

Abstract
Despite rapid growth in the empirical research on behavior change, modern science has yet to produce a coherent set of recommendations for individuals and organizations eager to align everyday actions with enduringly valued goals. We propose the process model of behavior change as a parsimonious framework for organizing strategies according to where they have their primary impact in the generation of behavioral impulses. To begin, individuals exist in objective situations, only certain features of which attract attention, which in turn lead to subjective appraisals, then finally give rise to response tendencies. Unhealthy habits develop when conflicting impulses are consistently resolved in favor of momentary temptations instead of valued goals. To change behavior for the better, we can strategically modify objective situations, where we pay attention, how we construct appraisals, and how we enact responses. Crucially, behavior change strategies can be initiated either by the individual (i.e., self-control) or by others (e.g., a benevolent employer).
Keywords: behavior change, health, goals, self-control, nudges, process model, incentives, motivation
Behavior change can be astonishingly difficult. For example, although the long-term benefits of physical activity, a balanced diet, and abstaining from smoking are well-known, failures to enact healthy behavior account for nearly half of premature deaths in the United States (National Research Council, 2010; Schroeder, 2007). We may resolve to take the stairs at work but then take the elevator instead. We may wish our afternoon snack were an apple but then find ourselves eating potato chips. We may promise our doctor we’ll get a flu shot and then neglect to do so. Why do so many of us who “know better” regularly succumb to unhealthy temptations?
When we fail to make healthy choices, it is common to blame lapses in willpower (American Psychological Association, 2012). But brute force suppression of impulses is nearly impossible to sustain (Cohen, 2005) and dramatically less efficient than more strategic approaches to self-control (Duckworth, Gendler, & Gross, 2016). Moreover, changing behavior for the better depends not only on our individual capacity to regulate impulses, but also on the ecosystems in which we operate—including shared structural affordances and impediments, social norms, culture-wide practices, and more (Bronfenbrenner, 1979; Klein, Austin, & Cooper, 2008; Lewin, 1939). In other words, successful behavior change calls for both self-initiated and other-initiated strategies.
There is no shortage of empirical insights on volitional behavior change, and yet scientific progress on this important topic has not been cumulative (Nielsen et al., 2018; Sheeran, Klein, & Rothman, 2017). Why not? One reason is that scientists working in different theoretical traditions tend to publish in different academic journals and attend different academic conferences. Likewise, journal articles are often indexed by target behaviors (e.g., physical activity, retirement savings, substance abuse) rather than shared underlying mechanisms. And finally, research on self-control—by definition, self-initiated goal-congruent behavior change—rarely makes contact with research on incentives, nudges, and other behavior change solutions initiated by organizations and policy makers. In this article, we suggest that a process-based approach can organize and integrate findings on human behavior change from diverse research traditions.
Goals and Goal Conflict
There are many reasons we might fail to make desirable changes to our behavior. For instance, we may lack the requisite information (e.g., eating fruits and vegetables is healthy) or skill (e.g., how to cook). But failures of behavior change can persist even when we know what we should do and how to do it. Nutritional literacy campaigns, for example, have increased public awareness of the health benefits of fruits and vegetables without concomitant increases in consumption (Wood & Neal, 2016). Likewise, many healthy behaviors (e.g., drinking water instead of soda) require no specialized skills. Our focus in this article is on how individuals and organizations can facilitate behavior change when information or specialized skill is not the issue.
Though there may be secondary benefits to the broader organization (e.g., lower healthcare costs) (Kessler & Zhang, 2015), volitional behavior change primarily concerns behaviors that individuals themselves prefer, upon reflection, to their status quo. To illustrate, Figure 1 depicts the conflict between taking the stairs, a new and preferred behavior, and taking the elevator, an established behavior that is momentarily more gratifying. Across theoretical traditions, various terms have been used to capture the tension between goals we recognize as more valuable and goals that are nevertheless more tempting in the moment: shoulds versus wants (Milkman, Rogers, & Bazerman, 2008); planner versus doer (Thaler & Shefrin, 1981); cool versus hot systems (Metcalfe & Mischel, 1999); reflective versus impulsive precursors of behavior (Hofmann, Friese, & Strack, 2009); and second-order versus first-order desires (Frankfurt, 1988).
Figure 1.
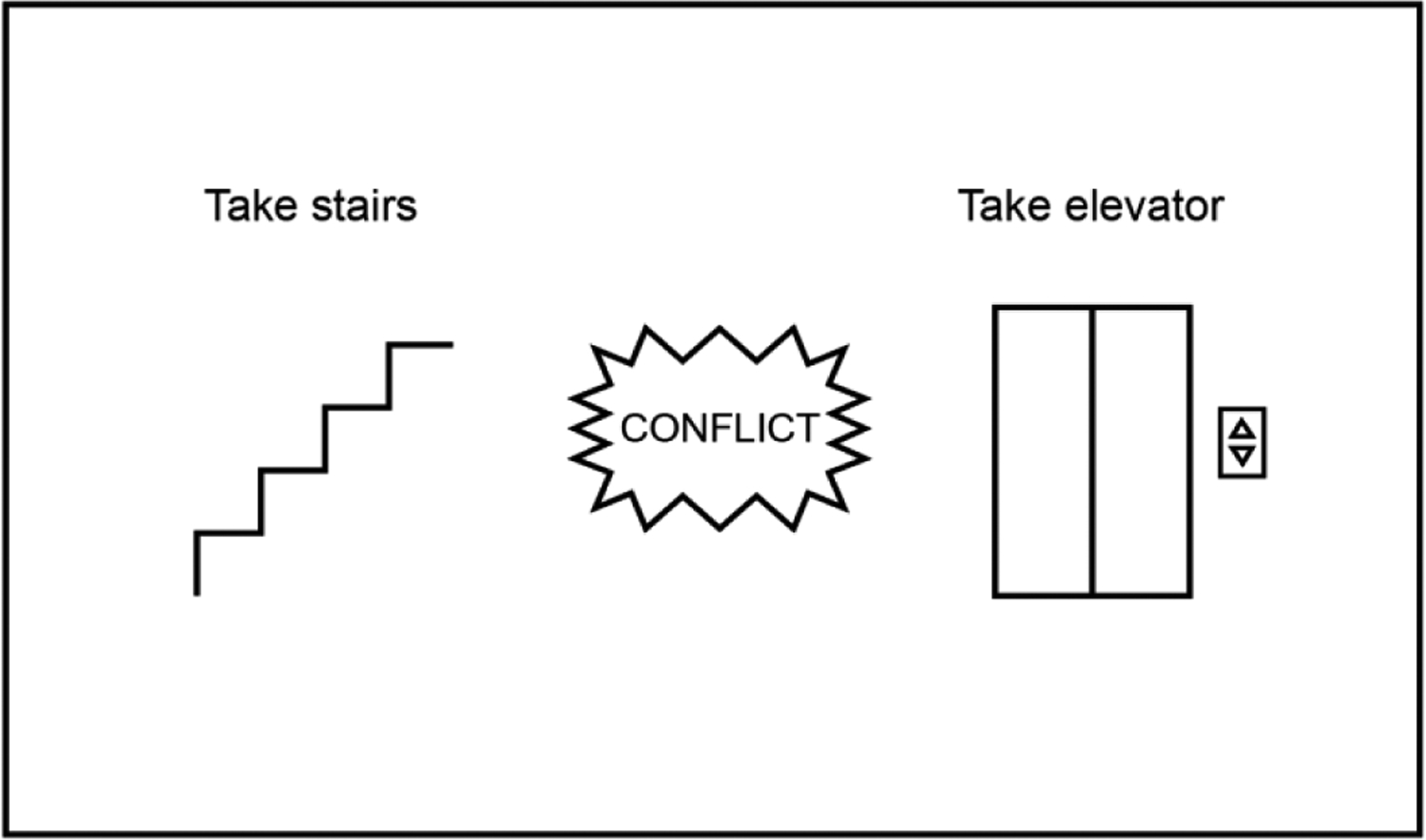
Taking the stairs is a behavior that advances the enduringly valued goal to increase physical activity. In contrast, taking the elevator is a behavior that advances the momentarily more rewarding goal to be comfortable. These goals conflict insofar as it is impossible to both take the stairs and the elevator at the same time.
Why don’t such goal conflicts resolve spontaneously in favor of the behavior that, upon reflection, we know is better for us in the long run? One explanation is present bias, the tendency to care more about our current experiences than about what might happen to us in the future (Ainslie, 2001; Laibson, 2001). Of course, future goals can lack psychological potency for other reasons, including being more abstract (versus concrete) and probabilistic (versus certain) than rewards in the here-and-now (Liberman & Trope, 2014). Further, since affective states vary over time and the future is less vivid than the present, it can be difficult for our “present self” to empathize or feel continuity with our “future self” (Bartels & Urminsky, 2011; Hershfield & Bartels, 2018; Sayette, Loewenstein, Griffin, & Black, 2008). Likewise, it is easy to imagine that our future self will take the stairs on all future days, thereby licensing the present self to take the elevator now—when, in fact, such overly optimistic projections are unlikely.
Another explanation is synchronous ambivalence between two “present selves” whose preferences differ. For instance, it is entirely possible to aspire to be more physically active and, at the very same time, crave comfort. As the poet Walt Whitman observed in “Song of Myself,” the self is not unitary:
Do I contradict myself?
Very well then I contradict myself,
(I am large, I contain multitudes.)
(1904, p. 69)
The idea that at any point in time, an individual encompasses multiple desires has deep roots in both philosophy (Plato, 380 BCE/1992) and psychology (Freud, 1916–1917/1977). More recently, brain imaging studies affirm the existence of distinct valuation systems, each with differential sensitivity to the same choice sets (Berkman, Hutcherson, Livingston, Kahn, & Inzlicht, 2017; Kable, 2014). Moreover, it is possible for a desirable new behavior to conflict with entrenched habits. As psychotherapists are fond of pointing out, we often yearn for change yet cling to the familiar (Burns, January/February 2013).
How Behavioral Impulses Are Generated
Understanding how behavior can be changed begins with understanding how behavior is generated in the first place. The process model of behavior change posits that all impulses to act, think, or feel in a certain way—regardless of whether they are good for us in the long run or merely satisfy momentary desires—are response tendencies that develop over the course of moments to minutes in qualitatively distinct stages (Duckworth, Gendler, & Gross, 2016). Specifically, as suggested in Figure 2, impulses evolve in a recursive (but one-way) cycle that may or may not include the active appraisal of our options. When impulses reach a certain threshold, they are enacted. These behavioral responses, in turn, may change our situation, which can redirect our attention, and so on.
Figure 2.
