

Abstract
Backgroud
There are many studies on the vertebral body-to-canal ratio, the so-called Pavlov's ratio of the cervical spine. However, there are no studies on its relation with age to clarify each bony component's contribution to the spinal canal formation and its size. The aim of this study was to investigate differences and changes in the vertebral body-to-canal ratio according to age in an asymptomatic population.
Methods
This is a cross-sectional study of 280 asymptomatic individuals. A total of 140 men and 140 women representing each decade of life from the first to the seventh were included in this study. The anteroposterior length of the vertebral body and canal from C3 to C6 was measured on sagittal radiographs to calculate the vertebral body-to-canal ratio.
Results
The average Pavlov's ratio was significantly larger (p < 0.001) in the first decade of life. The average Pavlov's ratio of the individuals in the first decade of life was 1.09 between C3 and C6 (1.08 at C3, 1.07 at C4, 1.11 at C5, and 1.13 at C6; range, 0.78–1.51). There was no significant difference among the other decades of life.
Conclusions
We assessed the Pavlov's ratio of the cervical spine in an asymptomatic population. It is our belief that the spinal canal size is the largest in the first decade of life, and the Pavlov's ratio becomes almost fixed throughout life after maturity.
Keywords: Cervical spine, Pavlov's ratio, Spinal canal, Torg–Pavlov ratio, Vertebral body
There are many studies regarding the cervical spinal canal morphology, which is closely related to spinal stenosis. It is well known that the anteroposterior (AP) diameter of the cervical spinal canal (segmental sagittal diameter) is a basic determinant of myelopathy.1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17) Herzog et al.18) reported that the most accurate measurement of the developmental sagittal diameter of the cervical spinal canal can be made on sagittal plane radiographs. Nevertheless, measurements on plain radiographs can have magnification errors. Ratio measurements, especially the Pavlov's ratio, are performed to overcome this problem. A Pavlov's ratio (defined as the vertebral body-to-canal ratio) of less than 0.82 indicates significant cervical spinal stenosis.3,9,11)
Goto et al.5) reported that younger Japanese generations had a wider cervical spinal canal than did older Japanese generations and the development of body build size was related to the AP size of the spinal canal. It may be a plausible explanation. However, we have considerable disagreement on their view, considering the structural development of the bony canal. The spinal canal is formed by the posterior wall of the vertebral body, pedicle, and lamina. Pedicle growth is the most important factor, and the neurocentral synchondrosis (growth plate of the pedicle) plays the most contributory role in the growth of the spinal canal. It is believed that the spinal canal increases in size relatively fast via synchondrotic growth until the age of 6 to 8 years.19) Because synchondrosis fuses by those ages, the spinal canal size is determined by the closure time of synchondrosis regardless of the body build size. Individuals with delayed closure of the synchondrosis will have a larger spinal canal than those with early closure. Appositional growth of the vertebral body continues steadily until maturity, but it does not directly contribute to the canal growth. Even after closure of synchondrosis, body growth continues till maturity. Consequently, the vertebral body-to-canal ratio decreases as the vertebral body grows because the canal diameter does not change after synchondrosis closure. Therefore, we can expect that the vertebral body-to-canal ratio is larger in those in the first decade of life than those in the later decades of life and after maturity, in whom there will be little difference by the decade of life. The aim of the present study was to investigate differences and changes in the vertebral body-to-canal ratio according to age in an asymptomatic population.
METHODS
This study was approved by the Institutional Review Board of Cheju Halla General Hospital (IRB No. MKIOR-127) and the need for patient consent was exempted by the ethics committee due to minimal risk of the study. A total of 280 subjects were included in the analyses. Among them, there were 140 men and 140 women; there were 40 subjects for each decade of life. They visited the emergency department of our institution with minor trauma from April 2018 to March 2019 and complained only of neck pain without neurologic symptoms. The neck pain improved after 2 weeks of conservative treatment. Those who had a history of fracture or surgical treatment or who had a congenital anomaly or ossification of the posterior longitudinal ligament in the cervical spine were excluded.
