had not graduated high school. At the individual level, the association between screen time and race/ethnicity was significant. For example, the detected β for 10% change comparing Black to White students was 6.43 (95% CI: 5.39, 7.51). At the school level, we detected an association between screen time and the percentage of students whose parents had a college degree (β for 10% change; 95% CI: −0.56; −1.06, −0.08), as well as with the percentage of students who were White (β for 10% change; 95% CI: −0.46; −0.79, −0.14). There was no association with the percentage of students in the school whose parent had received public assistance. Neighborhood-level fixed effects were not associated with continuous screen time.
Results from cross-classified logistic models predicting extended screen time (≥ 14 hours per week) during adolescence (Wave I) are presented in Supplementary Table 1. Results were comparable to the findings from linear regression with continuous screen time.
Table 3 presents results of fully-adjusted individual, school, and neighborhood CCMM models predicting continuous screen time (linear regression) and extended screen time (≥ 14 hours per week; logistic regression) among young adults at Wave IV. Fixed effect findings were similar to Wave I with differences by age, gender, race/ethnicity, and parental education. Though the school-level variance was attenuated, a small percentage of the variation in screen time in young adulthood was attributable to the adolescent school-level (ICC=1% in both linear and logistic models).
Table 3.
Linear and logistic cross-classified multilevel models (CCMM) predicting past week screen time in young adulthood in the National Longitudinal Study of Adolescent to Adult Health, Wave IV, 2007–2009 (N=14,195).
|
Screen Time (hours per week) |
Extended Screen
Time (≥14 hours per week) |
|
|---|---|---|
| Fixed Effect Estimates | β (95% CI) | Odds Ratio (95% CI) |
| Intercept | 30.55 (23.60, 37.69) | 0.97 (0.56, 1.63)† |
| Individual-Level | ||
| Age (years) | −0.33 (−0.54, −0.12) | 0.97 (0.95, 0.99) |
| Female Gender | −4.57 (−5.21, −3.93) | 0.69 (0.65, 0.75) |
| Race/Ethnicity | ||
| White | REF | |
| Black | 2.84 (1.70, 3.99) | 1.04 (0.91, 1.17) |
| Asian | 3.89 (2.24, 5.58) | 1.69 (1.39, 2.03) |
| Hispanic | −0.04 (−1.20, 1.17) | 1.04 (0.91, 1.18) |
| Other | 1.74 (−1.17, 4.61) | 0.96 (0.70, 1.29) |
| Multiracial | 3.20 (1.49, 4.91) | 1.10 (0.91, 1.31) |
| Parental Education | ||
| Less than high school | REF | REF |
| High school graduate/GED | 0.62 (−0.58, 1.80) | 1.14 (1.01, 1.29) |
| Some college | 1.08 (−0.08, 2.31) | 1.17 (1.04, 1.32) |
| College graduate or beyond | 1.19 (−0.03, 2.45) | 1.29 (1.13, 1.46) |
| Parent Receipt of Public Assistance | 1.04 (−0.13, 2.21) | 0.98 (0.86, 1.12) |
| School-Level* | ||
| Percent White Race | 0.15 (−0.14, 0.44) | 1.01 (0.99, 1.05) |
| Percent on Public Assistance | 0.77 (−0.10, 1.7) | 1.03 (0.95, 1.13) |
| Parental College Degree | 0.31 (−0.12, 0.74) | 1.04 (1.00, 1.09) |
| Neighborhood-Level* | ||
| Percent White Race | −0.03 (−0.27, 0.21) | 1.02 (0.98, 1.03) |
| Percent on Public Assistance | −0.57 (−1.29, 0.15) | 0.95 (0.88, 1.02) |
| Percent with College Degree | −0.23 (−0.63, 0.19) | 0.98 (0.93, 1.02) |
| Random Effect Estimates | Variance Parameter (95% Credible Interval) [ICC] | |
| Individual | 368.5 (360.2, 377.3) [99%] | N/A |
| School | 4.21 (2.45, 6.70) [1%] | 0.04 (0.002, 0.02) [1%] |
| Neighborhood | 0.39 (0.01, 1.21) [0%] | 0.01 (0.02, 0.06) [0%] |
β log odds (95% Credible Interval)
ICC: intra-class correlation
School and neighborhood-level predictors are presented as estimate for a 10% change in the predictor
Discussion
In this large multilevel cohort study of U.S. adolescents, we found that individual-level factors most influence youth screen time, with smaller yet significant contributions from school factors. Many of these individual- and school-level factors continued to influence reported screen time at 14-year follow-up into adulthood. At the individual level, younger age, male sex, Black or multiracial race, receipt of public assistance, and lower parental education were associated with higher adolescent screen time. At the school level, being out of session (i.e., school and national holidays including summer), having a higher proportion of non-White students, and having a lower proportion of students’ parents with a college education were associated with higher individual screen time in adolescents. After accounting for individual- and school-level contexts, neighborhood-level contexts were attenuated and not statistically significant. Moreover, comparable ICC values were also obtained for both the school and neighborhood (2% and 1%, respectively). These results suggest that the between-level variation in screen time was due largely to the observed individual characteristics across schools and neighborhoods, and that more of the variability in screen time was attributable to the school-level characteristics than the neighborhood level characteristics. Previous studies examining outcomes such as alcohol consumption and BMI have similarly found approximately 5% variance partitioned between school and neighborhood factors among adolescents and young adults and using Add Health data.49–51 Our study contributes to the sparse literature examining multiple contextual contributors to adolescent screen time and indicates that while individual environment is a significant predictor of screen time, among the contextual influences, school may be an important contributor to adolescent screen time.
