

Key Points
Question
Can the potential effects of different antihypertensive drug classes on psychiatric disorders be estimated using genetic data?
Findings
This genetic association study used a 2-sample mendelian randomization analysis and found that lower genetically estimated angiotensin-converting enzyme (ACE) messenger RNA and protein expression, as proxies for ACE inhibitor treatment, were associated with increased risk of schizophrenia.
Meaning
These findings warrant greater pharmacovigilance and further investigation through pharmacoepidemiology studies into the effect of ACE inhibitors, particularly those that are centrally acting, on psychiatric symptoms in patients with schizophrenia, as well as with incidence of late-onset schizophrenia.
This genetic association and mendelian randomization study estimates the potential effect of different antihypertensive drug classes on schizophrenia, bipolar disorder, and major depressive disorder.
Abstract
Importance
Observational studies have reported associations between antihypertensive medication and psychiatric disorders, although the reported direction of association appears to be dependent on drug class.
Objective
To estimate the potential effect of different antihypertensive drug classes on schizophrenia, bipolar disorder, and major depressive disorder.
Design, Setting, and Participants
This 2-sample mendelian randomization study assessed the association between a single-nucleotide variant (SNV) and drug target gene expression derived from existing expression quantitative trait loci (eQTL) data in blood (sample 1) and the SNV-disease association from published case-control genome-wide association studies (sample 2). Significant associations were corroborated using published brain eQTL and protein QTL data. Participants included 40 675 patients with schizophrenia and 64 643 controls, 20 352 patients with bipolar disorder and 31 358 controls, and 135 458 patients with major depressive disorder and 344 901 controls. Blood eQTL levels were measured in 31 684 individuals from 37 cohorts (eQTLGen consortium); prefrontal cortex eQTLs were measured from the PsychENCODE resource in 1387 individuals; and protein QTLs were measured in cerebral spinal fluid from 544 individuals and plasma from 818 individuals. Data were collected from October 4, 2019, to June 1, 2020, and analyzed from October 14, 2019, to June 6, 2020.
Exposures
Expression levels of antihypertensive drug target genes as proxies for drug exposure, and genetic variants robustly associated with the expression of these genes as mendelian randomization instruments.
Main Outcomes and Measures
Risk for schizophrenia, bipolar disorder, and major depressive disorder.
Results
A 1-SD lower expression of the angiotensin-converting enzyme (ACE) gene in blood was associated with lower systolic blood pressure of 4.0 (95% CI, 2.7-5.3) mm Hg, but increased risk of schizophrenia (odds ratio [OR], 1.75; 95% CI, 1.28-2.38; P = 3.95 × 10−4). A concordant direction of association was also observed between ACE expression in prefrontal cortex (OR, 1.33; 95% CI, 1.13-1.56) and ACE protein levels in cerebral spinal fluid (OR per 1-SD decrease, 1.12; 95% CI, 1.05-1.19) and plasma (OR per 1-SD decrease, 1.04; 95% CI, 1.01-1.07). We found no evidence for an association between genetically estimated SBP and schizophrenia risk.
Conclusions and Relevance
Findings suggest an adverse association of lower ACE messenger RNA and protein levels with schizophrenia risk. These findings warrant greater pharmacovigilance and further investigation into the effect of ACE inhibitors, particularly those that are centrally acting, on psychiatric symptoms in patients with schizophrenia, as well as the role of ACE inhibitor use in late-onset schizophrenia.
Introduction
A higher cardiovascular morbidity and mortality in individuals with psychiatric disorders has been partly attributed to both a higher incidence of risk factors for cardiovascular disease and less effective clinical management.1 Presence of risk factors for cardiovascular disease may be due to unfavorable effects of antipsychotic medication, adverse dietary habits, lack of exercise, and increased substance use. However, evidence of shared pathophysiological mechanisms also exists. A genome-wide association study (GWAS) of bipolar disorder, for example, identified genetic risk variants within the CACNA1C gene, whose encoded protein is the target of antihypertensive calcium channel blockers.2 The directionality of effect, if any, of this class of drugs on bipolar disorder remains unclear.3,4 Observational studies have reported associations between antihypertensive medication and psychiatric disorders, although the reported direction of association appears to depend on the drug class,5,6 suggesting that any effect could be independent of their blood pressure–lowering effect. Given the high prevalence of hypertension in patients with psychiatric disorders, understanding whether these medications may cause, exacerbate, or relieve neuropsychiatric symptoms will enable clinicians to make better-informed prescription decisions in comorbid individuals.