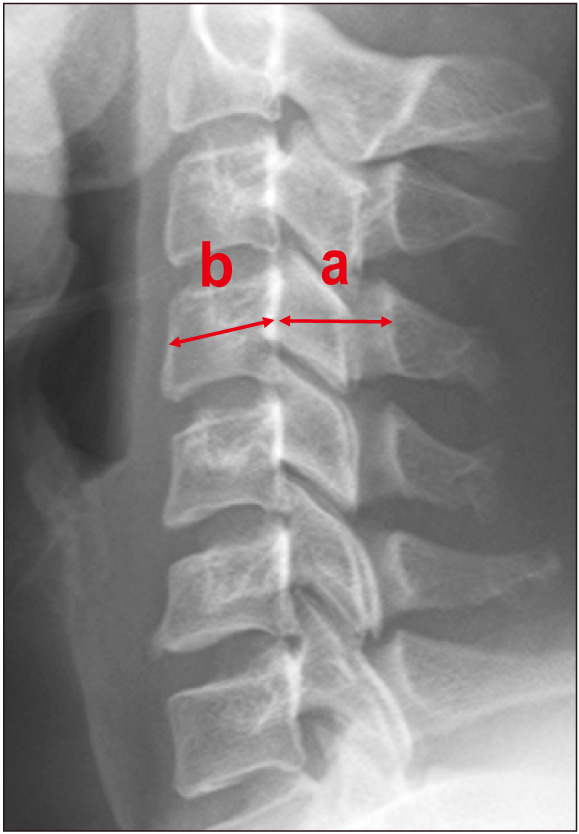
Lateral radiographs of the cervical spine in the neutral position were taken at the distance of 1.8 m between the X-ray tube and the film cassette. The AP diameters of the vertebral body and canal were measured from C3 to C6 in neutral position. The sagittal diameter of the vertebral body was measured at the midpoint between the anterior wall and the posterior wall. The spinal canal diameter was defined as the distance between the center of the posterior wall of the vertebral body and a line drawn parallel to the posterior wall of the vertebral body and tangent to the base of the spinous process, according to the method described by Goto et al.5) (Fig. 1). The Pavlov's ratio was measured twice with a digital measuring instrument on Piview STAR PACS ver. 5.0 (INFINITT Healthcare, Seoul, South Korea) by 2 spine surgeons (MSM, SMW) with a 4-week interval.
Fig. 1. The sagittal diameter of the spinal canal (a) is measured from the posterior surface of the vertebral body to the nearest point of the corresponding spinal laminar line. The sagittal diameter of the vertebral body (b) is measured at the midpoint between the anterior surface and the posterior surface. The Pavlov's ratio is measured using the formula a/b.
Statistical analyses were performed using SPSS ver. 14.0 (SPSS Inc., Chicago, IL, USA). Intraobserver and interobserver reliability were assessed by calculating the intraclass correlation coefficient (ICC). The ICC values range from 0 to 1, with a higher value indicating better reliability. An ICC less than 0.40 was considered as poor, 0.40 to 0.59 as fair, 0.60 to 0.74 as good, and 0.75 to 1.00 as excellent.20) Analysis of variance test was used for evaluation of the differences in each decade. A p-value < 0.05 was considered to be statistically significant.
RESULTS
Both interobserver and intraobserver ICCs were excellent with 0.95 and 0.83, respectively. The average Pavlov's ratio in the first decade of life was the greatest with 1.09 (range, 0.78–1.51); the average of each segmental ratio in the first decade of life was 1.08 at C3, 1.07 at C4, 1.11 at C5, and 1.13 at C6. The ratio in the second decade of life was 1.01 at C3, 0.99 at C4, 0.98 at C5, and 1.00 at C6 (Table 1). The average ratio of the second decade of life was smaller than that of the first decade of life (p < 0.001) (Table 2). This result indicates the growth cessation of neurocentral synchondrosis at the age of 6 to 8 years and continuing appositional growth of the vertebral body till maturity.