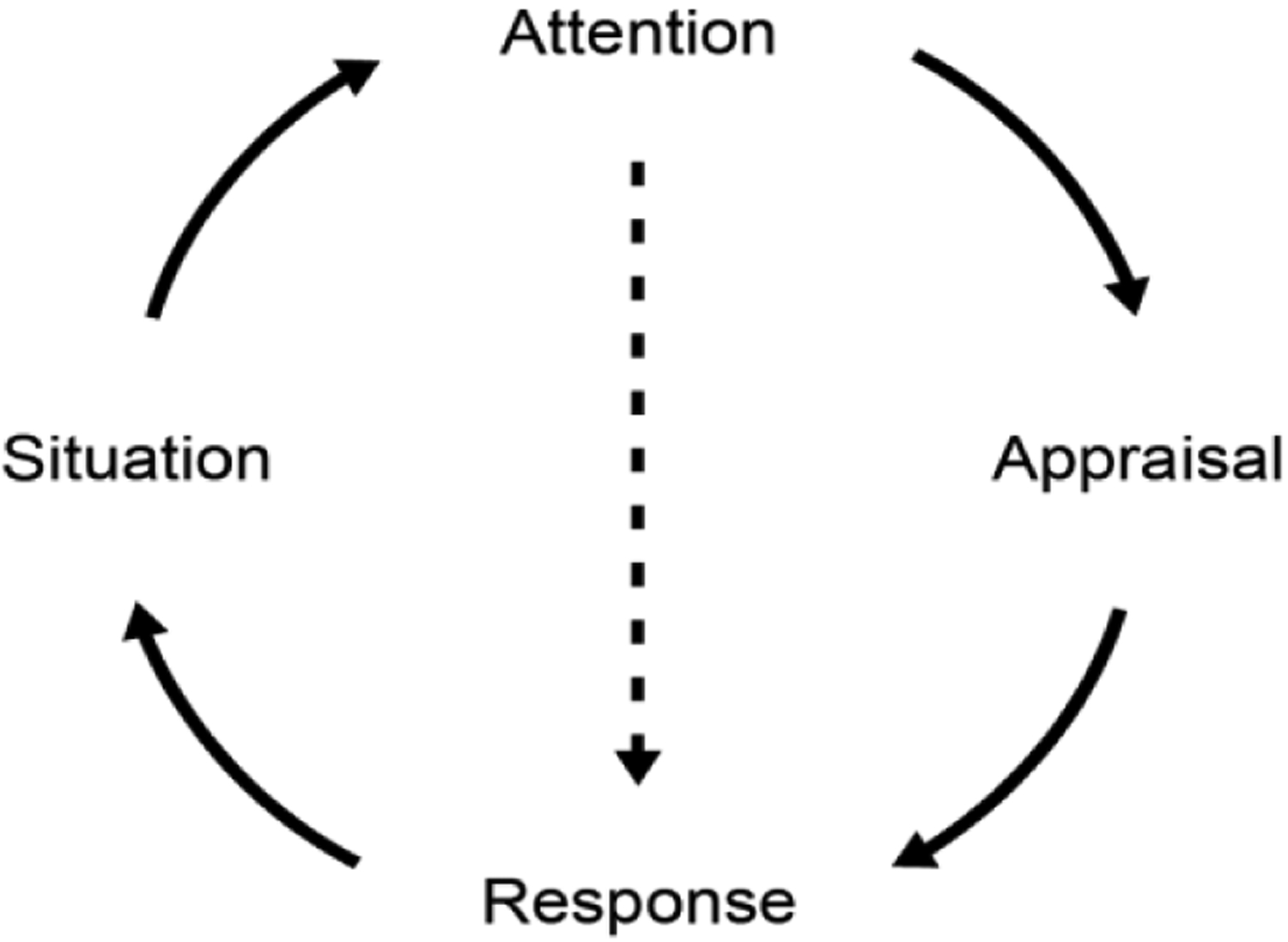
The process model of behavior change posits that behavioral responses are the outcome of a recursive cycle in which features of our objective situation are selected for attention and appraisal, which then may lead to a response. In the case of plans, personal rules, and habits, the perception of a situational cue may trigger a response directly, bypassing the appraisal stage, as indicated by the dotted line.
In its earliest iteration, the process model was introduced in the emotion regulation literature (Gross, 1998). Subsequently, the process model was extended to other domains in which individuals struggle to exercise self-control, including schoolwork (Duckworth, Gendler, & Gross, 2014), eating and exercise, substance use, and retirement savings (Duckworth, Gendler, & Gross, 2016). The expansion to domains and response types other than emotion accords with evidence that self-control varies across domains and yet, across these diverse contexts, shares common psychological processes (Duckworth & Tsukayama, 2015). In this article, we further extend the process model, showing how we can organize behavior change strategies initiated by others (e.g., an employer) according to the same underlying processes that are targeted by individuals themselves. In this exposition, we also elaborate strategies for short-circuiting the cycle of impulse generation by circumventing appraisals and directly responding to salient cues in our situation.
As a starting point, the process model of behavior change begins with the commonsense observation that our choices are influenced by the objective situation. Most obviously, our situation includes all of its physical features, but social influences are also paramount (Ross & Nisbett, 1991). It is impossible to be consciously aware of more than a tiny fraction of situational features at any given moment (Kahneman, 1973; Pashler & Johnston, 2016). Thus, the second stage entails paying attention to certain features of our situation and ignoring others. Our attentional spotlight can also toggle inward, activating a subset of memories, schema, or mental representations while leaving the rest inactive. We then construct appraisals: subjective interpretations of the subset of features that have entered awareness. Appraisals determine the expected value (i.e., the net anticipated benefits and costs) of potential responses to our situation (Ajzen, 1991; Bandura, 1977). These calculations are typically nonconscious and certainly need not be accurate, but they are nevertheless rational in the sense that their purpose is to enable choices that optimize net expected value (i.e., expected benefits minus expected costs). Appraisals in turn give rise to response tendencies that, upon reaching a certain threshold, are enacted as behavioral responses. Whether they take the form of manifest actions (e.g., picking up a candy bar), thoughts (e.g., “I’m never going to lose weight, anyway”), emotions (e.g., anger), or somatic states (e.g., fatigue), these responses can change our objective situation, thereby starting the cycle anew.
Although this is a fairly common way for impulses to be generated, we don’t always take the time to evaluate our options and deliberate about what to do. Instead, situational cues sometimes enter our awareness and immediately produce a behavioral response that circumvents the appraisal stage. This is most obvious in the case of habits—automatic responses that have previously been repeated and rewarded in the same context over extended time periods—and indeed, more than a third of our daily behaviors are thought to be habitual (Wood, Quinn, & Kashy, 2002). In contrast to goal-directed responses, habitual responses economize on cognitive effort and are enacted not because we calculate that their net benefits minus costs are optimal in the moment but rather because we have responded the same way in the same context and gotten a similar reward many times over in the past.
In the context of the process model, the idea that an individual “contains multitudes,” each with its own distinctive preferences or habits, plays out as follows: at any point in time, multiple situation-attention-appraisal-response or situation-attention-response loops may be in motion at once (Ochsner & Gross, 2014). Very often, the behavioral responses produced by these cycles are compatible (Hofmann, Baumeister, Förster, & Vohs, 2012). For instance, we can climb the stairs, furthering the goal of increasing our daily activity, while at the same time chatting with a co-worker who is also taking the stairs, furthering the goal of social bonding. However, as we elaborate in the next section, these behavior generation cycles can sometimes come into conflict (Hofmann et al., 2012).
When Behavioral Impulses Conflict
As illustrated in Figure 3, desirable behavioral impulses are not always compatible with less desirable behavioral impulses that are nevertheless more potent in the moment. Imagine, for example, standing in the office lobby and needing to get to a meeting on the second floor. We might glance toward the stairwell and remind ourselves of a New Year’s resolution to get more exercise, leading to an appraisal of the stairs as a way to enact that goal, thus strengthening the impulse to take the stairs. At the very same time, however, we may experience a conflicting impulse to take the elevator. We may, for example, turn to look at the elevator and realize how tired we feel, leading to an appraisal of the elevator as a way to maximize comfort, thus strengthening the impulse to take the elevator.
Figure 3.
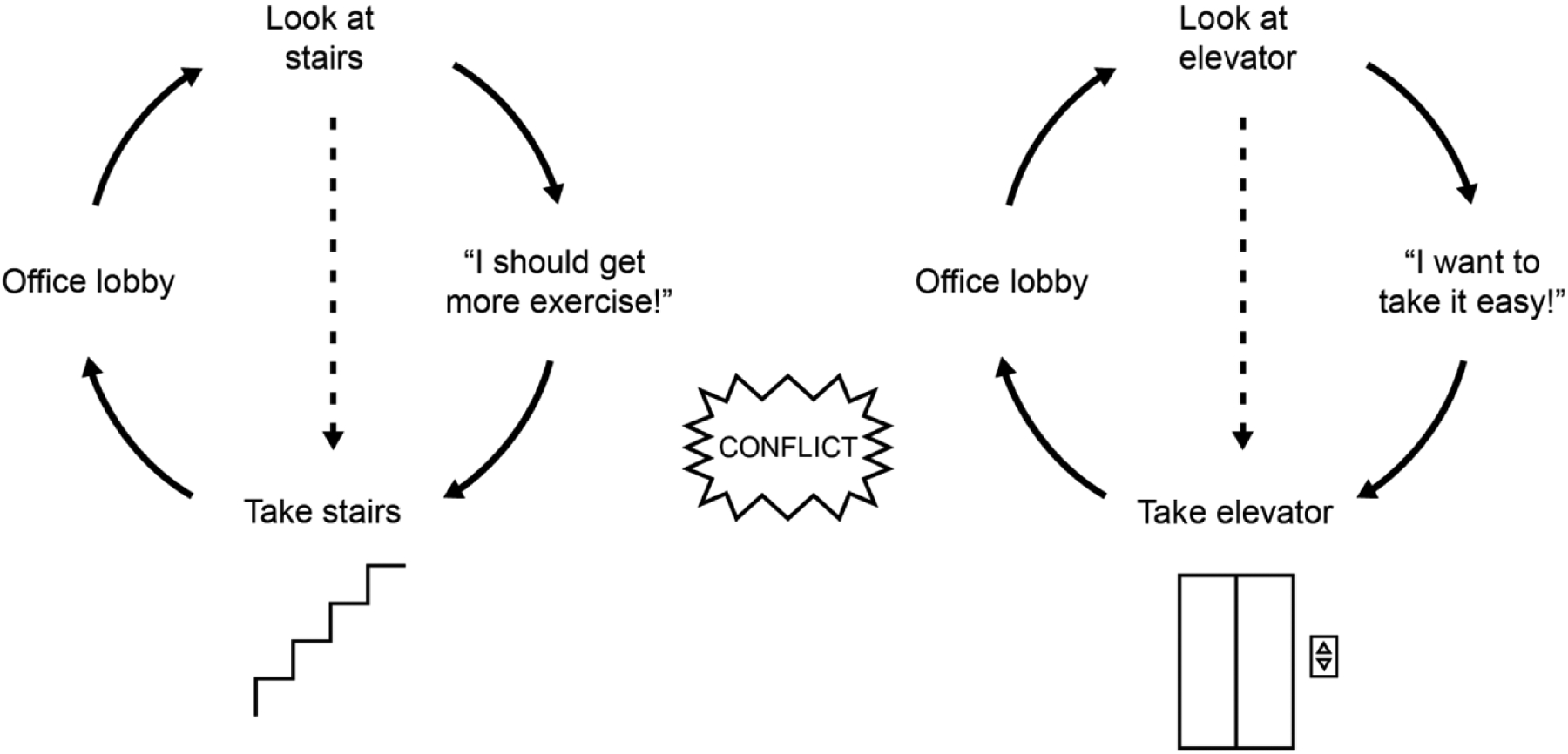
The recursive cycles that generate behavior can come into conflict. For example, it is possible to experience, at the very same time, the impulse to take the stairs and the impulse to take the elevator.
More immediately rewarding impulses tend to win out over impulses whose rewards are delayed (Rachlin, 2000; Sullivan, Hutcherson, Harris, & Rangel, 2014), and it is therefore likely in this scenario that we will take the elevator despite the sincere conviction that taking the stairs is the preferable choice. Importantly, how we adjudicate a single instance of goal conflict not only determines how we behave in the moment but also influences how we will behave in the future (Rachlin, 2000). For example, if today we choose to take the elevator and are rewarded by making it to our meeting with minimal effort, then we may be slightly more inclined to make the same choice the next day. Gradually, we might form a habit of taking the elevator. In contrast, if we instead choose to take the stairs today, we might be more inclined to make the same choice the next day, and again the next, gradually developing a healthy habit of taking the stairs.