The criterion standard approach for determining a causal effect of drug treatment would be randomized clinical trials (RCTs). However, RCTs are expensive and may not always be feasible, which may explain a current lack of large, high-quality RCTs investigating the effects of antihypertensives on psychiatric disorders. Mendelian randomization (MR) is a statistical genetics approach that uses genetic variants that are robustly associated with an exposure as potentially unconfounded instruments to infer whether an observed association between the exposure and outcome is causal or not. Genetic variants that are associated with drug target messenger RNA expression or protein levels, also referred to as expression or protein quantitative trait loci (eQTLs or pQTLs, respectively), can be used as MR instruments for drug exposure (Figure 1). Given that all assumptions are satisfied (eMethods in Supplement 1), MR analysis can be used to overcome 2 major limitations of observational studies: unmeasured confounding and the ability to infer cause or consequence.7 Recent examples of MR analyses with psychiatric disorders include investigating the association of vitamin D, inflammatory biomarkers, and metabolic traits with schizophrenia risk.8,9
Figure 1. Mendelian Randomization (MR) vs Randomized Clinical Trial (RCT).

The expected outcome from a hypothetical RCT of an inhibitor drug (A) compared with MR analysis using a single-nucleotide variant (SNV) associated with drug target gene expression (expression quantitative trait loci [eQTL]) as an instrument for drug exposure (B). The eQTL SNV may exert effects on gene expression by affecting binding of transcription regulators. The presence of the T allele is associated with lower gene expression. Assuming that the difference in gene expression translates to a difference in protein activity, individuals who carry a T allele at this eQTL SNV (genotypes CT or TT) are therefore comparable to the treatment arm of the RCT, whereas those who do not carry any T allele (genotype CC) are comparable to the control arm. mRNA indicates messenger RNA.
In this study, we aimed to identify potential association of antihypertensive treatment with psychiatric disorders using a 2-sample MR analysis. We used publicly available eQTL data to identify suitable genetic instruments for blood pressure–lowering drug target gene expression (as a proxy for drug exposure). We combined these data with summary data from the most recent and largest GWAS of psychiatric disorders in a 2-sample MR analysis.
Methods
This genetic association study used only published summary data from studies involving human participants, with written informed consent and approval by their respective institutional ethics review committees. This study is covered under the University of Queensland Human Research Ethics Committee approval. We followed the Strengthening the Reporting of Observational Studies in Epidemiology–Mendelian Randomization (STROBE-MR) reporting guidelines. The full period of data collection was October 4, 2019, to June 1, 2020.
Identification of Drug Target Genes
Drug target data were collected from October 4 to 11, 2019. Using the World Health Organization Collaborating Centre for Drug Statistics Methodology, we identified different classes of blood pressure–lowering drugs, as classified by the Anatomical Therapeutic Chemical classification system, and obtained a list of active ingredients within each drug class. Genes whose protein products are targeted by any one of these active ingredients were identified using the DrugBank10 (https://go.drugbank.com/) and ChEMBL11 (https://www.ebi.ac.uk/chembl/) databases. If a gene was named as a target in only 1 database, we looked at the referenced publications to determine whether experimental evidence was sufficient for inclusion as a drug target gene.
Genetic Instruments for Drug Target Gene Expression
We used publicly available data from the eQTLGen consortium (n = 31 684)12 (eTable 1 in Supplement 2) to identify common (minor allele frequency >1%) single-nucleotide variants (SNVs) associated with the expression of antihypertensive drug target genes in blood. Only cis associations are available in the eQTLGen data (distance between SNV and gene is <1 megabase). The eQTL data are on the scale of a 1-SD change in the expression level of the gene for each additional effect allele. The SNV instrument strength was assessed using the F statistic (details provided in the eMethods in Supplement 1).
Outcome Data
We obtained publicly available (prevalent) case-control GWAS summary data for schizophrenia (40 675 cases and 64 643 controls, approximately 95% European ancestry),13 bipolar disorder (20 352 cases and 31 358 controls of European ancestry),14 and major depressive disorder (135 458 cases and 344 901 controls of European ancestry)15 (eTable 2 in Supplement 2). Further details of samples and GWA analyses are provided elsewhere.13,14,15
2-Sample MR Analysis and Genetic Instrument Validation
We used the summary-based MR (SMR) method, version 1.02,16 to perform 2-sample MR analysis (eMethods in Supplement 1). To show that changes in gene expression reflect a blood pressure–lowering association with drug exposure, we performed SMR analysis with blood gene expression (using the eQTLGen data) as exposure and systolic blood pressure (SBP) as the outcome, using summary data from a GWAS of SBP in 757 601 individuals of European ancestry17 (eTable 2 and eFigure 3 in Supplement 2). Genes whose expression in blood was not associated with SBP with at least nominal significance (ie, P ≥ .05) were excluded from further analysis. The effect size estimate from SMR for the association between gene expression and SBP represents the change (in millimeters of mercury) in SBP per 1-SD increase in gene expression.
MR Analysis With Drug Target Gene Expression in Blood and Psychiatric Outcomes
We ran an SMR analysis to estimate the association of a 1-SD change in drug target blood gene expression levels (using eQTLGen data) with outcomes of interest (using GWAS summary data for schizophrenia, bipolar disorder, and major depressive disorder). Main results are presented as the odds ratio (OR) for disease per 1-SD change in gene expression, where the direction of gene expression change is harmonized to reflect an SBP-lowering association. The effect size estimates in the main results therefore suggest the potential direction of association of antihypertensive drug exposure with risk of psychiatric disorders. Bonferroni correction for multiple testing was used to identify significant associations.