Table 1. Average Pavlov's Ratio at Each Vertebral Level for Each Decade of Life.
| Decade of life | C3 | C4 | C5 | C6 | Average (C3 to C6) |
|---|---|---|---|---|---|
| First (n = 40) | 1.08 (0.80–1.41) | 1.07 (0.78–1.51) | 1.11 (0.83–1.40) | 1.13 (0.91–1.34) | 1.09 |
| Second (n = 40) | 0.97 (0.75–1.41) | 0.97 (0.77–1.22) | 0.97 (0.57–1.25) | 0.98 (0.78–1.20) | 0.97 |
| Third (n = 40) | 0.94 (0.70–1.27) | 0.98 (0.78–1.51) | 1.00 (0.73–1.12) | 0.98 (0.79–1.32) | 0.97 |
| Fourth (n = 40) | 0.96 (0.76–1.09) | 0.97 (0.88–1.15) | 0.99 (0.80–1.45) | 0.98 (0.65–1.14) | 0.97 |
| Fifth (n = 40) | 0.94 (0.72–1.12) | 0.94 (0.77–1.14) | 0.9 (0.82–1.10) | 1.00 (0.85–1.12) | 0.96 |
| Sixth (n = 40) | 0.97 (0.79–1.18) | 0.96 (0.68–1.19) | 0.97 (0.84–1.15) | 0.98 (0.73–1.22) | 0.97 |
| Seventh (n = 40) | 0.96 (0.71–1.44) | 0.94 (0.61–1.14) | 1.00 (0.75–1.38) | 0.99 (0.77–1.43) | 0.97 |
Values are ratio (range).
Table 2. Comparison of Pavlov's Ratio between the First Decade of Life and Other Decades of Life.
| Decade | Mean difference* | p-value† |
|---|---|---|
| Second | 0.124 | < 0.001 |
| Third | 0.122 | < 0.001 |
| Fourth | 0.122 | < 0.001 |
| Fifth | 0.132 | < 0.001 |
| Sixth | 0.126 | < 0.001 |
| Seventh | 0.124 | < 0.001 |
*Difference with the first decade of life. †The p-values were calculated with the use of one-way analysis of variance for normally distributed clinical characteristics.
In the third decade of life, the ratio was 0.94 at C3, 1.07 at C4, 1.00 at C5, and 1.00 at C6. Ratios from the fourth to seventh decade of life ranged from 0.96 to 1.09 on average (Table 1). Only statistically negligible ratio differences were noted between each decade of life. This result suggests the lifelong maintenance of vertebral body-to-canal ratio, which is established by the second decade of life (Fig. 2).
Fig. 2. Average value (C3 to C6) of the Pavlov's ratio for each decade of life.

DISCUSSION
Some patients have congenital stenosis of the bony canal and foramens of the mobile cervical and lumbar spines: for example, the spine of achondroplasia (short pedicle, thickened lamina) and syndromes involving short stature in which the Pavlov's ratio is low. Clinically, cervical spinal canal stenosis is caused primarily by disc degeneration with a narrow vertebral body-to-canal ratio, hypertrophic osteoarthropathy, and hypertrophic soft tissue (ligamentum flavum).
In many previous studies published by Japanese authors, the spinal canal size was particularly related with body build.4,5,6,8,13) Findings reported in these reports were interesting but there was lack of conclusive evidence, and the authors did not conduct comparative longitudinal studies, such as smaller body build vs. larger body build in individuals in each decade of life. Goto et al.5) attributed the smaller canal size of the older Japanese population to the smaller body build in comparison with the younger Japanese population who have larger build. However, we do not agree with them. Body build does not relate with the canal size except achondroplastic dwarfs in whom pedicle growth does not take place, while vertebral body and cord growth continue till maturity. There have been several studies on the AP canal diameter among Japanese patients stratified by age brackets, which showed there was a tendency that the younger the patient, the wider the canal, while the vertebral body-to-canal ratio decreased with age. They did not explain the possible relation with height and height changes in the young and old Japanese. Also, they did not provide plausible causes for the presence of wider canal in the younger population and the narrower canal in the older population. It is not clear whether canal narrowing in the elderly Japanese population was inherited or secondary to other causes such as lamina thickening or vertebral body hypertrophy. Hayashi et al.6) reported that the sagittal diameter of the spinal canal was found to decrease with age. However, the result was not statistically significant, and the authors did not provide a scientifically acceptable cause for the age-related narrowing of the spinal canal. They also measured and compared the AP diameters in the lateral radiographs of the cervical spine. An important consideration here is measurement errors caused by magnification. It has been demonstrated that using the Pavlov's ratio can eliminate the possibility of measurement error resulting from direct spinal canal measurement.3,9,16,21) Lee et al.21) reported that there was no corresponding influence of age on the Pavlov's ratio, which is more reliable than direct measurement of the AP diameter of the cervical spinal canal in the evaluation of spinal stenosis. Aebli et al.15) also reported there was no significant correlation between the Pavlov's ratio and age and that weight and height had no significant correlations with the Pavlov's ratio. The data of the Pavlov's ratio of the current study support the importance of contribution of neurocentral synchondrosis for canal formation, which was noted in achondroplastic dwarfs who had stunted neurocentral synchondrotic growth of pedicles. Theoretically, once the canal is formed by maturity, it must be balanced in dynamic state. That is, clinically, once the canal grows to a certain size to accommodate the spinal cord, then the size would be maintained.