Because in-the-moment skirmishes can favor unhealthy impulses, behavior change requires thinking ahead. Prospection, the mental representation of possible futures (Gilbert & Wilson, 2007; Seligman, Railton, Baumeister, & Sripada, 2016), makes it possible for individuals and organizations to form goals—imagined futures that are by definition more desirable than the status quo. A recent meta-analysis found that, across domains, when individuals set specific goals, they are more successful at enacting behavior change, particularly when goals are challenging, shared publicly, and specified for group (versus individual) targets (Epton, Currie, & Armitage, 2017). Likewise, organizations perform better when they set specific, challenging goals (Smith, Locke, & Barry, 1990). Of course, not all forms of prospection are equally conducive to behavior change. Indulging in positive fantasies about what it will be like to achieve our personal goals without anticipating reasons why we may not succeed can actually decrease motivation to change (Oettingen & Gollwitzer, 2018). Similarly, it is unwise for organizations to elaborate the benefits of a new initiative without also conducting a “premortem” (Klein, 2007) analysis of what could go wrong. For both individuals and organizations, therefore, optimal goal setting entails mentally contrasting a vivid picture of the desired future with specific obstacles that currently stand in the way (Oettingen & Gollwitzer, 2018).
How to Change Behavior
Whether undertaken by an individual or a broader organization, there are many ways to bring about behavior change. One recent review identified 93 discrete behavior change tactics (Michie et al., 2013); a compendium grounded in community-based participatory research identified 99 techniques (Kok et al., 2016); another catalogue restricted to what individuals can enact on their own identified 123 separate self-initiated techniques (Knittle et al., 2020); and a “very short guide” to nudges for policymakers lists no fewer than 10 different options for other-initiated change (Sunstein, 2014). As Schelling (1978) observed, there is no end to the “little tricks” that can be deployed to help us “do the things we ought to do or to keep us from the things we ought to foreswear” (p. 290).
As shown in Figure 4, the process model suggests a more parsimonious framework that categorizes both self-initiated and other-initiated approaches according to the underlying process they aim to influence (i.e., the objective situation, where we pay attention, how we appraise what we’re perceiving, how we respond to this evaluation, or associative links between salient cues and responses).
Figure 4.
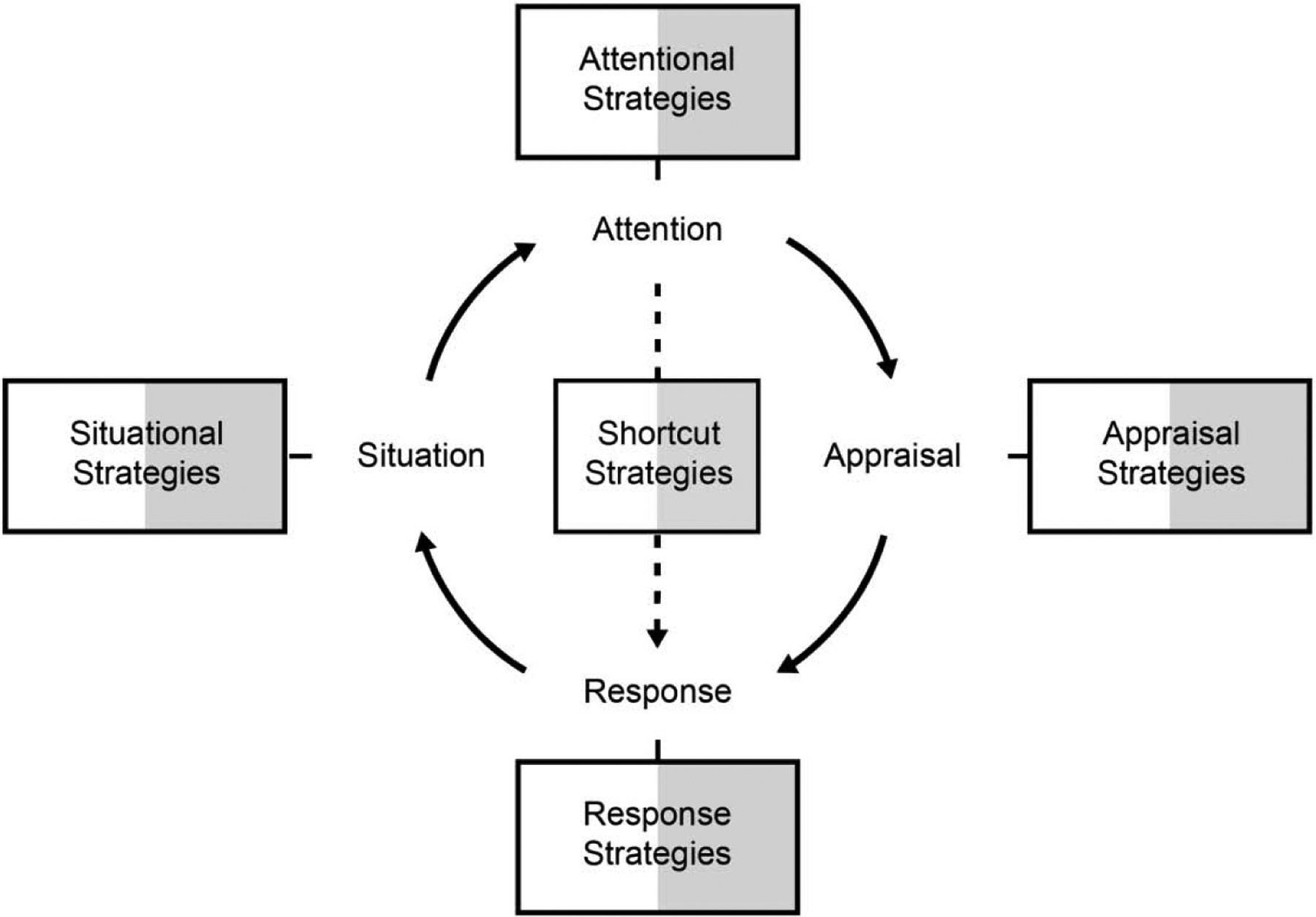
Behavior change can target any stage of impulse generation. Alternatively, it is possible to shortcut the appraisal stage altogether, as indicated by the dotted line. Strategies can be self-initiated (represented by the white-fill portion of each box) or other-initiated (e.g., by employers or policymakers; represented by the dark-fill portion of each box).
Many have found this framework to be useful, but it bears noting that the very nature of the recursive cycle we describe presents a challenge to classification. For instance, a company newsletter that highlights before/after stories of employees who have improved their fitness routines would be an “appraisal intervention” insofar as it aims to change social norms. However, the delivery of the newsletter itself is a change to the physical situation that in turn draws our attention to exemplars in our midst that we might otherwise have ignored. Likewise, incentives change the objective situation, but their ultimate effect is mediated by appraisals of the relative value of response options (Gneezy, Kajackaite, & Meier, in press).
One way to address the challenge to classification that this recursive cycle presents is to use the principle of substitutability: a target process is not substitutable, whereas what precedes or follows is. For example, targeting social norms is central to before/after stories but can also be accomplished via posters or a video shown at an annual meeting. Likewise, policymakers implementing incentive schemes may suspect a variety of cognitive mechanisms, but what is essential to their approach is a change in the objective situation.
Table 1 provides illustrative examples of strategies that an individual or organization can deploy in order to increase stair climbing and decrease using the elevator. Throughout the text and in Table 2, we suggest additional examples of process-targeted strategies for an array of other health-related behaviors, including sleeping, eating, and substance use. To foreground the similarities of self-initiated and other-initiated strategies, we now turn to a discussion of each process model category in turn, beginning with the earliest stage of impulse generation: the objective situation.
Table 1.
Examples of Self-Initiated Versus Other-Initiated Approaches to Encourage Physical Activity
| Target process | Self-initiated strategies | Other-initiated strategies |
|---|---|---|
| Situation | Wearing comfortable shoes to work; not carrying the elevator key | Installing artwork in stairwells; giving prizes to individuals or teams for increasing their step counts |
| Attention | Keeping track of the number of stairs climbed using a smartphone app | Sending text messages or emails reminding employees to minimize elevator use |
| Appraisal | Thinking about taking the stairs as an “energy break” | Publicizing injunctive norms: 90% of your coworkers say it’s better to take the stairs than the elevator |
| Response | Using willpower to just take the stairs | Banning elevator use |
| Shortcut | Having a personal rule: I always take the stairs | Instilling the custom: we always take the stairs |
Table 2.
Examples of Self-Initiated Versus Other-Initiated Behavior Change Approaches
| Target process | Self-initiated strategies | Other-initiated strategies |
|---|---|---|
| Situation | Setting an alarm for going to bed at the same time each night; packing healthy snacks to bring to work; keeping cell phone in a drawer to avoid disruptions during work day | Making fresh fruit available in common areas; offering free flu shots; providing fluoride rinse in bathrooms; cash bonuses for reaching step count targets |
| Attention | Keeping a food log; monitoring sleep quality using an activity tracker; looking away from desserts in the cafeteria | Sending text messages or emails reminding employees to eat healthy; posters reminding employees that it’s flu shot season |
| Appraisal | Thinking about smoking as inconsistent with company’s mission; thinking about exercise during the workday as a way to enhance overall job performance | Publicizing injunctive norms: 90% of your coworkers hope you get your flu shot ASAP; emphasizing prosocial aspects of behavior change: Washing your hands for 20 seconds helps your coworkers stay healthy |
| Response | Using willpower to resist ordering a cheeseburger and fries at lunch | Banning smoking |
| Shortcut | Having a personal rule: I always take 10,000 steps per day | Instilling the custom: Each November, we all participate in a charity walkathon |
Situational Strategies
Situational strategies take aim at our objective circumstances. As B. F. Skinner once quipped: “If you’re old, don’t try to change yourself, change your environment.” The process model unpacks this adage by showing that our physical and social circumstances matter because they have downstream effects on attention, appraisal, and behavior. It is therefore advantageous to proactively create situations that render desirable behaviors more salient, more rewarding, or easier to enact and/or make undesirable behaviors less salient, less rewarding, or more difficult (Duckworth et al., 2016).
Self-initiated situational strategies include commitment devices, contracts that create voluntary restrictions on future choices, most commonly by creating a penalty for failing to do as we intend (Bryan, Karlan, & Nelson, 2010; Rogers, Milkman, & Volpp, 2014). Hard commitments, such as taking Antabuse to avoid ingesting alcohol (Banys, 1988) or agreeing to pay a penalty if we start smoking (Giné, Karlan, & Zinman, 2010), exact tangible penalties for transgressions; soft commitments, such as posting New Year’s resolutions on social media, exact psychological penalties (Bryan et al., 2010). We can also take it upon ourselves to create positive contingencies for desired behavior. Temptation bundling, for example, entails committing to enjoy a pleasurable indulgence (e.g., listening to lowbrow television shows) only while simultaneously engaging in a behavior requiring self-control (e.g., running on the treadmill) (Milkman, Minson, & Volpp, 2014). Finally, we can make physical changes to our immediate surroundings—such as moving the office candy jar more than an arm’s length from where we sit (Wansink, Painter, & Lee, 2006) or choosing a smaller plate in the cafeteria line (Holden, Zlatevska, & Dubelaar, 2016).
Just as individuals can commit to penalties if they later yield to temptation, employers and policymakers can disincentivize undesirable behaviors by levying taxes and surcharges. For instance, taxing soda reliably decreases its consumption (Allcott, Lockwood, & Taubinsky, 2019). Since punishments as a behavior change strategy raise a host of practical, ethical, and legal concerns (Kazdin, 2009), incentives in the workplace more often take the form of rewards for desirable behaviors. For example, employees at a Fortune 500 company who were paid each time they visited the company gym exercised more and sustained this increased level of activity for several months after the conclusion of the incentive period (Beshears, Lee, Milkman, & Mislavsky, 2018). A recent review of financial incentives for physical activity concluded that conditional incentives (e.g., rewards for reaching physical activity goals) are generally more effective than unconditional incentives (e.g., free gym membership) (Barte & Wendel-Vos, 2017, but see Gneezy et al., in press). Commitment devices can extend the benefits of short-term incentives (Royer, Stehr, & Sydnor, 2015; Van Der Swaluw et al., 2018).
