

Supplemental Digital Content is available in the text.
Keywords: aging, neighborhood factors, telomere length, socioeconomic status
Abstract
Background:
Telomere length (TL) may serve as a biologic marker of aging. We examined neighborhood and individual-level socioeconomic status (SES) in relation to TL.
Methods:
The study included 84,996 non-Hispanic white subjects from the Genetic Epidemiology Research on Adult Health and Aging (GERA) cohort, part of the Research Program on Genes, Environment and Health. Relative TL (T/S) was log2 transformed to improve normality and standardized to have mean 0 and variance 1. Neighborhood SES was measured using the Neighborhood Deprivation Index (NDI), and individual SES was measured by self-reported education level. We fit linear regression models of TL on age, sex, smoking, body mass index, comorbidities, NDI, and education level. We tested for differences in the associations by sex and nonlinearity in the association of NDI with TL.
Results:
Each SD increase in NDI was associated with a decrease of 0.0192 in standardized TL, 95% confidence interval (CI) = −0.0306, −0.0078. There was no evidence of nonlinearity in the association of NDI with TL. We further found that less than high school education was associated with a decrease of 0.1371 in standardized TL, 95% CI = −0.1919, −0.0823 as compared to a college education. There were no differences in the associations by sex.
Conclusions:
We found evidence that both lower neighborhood SES and lower individual-level SES are associated with shorter TL among non-Hispanic whites. Our findings suggest that socioeconomic factors may influence aging by contributing to shorter TL.
What this study adds
Our study found independent associations of neighborhood SES and individual-level SES with TL. Our findings suggest that lower SES may influence aging by contributing to shorter TL, and that neighborhood effects may exist even after accounting for an individual’s education level. Moreover, our study included 84,996 non-Hispanic white subjects whose TL was uniformly measured in a single laboratory, more individuals than all previous studies of TL and SES combined.
Introduction
Telomeres are repetitive sequences of DNA and associated specialized proteins at chromosomal ends that help protect eukaryotic chromosomes from damage and promote and stabilize chromosomal recovery after replication.1–3 Telomeres frequently shorten with repeated replication cycles and severe shortening of telomeres elicits cell senescence. Shortened telomeres have been proposed as a partial contributor to human aging processes and age-related diseases.4,5 Studies have reported that shorter telomere length (TL) is associated with increased risk of mortality6–8 and with an increased risk of diseases, including cardiovascular disease,9–12 cancer,13,14 diabetes and diabetic complications,15,16 autoimmune disease,17–19 chronic obstructive pulmonary disease,20 and sleep disorders.21,22 TL has also been linked to the mechanisms of oxidative stress and inflammation.23–26 Increased psychological stress has been associated with shorter TL.27–32
Lower socioeconomic status (SES), measured at the individual level and at the neighborhood level, has been linked to adverse health outcomes33,34 as well as decreased life expectancy.35 Furthermore, studies have reported that neighborhood SES affects both morbidity36 and mortality37,38 even after controlling for individual-level SES. The pathways that underlie the relationship between SES and health are not yet well understood. One hypothesized pathway is that lower SES accelerates the rate of biological aging to affect health, which may in turn be reflected in shorter age-adjusted TL.39
Previous studies of the relationship between SES and TL have been severely underpowered due to small sample size, with most studies including fewer than 1,000 subjects.40 In studies examining the association of SES and TL, education level has been the most common measure of individual-level SES.40 Results from these small previous studies have been inconsistent, where several studies have reported an association between TL and education level, whereas other studies have found no statistically significant evidence of an association.40 Fewer studies have examined the relationship between neighborhood SES and TL, and the results have also been inconsistent.41,42
This study examines the effects of individual-level and neighborhood-level SES on TL in a large cohort of non-Hispanic white adults with uniformly measured TL. We hypothesized that (1) lower education levels would be associated with shorter TL and that (2) exposure to greater neighborhood socioeconomic deprivation would be independently associated with shorter TL.
Methods
Study participants
Study subjects were members of the Genetic Epidemiology Research on Adult Health and Aging (GERA) cohort. The GERA cohort is part of the Kaiser Permanente Northern California (KPNC) Research Program on Genes, Environment and Health (RPGEH). Participants in the GERA cohort were recruited from the adult membership of the KPNC health plan, a large integrated health care system that provides comprehensive medical services to four million members. The RPGEH was developed by the KPNC Division of Research as a resource that links together surveys, biospecimens and electronic health record data for research on the genetic and environmental determinants of common, age-related complex health conditions. Further details describing the GERA cohort and study design have been described previously.43–45 This cross-sectional study of TL included 84,996 non-Hispanic white adults in the GERA cohort who had a valid TL measurement that passed quality control checks and a successfully geocoded residential address.
Covariate data
Covariate data on age, sex, race/ethnicity, smoking, and comorbidities were obtained from both self-reported questionnaire data and the electronic health record data of KPNC. Education level was self-reported by questionnaire as the highest level of school completed: grade school or some high school (grades 1–11), high school or General Education Development, technical or trade school, some college, college, graduate school. All GERA cohort subjects completed the questionnaire before donating a saliva specimen for TL measurement. Weekly fruit and vegetable consumption was self-reported by questionnaire in the following categories: less than once per week, 1–2 times/week, 3–4 times/week, 5–6 times/week, or every day.
Neighborhood Deprivation Index
Cohort members reside primarily in a 22-county service area in northern and central California that encompasses over 28,000 square miles and includes urban, suburban, rural and agricultural land use (supplementary Figure 1; http://links.lww.com/EE/A39). Residential addresses at the date of saliva specimen collection for each participant were abstracted from the KPNC address databases. These residential addresses were then geocoded to latitude and longitude using ArcGIS, and each geocoded address was linked to its census tract. Census variables were obtained from the 2010 Census. The Neighborhood Deprivation Index (NDI) was calculated from eight census variables in the domains of income/poverty, education, employment, housing, and occupation using the method of Messer et al.46 Specifically, principal components (PCs) analysis was implemented, and the NDI was defined as the first PC, standardized to have mean 0 and variance 1. Thus, the NDI represents a weighted linear combination of the eight census variables. Higher values of NDI represent more deprivation in the neighborhood (i.e., lower neighborhood-level SES).