Sensitivity Analyses
Data were analyzed from October 14, 2019, to June 6, 2020. For significant MR associations, additional sensitivity analyses were performed, including assessing horizontal pleiotropy, colocalization analysis, simulation of the effect of selection bias, and ancestry-specific analyses. Where available, analyses using additional data sets were used to corroborate the main findings (eMethods in Supplement 1).
MR Analysis to Estimate the Association of SBP With Psychiatric Disorders
For significant MR associations, to determine whether the association between drug target gene expression and disease risk is likely to be mediated via changes in blood pressure or whether the association may be independent of blood pressure, we estimated the effect size for the association between genetically estimated SBP and the relevant psychiatric outcome using the generalized summary data–based MR method,18 an extension of SMR that uses multiple genetic variants associated with the risk factor to test for potential causality. We used summary data from the largest available GWAS on SBP in European individuals17 (eTable 2 in Supplement 2). Analysis was performed using generalized summary data–based MR implemented in GCTA (Genome-wide Complex Trait Analysis), version 1.91.7beta1. The default heterogeneity in dependent instrument (HEIDI) P < .01 was used to exclude pleiotropic SNVs. As sensitivity analyses, we also performed 2-sample MR analysis using other methods implemented in the TwoSampleMR, version 0.5.5, R package (R Project for Statistical Computing). Although all methods use the same underlying MR framework, the different methods have different specific assumptions that can lead to biased estimates in different situations. Agreement across methods provides more confidence that results may be robust. Analysis scripts are found at https://github.com/CNSGenomics/Antihypertensive-med.
Results
Genetic Instrument Selection
We identified a total of 110 genes whose encoded protein activity has been experimentally shown to be modified by 1 or more blood pressure–lowering drugs (eTable 3 in Supplement 2). Although 109 of 110 were reported by eQTLGen to be expressed in blood, 48 of the protein-encoding genes were absent in the meta-analyzed eQTLGen summary data, because they showed no variation in expression across samples and were filtered out during meta-analysis. We were therefore only able to query the eQTL data for 61 of the 110 drug target genes. For all 61 genes, the most significant cis-eQTL SNVs selected as genetic instruments had F statistics of greater than 10 (eTable 4 in Supplement 2). Of the 61 genes, 22 had gene expression levels in blood that were associated with SBP at nominal significance (SMR P < .05) (eTable 4 in Supplement 2), and these were taken forward to the main analysis.
MR Analysis With Blood Gene Expression and Psychiatric Outcomes
Using a significance threshold of P < 7.58 × 10−4 (Bonferroni correction for association testing of 22 genes with 3 disease phenotypes) and a HEIDI P ≥ .01 to rule out association due to linkage, we found that a 1-SD decrease in blood ACE expression (target for ACE inhibitors) was associated with a decrease in SBP of 4.0 (95% CI, 2.7-5.3) mm Hg and a higher risk of schizophrenia (OR, 1.75; 95% CI, 1.28-2.38; P = 3.95 × 10−4) (Figure 2A). Colocalization analysis gave a posterior probability of 85% for a common variant for ACE (OMIM 106180) expression and schizophrenia risk. Although expression of CYP17A1 (OMIM 609300; targeted by spironolactone, a potassium-sparing diuretic) and NISCH (OMIM 615507; targeted by moxonidine, a new-generation α-2/imidazoline receptor agonist) were associated with schizophrenia and bipolar disorder, the significant HEIDI P values suggest these associations were likely due to linkage. This possibility is corroborated by the low to moderate posterior probabilities for a common variant for these associations (<0.1% for CYP17A1 expression and schizophrenia risk, 53% for CYP17A1 expression and bipolar disorder risk, <0.1% for NISCH expression and schizophrenia risk, 36% for NISCH expression and bipolar disorder risk). These associations were therefore not taken forward for further analyses. The SMR results from the analysis between expression of the 22 drug target genes in blood with the 3 psychiatric disorders are provided in eTables 5 to 7 in Supplement 2. We observed concordant direction of association between ACE expression and schizophrenia risk using schizophrenia GWAS data from European ancestry–only and East Asian ancestry–only samples (eTable 8 in Supplement 2).
Figure 2. Association of Drug Target Gene Expression in Blood With Disease Risk.