Because incentives can backfire and are often expensive to administer at scale, it can be more advantageous for employers to “nudge” employees toward healthier choices through choice architecture (Benartzi et al., 2017; Kamenica, 2012). It costs almost nothing, for example, to arrange the cafeteria to make water bottles more easily accessible than soda, or to affix traffic-light labels that help employees distinguish between healthy (green) and unhealthy (red) selections in the cafeteria (Thorndike, Sonnenberg, Riis, Barraclough, & Levy, 2012). More vegetarian entrees are consumed at conferences when they are presented as the default option (Hansen, Schilling, & Malthesen, 2019), and when arranged alongside meat options, meat substitutes are purchased more often (Vandenbroele, Slabbinck, Van Kerckhove, & Vermeir, 2019). Even asking employees to place lunch orders in advance can help them resist high-calorie options (VanEpps, Downs, & Loewenstein, 2016).
Attentional Strategies
Without changing our objective situations, attentional strategies manipulate the psychological salience of enduringly valued goals and/or temptations. Deliberately selecting where to place the spotlight of conscious awareness is particularly helpful when desirable behaviors (taking the stairs, eating healthier snacks) must be repeated over time and are easily forgotten, or undesirable behaviors (taking the elevator, eating unhealthy snacks) have already become entrenched habits (see also Karlan, McConnell, Mullainathan, & Zinman, 2016).
Perhaps the best-studied self-initiated attentional strategy is self-monitoring, the intentional and consistent observation of one’s own behavior (Snyder, 1974). One early investigation found that dieters who consistently monitored their food intake lost more weight than those who did not (Baker & Kirschenbaum, 1993); a more recent systematic review found a consistent relationship between self-monitoring and weight loss (Burke, Wang, & Sevick, 2011). Self-monitoring has also been shown to reduce problematic drinking (Helzer, Badger, Rose, Mongeon, & Searles, 2002) and to promote physical activity (Greaves et al., 2011; Kang, Marshall, Barreira, & Lee, 2009; Turner-McGrievy et al., 2013). Across domains, a recent meta-analytic review identified a reliable effect of self-monitoring interventions on goal attainment, with greater benefits when the monitoring is public and recorded physically (Harkin et al., 2016). Notably, while it can be beneficial to ignore temptations altogether (van Dillen & Papies, 2015), self-monitoring can usefully heighten attention to temptations, obviating mindless snacking, excessive drinking, and other unhealthy behavior.
With respect to other-initiated attentional strategies, several studies have shown that reminders provided by others can also support goal-directed behavior. In one early random-assignment study, employees who received email messages prompting them to eat healthy and stay physically active reported improvements one week later (Plotnikoff, McCargar, Wilson, & Loucaides, 2005). A systematic review of email, mail, and telephone reminders to promote healthy behavior concluded that such prompts can be effective at promoting weight loss, physical activity, and healthy eating, particularly when prompts are frequent and personalized via personal contact with a counselor (Neff & Fry, 2009). A more recent systematic review of text message interventions to increase physical activity in adults was similarly optimistic (Buchholz, Wilbur, Ingram, & Fogg, 2013). Reminders can also be implicit. For example, in one study, a menu with diet-related descriptors (e.g., “low in calories”) led to healthier choices among dieters (Papies & Veling, 2013), and simply drawing diners’ attention to the option to downsize fast-food portions can reduce consumption (Schwartz, Riis, Elbel, & Ariely, 2012).
While the potential for attentional strategies is clear, it bears noting that evidence for the benefits of self-monitoring devices, particularly over extended periods of time, is mixed (Behrens, Domina, & Fletcher, 2007; Freak‐Poli, Cumpston, Peeters, & Clemes, 2013). One possibility is that we quickly habituate to such devices or, ironically, forget to use them (Rapp & Cena, 2014). Likewise, it is easy to ignore automated emails or text messages from our employer reminding us to engage in healthy behavior. Thus, reminders are more effective when they are distinctive (e.g., unusual, novel) (Rogers & Milkman, 2016) and received “just in time” (e.g., at the moment we are making a decision as opposed to hours before or after) (Austin, Sigurdsson, & Rubin, 2006).
Appraisal Strategies
Even when situations cannot be altered and temptations are unavoidably more salient than healthy alternatives, it is still possible to use appraisal strategies to change how we make meaning of what we perceive. The appraisals we construct can seem incontrovertibly “real,” but in fact, how we interpret our circumstances is subjective and open to revision (Beck & Dozois, 2011; Ross, 2018). For behavior change, it is beneficial to appraise situations in ways that make healthy behaviors more attractive and unhealthy behaviors less attractive.
One strategy for enhancing the value of long-term goals is called “episodic future thinking”: for example, overweight and obese adults who were randomly assigned to visualize personal events they anticipated happening at a series of time points from one day to two years later subsequently ate less than adults in a control group (Daniel, Stanton, & Epstein, 2013). Rather than accentuating the importance of our future well-being, it may be even more effective to frame healthy behaviors as immediately rewarding (Woolley & Fishbach, 2016b). In one study, encouraging gym goers to choose a workout that’s especially fun rather than a workout that is especially useful led to more persistent exercise (Woolley & Fishbach, 2016a). A less instrumental appraisal strategy entails seeing healthy behaviors as relevant to our identity (e.g., “I’m the sort of person who stays physically active.”) (Berkman, Livingston, & Kahn, 2017; Oyserman et al., 2017) or as moral priorities (e.g., “Taking the stairs is good for the planet.” (Mooijman et al., 2018). And, finally, appraisal of time cues, like the first of the month, a birthday, or other temporal landmarks, can also motivate behavior (Dai, Milkman, & Riis, 2014; Tu & Soman, 2014).
We can also think about temptations differently. For example, in one study, adults who repeatedly imagined eating a food (e.g., cheese) many times subsequently ate less of it (Morewedge, Huh, & Vosgerau, 2010). In another study, adults who practiced looking at junk food and reappraising it (e.g., imagining that someone had sneezed on it) later reported diminished cravings (Giuliani, Calcott, & Berkman, 2013). Inversely, other research has shown that vividly imagining the pleasure associated with a food led adults and children to focus on enjoyment, rather than hunger satiation, and subsequently choose smaller food portions (Cornil & Chandon, 2016). Mindfulness, which encourages a detached, non-judgmental perspective on experience, has been shown to reduce impulsive eating and increase physical activity (Ruffault et al., 2017).
In some ways, changing how we think is more easily accomplished by others than by ourselves. Consider, for example, handwashing. Washing your hands for 20 seconds using warm, soapy water has been widely recommended for preventing disease transmission. However, compliance with handwashing, even among health care and food service professionals, is shockingly low (Allegranzi & Pittet, 2009; Green et al., 2007). In one field experiment, signs posted throughout a hospital that framed handwashing as a matter of patient safety “Hand hygiene prevents patients from catching diseases” increased compliance among health care professionals whereas posters emphasizing personal safety (“Hand hygiene prevents you from catching diseases”) did not (Grant & Hofmann, 2011).
Social norms are a particularly powerful lever for changing attitudes and behavior (Ajzen, 1991; Reid, Cialdini, & Aiken, 2010; Rivis & Sheeran, 2003), and employers, as opposed to individuals, are ideally suited to frame healthy behaviors as either descriptive norms (i.e., what we think most other people are doing) or injunctive norms (i.e., what we think most of our peers approve of doing) (Reid et al., 2010). Norms interventions are especially helpful when behavior change is undermined by pluralistic ignorance (i.e., when the typical individual misjudges the behavior or beliefs of others) (Bicchieri, 2016). In one field study, employees purchased more servings of vegetables when their workplace cafeterias were decorated with posters containing descriptive norm information (i.e., “Most people here choose to eat vegetables with their lunch”) (Thomas et al., 2017). Another study surveyed women living in sunny Phoenix, Arizona, and found they dramatically underestimated injunctive norms about sun protection and tanning (Reid & Aiken, 2013). Compared to an information-only condition, a treatment that updated these beliefs to be more accurate effectively changed attitudes, intentions, and behavior four weeks later. How can the power of norms be harnessed when a desirable behavior is not yet practiced by the majority? Sparkman and Walton (2017) have shown that information about how a desirable behavior is increasing in prevalence can also change behavior. Compared to a static descriptive norms message (i.e., “3 in 10 people eat less meat than they otherwise would”), a dynamic descriptive norms message (i.e., “3 in 10 people have changed their behavior and begun to eat less meat than they otherwise would”) effectively doubled meatless orders at a university cafe.
Response Modulation Strategies
Appraisals lead to response tendencies, and only impulses that cross a certain threshold are enacted. However, regardless of how valuable we expect them to be, we can effortfully modulate our responses at this final stage in the process of impulse generation. For example, despite a strong urge to smoke a cigarette during a break, we can force ourselves to abstain. Likewise, we may not feel like taking the stairs at work but can use “willpower” to force ourselves to do so. Though the least proactive of all approaches to behavior change, response modulation is also the most obvious (Sklar, Rim, & Fujita, 2017). For instance, adults who fail to follow through on their New Year’s resolutions cite willpower more than any other reason (American Psychological Association, 2012). Ironically, individuals who identify internal barriers such as willpower as the chief barrier to changing their diet and exercise habits fail to follow through with their behavior change goals more often than individuals who identify external barriers such as lack of transportation (Ziebland, Thorogood, Yudkin, Jones, & Coulter, 1998).
The capacity to effortfully inhibit or enact responses appears to be more developed in human beings than in any other species, but it is nevertheless highly fallible (Cohen, 2005; Hofmann & Kotabe, 2012). Moreover, response modulation is no fun: the experience of exerting willpower is typically described as effortful, difficult, and unpleasant (Inzlicht, Schmeichel, & Macrae, 2014; Kurzban, Duckworth, Kable, & Myers, 2013; Westbrook & Braver, 2015). Moreover, the experience of denying oneself a pleasure that has already been appraised as valuable, or forcing oneself to enact a virtuous behavior that has already been appraised as costly, may incite reactance—the agitation that arises when we perceive our freedoms have been restricted (Brehm, 1966). The process model, therefore, concurs with ancient Buddhist wisdom (Nanamoli & Bodhi, 1995) in deeming response modulation as the self-control strategy of last resort.
Just as an individual can force or suppress behaviors that are at odds with online appraisals of expected value, an employer can do the same. For instance, we may feel like smoking a cigarette on our break but not enact this behavior if our employer has banned smoking. The Cleveland Clinic, for example, conducts random drug tests among doctors, nurses, and other healthcare staff for nicotine and other addictive drugs (Sandy, 2015). Earlier than many other employers, the Cleveland Clinic also banned smoking on premises. In our view, it seems sensible to respect the rights of individuals to make their own choices whenever those choices do not carry substantial externalities, but paternalistic bans are justifiable when unhealthy behaviors cause significant harm to others (Camerer, 2006; Glaeser, 2005; Loewenstein, Brennan, & Volpp, 2007; Thaler & Sunstein, 2008). For instance, it is well-established that secondhand smoke harms others (Oberg et al., 2011), justifying laws prohibiting smoking in workplaces, restaurants, bars, and other public places (https://www.lung.org/policy-advocacy/tobacco/smokefree-environments/smokefree-air-laws). Regardless of whether hard paternalism is justified, the full suite of self-initiated and other-initiated process model strategies can, in our view, make bans more palatable and more effective (Bavel et al., 2020; Duckworth, Ungar, & Emanuel, 2020).