We found several individual-level factors associated with adolescent screen time that add to the literature by accounting for school- and neighborhood-level factors. We found that adolescent boys reported more screen time than adolescent girls, similar to prior literature finding this gender difference due to the association between adolescent boys and computers and electronic games.25 We found that Black adolescents in particular were more likely than White adolescents to report more screen time, similar to prior findings in the U.S.26 and Brazil.27 In terms of individual socio-economic indicators, we found that receipt of public assistance and lack of parental college education was associated with higher adolescent screen time. Prior studies have found that adolescents in low-income households reported more screen time than adolescents in high-income households.28 None of these prior studies simultaneously accounted for school- or neighborhood-level factors, which is a novel contribution of the current study.
Our study finds that schools had more influence on adolescents’ screen time than neighborhoods. This finding builds on prior literature showing that school environments are associated with screen time.29,30,52,53 Factors previously shown to be associated with lower screen time included feeling safe at school, perceiving teachers to be fair,29 and participation in extracurricular school-based activities,30 particularly sports.30 Our study builds on these findings by showing that socio-demographic school-level factors such as parental education and race, as well as school being in session, contribute to adolescent screen time, net of other neighborhood or individual factors. The percent of parents with a college education at the adolescent’s school was associated with screen time 14-years later when participants were 24–32 years old, consistent with previous findings’ suggestions that the transition from adolescence to young adulthood may be a period that sets sedentary behavior trajectories for the rest of adulthood and thus represents an important window for early intervention.48,54,55 The socio-demographic breakdown of schools may influence adolescents’ screen time net of their individual factors given that adolescents spend many hours in schools and with their peers. The prior school-level literature did not account for neighborhood-level factors.
In models only accounting for neighborhood-level factors, neighborhood-level SES/demographics such as education and race were associated with adolescent screen time. Prior studies have shown that neighborhood-level factors such as poorer perceived aesthetics31, higher social neighborhood disorder,32 and inadequate access to outdoor activities30 were associated with higher adolescent screen time. However, these studies did not also account for school- and individual-level factors. We found that when accounting for the school and individual contexts, neighborhood contexts were no longer significantly associated with adolescent screen time. Similarly, one Brazilian study found that no neighborhood characteristics were associated with screen time, after adjusting for confounders.56
Limitations
This study has limitations that merit acknowledgement. First, the screen time measure was based on self-report of hours per week not hours per week or weekend days. Therefore, we extrapolated the American Academy of Pediatrics guideline of ≤2 hours of daily screen time to a seven-day week and used ≤14 hours per week threshold in our analyses, an approach that may be subject to misclassification of the outcome variable of interest. Although 45% of neighborhoods at Wave I contained a single respondent, prior work using Add Health has indicated no issue with bias in the random effect estimates as a result of small neighborhood sizes.51 Third, baseline data in Add Health were collected in the 1990s, and due to enhanced technology, several discretionary screen time behaviors that are common now (e.g., streaming online content) were not captured or available then. However, Add Health is one of the few large, national samples of adolescents in the US that collected school and neighborhood-level data and was therefore appropriate to apply the Cross-Classified Multilevel Model framework. Of note, data on young adult neighborhood and school contexts after Wave 1 were not collected and thus a longitudinal analysis was not possible. Further, all screen time behaviors included as recall prompts in the Wave 1 survey are all relevant and common today. Data were unweighted in these analyses because complex sample weighting techniques for CCMMs are not well-established. Nonetheless, strengths of the study included a large, national sample and a longitudinal study design. To our knowledge, this is the first study to examine the influence of schools, neighborhoods, and individual factors simultaneously on adolescent screen time.