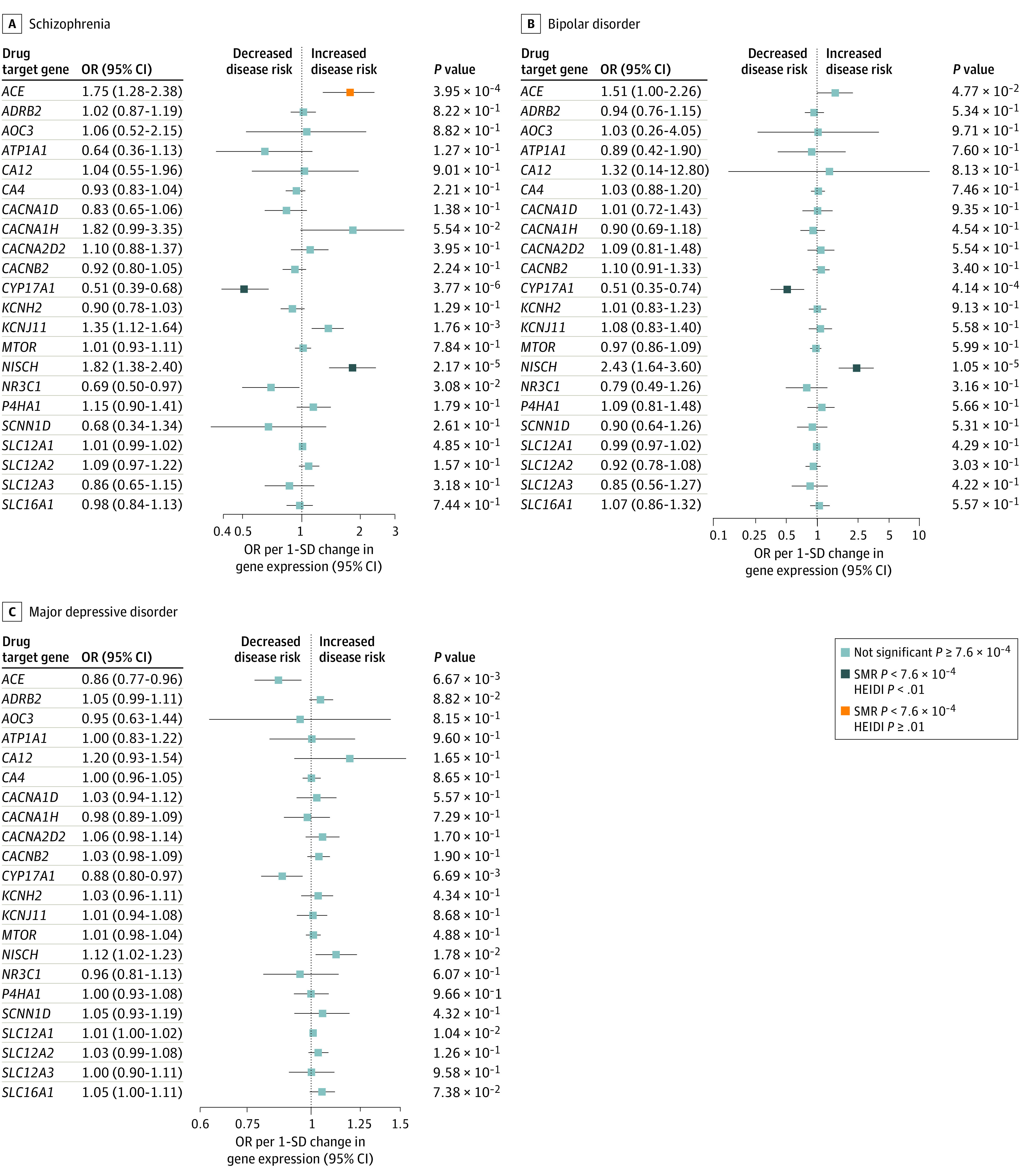
Forest plot of the association between a 1-SD change in expression of 22 blood pressure–lowering drug target genes in blood with risk for schizophrenia (A), bipolar disorder (B), and major depressive disorder (C). Data are represented as odds ratios (ORs) with 95% CI (error bars). The direction of gene expression change reflects the systolic blood pressure–lowering association. Therefore, an OR of greater than 1.00 suggests an increased risk of disease associated with blood pressure–lowering drug treatment. Associations are statistically significant after correcting for multiple testing (22 genes x 3 phenotypes) and have a heterogeneity in dependent instrument (HEIDI) P ≥ .01, statistically significant after correcting for multiple testing but have a HEIDI P < .01 (indicating association likely due to linkage) or did not pass the multiple testing correction. SMR indicates summary-based mendelian randomization.
Sensitivity Analyses
MR Analysis of ACE Brain Expression
The eQTL SNP instrument for expression of ACE in brain prefrontal cortex (rs6504163) was in high linkage disequilibrium with the blood eQTL (r2 = 0.93 in individuals of European ancestry). As observed in blood samples, lower ACE expression in the prefrontal cortex was associated with higher risk of schizophrenia (OR, 1.33; 95% CI, 1.13-1.56; P = 5.69 × 10−4) (Figure 3). We observed concordant direction of association using schizophrenia GWAS data from individuals of European and East Asian ancestry (eTable 8 in Supplement 2). Extending analysis to other brain regions, significant associations between ACE expression with schizophrenia risk were observed for cortex regions, cerebellum, and cerebral hemisphere after multiple testing correction (P < 3.57 × 10−3) (Figure 3).
Figure 3. Mendelian Randomization (MR) Analysis of Angiotensin-Converting Enzyme (ACE) Gene Expression in Brain Tissue With Risk of Schizophrenia.