Shortcut Strategies
In addition to targeting one or more of the stages of impulse generation, we can directly link anticipated situational cues with desired responses. As suggested by the dotted lines in Figures 2, 3, and 4, doing so bypasses the appraisal stage altogether. Circumventing the deliberation of how good or bad something is for us supports self-control because a one-time immediately rewarding indulgence made in the heat of the moment is likely to be judged superior to a less immediately rewarding investment in our future (Loewenstein & Prelec, 1992; Rachlin, 2000). For example, taking the stairs every day can make a meaningful difference to our physical health over the long term, but the competing response of taking the elevator “just this once” more likely increases our happiness in the short term. Individually appraising each decision in isolation, therefore, can lead to repeatedly choosing comfort over health.
As noted above, foreseeing this dilemma enables planning in advance how we hope to act. Implementation intentions are an especially powerful form of plan that uses an if-then format to forge mental associations between anticipated cues and desired actions (e.g., “If I am leaving for work in the morning, then I will pack some fruit and nuts for an afternoon snack!” (Gollwitzer, 1999). As illustrated in Figure 2, implementation intentions create a “shortcut” that biases attention toward anticipated cues in our situation and, crucially, bypasses the appraisal step (Gollwitzer, 1999). Longitudinal research shows that individuals who make plans on their own are more physically active (Ludwig, Srivastava, & Berkman, 2019), but planning can also be other-initiated. Indeed, planning prompts have been shown to increase goal attainment across a wide range of domains (Gollwitzer & Sheeran, 2006; Milkman, Beshears, Choi, Laibson, & Madrian, 2013; Rogers, Milkman, John, & Norton, 2015).
Personal rules (Ainslie & Haslam, 1992) likewise link situational cues directly to desired behavioral responses but, because exceptions undermine their power, take the form of categorical declarations (e.g., “I always take the stairs!” “I never drink soda!”) (Bénabou & Tirole, 2004). Although rigidity has its costs, personal rules obviate the “just this once” rationalizing that favors unhealthy impulses. Specifically, a personal rule “overrides cost-benefit calculation with respect to that action” (Prelec & Herrnstein, 1991, pp. 320–321). Kirby (2014) points out that Gandhi was both an exemplar and advocate of personal rules, which Gandhi described as “a promise made by oneself to oneself” (Gandhi, October 31, 1930). Gandhi further suggested that “when after a series of efforts we fail in doing certain things, by taking a vow to do them we draw a cordon round ourselves, from which we may never be free and thus we avoid failures” (Gandhi, April 8, 1919) and, thus, “a vow…helps us against temptations” (Gandhi, October 14, 1930). Despite speculation that “making personal rules is obviously a learnable skill” (Ainslie & Haslam, 1992, p. 190), empirical tests of their benefits, particularly from field interventions, is lacking.
Whereas individuals can legislate personal rules for themselves, customs are forged at the level of the group. Specifically, customs are behaviors that a group of people traditionally enact, the original function of which may be long forgotten (Bicchieri, 2016). Many religious traditions promulgate customs for forgoing temptations (McCullough & Willoughby, 2009). There is, for example, the Catholic tradition of abstaining from meat on Fridays, the Buddhist tradition of vegetarianism, and the Mormon tradition of abstaining from caffeine and alcohol. The secular custom of eating dessert after, not before, dinner may be a way of limiting sweets. Likewise, organizations may benefit from replacing an established tradition of donut deliveries on Friday mornings with a healthier custom (e.g., Fresh Fruit Fridays). Introducing healthy customs doesn’t always require displacing unhealthy ones. For instance, team meetings can begin with a minute of deep breathing, and SWAG can include branded activewear. Not surprisingly, it is difficult to conduct randomized controlled trials of customs and behavior change, but the future seems bright for creative approaches to such investigations (Bicchieri, 2016; Paluck & Cialdini, 2014; Rapkin & Trickett, 2005).
It is not difficult to imagine how an individual might try out a variety of plans, eventually deciding on one that works best (e.g. “If it’s Friday, I’ll walk to and from work!”). That plan may become a personal rule (e.g., “I always walk to and from work on Fridays!”) that further reinforces the value of consistency and discourages one-off exceptions. And, finally, after dozens of repetitions, that personal rule may recede from conscious awareness, leaving an automatic habit in its place (e.g., on Fridays, without even thinking, I set off to work on foot). Similarly, an employer might prompt each of its employees to make a plan (e.g., “When and where do you plan to get your 10,000 steps?”) which becomes a company-wide custom (e.g., On our team, we always walk 10,000 steps) and, finally, a matter of corporate identity (e.g., We’re the sort of company that stays moving!).
Conclusion
In this article, we have proposed the process model of behavior change as a parsimonious framework for organizing, analyzing, and comparing behavior change strategies. Throughout, we have used physical health (Mann, de Riddler, & Fujita, 2013) as our primary illustrative example, but as we suggest in Table 2, there are many domains in which enduringly valuable goals and momentary temptations can come into conflict (e.g., procrastination, honesty, financial decision-making). Our main point is that any behavior change intervention—whether self-initiated or other-initiated—can be understood in terms of how it redirects the processes by which healthy and unhealthy impulses are generated.
As our framework makes clear, volitional behavior change is not the sole responsibility of the individual. Individuals flourish in psychologically wise social structures that make it easier, more attractive, and more obvious to align behavior with goals of enduring personal significance (Camerer, 2006; Loewenstein et al., 2007; Thaler & Sunstein, 2008). In many cases, individuals need not be aware of choice architecture to reap its benefits (Duckworth, Milkman, & Laibson, 2018; Hertwig & Grune-Yanoff, 2017). At the same time, the very notion of freedom of the will implies that individuals take responsibility for how they act, think, and feel (Frankfurt, 1988; Holton, 1999). Moreover, self-initiated strategies, once mastered, promise spillover benefits to other domains, whereas the benevolent initiatives of an employer do not (Hertwig & Grune-Yanoff, 2017). And, finally, not all organizations are benevolent (Thaler, 2018). Individuals who understand and master their own impulses are in a better position to recognize and defend themselves against behavior change strategies deployed by malevolent organizations. Indeed, history abounds with examples of psychologically sophisticated but nefarious manipulation of individual behavior, and even current corporate motives are in tension with individual well-being.
We have argued that behavior change strategies can be organized by the stage(s) of impulse generation they target, but it is a critical and common error to neglect processes upstream or downstream of a targeted process. Any comprehensive approach to behavior change must address, directly or indirectly, all stages of impulse generation. For example, incentives that unequivocally change our situation may fail to change behavior if, absent proper marketing, they fail to capture attention (Kim et al., 2012). Indeed, we are most optimistic about approaches that creatively target multiple stages of impulse generation. For instance, self-monitoring can be creatively coupled with incentives (Behrens et al., 2007; Finkelstein et al., 2016). And framing an incentive as a “surcharge” as opposed to a “discount” harnesses the power of descriptive and injunctive norms (Lieberman et al., 2018).
Both individuals and organizations might use the process model to “backward plan” (Park, Lu, & Hedgcock, 2017), beginning with the specification of behavior change goals, then identifying the appraisals that would lead to such goals, the attentional processes that would make those appraisals more likely, and, finally, the situational features that would give rise to those perceptions. Relatedly, we recommend conducting a behavior change “premortem” (Klein, 2007)—vividly imagining a future in which behavior did not change and then identifying likely failures at each stage in the process model. Identifying likely obstacles to behavior change in advance at each stage of impulse generation sets up the individual and the organization to devise feasible, effective plans for overcoming or avoiding them (Oettingen & Gollwitzer, 2018).
Despite our enthusiasm for the process model of behavior change, we recognize that alternative theoretical models may be more appropriate, depending on the purpose. In particular, policymakers may find it useful to take a more abstract view (Duckworth et al., 2018). Understanding behavior change over longer time scales—weeks to years, say, rather than moments to minutes—requires a model of how the motivation to change behavior develops in the first place, as well as how change is maintained despite inevitable relapses (Achtziger & Gollwitzer, 2008; Prochaska, Redding, & Evers, 2008; Sheeran et al., 2017). In contrast, practitioners may benefit from more fine-grained taxonomies, including classification schemes that allow for a given behavior change strategy to target multiple stages in the process model (Hollands et al., 2017; Kok et al., 2016; Michie et al., 2013).
As a general framework, the process model of behavior change is designed to supplement, not supplant, theories that seek to explain specific behavior generation processes. For example, to change appraisal in the choice between taking the stairs or the elevator, Suri, Sheppes, and Gross (2014) drew on self-determination theory and the heuristic system model. Likewise, the insight that incentives can be classified as an other-initiated situational strategy does not illuminate the differential benefits of group versus individual incentives (Kullgren et al., 2013), different lottery schemes (Patel et al., 2016; Patel et al., 2018), or framing as gains versus losses (Patel et al., 2016). Such nuanced explorations of specific processes in the generation and regulation of behavior are essential. Our hope is that in its simplicity and breadth, the process model of behavior change will help to organize these and other insights, laying the foundation for a more cumulative science of behavior change.
Highlights.
Volitional behavior change concerns behaviors that individuals themselves prefer, upon reflection, to their status quo.
Behavior change is challenging insofar as our status quo behavior (e.g., eating junk food) is more immediately rewarding than an alternative behavior (e.g., eating fruit and vegetables) that we know to be more enduringly valued.
Behavior change strategies can be initiated either by the individual (i.e., self-control) or by others (e.g., a benevolent employer).
We propose the process model of behavior change as a parsimonious framework for organizing both self-initiated and other-initiated strategies according to where they have their primary impact in the generation of behavioral impulses.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
We see no conflicts of interest. Support for our research on behavior change includes the following federal and philanthropic sources: National Institute on Aging R24-AG048081–01, the Walton Family Foundation, Vikki and Michael Price, the Marc J. Leder Foundation, and the John Templeton Foundation.
The content of this manuscript is solely the responsibility of the authors and does not necessarily represent the official views of funding agencies.