Conclusion
In conclusion, we find that schools and individual-level factors influence youth screen time more than neighborhoods. Understanding the relative importance of these various contexts is important for developing targeted interventions to reduce screen time and sedentary behavior among adolescents, which are linked to poor health outcomes including sleep disturbances and cardiovascular disease. Future research is needed to capture more contemporary types of screen time and to delineate the specific mechanisms by which these contexts influence screen time.
Supplementary Material
Highlights:
Cross-classified mixed models examined contextual associations with screen time
Individual-level factors most strongly influence adolescent screen time
Younger age, male sex, Black/multiracial race were associated with higher screen time
Public assistance and lower parental education were associated with higher screen time
School-level factors have a small yet significant influence on adolescent screen time
Acknowledgments:
The authors thank Samuel E. Benabou for editorial assistance.
This research uses data from Add Health, a program project directed by Kathleen Mullan Harris and designed by J. Richard Udry, Peter S. Bearman, and Kathleen Mullan Harris at the University of North Carolina at Chapel Hill, and funded by grant P01-HD31921 from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, with cooperative funding from 23 other federal agencies and foundations. No direct support was received from grant P01-HD31921 for this analysis.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Sawyer SM, Azzopardi PS, Wickremarathne D & Patton GC The age of adolescence. The Lancet Child & Adolescent Health 2, 223–228 (2018). [DOI] [PubMed] [Google Scholar]
- 2.Tremblay MS et al. Sedentary behavior research network (SBRN)–terminology consensus project process and outcome. International Journal of Behavioral Nutrition and Physical Activity 14, 75 (2017). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Pate RR, Mitchell JA, Byun W & Dowda M Sedentary behaviour in youth. British journal of sports medicine 45, 906–913 (2011). [DOI] [PubMed] [Google Scholar]
- 4.Carson V et al. Systematic review of sedentary behaviour and health indicators in school-aged children and youth: an update. Applied Physiology, Nutrition, and Metabolism 41, S240–S265 (2016). [DOI] [PubMed] [Google Scholar]
- 5.Mitchell J, Pate R, Beets M & Nader P Time spent in sedentary behavior and changes in childhood BMI: a longitudinal study from ages 9 to 15 years. International journal of obesity 37, 54–60 (2013). [DOI] [PubMed] [Google Scholar]
- 6.Thorp AA, Owen N, Neuhaus M & Dunstan DW Sedentary behaviors and subsequent health outcomes in adults: a systematic review of longitudinal studies, 1996–2011. American journal of preventive medicine 41, 207–215 (2011). [DOI] [PubMed] [Google Scholar]
- 7.de Rezende LFM, Rodrigues Lopes M, Rey-López JP, Matsudo VKR & Luiz O. d. C. Sedentary behavior and health outcomes: an overview of systematic reviews. PloS one 9, e105620–e105620, 10.1371/journal.pone.0105620 (2014). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Marshall SJ & Ramirez E Reducing sedentary behavior: a new paradigm in physical activity promotion. American Journal of Lifestyle Medicine 5, 518–530 (2011). [Google Scholar]
- 9.Owens CS, Crone D & James DV Physical activity and sedentary behaviour among adolescents. Youth Sport, Physical Activity and Play: Policy, Intervention and Participation, 113–125 (2013).