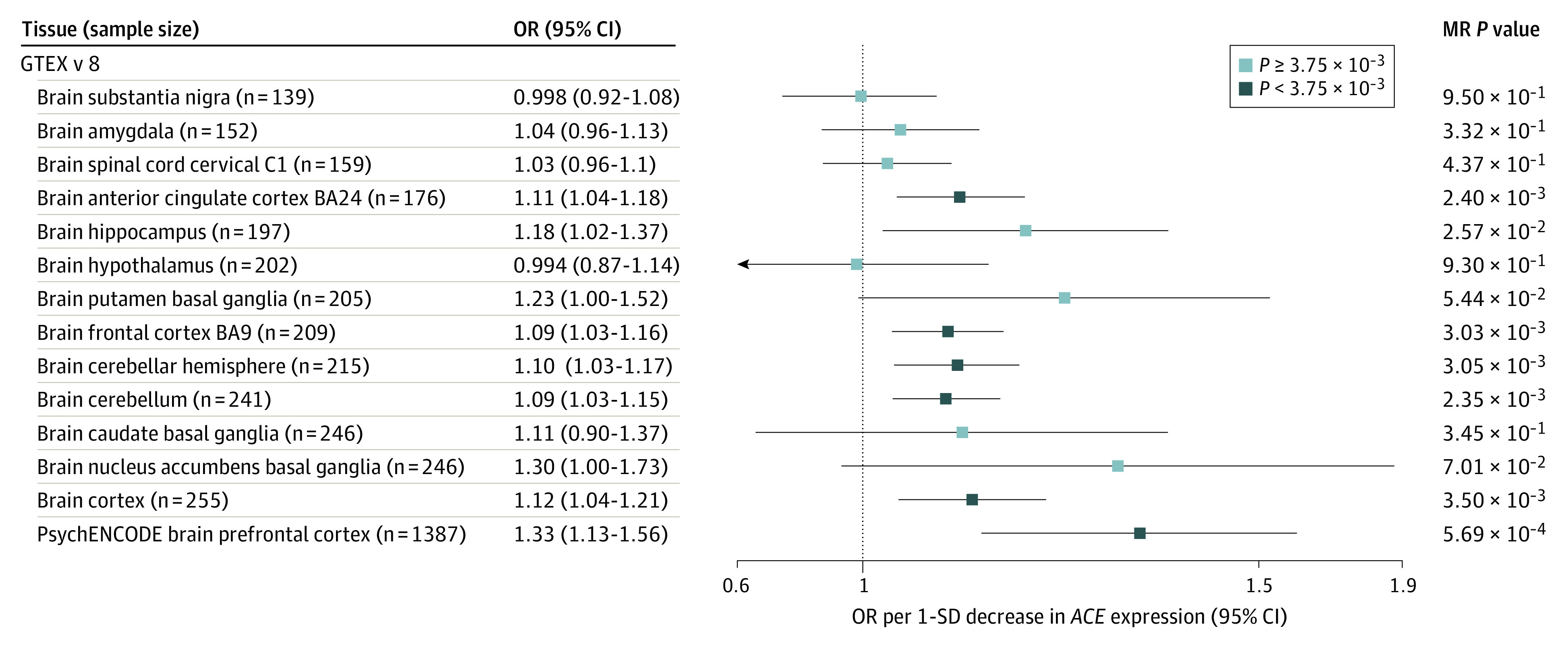
Forest plot showing the odds ratio (OR) and 95% CI (error bars) for schizophrenia risk per 1-SD decrease in ACE gene expression in different brain regions. Expression quantitative trait loci data were queried for 13 different brain regions from GTEX v8 and the prefrontal cortex region from PsychENCODE databases. Associations are statistically significant after correcting for 14 tests or did not pass the multiple testing correction. BA indicates Brodmann area.
Assessing the ACE eQTL for Horizontal Pleiotropy
The eQTL SNV instrument for ACE expression in blood (rs4277405) was also associated with the expression of 10 adjacent genes at P < .05, including 5 genes at P < 1×10−5 (FTSJ3 [OMIM 618411], TANC2 [OMIM 615047], SMARDC2 [OMIM 601736], ICAM2 [OMIM 146630], and STRADA [OMIM 608626]) in blood samples (eTable 9 in Supplement 2). However, SMR and colocalization analyses did not provide any evidence of an association between expression of these adjacent genes with schizophrenia (eTable 10 in Supplement 2) and, therefore, no evidence for horizontal pleiotropy.
MR Analysis Using a Proxy for the ACE Insertion/Deletion as an Instrument
We used rs4343, a proxy for the ACE indel that has previously been associated with ACE activity19 and is not highly correlated with the ACE blood eQTL rs4277405 (r2 = 0.35 in individuals of European ancestry), as an instrument. We observed a concordant direction of association of a 1-SD decrease in ACE gene expression in blood with lower SBP (β = −2.40 mm Hg; SE, 0.76 mm Hg; P = 1.75 × 10−3), and higher risk of schizophrenia (OR, 1.81; 95% CI, 1.36-2.26; P = 9.40 × 10−3) (eTable 11 in Supplement 2).