Contributor Information
Angela L. Duckworth, University of Pennsylvania
James J. Gross, Stanford University
References
- Achtziger A, & Gollwitzer PM (2008). Motivation and volition in the course of action. In Heckhausen J & Heckhausen H (Eds.), Motivation and action (pp. 273–295). New York, NY: Cambridge University Press. [Google Scholar]
- Ainslie G (2001). Breakdown of will. New York, NY: Cambridge University Press. [Google Scholar]
- Ainslie G, & Haslam N (1992). Self-control. In Loewenstein G & Elster J (Eds.), Choice over time. New York, NY: Russell Sage Foundation. [Google Scholar]
- Ajzen I (1991). The theory of planned behavior. Organizational Behavior and Human Decision Processes, 50, 179–211. [Google Scholar]
- Allcott H, Lockwood BB, & Taubinsky D (2019). Should we tax soda? An overview of theory and evidence. Journal of Economic Perspectives, 33(3), 202–227. doi: 10.1257/jep.33.3.202 [DOI] [Google Scholar]
- Allegranzi B, & Pittet D (2009). Role of hand hygiene in healthcare-associated infection prevention. Journal of Hospital Infection, 73(4), 305–315. doi: 10.1016/j.jhin.2009.04.019 [DOI] [PubMed] [Google Scholar]
- American Psychological Association. (2012). What Americans think of willpower. A survey of perceptions of willpower and its role in achieving lifestyle and behavior change goals. Retrieved from https://www.apa.org/images/stress-willpower_tcm7-130920.pdf [Google Scholar]
- Austin J, Sigurdsson SO, & Rubin YS (2006). An examination of the effects of delayed versus immediate prompts on safety belt use. Environment and Behavior, 38(1), 140–149. [Google Scholar]
- Baker RC, & Kirschenbaum DS (1993). Self-monitoring may be necessary for successful weight control. Behavior Therapy, 24(3), 377–394. doi: 10.1016/S0005-7894(05)80212-6 [DOI] [Google Scholar]
- Bandura A (1977). Self-efficacy: Toward a unifying theory of behavioral change. Psychological Review, 84(2), 191–215. [DOI] [PubMed] [Google Scholar]
- Banys P (1988). The clinical use of disulfiram (Antabuse®): A review. Journal of Psychoactive Drugs, 20(3), 243–261. doi: 10.1080/02791072.1988.10472495 [DOI] [PubMed] [Google Scholar]
- Barte JCM, & Wendel-Vos GCW (2017). A systematic review of financial incentives for physical activity: The effects on physical activity and related outcomes. Behavioral Medicine, 43(2), 79–90. doi: 10.1080/08964289.2015.1074880 [DOI] [PubMed] [Google Scholar]
- Bartels DM, & Urminsky O (2011). On intertemporal selfishness: How the perceived instability of identity underlies impatient consumption. Journal of Consumer Research, 38(1), 182–198. [Google Scholar]
- Bavel JJV, Baicker K, Boggio PS, Capraro V, Cichocka A, Cikara M, … Willer R (2020). Using social and behavioural science to support COVID-19 pandemic response. Nature Human Behaviour, 4(5), 460–471. doi: 10.1038/s41562-020-0884-z [DOI] [PubMed] [Google Scholar]
- Beck AT, & Dozois DJA (2011). Cognitive therapy: Current status and future directions. Annual Review of Medicine, 62(1), 397–409. doi: 10.1146/annurev-med-052209-100032 [DOI] [PubMed] [Google Scholar]
- Behrens TK, Domina L, & Fletcher GM (2007). Evaluation of an employer-sponsored pedometer-based physical activity program. Perceptual and Motor Skills, 105(3), 968–976. [DOI] [PubMed] [Google Scholar]
- Bénabou R, & Tirole J (2004). Willpower and personal rules. Journal of Political Economy, 112(4), 848–886. [Google Scholar]
- Benartzi S, Beshears J, Milkman K, Sunstein CR, Thaler RH, Shankar M, … Galing S (2017). Should governments invest more in nudging? Psychological Science, 28, 1041–1055. doi: 10.1177/0956797617702501 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berkman ET, Hutcherson C, Livingston JL, Kahn LE, & Inzlicht M (2017). Self-control as value-based choice. Current Directions in Psychological Science, 26(5), 422–428. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berkman ET, Livingston JL, & Kahn LE (2017). Finding the “self” in self-regulation: The identity-value model. Psychological Inquiry, 28(2–3), 77–98. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beshears J, Lee B, Milkman KL, & Mislavsky R (2018). Creating exercise habits through incentives: The tradeoff between flexibility and routinization. Working paper. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bicchieri C (2016). Diagnosing norms. In Norms in the wild: How to diagnose, measure, and change social norms. Oxford, England: Oxford University Press. [Google Scholar]
- Brehm JW (1966). A theory of psychological reactance. New York, NY: Academic Press. [Google Scholar]
- Bronfenbrenner U (1979). The ecology of human development: Experiments by nature and design. Cambridge, MA: Harvard University Press. [Google Scholar]
- Bryan G, Karlan D, & Nelson S (2010). Commitment devices. Annual Review of Economics, 2(1), 671–698. doi: 10.1146/annurev.economics.102308.124324 [DOI] [Google Scholar]
- Buchholz SW, Wilbur J, Ingram D, & Fogg L (2013). Physical activity text messaging interventions in adults: A systematic review. Worldviews on Evidence-Based Nursing, 10(3), 163–173. doi: 10.1111/wvn.12002. [DOI] [PubMed] [Google Scholar]
- Burke LE, Wang J, & Sevick MA (2011). Self-monitoring in weight loss: A systematic review of the literature. Journal of the American Dietetic Association, 111(1), 92–102. doi: 10.1016/j.jada.2010.10.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Burns D (2013, January/February). Living with the devil we know. Psychotherapy Networker. Retrieved from https://www.psychotherapynetworker.org/magazine/article/213/living-with-the-devil-we-know# [Google Scholar]
- Camerer CF (2006). Wanting, liking, and learning: Neuroscience and paternalism. The University of Chicago Law Review, 73(1), 87–110. doi: 10.2307/4495545 [DOI] [Google Scholar]
- Cohen JD (2005). The vulcanization of the human brain: A neural perspective on interactions between cognition and emotion. The Journal of Economic Perspectives, 19(4), 3–24. doi: 10.1257/089533005775196750 [DOI] [Google Scholar]
- Cornil Y, & Chandon P (2016). Pleasure as a substitute for size: How multisensory imagery can make people happier with smaller food portions. Journal of Marketing Research, 53(5), 847–864. [Google Scholar]
- Dai H, Milkman KL, & Riis J (2014). The fresh start effect: Temporal landmarks motivate aspirational behavior. Management Science, 60(10), 2563–2582. [Google Scholar]
- Daniel TO, Stanton CM, & Epstein LH (2013). The future is now: Reducing impulsivity and energy intake using episodic future thinking. Psychological Science, 24(11), 2339–2342. doi: 10.1177/0956797613488780 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Duckworth AL, Gendler TS, & Gross JJ (2016). Situational strategies for self-control. Perspectives on Psychological Science, 11(1), 35–55. doi: 10.1177/1745691615623247 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Duckworth AL, Milkman KL, & Laibson D (2018). Beyond willpower: Strategies for reducing failures of self-control. Psychological Science in the Public Interest, 19(3), 102–129. doi: 10.1177/1529100618821893 [DOI] [PubMed] [Google Scholar]
- Duckworth AL, Ungar L, & Emanual E (2020, May 27). There are 3 things we have to do to get people wearing masks. New York Times. Retrieved from https://nyti.ms/3er7BT1 [Google Scholar]
- Epton T, Currie S, & Armitage CJ (2017). Unique effects of setting goals on behavior change: Systematic review and meta-analysis. Journal of Consulting and Clinical Psychology, 85(12), 1182–1198. doi: 10.1037/ccp0000260 [DOI] [PubMed] [Google Scholar]
- Finkelstein EA, Haaland BA, Bilger M, Sahasranaman A, Sloan RA, Nang EEK, & Evenson KR (2016). Effectiveness of activity trackers with and without incentives to increase physical activity (TRIPPA): A randomised controlled trial. The Lancet Diabetes & Endocrinology, 4(12), 983–995. doi: 10.1016/S2213-8587(16)30284-4 [DOI] [PubMed] [Google Scholar]
- Frankfurt HG (1988). Freedom of the will and the concept of a person. In Goodman MF (Ed.), What is a person? New York, NY: Springer. [Google Scholar]
- Freak-Poli RLA, Cumpston M, Peeters A, & Clemes SA (2013). Workplace pedometer interventions for increasing physical activity. Cochrane Database of Systematic Reviews, (4). doi: 10.1002/14651858.CD009209.pub2 [DOI] [PubMed] [Google Scholar]
- Freud S (1916–1917/1977). Introductory lectures on psychoanalysis. New York, NY: W. W. Norton & Company. [Google Scholar]
- Gandhi. (1919, April 8). The Swadeshi Vow-I. The Bombay Chronicle, The collected works of Mahatma Gandhi, 15, p. 195. Retrieved from https://www.gandhiheritageportal.org/cwmg_volume_thumbview/MTU=#page/226/mode/2up [Google Scholar]
- Gandhi. (1930, October 14). [Letter to Narandas Gandhi]. The collected works of Mahatma Gandhi, 44, p. 219. Retrieved from https://www.gandhiheritageportal.org/cwmg_volume_thumbview/NDQ=#page/1/mode/2up [Google Scholar]
- Gandhi. (1930, October 31). [Letter to J. C. Kumarappa]. The collected works of Mahatma Gandhi, 44, p. 264. Retrieved from https://www.gandhiheritageportal.org/cwmg_volume_thumbview/NDQ=#page/304/mode/2up [Google Scholar]
- Gilbert DT, & Wilson TD (2007). Prospection: Experiencing the future. Science, 317(5843), 1351–1354. [DOI] [PubMed] [Google Scholar]
- Giné X, Karlan D, & Zinman J (2010). Put your money where your butt is: A commitment contract for smoking cessation. American Economic Journal: Applied Economics, 2(4), 213–235. doi: 10.2307/25760239 [DOI] [Google Scholar]
- Giuliani NR, Calcott RD, & Berkman ET (2013). Piece of cake. Cognitive reappraisal of food craving. Appetite, 64, 56–61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Glaeser EL (2005). Paternalism and psychology (0898–2937). Retrieved from [Google Scholar]
- Gneezy U, Kajackaite A, & Meier S (in press). Incentive-based interventions. In Hagger MS, Cameron LD, Hamilton K, Hankonen N, & Lintunen T (Eds.), The handbook of behavior change. New York, NY: Cambridge University Press. [Google Scholar]
- Gollwitzer PM (1999). Implementation intentions: Strong effects of simple plans. American Psychologist, 54(7), 493–503. doi: 10.1037/0003-066X.54.7.493 [DOI] [Google Scholar]
- Gollwitzer PM, & Sheeran P (2006). Implementation intentions and goal achievement: A meta-analysis of effects and processes. Advances in Experimental Social Psychology, 38, 69–119. doi: 10.1016/S0065-2601(06)38002-1 [DOI] [Google Scholar]
- Grant AM, & Hofmann DA (2011). It’s not all about me: Motivating hand hygiene among health care professionals by focusing on patients. Psychological Science, 22(12), 1494–1499. doi: 10.1177/0956797611419172 [DOI] [PubMed] [Google Scholar]
- Greaves CJ, Sheppard KE, Abraham C, Hardeman W, Roden M, Evans PH, & Schwarz P (2011). Systematic review of reviews of intervention components associated with increased effectiveness in dietary and physical activity interventions. BMC Public Health, 11(1), 1–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Green LR, Radke V, Mason R, Bushnell L, Reimann DW, Mack JC, … Selman CA (2007). Factors related to food worker hand hygiene practices. Journal of food protection, 70(3), 661–666. [DOI] [PubMed] [Google Scholar]
- Hansen PG, Schilling M, & Malthesen MS (2019). Nudging healthy and sustainable food choices: Three randomized controlled field experiments using a vegetarian lunch-default as a normative signal. Journal of Public Health, 41(4), 1–6. doi: 10.1093/pubmed/fdz154 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harkin B, Webb TL, Chang BPI, Prestwich A, Conner M, Kellar I, … Sheeran P (2016). Does monitoring goal progress promote goal attainment? A meta-analysis of the experimental evidence. Psychological Bulletin, 142(2), 198–229. doi: 10.1037/bul0000025 [DOI] [PubMed] [Google Scholar]