Telomere length measurement
Relative TL is measured as the ratio of telomeric product (T) versus the single copy gene product (S) obtained using quantitative polymerase chain reaction.47 Details on the TL measurements and quality control for the GERA cohort have been described previously.44 During July 2008–February 2011, study subjects who completed the questionnaire and consent forms were mailed Oragene saliva collection kits (DNA Genotek; Kanata, Ontario, Canada). DNA was extracted at the KPNC RPGEH biorepository, and samples were shipped in 96-well plates to the Blackburn lab at UCSF for TL analysis. The TL analysis required the design and construction of a novel automated integrated robotic system to reliably handle the high-throughput processing of samples. For this study, the entire system was capable of running 24 hours/day with live video, data streams, and environmental variables monitored and controlled remotely. With an overall daily throughput of 1,920 patient samples, laboratory processing of all samples was efficiently completed within 4 months. Each sample was run at least three times on different plates, so a typical sample had 12 measurements. Quality control procedures included filtering out poor control sets based on the median of the derived standard curve slopes from the dilution sequences for all the control sets. The distribution of relative TL (T/S) was found to be positively skewed. For all analyses, (T/S) was log2 transformed to obtain a more Gaussian distribution and standardized to have mean 0 and variance 1.
Statistical analysis
We computed correlations between covariates using Spearman’s rank correlation coefficient. We modeled a standardized TL as a continuous outcome variable using linear regression analyses. We evaluated the effects of education level and NDI on TL in minimally adjusted models and fully adjusted models, with covariates chosen a priori.40,41 Minimally adjusted models controlled for age, sex and race/ethnicity. The fully adjusted model included age, sex and race/ethnicity, smoking, body mass index (BMI), comorbidities (cardiovascular disease, diabetes, cancer, and Parkinson’s), diet (fruit and vegetable consumption), NDI, and education level. Thus, in the fully adjusted model, the association of NDI was adjusted for the effect of education level, and similarly, the association of education level was adjusted for the effect of NDI. Education level was modeled in categories, including a category for the unknown when the survey question on highest education level was not answered. We tested for a linear trend across increasing levels of education. NDI was modeled as a continuous variable with a linear effect on TL. To determine whether there were differences in these associations by sex, we included interaction terms between education level and sex and between NDI and sex. Formal tests for statistical significance of the interaction terms were performed. To assess potential nonlinearity in the association of NDI with TL, we fit a generalized additive model with spline effects for NDI using three degrees of freedom and we formally tested for the statistical significance of a nonlinear effect.48 We conducted a sensitivity analysis of the association of NDI and TL by restricting to the subjects who had lived at the same address for at least 5 years to assess the influence of recent moving. We evaluated the characteristics of the NDI including the weights and the correlations between each census variable and the NDI measure. The NDI is a weighted and standardized linear combination of a set of eight census variables; the weights of the census variables are determined by the PCs method, so the weights vary from study to study depending on the underlying joint distribution of those census variables within the region studied. We compared the NDI weights of the eight census variables in our study with the weights previously published in Messer et al (2006). Analyses were performed in SAS 9.3 and in R 3.2.2.
Results
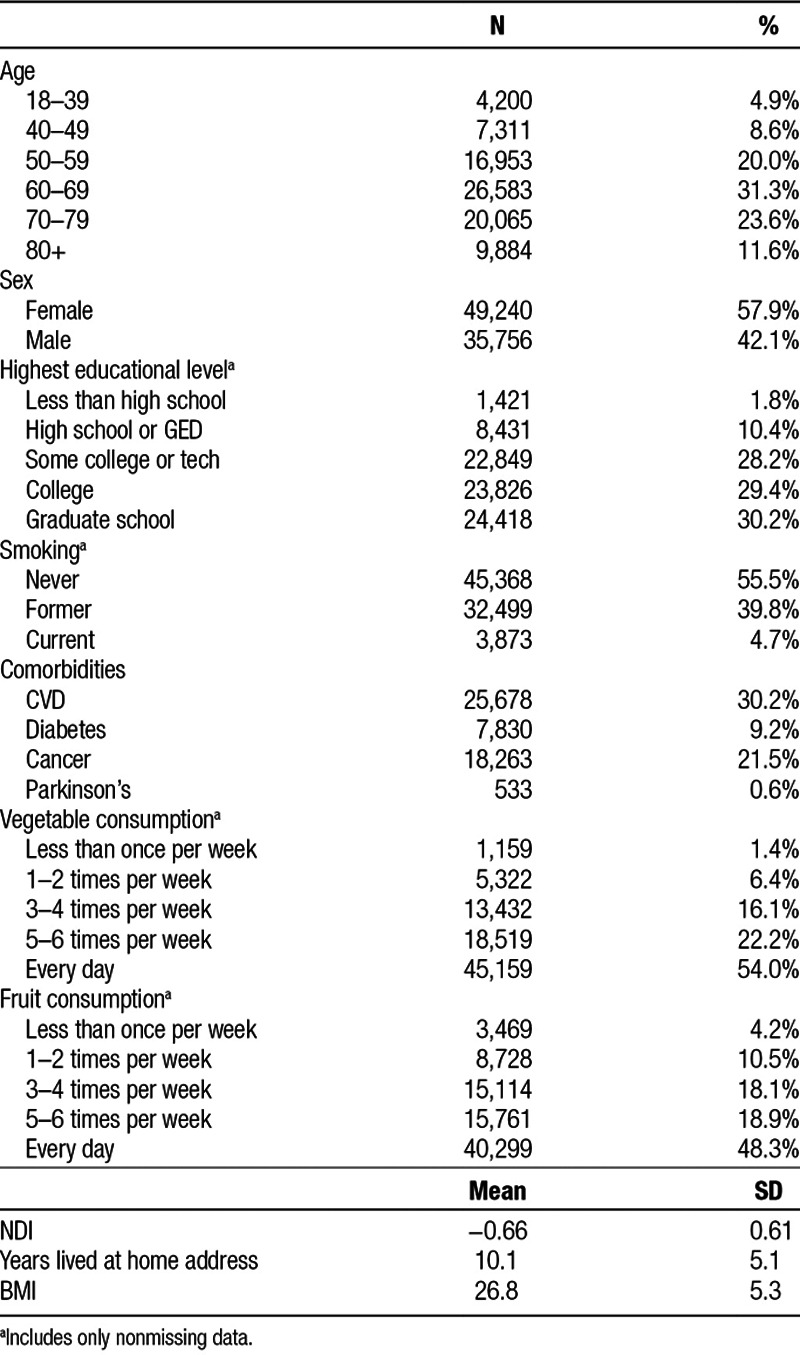
Table 1 shows the descriptive characteristics of the 84,996 non-Hispanic white adults in the GERA cohort who were part of this study. The mean age was 63.9 (range 19–101), and there were more women (N = 49,240; 57.9%) than men (N = 35,756; 42.1%). Study subjects were well-educated, with most completing college or graduate school (N = 48,244; 59.6%), and very few with a less than high school education (N = 1,421; 1.8%). There was a small proportion of missing data for the survey question on education level (4.8% missing).