This is the first study that investigated the Pavlov's ratio by each decade of life to compare the difference in the spinal canal size between age groups. In particular, we included subjects in the first decade of life in the analysis to investigate the importance of spinal canal size determination by neurocentral synchondrosis. The present study suggests that age does not significantly influence the Pavlov's ratio in adults, and it is presumed that bony narrowing of the spinal canal does not progress with age in adults, except for patients with ossification of the posterior longitudinal ligament and diseases that cause bony overgrowth, such as pituitary adenoma. Clinically, evaluating the Pavlov's ratio to assess risks or predictive factors of cervical myelopathy may be useful for confirming congenital spinal stenosis, and if the Pavlov's ratio decreases with age, additional diagnostic evaluation for pathological conditions such as ossification of ligament and bony overgrowth will be needed.
Based on this preliminary study, we will conduct a comparative study by generation of patients with myelopathy and another comparative study between patients with myelopathy and without. There are some limitations of this study. First, the study population was limited to Korean subjects, so possible ethnic differences were not considered. Second, we compared different individuals in the different age groups because this was a cross-sectional rather than a longitudinal study. A comparative longitudinal study would be necessary.
In conclusion, this study provides the basic data of the Pavlov's ratio of an asymptomatic population stratified by age. It is our belief that the spinal canal size and vertebral body-to-canal ratio are the largest in the first decade of life and that the size is almost fixed by the time of maturity and maintained throughout life despite continuous internal remodeling.
Footnotes
CONFLICT OF INTEREST: No potential conflict of interest relevant to this article was reported.
References
- 1.Marques C, Granstrom E, MacDowall A, Moreira NC, Skeppholm M, Olerud C. Accuracy and reliability of X-ray measurements in the cervical spine. Asian Spine J. 2020;14(2):169–176. doi: 10.31616/asj.2019.0069. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Alijani B, Rasoulian J. The sagittal balance of the cervical spine: radiographic analysis of interdependence between the occipitocervical and spinopelvic alignment. Asian Spine J. 2020;14(3):287–297. doi: 10.31616/asj.2019.0165. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Pavlov H, Torg JS, Robie B, Jahre C. Cervical spinal stenosis: determination with vertebral body ratio method. Radiology. 1987;164(3):771–775. doi: 10.1148/radiology.164.3.3615879. [DOI] [PubMed] [Google Scholar]
- 4.Ishikawa M, Matsumoto M, Fujimura Y, Chiba K, Toyama Y. Changes of cervical spinal cord and cervical spinal canal with age in asymptomatic subjects. Spinal Cord. 2003;41(3):159–163. doi: 10.1038/sj.sc.3101375. [DOI] [PubMed] [Google Scholar]
- 5.Goto S, Umehara J, Aizawa T, Kokubun S. Comparison of cervical spinal canal diameter between younger and elder generations of Japanese. J Orthop Sci. 2010;15(1):97–103. doi: 10.1007/s00776-009-1427-7. [DOI] [PubMed] [Google Scholar]
- 6.Hayashi H, Okada K, Hamada M, Tada K, Ueno R. Etiologic factors of myelopathy: a radiographic evaluation of the aging changes in the cervical spine. Clin Orthop Relat Res. 1987;(214):200–209. [PubMed] [Google Scholar]