MR Analysis of Renin-Angiotensin System Pathway Genes
Because AGT (OMIIM 106150), AGTR1 (OMIM 106165), and REN (OMIM 179820) were absent in the blood eQTL summary data set, we queried brain eQTL data. The eQTL SNV instruments for expression of AGT, AGTR1, and REN in brain tissue all had F statistics of greater than 10. We found no evidence of an association between expression of these 3 renin-angiotensin system (RAS) pathway genes in brain tissue and schizophrenia risk (eTable 12 in Supplement 2).
MR Analysis Using ACE Protein Levels in Plasma and Cerebral Spinal Fluid
Using summary data from GWAS of plasma and cerebrospinal fluid ACE levels, a 1-SD decrease in ACE protein levels in plasma (OR, 1.04; 95% CI, 1.01-1.07; P = 4.41 × 10−3) and cerebrospinal fluid (OR, 1.12; 95% CI, 1.05-1.19; P = 9.44 × 10−4) were associated with increased schizophrenia risk. We observed concordant effect sizes using a multi-SNV MR approach that included 1 cis and 1 trans-SNV associated with plasma ACE levels (eFigure 1 in Supplement 1). Reverse MR analysis found no association of schizophrenia case-control status with ACE protein levels (eTable 13 in Supplement 2). The results of these sensitivity analyses of ACE and schizophrenia risk are summarized in eFigure 2 in Supplement 1.
MR Analysis of Blood Pressure and Schizophrenia Risk
Using 727 SNVs that were independently associated at genome-wide significance (GWAS association P < 5 × 10−8) with SBP as MR instruments (after HEIDI outlier filtering to remove pleiotropic SNVs), we found no evidence to support an association between genetically estimated SBP and schizophrenia risk (OR per 1–mm Hg increase, 1.00; 95% CI, 0.99-1.00; P = .14) (eFigure 3 in Supplement 1). Results were consistent without HEIDI outlier filtering and using other MR methods (eTable 14 in Supplement 2).
Discussion
We used QTL and GWAS summary data in a 2-sample MR analysis to infer potential effects of antihypertensive medication on psychiatric disorders. Lower expression of the ACE gene, a target for ACE inhibitors, was associated with decreased SBP but increased risk of schizophrenia. A summary of the study design and results is shown in Figure 4. We found no evidence for an association between genetically estimated SBP and schizophrenia risk. This suggests that even small potential effects of blood pressure on schizophrenia are unlikely and implies that any association of ACE with schizophrenia is likely to be independent of its association with blood pressure.
Figure 4. Summary of Study Design and Results.

ACE indicates angiotensin-converting enzyme; BP, blood pressure; bxy, estimated effect of the exposure on outcome; eQTL, expression quantitative trait loci; GWAS, genome-wide association study; HEIDI, heterogeneity in dependent instrument; MR, mendelian randomization; SBP, systolic BP; SMR, summary-based MR; SNV, single-nucleotide variant; and WHOCC, World Health Organization Collaborating Centre.
ACE is a component of the RAS that regulates blood pressure. In addition to the circulating RAS, nearly all organs of the body have their own local paracrinelike RAS, with organ-specific actions.20 Although we were unable to test the association between expression of other RAS components in blood, we found little evidence for an association between expression in brain tissues of other RAS pathway genes, namely AGT, AGTR1, and REN, with schizophrenia risk. Larger brain eQTL data sets would be needed to rule out small but clinically relevant effects of these genes. ACE consists of 2 catalytic domains, the C-domain and N-domain. The N-domain has been shown to bind multiple substrates with varying affinities.21 The location of ACE on the cellular membrane of neurons and its ability to cleave several neuropeptides suggests a role for ACE in central nervous system functions. ACE has also been shown to play a role in innate and adaptive immunity,22 which is also implicated in the pathogenesis of schizophrenia.23
Comparison With Other Studies
An MR analysis of antihypertensive drug exposure and risk of psychiatric disorders has not been previously conducted. Observational studies have reported contradictory associations. Boal et al5 found that calcium channel antagonists and β-blockers were associated with increased risk of mood disorder admissions, whereas users of drugs targeting the RAS pathway had the lowest risk. Hayes et al6 found reduced rates of psychiatric hospitalization and self-harm in patients with bipolar disorder and schizophrenia who were treated with calcium channel antagonists, but the investigators did not look at other antihypertensive drug classes. A systematic review of 23 studies investigating verapamil hydrochloride, a calcium channel blocker, in acute mania, found no evidence of an effect.3
Previous genetic studies24,25 have identified an association between the ACE insertion/deletion and schizophrenia; however, the findings have been contradictory. Similarly, paradoxical findings can be found for ACE activity and protein levels when comparing patients with schizophrenia with controls.26,27 The Schizophrenia Working Group of the Psychiatric Genetics Consortium28 recently published a preprint of the latest schizophrenia GWAS, consisting of 39 369 cases and 236 642 controls. They report variants within the ACE gene reaching genome-wide significance for the first time and SMR analysis showing an association of decreased ACE expression in blood with increased risk of schizophrenia, corroborating our findings.