Table 1.
Characteristics of the study cohort, N = 84,996.
The NDI was weakly inversely correlated with education (r = −0.22), vegetable consumption (r = −0.10), and fruit consumption (r = −0.10), and weakly positively correlated with BMI (r = 0.15), smoking (r = 0.03), and number of comorbidities (r = 0.05); thus those living in neighborhoods with more deprivation tended to have a lower education level, lower intake of fruits and vegetables, higher BMI, be more likely to smoke, and have more comorbidities. Similarly, education level was weakly positively correlated with vegetable consumption (r = 0.15) and fruit consumption (r = 0.15), and weakly inversely correlated with BMI (r = −0.14), smoking (r = −0.12), and number of comorbidities (r = −0.09); thus those with higher education levels tended to have higher intake of fruits and vegetables, lower BMI be less likely to smoke, and have fewer comorbidities.
We found that TL increased with increasing levels of education in both minimally adjusted and fully adjusted models (P-value for linear trend <0.0001). Figure 1 illustrates this trend between education level and TL in the fully adjusted model. Compared to those with a college education, a less than high school education was associated with a change in standardized TL of −0.1371 (95% confidence interval [CI] = −0.1919, −0.0823) and a high school education was associated with a change in standardized TL of −0.0719 (95% CI = −0.0976, −0.0462). Some college or technical training was associated with a change in standardized TL of −0.0408 (95% CI = −0.0593, −0.0223) and graduate school was associated with an increase in standardized TL of 0.0201 (95% CI = 0.0022, 0.0381) compared to the reference category of college. There were no differences by sex in the associations between education level and TL (P-value = 0.1338). Supplementary Figure 2; http://links.lww.com/EE/A39 illustrates the trend between education level and TL separately by sex. Numeric results for education level in minimally adjusted and fully adjusted models overall and by sex are given in Supplementary Table 1; http://links.lww.com/EE/A39.
Figure 1.
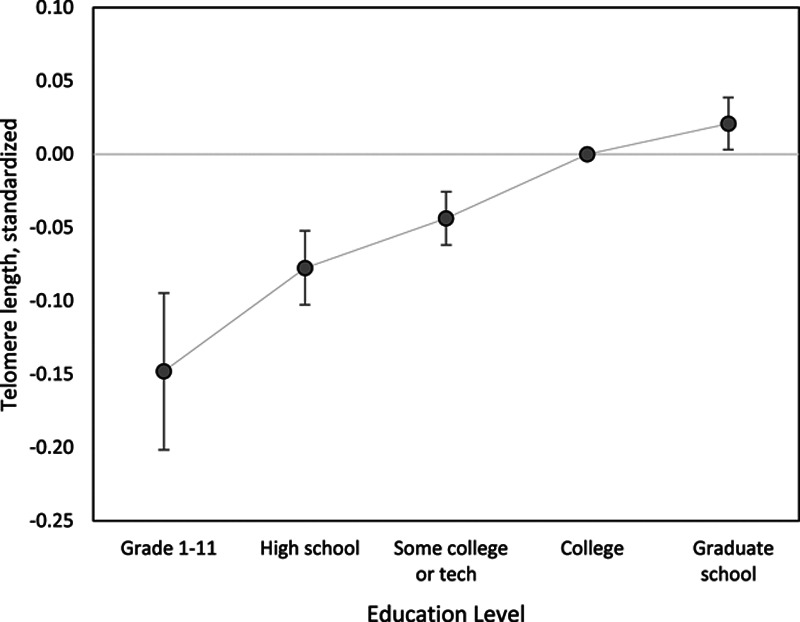
Association between standardized TL and education level in the fully adjusted model, showing the estimated effect size and 95% CI for each education level as compared to the reference level of those with a college education. Fully adjusted model includes age, sex, smoking, BMI, comorbidities, diet, NDI, and education level.
We found that NDI was inversely associated with TL in the minimal and fully-adjusted models, where higher neighborhood deprivation was associated with shorter TL. Results for the association between NDI and TL in the fully adjusted model are shown in Figure 2A, with results shown overall and by sex. Overall, a one SD increase in NDI was associated with a decrease of 0.0192 in standardized TL, 95% CI = −0.0306, −0.0078. Associations between NDI and TL did not vary by sex (P-value = 0.8973). Among women, a one SD increase in NDI was associated with a decrease of 0.0201 in standardized TL (95% CI = −0.0350, −0.0053) and among men a one SD increase in NDI of was associated with a decrease of 0.0186 in standardized TL (95% CI = −0.0362, −0.0010). Numeric results for NDI in minimally adjusted and fully adjusted models are given in Supplementary Table 2, http://links.lww.com/EE/A39.