- 7.Hukuda S, Xiang LF, Imai S, Katsuura A, Imanaka T. Large vertebral body, in addition to narrow spinal canal, are risk factors for cervical myelopathy. J Spinal Disord. 1996;9(3):177–186. [PubMed] [Google Scholar]
- 8.Tanaka Y. Morphological changes of the cervical spinal canal and cord due to aging. Nihon Seikeigeka Gakkai Zasshi. 1984;58(9):873–886. [PubMed] [Google Scholar]
- 9.Torg JS, Pavlov H, Genuario SE, et al. Neurapraxia of the cervical spinal cord with transient quadriplegia. J Bone Joint Surg Am. 1986;68(9):1354–1370. [PubMed] [Google Scholar]
- 10.Moon MS, Ha KY, Jeong DY. Pavlov's ratio of cervical spine of normal Koreans: determining spinal stenosis on routine lateral roentgenograms. J Korean Orthop Assoc. 1989;24(5):1307–1312. [Google Scholar]
- 11.Torg JS. Pavlov's ratio: determining cervical spinal stenosis on routine lateral roentgenograms. Contemp Orthop. 1989;18:153–160. [Google Scholar]
- 12.Suk KS, Kim KT, Lee JH, Lee SH, Kim JS, Kim JY. Reevaluation of the Pavlov ratio in patients with cervical myelopathy. Clin Orthop Surg. 2009;1(1):6–10. doi: 10.4055/cios.2009.1.1.6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Sasaki T, Kadoya S, Iizuka H. Roentgenological study of the sagittal diameter of the cervical spinal canal in normal adult Japanese. Neurol Med Chir (Tokyo) 1998;38(2):83–88. doi: 10.2176/nmc.38.83. [DOI] [PubMed] [Google Scholar]
- 14.Hinck VC, Hopkins CE, Savara BS. Sagittal diameter of the cervical spinal canal in children. Radiology. 1962;79:97–108. doi: 10.1148/79.1.97. [DOI] [PubMed] [Google Scholar]
- 15.Aebli N, Wicki AG, Ruegg TB, Petrou N, Eisenlohr H, Krebs J. The Torg-Pavlov ratio for the prediction of acute spinal cord injury after a minor trauma to the cervical spine. Spine J. 2013;13(6):605–612. doi: 10.1016/j.spinee.2012.10.039. [DOI] [PubMed] [Google Scholar]
- 16.Yue WM, Tan SB, Tan MH, Koh DC, Tan CT. The Torg--Pavlov ratio in cervical spondylotic myelopathy: a comparative study between patients with cervical spondylotic myelopathy and a nonspondylotic, nonmyelopathic population. Spine (Phila Pa 1976) 2001;26(16):1760–1764. doi: 10.1097/00007632-200108150-00006. [DOI] [PubMed] [Google Scholar]
- 17.Hashimoto I, Tak YK. The true sagittal diameter of the cervical spinal canal and its diagnostic significance in cercical myelopathy. J Neurosurg. 1977;47(6):912–916. doi: 10.3171/jns.1977.47.6.0912. [DOI] [PubMed] [Google Scholar]
- 18.Herzog RJ, Wiens JJ, Dillingham MF, Sontag MJ. Normal cervical spine morphometry and cervical spinal stenosis in asymptomatic professional football players: plain film radiography, multiplanar computed tomography, and magnetic resonance imaging. Spine (Phila Pa 1976) 1991;16(6 Suppl):S178–S186. doi: 10.1097/00007632-199106001-00001. [DOI] [PubMed] [Google Scholar]
- 19.Bunch JT, Dimar Ii JR. Spinal trauma in the pediatric polytrauma patient. Instr Course Lect. 2018;67:299–311. [PubMed] [Google Scholar]
- 20.Gstoettner M, Sekyra K, Walochnik N, Winter P, Wachter R, Bach CM. Inter-and intraobserver reliability assessment of the Cobb angle: manual versus digital measurement tools. Eur Spine J. 2007;16(10):1587–1592. doi: 10.1007/s00586-007-0401-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Lee HM, Kim NH, Kim HJ, Chung IH. Mid-sagittal canal diameter and vertebral body/canal ratio of the cervical spine in Koreans. Yonsei Med J. 1994;35(4):446–452. doi: 10.3349/ymj.1994.35.4.446. [DOI] [PubMed] [Google Scholar]