- Helzer JE, Badger GJ, Rose GL, Mongeon JA, & Searles JS (2002). Decline in alcohol consumption during two years of daily reporting. Journal of Studies on Alcohol, 63(5), 551–558. [DOI] [PubMed] [Google Scholar]
- Hershfield HE & Bartels DM (2018). The future self. In Oettingen G, Sevincer AT, & Gollwitzer PM (Eds.), The psychology of thinking about the future (pp. 89–109). The Guilford Press. [Google Scholar]
- Hertwig R, & Grune-Yanoff T (2017). Nudging and boosting: Steering or empowering good decisions. Perspectives on Psychological Science, 12(6), 973–986. doi: 10.1177/1745691617702496 [DOI] [PubMed] [Google Scholar]
- Hofmann W, Baumeister RF, Förster G, & Vohs KD (2012). Everyday temptations: An experience sampling study of desire, conflict, and self-control. Journal of Personality and Social Psychology, 102(6), 1318–1335. doi: 10.1037/a0026545 [DOI] [PubMed] [Google Scholar]
- Hofmann W, Friese M, & Strack F (2009). Impulse and self-control from a dual-systems perspective. Perspectives on Psychological Science, 4(2), 162–176. doi: 10.1111/j.1745-6924.2009.01116.x [DOI] [PubMed] [Google Scholar]
- Hofmann W, & Kotabe H (2012). A general model of preventive and interventive self-control. Social and Personality Psychology Compass, 6(10), 707–722. doi: 10.1111/j.1751-9004.2012.00461.x [DOI] [Google Scholar]
- Holden SS, Zlatevska N, & Dubelaar C (2016). Whether small plates reduce consumption depends on who’s serving and who’s looking: A meta-analysis. Journal of the Association for Consumer Research, 1(1), 134–146. [Google Scholar]
- Hollands GJ, Bignardi G, Johnston M, Kelly MP, Ogilvie D, Petticrew M, … Marteau TM (2017). The TIPPME intervention typology for changing environments to change behaviour. Nature Human Behaviour, 1(8), 1–9. [Google Scholar]
- Holton R (1999). Intention and weakness of will. The Journal of Philosophy, 96(5), 241–262. [Google Scholar]
- Inzlicht M, Schmeichel BJ, & Macrae CN (2014). Why self-control seems (but may not be) limited. Trends in Cognitive Sciences, 18(3), 127–133. doi: 10.1016/j.tics.2013.12.009 [DOI] [PubMed] [Google Scholar]
- Kable JW (2014). Valuation, intertemporal choice, and self-control. In Glimcher PW & Fehr E (Eds.), Neuroeconomics: Decision making and the brain (2nd ed., pp. 173–192). San Diego, CA: Elsevier Academic Press. [Google Scholar]
- Kahneman D (1973). Attention and effort. Englewood Cliffs, NJ: Prentice-Hall. [Google Scholar]
- Kamenica E (2012). Behavioral economics and psychology of incentives. Annual Review of Economics, 4, 427–452. doi: 10.1146/annurev-economics-080511-110909 [DOI] [Google Scholar]
- Kang M, Marshall SJ, Barreira TV, & Lee J-O (2009). Effect of pedometer-based physical activity interventions: A meta-analysis. Research Quarterly for Exercise and Sport, 80(3), 648–655. doi: 10.1080/02701367.2009.10599604 [DOI] [PubMed] [Google Scholar]
- Karlan D, McConnell M, Mullainathan S, & Zinman J (2016). Getting to the top of mind: How reminders increase saving. Management Science, 62(12), 3393–3411. doi: 10.1287/mnsc.2015.2296 [DOI] [Google Scholar]
- Kazdin AE (2009). The Kazdin method for parenting the defiant child: With no pills, no therapy, no contest of wills. Boston, MA: Houghton Mifflin. [Google Scholar]
- Kessler JB, & Zhang CY (2015). Behavioral economics and health. In Detels R, Gulliford M, Karim QA, & Tan CC (Eds.), Oxford Textbook of Global Public Health (6th ed.). Oxford, England: Oxford University Press. [Google Scholar]
- Kim AE, Towers A, Renaud J, Zhu J, Shea JA, Galvin R, & Volpp KG (2012). Application of the RE-AIM Framework to evaluate the impact of a worksite-based financial incentive intervention for smoking cessation. Journal of Occupational and Environmental Medicine, 54(5), 610–614. doi: 10.1097/JOM.0b013e31824b2171 [DOI] [PubMed] [Google Scholar]
- Klein G (2007). Performing a project premortem. Harvard Business Review, 85(9), 18–19. [Google Scholar]
- Klein HJ, Austin JT, & Cooper JT (2008). Goal choice and decision processes. In Kanfer R, Chen G, & Pritchard RD (Eds.), The organizational frontiers series: Vol. 27. Work motivation: Past, present, and future (pp. 101–150). New York, NY: Routledge/Taylor & Francis Group. [Google Scholar]
- Knittle K, Heino M, Marques MM, Stenius M, Beattie M, Ehbrecht F, … Hankonen N (2020). The compendium of self-enactable techniques to change and self-manage motivation and behaviour v. 1.0. Nature Human Behaviour, 4(2), 215–223. doi: 10.1038/s41562-019-0798-9 [DOI] [PubMed] [Google Scholar]
- Kok G, Gottlieb NH, Peters G-JY, Mullen PD, Parcel GS, Ruiter RAC, … Bartholomew LK (2016). A taxonomy of behaviour change methods: An Intervention Mapping approach. Health Psychology Review, 10(3), 297–312. doi: 10.1080/17437199.2015.1077155 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kullgren JT, Troxel AB, Loewenstein G, Asch DA, Norton LA, Wesby L, … Volpp KG (2013). Individual-versus group-based financial incentives for weight loss: a randomized, controlled trial. Annals of Internal Medicine, 158(7), 505–514. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kurzban R, Duckworth A, Kable JW, & Myers J (2013). An opportunity cost model of subjective effort and task performance. Behavioral and Brain Sciences, 36(6), 661–679. doi: 10.1017/S0140525X12003196 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Laibson D (2001). Golden eggs and hyperbolic discounting. The Quarterly Journal of Economics, 112, 443–477. [Google Scholar]
- Lewin K (1939). Field theory and experiment in social psychology: concepts and methods. American Journal of Sociology, 44, 868–896. [Google Scholar]
- Liberman N, & Trope Y (2014). Traversing psychological distance. Trends in Cognitive Sciences, 18(7), 364–369. doi: 10.1016/j.tics.2014.03.001 [DOI] [PubMed] [Google Scholar]
- Loewenstein G, Brennan T, & Volpp KG (2007). Asymmetric paternalism to improve health behaviors. JAMA, 298(20), 2415–2417. doi: 10.1001/jama.298.20.2415 [DOI] [PubMed] [Google Scholar]
- Loewenstein G, & Prelec D (1992). Anomalies in intertemporal choice: Evidence and an interpretation. Quarterly Journal of Economics, 107(2), 573–597. doi: 10.2307/2118482 [DOI] [Google Scholar]
- Ludwig RM, Srivastava S, & Berkman ET (2019). Predicting exercise with a personality facet: Planfulness and goal achievement. Psychological Science, 30(10), 1510–1521. doi: 10.1177/0956797619868812 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mann T, de Riddler D, & Fujita K (2013). Self-regulation of health behavior: Social psychological approaches to goal setting and goal striving. Health Psychology, 32(5), 487–498. doi: 10.1037/a0028533 [DOI] [PubMed] [Google Scholar]
- McCullough ME, & Willoughby BL (2009). Religion, self-regulation, and self-control: Associations, explanations, and implications. Psychological Bulletin, 135(1), 69–93. [DOI] [PubMed] [Google Scholar]
- Metcalfe J, & Mischel W (1999). A hot/cool-system analysis of delay of gratification: Dynamics of willpower. Psychological Review, 106(1), 3–19. [DOI] [PubMed] [Google Scholar]
- Michie S, Richardson M, Johnston M, Abraham C, Francis J, Hardeman W, … Wood CE (2013). The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behavior change interventions. Annals of Behavioral Medicine, 46(1), 81–95. doi: 10.1007/s12160-013-9486-6 [DOI] [PubMed] [Google Scholar]
- Milkman KL, Beshears J, Choi JJ, Laibson D, & Madrian BC (2013). Planning prompts as a means of increasing preventive screening rates. Preventive Medicine, 56(1), 92–93. [DOI] [PubMed] [Google Scholar]
- Milkman KL, Minson JA, & Volpp KG (2014). Holding the Hunger Games hostage at the gym: An evaluation of temptation bundling. Management Science, 60(2), 283–299. doi:doi: 10.1287/mnsc.2013.1784 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Milkman KL, Rogers T, & Bazerman MH (2008). Harnessing our inner angels and demons: What we have learned about want/should conflicts and how that knowledge can help us reduce short-sighted decision making. Perspectives on Psychological Science, 3(4), 324–338. [DOI] [PubMed] [Google Scholar]
- Mooijman M, Meindl P, Oyserman D, Monterosso J, Dehghani M, Doris JM, & Graham J (2018). Resisting temptation for the good of the group: Binding moral values and the moralization of self-control. Journal of Personality and Social Psychology, 115(3), 585–599. doi: 10.1037/pspp0000149 [DOI] [PubMed] [Google Scholar]
- Morewedge CK, Huh YE, & Vosgerau J (2010). Thought for food: Imagined consumption reduces actual consumption. Science, 330(6010), 1530–1533. [DOI] [PubMed] [Google Scholar]
- Nanamoli B, & Bodhi B (1995). Vitakkasanthana sutta: The removal of distracting thoughts. In The middle length discourses of the Buddha: A translation of the Majjhima Nikaya (pp. 211–216). Somerville, MA: Wisdom Publications. [Google Scholar]
- National Research Council. (2010). International differences in mortality at older ages: Dimensions and sources. Washington, DC: National Academies Press. doi: 10.17226/12945 [DOI] [PubMed] [Google Scholar]
- Neff R, & Fry J (2009). Periodic prompts and reminders in health promotion and health behavior interventions: Systematic review. Journal of Medical Internet Research, 11(2), e16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nielsen L, Riddle M, King JW, Team N. I. H. S. o. B. C. I., Aklin WM, Chen W, … Weber W (2018). The NIH Science of Behavior Change Program: Transforming the science through a focus on mechanisms of change. Behaviour Research and Therapy, 101, 3–11. doi: 10.1016/j.brat.2017.07.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Öberg M, Jaakkola MS, Woodward A, Peruga A, & Prüss-Ustün A (2011). Worldwide burden of disease from exposure to second-hand smoke: a retrospective analysis of data from 192 countries. The Lancet, 377(9760), 139–146. [DOI] [PubMed] [Google Scholar]
- Ochsner K, & Gross JJ (2014). The neural bases of emotion and emotion regulation: A valuation perspective. In Gross JJ (Ed.), Handbook of emotion regulation (2nd ed.). New York, NY: Guilford. [Google Scholar]
- Oettingen G, & Gollwitzer PM (2018). Health behavior change by self-regulation of goal pursuit: Mental contrasting with implementation intentions. In The Routledge international handbook of self-control in health and well-being. (pp. 418–430). New York, NY: Routledge/Taylor & Francis Group. [Google Scholar]
- Oyserman D, Lewis NA, Yan VX, Fisher O, O’Donnell SC, & Horowitz E (2017). An identity-based motivation framework for self-regulation. Psychological Inquiry, 28(2–3), 139–147. doi: 10.1080/1047840X.2017.1337406 [DOI] [Google Scholar]
- Paluck EL, & Cialdini RB (2014). Field research methods. In Reis HT & Judd CM (Eds.), Handbook of research methods in social and personality psychology (2nd ed., pp. 81–97). New York, NY: Cambridge University Press. [Google Scholar]
- Papies EK, & Veling H (2013). Healthy dining. Subtle diet reminders at the point of purchase increase low-calorie food choices among both chronic and current dieters. Appetite, 61(1), 1–7. [DOI] [PubMed] [Google Scholar]
- Park J, Lu F-C, & Hedgcock WM (2017). Relative effects of forward and backward planning on goal pursuit. Psychological Science, 28(11), 1620–1630. 10.1177/0956797617715510 [DOI] [PubMed] [Google Scholar]
- Pashler H, & Johnston JC (2016). Attentional limitations in dual-task performance. In Pashler H (Ed.), Attention (pp. 155–189). Hove, UK: Psychology Press. [Google Scholar]