Figure 2.
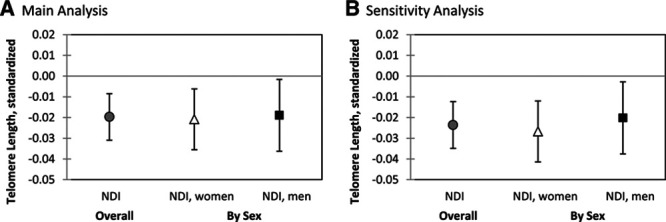
Association between TL and NDI overall and by sex in the fully adjusted model, showing the estimated effect size and 95% CI associated with an increase of one SD in the NDI. Plot (A) shows the main analysis of NDI and TL and plot (B) shows the sensitivity analysis restricting to subjects who lived at their current address for at least 5 years. Fully adjusted model includes age, sex, smoking, BMI, comorbidities, diet, NDI, and education level. There were no statistically significant differences in the association between NDI and TL by sex (P-value for interaction 0.8973).
We conducted a sensitivity analysis of the association of NDI and TL by restricting to the subjects who had lived at the same address for at least 5 years to reduce the influence of recent moving (N = 65,541; 77.1%). The estimated association of NDI with TL in the sensitivity analysis appeared slightly stronger (Figure 2B); an increase of one SD in the NDI was associated with a decrease of 0.0236 in standardized TL (95% CI = −0.0366, −0.0107, P-value = 0.0004). Associations between NDI and TL in the sensitivity analysis did not vary by sex (P-value = 0.7146). Among women, a one SD increase in NDI of was associated with a decrease of 0.0260 in standardized TL (95% CI = −0.0436, −0.0099) and among men a one SD increase in NDI of was associated with a decrease of 0.0212 in standardized TL (95% CI = −0.0410, −0.0013). Numeric results for NDI in sensitivity analyses of minimally adjusted and fully adjusted models are given in Supplementary Table 3, http://links.lww.com/EE/A39.
In our main analyses, we modeled NDI as a continuous variable with a linear relationship to TL. We considered whether the shape of the relationship between NDI and TL might be nonlinear, and we used splines to allow for a potentially nonlinear association of NDI with TL. Figure 3 illustrates the association between NDI and TL among whites when modeled using splines. We see that the association looks nearly linear for NDI ranging from −1 to 1, with a suggestive attenuation of the effect for NDI less than −1 or greater than 1. However, the test for nonlinearity in the association between NDI and TL among whites was not statistically significant (P-value = 0.1848), indicating that the spline model did not provide a better goodness-of-fit to TL than the linear model.
Figure 3.
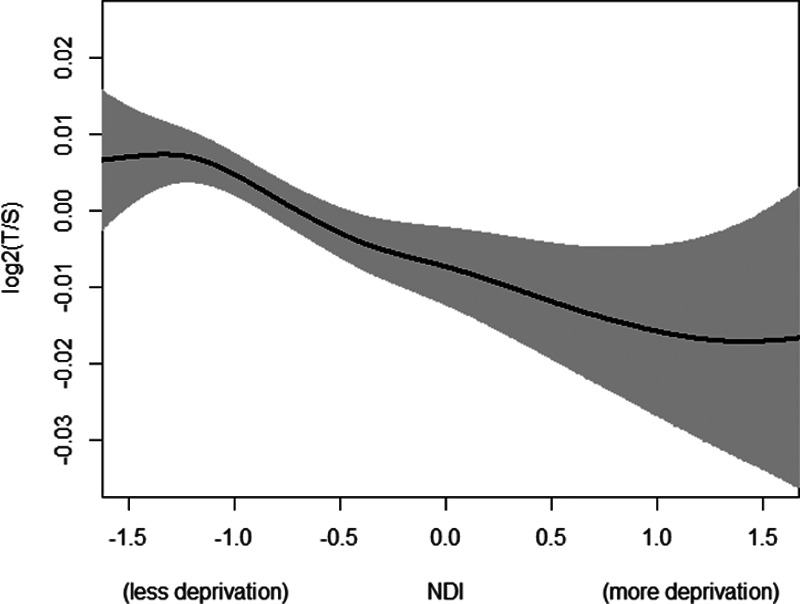
Relationship between the NDI and TL when modeled as a spline effect. The association between NDI and TL was statistically significant when modeled as a spline effect (P-value = 0.0007) and when modeled as a linear effect (P-value = 0.0008). There was no statistically significant evidence of nonlinearity in the association between NDI and TL (P-value = 0.1848).
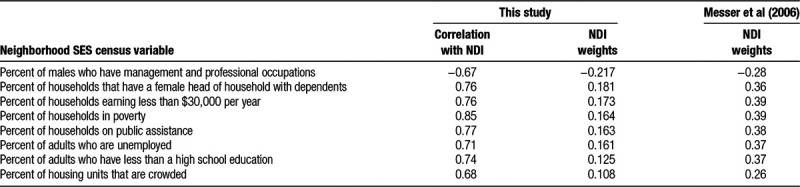
We further evaluated the characteristics of the NDI, with results given in Table 2. We found moderate to high correlations (ranging from 0.67 to 0.85) between each of the eight census variables with the NDI composite score. The NDI was most highly correlated with the percent of households in poverty (r = 0.85). We compared our study’s NDI weights for the eight census variables with the weights in Messer et al (2006); because these weights are determined by the PCs, they vary by study and region. The rows of Table 2 are ordered by the magnitude of each NDI weight in our study from largest to smallest. The NDI weights in our study varied, where the largest weight (for the percent of males who have management and professional occupations) had twice the magnitude of the smallest weight (for percent of housing units that are crowded). In contrast, Messer et al (2006) reported that six of the eight variables had nearly equal weight, and the two remaining variables had a weight that was approximately 25% smaller.
Table 2.
Characteristics of the NDI, weights determined by PCs analysis.