- 10.Fox M What is sedentarism? Journal of the Academy of Nutrition and Dietetics 112, 1124 (2012). [DOI] [PubMed] [Google Scholar]
- 11.Lubans DR et al. A systematic review of the validity and reliability of sedentary behaviour measures used with children and adolescents. Obesity reviews 12, 781–799 (2011). [DOI] [PubMed] [Google Scholar]
- 12.Matthews CE et al. Amount of time spent in sedentary behaviors in the United States, 2003–2004. American journal of epidemiology 167, 875–881 (2008). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Children, Adolescents, and the Media. Pediatrics 132, 958–961, 10.1542/peds.2013-2656 (2013). [DOI] [PubMed] [Google Scholar]
- 14.Mamun AA, O’Callaghan MJ, Williams G & Najman JM Television watching from adolescence to adulthood and its association with BMI, waist circumference, waist-to-hip ratio and obesity: a longitudinal study. Public Health Nutrition 16, 54–64 (2013). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Chassiakos YLR, Radesky J, Christakis D, Moreno MA & Cross C Children and adolescents and digital media. Pediatrics 138, e20162593 (2016). [DOI] [PubMed] [Google Scholar]
- 16.Lissak G Adverse physiological and psychological effects of screen time on children and adolescents: Literature review and case study. Environmental research 164, 149–157 (2018). [DOI] [PubMed] [Google Scholar]
- 17.Brodersen NH, Steptoe A, Boniface DR & Wardle J Trends in physical activity and sedentary behaviour in adolescence: ethnic and socioeconomic differences. British journal of sports medicine 41, 140–144 (2007). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Whitt-Glover MC et al. Disparities in physical activity and sedentary behaviors among US children and adolescents: prevalence, correlates, and intervention implications. Journal of public health policy 30, S309–S334 (2009). [DOI] [PubMed] [Google Scholar]
- 19.Van Der Horst K, Paw MJCA, Twisk JW & Van Mechelen W A brief review on correlates of physical activity and sedentariness in youth. Medicine & Science in Sports & Exercise 39, 1241–1250 (2007). [DOI] [PubMed] [Google Scholar]
- 20.Basterfield L et al. Longitudinal study of physical activity and sedentary behavior in children. Pediatrics 127, e24–e30 (2011). [DOI] [PubMed] [Google Scholar]
- 21.Harding SK, Page AS, Falconer C & Cooper AR Longitudinal changes in sedentary time and physical activity during adolescence. International Journal of Behavioral Nutrition and Physical Activity 12, 44 (2015). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Tsiros MD et al. Health-related quality of life in obese children and adolescents. International journal of obesity 33, 387 (2009). [DOI] [PubMed] [Google Scholar]
- 23.Iannotti RJ & Wang J Trends in physical activity, sedentary behavior, diet, and BMI among US adolescents, 2001–2009. Pediatrics 132, 606–614 (2013). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Liu J, Kim J, Colabianchi N, Ortaglia A & Pate RR Co-varying patterns of physical activity and sedentary behaviors and their long-term maintenance among adolescents. Journal of Physical Activity and Health 7, 465–474 (2010). [DOI] [PubMed] [Google Scholar]
- 25.Bounova A, Michalopoulou M, Agelousis N, Kourtessis T & Gourgoulis V Home and neighborhood environment predictors of adolescents’ screen viewing. Journal of Physical Activity and Health 13, 1310–1316 (2016). [DOI] [PubMed] [Google Scholar]
- 26.Carson V, Staiano AE & Katzmarzyk PT Physical activity, screen time, and sitting among US adolescents. Pediatric exercise science 27, 151–159 (2015). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Sousa G. R. d. & Silva DAS Comportamento sedentário baseado em tempo de tela: prevalência e fatores sociodemográficos associados em adolescentes. Ciência & Saúde Coletiva 22, 4061–4072 (2017). [DOI] [PubMed] [Google Scholar]
- 28.Hunt ET et al. Income, race and its association with obesogenic behaviors of US children and adolescents, NHANES 2003–2006. Journal of Community Health 44, 507–518 (2019). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Katapally TR, Laxer RE, Qian W & Leatherdale ST Do school physical activity policies and programs have a role in decreasing multiple screen time behaviours among youth? Preventive medicine 110, 106–113 (2018). [DOI] [PubMed] [Google Scholar]
- 30.Minges KE et al. Reducing youth screen time: qualitative metasynthesis of findings on barriers and facilitators. Health Psychology 34, 381 (2015). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Bejarano CM et al. Neighborhood built environment associations with adolescents’ location-specific sedentary and screen time. Health & place 56, 147–154 (2019). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Carson V & Janssen I Neighborhood disorder and screen time among 10–16 year old Canadian youth: a cross-sectional study. International journal of behavioral nutrition and physical activity 9, 66 (2012). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Patton GC et al. Our future: a Lancet commission on adolescent health and wellbeing. Lancet 387, 2423–2478, 10.1016/S0140-6736(16)00579-1 (2016). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Nagata JM, Ferguson BJ & Ross DA Research priorities for eight areas of adolescent health in low-and middle-income countries. Journal of Adolescent Health 59, 50–60 (2016). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Harris KM & Udry JR National longitudinal study of adolescent to adult health (add health), 1994–2008 [Public Use]. Inter-university Consortium for Political and Social Research (ICPSR)[distributor] (2017).