- Patel MS, Asch DA, Rosin R, Small DS, Bellamy SL, Heuer J, … Volpp KG (2016). Framing financial incentives to increase physical activity among overweight and obese adults. Annals of Internal Medicine, 164(6), 385–394. doi: 10.7326/M15-1635 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Patel MS, Volpp KG, Rosin R, Bellamy SL, Small DS, Heuer J, … Asch DA (2018). A randomized, controlled trial of lottery-based financial incentives to increase physical activity among overweight and obese adults. American Journal of Health Promotion, 32(7), 1568–1575. doi: 10.1177/0890117118758932 [DOI] [PubMed] [Google Scholar]
- Plato. (380 BCE/1992). The republic (G. M. A. Grube & C. D. C. Reeve, Trans.) (2nd ed.). Indianapolis, IN: Hackett Publishing Company. [Google Scholar]
- Plotnikoff RC, McCargar LJ, Wilson PM, & Loucaides CA (2005). Efficacy of an E-mail intervention for the promotion of physical activity and nutrition behavior in the workplace context. American Journal of Health Promotion, 19(6), 422–429. [DOI] [PubMed] [Google Scholar]
- Prelec D, & Herrnstein RJ (1991). Preferences or principles: Alternative guidelines for choice. In Zeckhauser R (Ed.), Strategy and choice (pp. 319–340). Cambridge, MA: MIT Press. [Google Scholar]
- Prochaska JO, Redding CA, & Evers KE (2008). The transtheoretical model and stages of change. In Glanz K, Rimer BK, & Viswanath K (Eds.), Health behavior and health education: Theory, research, and practice (4th ed., pp. 97–121). San Francisco, CA: Jossey-Bass. [Google Scholar]
- Rachlin H (2000). The science of self-control. Cambridge, MA: Harvard University Press. [Google Scholar]
- Rapkin BD, & Trickett EJ (2005). Comprehensive dynamic trial designs for behavioral prevention research with communities: Overcoming inadequacies of the randomized controlled trial paradigm. In Trickett EJ & Pequegnat W (Eds.), Community interventions and AIDS (pp. 249–277). Cary, NC: Oxford University Press. [Google Scholar]
- Rapp A, & Cena F (2014). Self-monitoring and technology: Challenges and open issues in personal informatics. Paper presented at the International Conference on Universal Access in Human-Computer Interaction. [Google Scholar]
- Reid AE, & Aiken LS (2013). Correcting injunctive norm misperceptions motivates behavior change: A randomized controlled sun protection intervention. Health Psychology, 32(5), 551–560. doi: 10.1037/a0028140 [DOI] [PubMed] [Google Scholar]
- Reid AE, Cialdini RB, & Aiken LS (2010). Social norms and health behavior. In Handbook of behavioral medicine (pp. 263–274). New York, NY: Springer. [Google Scholar]
- Rivis A, & Sheeran P (2003). Social influences and the theory of planned behaviour: Evidence for a direct relationship between prototypes and young people’s exercise behaviour. Psychology and Health, 18(5), 567–583. [Google Scholar]
- Rogers T, & Milkman KL (2016). Reminders through association. Psychological Science, 27(7), 973–986. doi: 10.1177/0956797616643071 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rogers T, Milkman KL, John LK, & Norton MI (2015). Beyond good intentions: Prompting people to make plans improves follow-through on important tasks. Behavioral Science & Policy, 1(2), 33–41. [Google Scholar]
- Rogers T, Milkman KL, & Volpp KG (2014). Commitment devices: Using initiatives to change behavior. JAMA, 311(20), 2065–2066. doi: 10.1001/jama.2014.3485 [DOI] [PubMed] [Google Scholar]
- Ross L (2018). From the fundamental attribution error to the truly fundamental attribution error and beyond: My research journey. Perspectives on Psychological Science, 13(6), 750–769. [DOI] [PubMed] [Google Scholar]
- Ross L, & Nisbett RE (1991). The person and the situation: Perspectives of social psychology. Philadelphia, PA: Temple University Press. [Google Scholar]
- Royer H, Stehr M, & Sydnor J (2015). Incentives, commitments, and habit formation in exercise: Evidence from a field experiment with workers at a Fortune-500 company. American Economic Journal: Applied Economics, 7(3), 51–84. doi: 10.1257/app.20130327 [DOI] [Google Scholar]
- Ruffault A, Czernichow S, Hagger MS, Ferrand M, Erichot N, Carette C, … Flahault C (2017). The effects of mindfulness training on weight-loss and health-related behaviours in adults with overweight and obesity: A systematic review and meta-analysis. Obesity Research & Clinical Practice, 11(5), 90–111. [DOI] [PubMed] [Google Scholar]
- Sandy E (2015, November 20). Cleveland Clinic to begin randomly drug-screening all employees Jan. 1. Cleveland Scene. Retrieved from https://www.clevescene.com/scene-and-heard/archives/2015/11/20/cleveland-clinic-to-begin-randomly-drug-screening-all-employees-jan-1 [Google Scholar]
- Sayette MA, Loewenstein G, Griffin KM, & Black JJ (2008). Exploring the cold-to-hot empathy gap in smokers. Psychological Science, 19(9), 926–932. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schelling TC (1978). Egonomics, or the art of self-management. The American Economic Review, 68(2), 290–294. doi: 10.2307/1816707 [DOI] [Google Scholar]
- Schroeder SA (2007). We can do better—Improving the health of the American people. New England Journal of Medicine, 357(12), 1221–1228. [DOI] [PubMed] [Google Scholar]
- Schwartz J, Riis J, Elbel B, & Ariely D (2012). Inviting consumers to downsize fast-food portions significantly reduces calorie consumption. Health Affairs, 31(2), 399–407. [DOI] [PubMed] [Google Scholar]
- Seligman MEP, Railton P, Baumeister RF, & Sripada C (2016). Homo prospectus. New York, NY: Oxford University Press. [Google Scholar]
- Sheeran P, Klein WM, & Rothman AJ (2017). Health behavior change: Moving from observation to intervention. Annual Review of Psychology, 68, 573–600. [DOI] [PubMed] [Google Scholar]
- Sklar A, Rim S, & Fujita K (2017). Proactive and reactive self-control. In de Ridder D, Adriaanse M, & Fujita K (Eds.), The Routledge international handbook of self-control in health and well-being (pp. 24–34). London, UK: Routledge. [Google Scholar]
- Smith KG, Locke EA, & Barry D (1990). Goal setting, planning, and organizational performance: An experimental simulation. Organizational Behavior and Human Decision Processes, 46(1), 118–134. [Google Scholar]
- Snyder M (1974). Self-monitoring of expressive behavior. Journal of Personality and Social Psychology, 30(4), 526–537. doi: 10.1037/h0037039 [DOI] [Google Scholar]
- Sparkman G, & Walton GM (2017). Dynamic norms promote sustainable behavior, even if it is counternormative. Psychological Science, 28(11), 1663–1674. doi: 10.1177/0956797617719950 [DOI] [PubMed] [Google Scholar]
- Sullivan N, Hutcherson C, Harris A, & Rangel A (2014). Dietary self-control is related to the speed with which attributes of healthfulness and tastiness are processed. Psychological Science, 26(2), 122–134. doi: 10.1177/0956797614559543 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sunstein CR (2014). Nudging: A very short guide. Journal of Consumer Policy, 37(4), 583–588. [Google Scholar]
- Suri G, Sheppes G, Leslie S, & Gross JJ (2014). Stairs or escalator? Using theories of persuasion and motivation to facilitate healthy decision making. Journal of Experimental Psychology: Applied, 20(4), 295–302. doi: 10.1037/xap0000026 [DOI] [PubMed] [Google Scholar]
- Thaler RH, & Shefrin HM (1981). An economic theory of self-control. Journal of Political Economy, 89(2), 392–406. [Google Scholar]
- Thaler RH, & Sunstein CR (2008). Nudge: Improving decisions about health, wealth, and happiness. New Haven, CT: Yale University Press. [Google Scholar]
- Thomas JM, Ursell A, Robinson EL, Aveyard P, Jebb SA, Herman CP, & Higgs S (2017). Using a descriptive social norm to increase vegetable selection in workplace restaurant settings. Health Psychology, 36(11), 1026–1033. doi: 10.1037/hea0000478 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thorndike AN, Sonnenberg L, Riis J, Barraclough S, & Levy DE (2012). A 2-phase labeling and choice architecture intervention to improve healthy food and beverage choices. American Journal of Public Health, 102(3), 527–533. doi: 10.2105/ajph.2011.300391 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tu Y, & Soman D (2014). The categorization of time and its impact on task initiation. Journal of Consumer Research, 41(3), 810–822. [Google Scholar]
- Turner-McGrievy GM, Beets MW, Moore JB, Kaczynski AT, Barr-Anderson DJ, & Tate DF (2013). Comparison of traditional versus mobile app self-monitoring of physical activity and dietary intake among overweight adults participating in an mHealth weight loss program. Journal of the American Medical Informatics Association, 20(3), 513–518. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Van Der Swaluw K, Lambooij MS, Mathijssen JJ, Schipper M, Zeelenberg M, Berkhout S, … Prast HM (2018). Commitment lotteries promote physical activity among overweight adults—A cluster randomized trial. Annals of Behavioral Medicine, 52(4), 342–351. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vandenbroele J, Slabbinck H, Van Kerckhove A, & Vermeir I (2019). Mock meat in the butchery: Nudging consumers toward meat substitutes. Organizational Behavior and Human Decision Processes. doi: 10.1016/j.obhdp.2019.09.004 [DOI] [Google Scholar]
- van Dillen LF, & Papies EK (2015). From distraction to mindfulness: Psychological and neural mechanisms of attention strategies in self-regulation. In Gendolla GHE, Tops M, & Koole SL (Eds.), Handbook of Biobehavioral Approaches to Self-Regulation (pp. 141–154). New York, NY: Springer. [Google Scholar]
- VanEpps EM, Downs JS, & Loewenstein G (2016). Advance ordering for healthier eating? Field experiments on the relationship between the meal order–Consumption time delay and meal content. Journal of Marketing Research, 53(3), 369–380. doi: 10.1509/jmr.14.0234 [DOI] [Google Scholar]
- Wansink B, Painter JE, & Lee YK (2006). The office candy dish: Proximity’s influence on estimated and actual consumption. International Journal of Obesity, 30(5), 871–875. [DOI] [PubMed] [Google Scholar]
- Westbrook A, & Braver TS (2015). Cognitive effort: A neuroeconomic approach. Cognitive, Affective, & Behavioral Neuroscience, 15, 395–415. doi: 10.3758/s13415-015-0334-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- Whitman W (1904). Song of myself. East Aurora, NY: Roycrofters. [Google Scholar]
- Wood W, & Neal DT (2016). Healthy through habit: Interventions for initiating & maintaining health behavior change. Behavioral Science & Policy, 2(1), 1–13. [Google Scholar]
- Wood W, Quinn JM, & Kashy DA (2002). Habits in everyday life: Thought, emotion, and action. Journal of Personality and Social Psychology, 83(6), 1281–1297. doi: 10.1037/0022-3514.83.6.1281 [DOI] [PubMed] [Google Scholar]
- Woolley K, & Fishbach A (2016a). For the fun of it: Harnessing immediate rewards to increase persistence in long-term goals. Journal of Consumer Research, 42(6), 952–966. doi: 10.1093/jcr/ucv098 [DOI] [Google Scholar]
- Woolley K, & Fishbach A (2016b). Immediate rewards predict adherence to long-term goals. Personality and Social Psychology Bulletin, 43(2), 151–162. doi: 10.1177/0146167216676480 [DOI] [PubMed] [Google Scholar]
- Ziebland S, Thorogood M, Yudkin P, Jones L, & Coulter A (1998). Lack of willpower or lack of wherewithal? “Internal” and “external” barriers to changing diet and exercise in a three year follow-up of participants in a health check. Social Science & Medicine, 46(4–5), 461–465. [DOI] [PubMed] [Google Scholar]