Discussion
In this study, we found that lower SES at the individual and neighborhood level were both independently associated with shorter TL among non-Hispanic whites. Using the education level as a measure of individual-level SES, we found a clear trend of decreasing TL with decreasing levels of education. Using the NDI as a measure of neighborhood-level SES, we found that greater neighborhood deprivation was associated with shorter TL. These neighborhood-level and individual-level SES measures showed independent effects that were statistically significant in fully adjusted models where both neighborhood and individual-level SES were included simultaneously. We found no differences by sex.
Comparison to previous studies
Previous studies of the relationship between individual-level SES and TL have been substantially smaller in sample size. A 2012 review and meta-analysis of 14 studies combining results of N = 8,324 individuals found that higher educational level was associated with longer telomeres.40 Most of these studies included populations drawn from the United States or the United Kingdom. The results were broadly consistent with our finding among non-Hispanic whites. The random-effects meta-analysis found a standardized mean difference in TL of 0.060 (95% CI = 0.002, 0.118) between low and high education categories, where the high category typically corresponded to college graduate. Comparing subjects with less than high school to those who completed college in our study, we found a mean difference in standardized TL of 0.1371 (95% CI = 0.1919, 0.0823) among non-Hispanic whites. Thus, our study results were in the same direction as previous studies, with an estimated effect size was twice that reported in previous studies. Our results were also consistent with a 2013 study using data from the National Health and Nutrition Examination Survey found that subjects with less than a high school education had significantly shorter telomeres than those who graduated from college, but effect sizes were not reported per SD change in TL and could not be directly compared to our study.49
Even less is known about the association between neighborhood SES and TL. One study of 978 subjects from a multi-ethnic cohort found no association between neighborhood socioeconomic disadvantage and TL.41 That study also used PCs methodology to combine six census tract variables into a summary measure of neighborhood SES: percent in census tract with a bachelor’s degree; percent with a managerial/professional occupation; percent with a high school education; median home value; median household income; and percent with household income greater than $50,000 per year. These variables are similar to those used in our NDI measure; however, the weights on each census variable used to create this PC score were not published, so we cannot further compare the measures. The much smaller sample size of that study as well as the finding of differences in association of NDI by race/ethnicity in our study could explain why that study found no association. Another study in a cohort of N = 2,902 subjects with northern European ancestry found an association between perceived neighborhood quality and shorter TL.42 Perceived neighborhood quality was assessed using self-reported answers to questions about noise, vandalism, and safety.50,51 The direction of their association was consistent with our finding in non-Hispanic whites, although their self-reported neighborhood measure is likely to be capturing a different construct of neighborhood features than our measure of NDI. Our finding among whites that neighborhood SES is associated with TL even after adjusting for education level is consistent with studies that have reported that neighborhood SES affects both morbidity36 and mortality37,38 even after controlling for individual-level SES.
Mechanisms
Socioeconomic differences in health have been widely documented across numerous populations and health outcomes, but the precise pathways and mechanisms that link SES and health are not yet understood.34,35,52 It has been hypothesized that socioeconomic differences in health may result in part from an accelerated aging process among those with lower SES.39 Previous studies have shown that lower SES is associated with increased exposure to a wide variety of risk factors, from individual behaviors to environmental exposures.39,52,53 These factors include cigarette smoking, radiation, and air pollution, each of which increases oxidative stress.39 These increased exposures are thought to lead to a greater risk of cellular and genomic damage and depleted repair and protection mechanisms.54 This damage can be viewed as accelerated aging, which may be reflected in shorter age-adjusted TL and may increase the risk of premature death and chronic diseases.39,55 Furthermore, important antioxidants and cofactors for antioxidant enzymes are derived through dietary intake of fresh fruits and vegetables,56 which is why it is crucial to control for fruit and vegetable consumption as we did in this study.
An important next step of this work would be to conduct an analysis that evaluates the mediating role of environmental exposures (e.g., air pollution, noise) and neighborhood stressors (e.g., violence, crime) and decomposes the total effect of neighborhood SES into direct and indirect effects using mediation analysis methodology. The present study uses residential addresses of the study participants at the time of specimen collection to determine TL; these addresses have been geocoded and linked to census data. Data on neighborhood stressors such as violence and crime could be assembled from publicly available data sources and linked to the geocoded addresses in this study. Longer address histories are available for a subset of study subjects, and future studies could link spatial or spatio-temporal data from models of air pollution and noise to these addresses. Also, the present study looks at the effect of neighborhood SES after accounting for the impact of individual-level health factors, but another perspective would be first describing the overall differences in TL by neighborhood SES and then examining how much of that overall effect is accounted for by individual-level health factors and behaviors, how much is accounted for by other spatially-varying exposures such as environmental exposures and neighborhood stressors, and how much of that overall effect is as yet unexplained. In addition to the data on individual-level covariates used in this analysis (age, sex, smoking, BMI, comorbidities, and diet), additional individual-level data has been collected on this cohort including: marital status, allergies, physical activity, sedentary activity, and self-reported chronic pain. Employment status data is available (e.g., working full time, retired), but detailed occupation data is not available for this cohort.
Psychological stress may also play a role in the pathway through which lower SES leads to shortened telomeres. Many studies have shown that lower SES at the individual-level and neighborhood-level is associated with a greater level of stress.57–59 Support for this relationship has been strengthened by evidence that lower SES is related to higher levels of stress hormones cortisol, epinephrine, and norepinephrine.60 Furthermore, increased psychological stress has been associated with shorter TL.27–32,61 Both perceived stress and chronicity of stress have been significantly associated with higher oxidative stress,61 and oxidative stress has been linked to shorter TL.23–25 A future study could evaluate this mechanism further by conducting a mediation analysis that estimates the indirect effect of a measure of psychological stress acting as a fraction of the total effect of neighborhood SES on TL to gain further insight into the potential role of psychological stress may play in the pathway through which lower SES leads to shortened telomeres.