- 36.Harris KM The add health study: Design and accomplishments. Chapel Hill: Carolina Population Center, University of North Carolina at Chapel Hill, 1–22 (2013). [Google Scholar]
- 37.Badon SE, Littman AJ, Chan KCG, Williams MA & Enquobahrie DA Trajectories of maternal leisure-time physical activity and sedentary behavior during adolescence to young adulthood and offspring birthweight. Annals of epidemiology 27, 701–707. e703 (2017). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Carter JS, Dellucci T, Turek C & Mir S Predicting depressive symptoms and weight from adolescence to adulthood: stressors and the role of protective factors. Journal of youth and adolescence 44, 2122–2140 (2015). [DOI] [PubMed] [Google Scholar]
- 39.Lee PH Association between adolescents’ physical activity and sedentary behaviors with change in BMI and risk of type 2 diabetes. PloS one 9 (2014). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Lee PH Physical activity, sedentary behaviors, and Epstein-Barr virus antibodies in young adults. Physiology & behavior 164, 390–394 (2016). [DOI] [PubMed] [Google Scholar]
- 41.Pettee KK, Ham SA, Macera CA & Ainsworth BE The reliability of a survey question on television viewing and associations with health risk factors in US adults. Obesity 17, 487–493 (2009). [DOI] [PubMed] [Google Scholar]
- 42.Stasburger V, Hogan M & Mulligan D American Academy of Pediatrics committee on communication: Children, adolescents, and the media. Pediatrics 132, 958–961 (2013). [DOI] [PubMed] [Google Scholar]
- 43.Browne W MCMC estimation in MLwiN v. 3.01. Centre for Multilevel Modelling, University of Bristol: Bristol, UK: (2017). [Google Scholar]
- 44.Rabash J & Browne W (New York, NY: Wiley and Sons, 2001). [Google Scholar]
- 45.Rasbash J, Steele F, Browne WJ, Goldstein H & Charlton C A user’s guide to MLwiN. Accessed 12, 13 (2017). [Google Scholar]
- 46.Rodríguez G & Goldman N An assessment of estimation procedures for multilevel models with binary responses. Journal of the Royal Statistical Society: Series A (Statistics in Society) 158, 73–89 (1995). [Google Scholar]
- 47.Goldstein H, Browne W & Rasbash J Partitioning variation in multilevel models. Understanding statistics: statistical issues in psychology, education, and the social sciences 1, 223–231 (2002). [Google Scholar]
- 48.Vespa J The changing economics and demographics of young adulthood: 1975–2016. (US Department of Commerce, Economics and Statistics Administration, US: …, 2017). [Google Scholar]
- 49.Pedersen W, Bakken A & von Soest T Neighborhood or school? Influences on alcohol consumption and heavy episodic drinking among urban adolescents. Journal of youth and adolescence 47, 2073–2087 (2018). [DOI] [PubMed] [Google Scholar]
- 50.Niu L, Hoyt LT & Pachucki MC Context Matters: Adolescent Neighborhood and School Influences on Young Adult Body Mass Index. Journal of Adolescent Health 64, 405–410 (2019). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Milliren CE, Evans CR, Richmond TK & Dunn EC Does an uneven sample size distribution across settings matter in cross-classified multilevel modeling? Results of a simulation study. Health & place 52, 121–126 (2018). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Katapally TR, Thorisdottir AS, Laxer R, Qian W & Leatherdale ST Recherche quantitative originale–Association entre le sentiment d’appartenance à l’école, la participation à l’intimidation et divers comportements associés au temps passé devant un écran chez les jeunes dans deux provinces canadiennes: une étude COMPASS. [DOI] [PMC free article] [PubMed]
- 53.Vandendriessche A et al. Does sleep mediate the association between school pressure, physical activity, screen time, and psychological symptoms in early adolescents? A 12-country study. International journal of environmental research and public health 16, 1072 (2019). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Kwon S, Janz KF, Letuchy EM, Burns TL & Levy SM Developmental trajectories of physical activity, sports, and television viewing during childhood to young adulthood: Iowa bone development study. JAMA pediatrics 169, 666–672 (2015). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Schmitz K, Jacobs D, Leon A, Schreiner P & Sternfeld B Physical activity and body weight: associations over ten years in the CARDIA study. International journal of obesity 24, 1475–1487 (2000). [DOI] [PubMed] [Google Scholar]
- 56.Parajára MDC, Andrade ACDS, Xavier CC, Proietti FA & Meireles AL Associations of the perceived neighborhood environment and screen time in adolescents living in a medium-sized city in Brazil: a cross-sectional study. International journal of environmental health research, 1–13 (2019). [DOI] [PubMed]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.