Strengths and Limitations
This study has some particular strengths. Human genetics is an increasingly crucial source of evidence guiding the selection of new targets for drug discovery as well as evaluating drug safety.29,30 Loss-of-function mutations in the drug target genes would make for ideal MR instruments. However, given such variants are very rare, an MR study using loss-of-function variants would not currently be feasible.31 Alternatively, eQTL variants can be used as MR instruments. Two-sample MR analysis allows us to use the largest available GWAS and eQTL data sets to investigate causality by overcoming some of the caveats of observational studies and RCTs, such as sample size, confounding bias, and feasibility, while using cis-SNVs to instrument messenger RNA or protein expression minimizes the potential for horizontal pleiotropy, which would violate an assumption of MR.
Several sensitivity analyses suggest a robust association between ACE expression and schizophrenia. Figure 5 summarizes the possible scenarios that may lead to the observed association between ACE expression and schizophrenia risk and the analyses performed to assess these scenarios.
Figure 5. Possible Explanations for Observed Association in Mendelian Randomization (MR) Analysis Between Angiotensin-Converting Enzyme (ACE) Gene Expression and Schizophrenia Risk.

A, ACE has an effect on schizophrenia that is independent of its effect on blood pressure, assessed by MR analysis using blood pressure as exposure. B, The effect of ACE on schizophrenia risk is mediated through blood pressure change, assessed by MR analysis using blood pressure as exposure. C, The ACE expression quantitative trait loci (eQTL) single-nucleotide variant (SNV) instrument is also associated with expression of another gene. Schizophrenia risk is mediated through this gene rather than through ACE and assessed by MR and colocalization analysis of other genes associated with the ACE SNV instrument. D, Linkage association, whereby 2 SNVs are in linkage disequilibrium. One SNV affects ACE expression whereas the other affects schizophrenia risk through its effect on expression of another gene. The association is assessed by heterogeneity in dependent instrument test and colocalization analysis.
In terms of limitations, reduced life expectancy in individuals with schizophrenia may be accelerated by the presence of cardiovascular disease. This could lead to survival bias in case-control GWAS data, because studies included prevalent cases. However, our simulations show that the observed association is unlikely to be driven by selection bias (eTables 15 and 16 in Supplement 1).
This study assumes that changes in gene expression may reflect changes in protein levels and/or activity, which may not always be the case. Therefore, lack of association in our analysis does not necessarily mean lack of biological effect of drug treatment, but rather lack of evidence that change in drug target gene expression in the tested tissues is not associated with outcome, which could also reflect power to detect an outcome (for power calculations, see eTables 18-20 in Supplement 1). The effect sizes estimated from MR analysis may not reflect the true effect of drug exposure. Variables such as drug dose, duration of exposure, interindividual variation in drug metabolism, ability to reach the tissue of relevance (eg, cross the blood-brain barrier), and drug-binding affinity all play a role in modifying drug efficacy and toxicity, making it difficult to extrapolate the actual effect of drug exposure from genetic analyses.
The power to conduct tissue-specific analysis is currently restricted by sample size of available eQTL data sets. Although relatively high correlation has been observed between blood and brain eQTLs,32 any extrapolation will be restricted to genes that are expressed and have eQTLs in both. Given the small brain eQTL sample sizes and varying instrument strength in the different brain regions (eTable 17 in Supplement 1), smaller but clinically relevant effects of ACE expression in other brain regions cannot be ruled out.
Genetic variants may reflect the effect of lifelong exposure on an outcome. Although results from these analyses cannot be directly translated into effects of short-term drug treatment on disease risk, they may prove useful in estimating effects of long-term exposure beyond what is feasible in RCTs.
Conclusions
In this study, we found an adverse association of lower ACE messenger RNA and protein levels with schizophrenia risk, with sensitivity analyses suggesting that any association of ACE with schizophrenia risk is likely to be independent of its association with blood pressure. Although approximately 20% of individuals with schizophrenia are reported to have late-onset disease (>40 years of age),33 for most patients, onset occurs in late adolescence or early adult life, ruling out ACE inhibitor treatment as a potential causal factor for most cases. However, if lower ACE levels play a causal role for schizophrenia risk, it would be reasonable to hypothesize that further lowering of ACE activity in existing patients could worsen symptoms or trigger a new episode. We cannot draw full conclusions with statistical evidence alone, and these results are not sufficient to justify changes to current prescription guidelines, especially given their known beneficial cardiovascular effects. However, given that visual hallucinations and reversible psychosis have been reported after ACE inhibitor treatment,34,35,36,37,38 our findings warrant further research into the functional role of ACE in schizophrenia, as well as greater pharmacovigilance. Access to massive electronic health record databases provide the opportunity to conduct pharmacoepidemiological studies to look at the association between ACE inhibitor use and psychiatric symptoms, hospitalization, and mortality in patients with schizophrenia, or with the incidence of late-onset schizophrenia. However, the issue of sample size for the latter, given the low prevalence, and inaccurate recording of psychiatric symptoms, are important considerations for such studies in the future.