Strengths and limitations
This study has a number of strengths and limitations. Our study population was large, with substantially more participants than all previous studies of SES and TL combined. A limitation is that our study lacked racial and ethnic diversity by only including non-Hispanic whites. However, most previous studies of education level and TL also lacked diversity, with study populations that were mostly white drawn from the United States or the United Kingdom. Furthermore, only two previous studies of neighborhood SES and TL have been published previously. Thus, our findings from this large study of non-Hispanic whites add substantial knowledge to this understudied research question. Further studies including populations with more racial and ethnic diversity are needed to understand whether these findings among non-Hispanic whites are generalizable to other populations or whether these relationships vary by race/ethnicity.
Study participants were KPNC members who resided in Northern California. Most study subjects were also highly educated, where only a small percentage of study subjects had less than high school education. These factors could limit the generalizability to other populations. However, the KPNC population is community-based, and members are insured through employer-based plans, Medicare and Medicaid. In addition, comparisons of KP members to that of the CA population living in the same counties have shown that KPNC members have shown similar profiles across demographic, ethnic and SES, and self-reported health behaviors, with the exception of slightly higher median incomes among KPNC members (65% vs. 58% with >$35,000 annual household income, respectively) and slightly lower proportion of KPNC members living in high-poverty neighborhoods compared to the general population (8.2 vs. 9.9%, respectively).62,63
TL was measured in a single laboratory using a uniform, redundant and robust assay, conducted with a high level of quality control and extensive quality evaluation, which is a strength of our study. Most previous studies have used leukocyte TL measured from blood samples whereas our study obtained TL measures from saliva samples, which could make direct comparisons or TL results across studies more difficult to interpret. However, up to 74% of the DNA in saliva derives from leukocytes,64 which suggests that results obtained from saliva samples would demonstrate characteristics comparable to blood-derived DNA. This study focuses on a plausible biological mechanism by which SES may act through psychological stress to shorten telomeres.
We focused on previously established measures of individual-level and neighborhood-level SES: education level and the NDI. Education level has been widely used as a measure of individual-level SES in previous research. Previous studies have used the NDI or similar measures that combine several census variables using PCs analysis to measure neighborhood SES. The NDI is a weighted and standardized linear combination of a set of eight census variables where the weights are determined by the PCs method. Thus, the weights vary from study to study depending on the underlying joint distribution of those census variables within the region studied. Many previous studies have not published the weights used to create their neighborhood SES measure, nor have they published the correlations between the overall neighborhood SES measure with the individual census variables, making comparisons across studies more difficult. We have used a previously established measure of NDI, and we have provided additional information on the characteristics of the NDI in this study to aid in interpretation.
TL was measured at only one-time point for each study participant in this cross-sectional study. Although cross-sectional studies have inherent limitations in establishing temporal sequence of exposure and outcome, this study uses measures of past education level and neighborhood characteristics at home addresses where participants had often lived for many years. On average subjects had lived at their home address for 10.1 years preceding the date that the saliva was collected to measure TL (Table 1), and results of our sensitivity analysis showed that estimated effect sizes were slightly larger when restricting to subjects who lived at their current address for at least 5 years. Similarly, given the mean age of 63.9 in this cohort, the highest education level reported by each subject is likely to have occurred decades before the measurement of the TL outcome. Still, as with any cross-sectional study, we cannot completely rule out the possibility of reverse causation for NDI where subjects with shorter TL moved to low-SES neighborhoods. This issue could be addressed in future studies that collect longitudinal measurements of TL repeated over many years.
Since TL is considered a marker of aging, we can gain some further insight into the interpretation of the effects sizes of neighborhood and individual-level SES on TL in relation to the effect size of age on TL. Our effect estimate for a 1-SD change NDI on TL translates to approximately 2 years of aging, so the difference of very high NDI and very low NDI (4-SDs) translates to approximately 8 years of aging. For education, the difference of a high school education and a college education translates to approximately 7 years of aging, and the difference of less than high school education as compared to college education translates to approximately 14 years of aging.
This study examined the relationship of individual-level and neighborhood-level SES to TL among 84,996 non-Hispanic white subjects in the GERA cohort. We found that lower education levels were associated with shorter TL and that greater neighborhood socioeconomic deprivation was associated with shorter TL. We found that both individual-level and neighborhood-level SES have independent effects on TL. We found no differences by sex. Further research is needed to understand how these measures of individual-level and neighborhood-level SES relate to psychological stress and the cellular aging process so that these associations with TL can be better understood.
ACKNOWLEDGMENTS
We thank the Kaiser Permanente Northern California members who have generously agreed to participate in the Research Program on Genes, Environment and Health.
Supplementary Material
Footnotes
Published online 1 May 2019
Supplemental digital content is available through direct URL citations in the HTML and PDF versions of this article (www.environepidem.com).
S.E.A., C.A.S., E.J., L.C.S., C.P.Q., and S.K.V. are employees of The Permanente Medical Group. All other authors declare they have no actual or potential competing financial interests.
References
- 1.Blackburn EH. Telomeres and telomerase: the means to the end (Nobel lecture). Angew Chem Int Ed Engl 2010497405–7421 [DOI] [PubMed] [Google Scholar]
- 2.Greider CW. Telomerase discovery: the excitement of putting together pieces of the puzzle (Nobel lecture). Angew Chem Int Ed Engl 2010497422–7439 [DOI] [PubMed] [Google Scholar]
- 3.Szostak JW. DNA ends: just the beginning (Nobel lecture). Angew Chem Int Ed Engl 2010497386–7404 [DOI] [PubMed] [Google Scholar]
- 4.von Zglinicki T, Martin-Ruiz CM. Telomeres as biomarkers for ageing and age-related diseases. Curr Mol Med 20055197–203 [DOI] [PubMed] [Google Scholar]
- 5.Blackburn EH, Epel ES, Lin J. Human telomere biology: a contributory and interactive factor in aging, disease risks, and protection. Science 20153501193–1198 [DOI] [PubMed] [Google Scholar]
- 6.Bakaysa SL, Mucci LA, Slagboom PE, et al. Telomere length predicts survival independent of genetic influences. Aging Cell 20076769–774 [DOI] [PubMed] [Google Scholar]
- 7.Cawthon RM, Smith KR, O’Brien E, Sivatchenko A, Kerber RA. Association between telomere length in blood and mortality in people aged 60 years or older. Lancet 2003361393–395 [DOI] [PubMed] [Google Scholar]
- 8.Fitzpatrick AL, Kronmal RA, Kimura M, et al. Leukocyte telomere length and mortality in the Cardiovascular Health Study. J Gerontol A Biol Sci Med Sci 201166421–429 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Epel ES, Merkin SS, Cawthon R, et al. The rate of leukocyte telomere shortening predicts mortality from cardiovascular disease in elderly men. Aging (Albany NY) 2008181–88 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Mainous AG, III, Codd V, Diaz VA, et al. Leukocyte telomere length and coronary artery calcification. Atherosclerosis 2010210262–267 [DOI] [PubMed] [Google Scholar]
- 11.Farzaneh-Far R, Lin J, Epel E, Lapham K, Blackburn E, Whooley MA. Telomere length trajectory and its determinants in persons with coronary artery disease: longitudinal findings from the heart and soul study. PLoS One 20105e8612. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Hoffmann J, Spyridopoulos I. Telomere length in cardiovascular disease: new challenges in measuring this marker of cardiovascular aging. Future Cardiol 20117789–803 [DOI] [PubMed] [Google Scholar]
- 13.Prescott J, Wentzensen IM, Savage SA, De Vivo I. Epidemiologic evidence for a role of telomere dysfunction in cancer etiology. Mutat Res 201273075–84 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Wentzensen IM, Mirabello L, Pfeiffer RM, Savage SA. The association of telomere length and cancer: a meta-analysis. Cancer Epidemiol Biomarkers Prev 2011201238–1250 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Murillo-Ortiz B, Albarrán-Tamayo F, Arenas-Aranda D, et al. Telomere length and type 2 diabetes in males, a premature aging syndrome. Aging Male 20121554–58 [DOI] [PubMed] [Google Scholar]
- 16.Testa R, Olivieri F, Sirolla C, et al. Leukocyte telomere length is associated with complications of type 2 diabetes mellitus. Diabet Med 2011281388–1394 [DOI] [PubMed] [Google Scholar]
- 17.Goronzy JJ, Fujii H, Weyand CM. Telomeres, immune aging and autoimmunity. Exp Gerontol 200641246–251 [DOI] [PubMed] [Google Scholar]
- 18.Georgin-Lavialle S, Aouba A, Mouthon L, et al. The telomere/telomerase system in autoimmune and systemic immune-mediated diseases. Autoimmun Rev 20109646–651 [DOI] [PubMed] [Google Scholar]
- 19.Sanders JL, Iannaccone A, Boudreau RM, et al. ; Health ABC Study The association of cataract with leukocyte telomere length in older adults: defining a new marker of aging. J Gerontol A Biol Sci Med Sci 201166639–645 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Savale L, Chaouat A, Bastuji-Garin S, et al. Shortened telomeres in circulating leukocytes of patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2009179566–571 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Barceló A, Piérola J, López-Escribano H, et al. Telomere shortening in sleep apnea syndrome. Respir Med 20101041225–1229 [DOI] [PubMed] [Google Scholar]
- 22.Prather AA, Puterman E, Lin J, et al. Shorter leukocyte telomere length in midlife women with poor sleep quality. J Aging Res 20112011721390. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Uziel O, Reshef H, Ravid A, et al. Oxidative stress causes telomere damage in Fanconi anaemia cells—a possible predisposition for malignant transformation. Br J Haematol 200814282–93 [DOI] [PubMed] [Google Scholar]
- 24.Kurz DJ, Decary S, Hong Y, Trivier E, Akhmedov A, Erusalimsky JD. Chronic oxidative stress compromises telomere integrity and accelerates the onset of senescence in human endothelial cells. J Cell Sci 2004117pt 112417–2426 [DOI] [PubMed] [Google Scholar]
- 25.von Zglinicki T. Oxidative stress shortens telomeres. Trends Biochem Sci 200227339–344 [DOI] [PubMed] [Google Scholar]
- 26.O’Donovan A, Pantell MS, Puterman E, et al. ; Health Aging and Body Composition Study Cumulative inflammatory load is associated with short leukocyte telomere length in the Health, Aging and Body Composition Study. PLoS One 20116e19687. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Drury SS, Theall K, Gleason MM, et al. Telomere length and early severe social deprivation: linking early adversity and cellular aging. Mol Psychiatry 201217719–727 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Entringer S, Epel ES, Kumsta R, et al. Stress exposure in intrauterine life is associated with shorter telomere length in young adulthood. Proc Natl Acad Sci U S A 2011108E513–E518 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Epel ES. Psychological and metabolic stress: a recipe for accelerated cellular aging? Hormones (Athens) 200987–22 [DOI] [PubMed] [Google Scholar]
- 30.Kananen L, Surakka I, Pirkola S, et al. Childhood adversities are associated with shorter telomere length at adult age both in individuals with an anxiety disorder and controls. PLoS One 20105e10826. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Surtees PG, Wainwright NW, Pooley KA, et al. Life stress, emotional health, and mean telomere length in the European Prospective Investigation into Cancer (EPIC)-Norfolk population study. J Gerontol A Biol Sci Med Sci 2011661152–1162 [DOI] [PubMed] [Google Scholar]
- 32.Hanssen LM, Schutte NS, Malouff JM, Epel ES. The relationship between childhood psychosocial stressor level and telomere length: a meta-analysis. Health Psychol Res 201756378. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Mackenbach JP, Bakker MJ; European Network on Interventions and Policies to Reduce Inequalities in Health Tackling socioeconomic inequalities in health: analysis of European experiences. Lancet 20033621409–1414 [DOI] [PubMed] [Google Scholar]
- 34.Dow WH, Rehkopf DH. Socioeconomic gradients in health in international and historical context. Ann N Y Acad Sci 2010118624–36 [DOI] [PubMed] [Google Scholar]
- 35.Singh GK, Siahpush M. Widening socioeconomic inequalities in US life expectancy, 1980–2000. Int J Epidemiol 200635969–979 [DOI] [PubMed] [Google Scholar]
- 36.Diez Roux AV, Mair C. Neighborhoods and health. Ann N Y Acad Sci 20101186125–145 [DOI] [PubMed] [Google Scholar]
- 37.Meijer M, Röhl J, Bloomfield K, Grittner U. Do neighborhoods affect individual mortality? A systematic review and meta-analysis of multilevel studies. Soc Sci Med 2012741204–1212 [DOI] [PubMed] [Google Scholar]
- 38.Wight RG, Cummings JR, Karlamangla AS, Aneshensel CS. Urban neighborhood context and mortality in late life. J Aging Health 201022197–218 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Adams JM, White M. Biological ageing: a fundamental, biological link between socio-economic status and health? Eur J Public Health 200414331–334 [DOI] [PubMed] [Google Scholar]
- 40.Robertson T, Batty GD, Der G, Fenton C, Shiels PG, Benzeval M. Is socioeconomic status associated with biological aging as measured by telomere length? Epidemiol Rev 20133598–111 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Needham BL, Carroll JE, Diez Roux AV, Fitzpatrick AL, Moore K, Seeman TE. Neighborhood characteristics and leukocyte telomere length: the Multi-Ethnic Study of Atherosclerosis. Health Place 201428167–172 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Park M, Verhoeven JE, Cuijpers P, Reynolds CF, III, Penninx BW. Where you live may make you old: the association between perceived poor neighborhood quality and leukocyte telomere length. PLoS One 201510e0128460. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Banda Y, Kvale MN, Hoffmann TJ, et al. Characterizing race/ethnicity and genetic ancestry for 100,000 subjects in the Genetic Epidemiology Research on Adult Health and Aging (GERA) cohort. Genetics 20152001285–1295 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Lapham K, Kvale MN, Lin J, et al. Automated assay of telomere length measurement and informatics for 100,000 subjects in the Genetic Epidemiology Research on Adult Health and Aging (GERA) cohort. Genetics 20152001061–1072 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Kvale MN, Hesselson S, Hoffmann TJ, et al. Genotyping informatics and quality control for 100,000 subjects in the genetic epidemiology research on adult health and aging (GERA) cohort. Genetics 20152001051–1060 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Messer LC, Laraia BA, Kaufman JS, et al. The development of a standardized neighborhood deprivation index. J Urban Health 2006831041–1062 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Cawthon RM. Telomere measurement by quantitative PCR. Nucleic Acids Res 200230e47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Hastie TJ, Tibshirani RJ. Generalized Additive Models, Volume 43 of Monographs on Statistics and Applied Probability 1990London, United Kingdom: Chapman & Hall [Google Scholar]
- 49.Needham BL, Adler N, Gregorich S, et al. Socioeconomic status, health behavior, and leukocyte telomere length in the National Health and Nutrition Examination Survey, 1999–2002. Soc Sci Med 2013851–8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Ross CE, Mirowsky J. Neighborhood disadvantage, disorder, and health. J Health Soc Behav 200142258–276 [PubMed] [Google Scholar]
- 51.Baker MH, Nienstedt BC, Everett RS, McCleary R. The impact of a crime wave: perceptions, fear, and confidence in the police. Law Soc Rev 198317319–335 [Google Scholar]
- 52.Angell M. Privilege and health—what is the connection? N Engl J Med 1993329126–127 [DOI] [PubMed] [Google Scholar]
- 53.Whitehead M. The concepts and principles of equity and health. Health Promot Int 19916217–228 [Google Scholar]
- 54.Adler NE, Stewart J. Health disparities across the lifespan: meaning, methods, and mechanisms. Ann N Y Acad Sci 201011865–23 [DOI] [PubMed] [Google Scholar]
- 55.Batty GD, Wang Y, Brouilette SW, et al. Socioeconomic status and telomere length: the West of Scotland Coronary Prevention Study. J Epidemiol Community Health 200963839–841 [DOI] [PubMed] [Google Scholar]
- 56.Taylor A, Jacques PF, Epstein EM. Relations among aging, antioxidant status, and cataract. Am J Clin Nutr 1995626 suppl1439S–1447S [DOI] [PubMed] [Google Scholar]
- 57.Lantz PM, House JS, Mero RP, Williams DR. Stress, life events, and socioeconomic disparities in health: results from the Americans’ Changing Lives Study. J Health Soc Behav 200546274–288 [DOI] [PubMed] [Google Scholar]
- 58.McLeod JD, Kessler RC. Socioeconomic status differences in vulnerability to undesirable life events. J Health Soc Behav 199031162–172 [PubMed] [Google Scholar]
- 59.Matthews KA, Räikkönen K, Everson SA, et al. Do the daily experiences of healthy men and women vary according to occupational prestige and work strain? Psychosom Med 200062346–353 [DOI] [PubMed] [Google Scholar]
- 60.Cohen S, Doyle WJ, Baum A. Socioeconomic status is associated with stress hormones. Psychosom Med 200668414–420 [DOI] [PubMed] [Google Scholar]
- 61.Epel ES, Blackburn EH, Lin J, et al. Accelerated telomere shortening in response to life stress. Proc Natl Acad Sci U S A 200410117312–17315 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Gordon N, Lin T. The Kaiser Permanente Northern California adult member health survey. Perm J 20162015–225 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Krieger N. Overcoming the absence of socioeconomic data in medical records: validation and application of a census-based methodology. Am J Public Health 199282703–710 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Thiede C, Prange-Krex G, Freiberg-Richter J, Bornhäuser M, Ehninger G. Buccal swabs but not mouthwash samples can be used to obtain pretransplant DNA fingerprints from recipients of allogeneic bone marrow transplants. Bone Marrow Transplant 200025575–577 [DOI] [PubMed] [Google Scholar]