eMethods. MR Analysis
eFigure 1. Multi-SNP MR for ACE Protein Levels and Schizophrenia Risk
eFigure 2. Summary of Results From Sensitivity Analyses of the Effect of ACE Gene Expression or Protein Levels on Schizophrenia Risk
eFigure 3. MR Analysis of Systolic Blood Pressure as Exposure With Schizophrenia Risk
eTable 15. Estimates of bxy Under the Null With Selection Bias
eTable 16. Estimates of bxy Under the Causality With Selection Bias
eTable 17. Association Between ACE Brain Expression and Schizophrenia Risk
eTable 18. Association Between Blood Gene Expression and Schizophrenia Risk
eTable 19. Association Between Blood Gene Expression and Bipolar Disorder
eTable 20. Association Between Blood Gene Expression and Major Depression
eReferences.
eTable 1. Expression Quantitative Trait Loci (eQTL) Datasets
eTable 2. Genome-wide Association Studies Used in Mendelian Randomization Analysis
eTable 3. Target Genes for Antihypertensive Drug Classes Identified Using DrugBank and ChEMBL Databases
eTable 4. MR Association Between Drug Target Gene Expression in Blood and Systolic Blood Pressure
eTable 5. MR Association Between Drug Target Gene Expression in Blood and Schizophrenia Risk
eTable 6. MR Association Between Drug Target Gene Expression in Blood and Bipolar Disorder Risk
eTable 7. MR Association Between Drug Target Gene Expression in Blood and Major Depressive Disorder Risk
eTable 8. MR Association Between ACE Gene Expression in Blood and Prefrontal Cortex With Schizophrenia Risk
eTable 9. Association Between ACE eQTL SNV in Blood (rs4277405) With Expression of Other Nearby Genes
eTable 10. MR Association Between Expression in Blood of Genes Surrounding ACE and Schizophrenia Risk
eTable 11. MR Analysis Using rs4343 as an Instrument for ACE Expression in Blood and Psychiatric Disorders as Outcome
eTable 12. MR Association Between Expression of Renin-Angiotensin Pathway Genes in Brain and Schizophrenia Risk
eTable 13. Effect of Schizophrenia Risk on ACE Plasma and CSF Levels
eTable 14. Causal Estimates From Different MR Methods for the Association of Systolic Blood Pressure With Schizophrenia Risk
References
- 1.Ayerbe L, Forgnone I, Addo J, Siguero A, Gelati S, Ayis S. Hypertension risk and clinical care in patients with bipolar disorder or schizophrenia: a systematic review and meta-analysis. J Affect Disord. 2018;225:665-670. doi: 10.1016/j.jad.2017.09.002 [DOI] [PubMed] [Google Scholar]
- 2.Ferreira MAR, O’Donovan MC, Meng YA, et al. ; Wellcome Trust Case Control Consortium . Collaborative genome-wide association analysis supports a role for ANK3 and CACNA1C in bipolar disorder. Nat Genet. 2008;40(9):1056-1058. doi: 10.1038/ng.209 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Cipriani A, Saunders K, Attenburrow M-J, et al. A systematic review of calcium channel antagonists in bipolar disorder and some considerations for their future development. Mol Psychiatry. 2016;21(10):1324-1332. doi: 10.1038/mp.2016.86 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Dubovsky SL. Applications of calcium channel blockers in psychiatry: pharmacokinetic and pharmacodynamic aspects of treatment of bipolar disorder. Expert Opin Drug Metab Toxicol. 2019;15(1):35-47. doi: 10.1080/17425255.2019.1558206 [DOI] [PubMed] [Google Scholar]
- 5.Boal AH, Smith DJ, McCallum L, et al. Monotherapy with major antihypertensive drug classes and risk of hospital admissions for mood disorders. Hypertension. 2016;68(5):1132-1138. doi: 10.1161/HYPERTENSIONAHA.116.08188 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hayes JF, Lundin A, Wicks S, et al. Association of hydroxylmethyl glutaryl coenzyme A reductase inhibitors, L-type calcium channel antagonists, and biguanides with rates of psychiatric hospitalization and self-harm in individuals with serious mental illness. JAMA Psychiatry. 2019;76(4):382-390. doi: 10.1001/jamapsychiatry.2018.3907 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Davies NM, Holmes MV, Davey Smith G. Reading mendelian randomisation studies: a guide, glossary, and checklist for clinicians. BMJ. 2018;362:k601. doi: 10.1136/bmj.k601 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Revez JA, Lin T, Qiao Z, et al. Genome-wide association study identifies 143 loci associated with 25 hydroxyvitamin D concentration. Nat Commun. 2020;11(1):1647. doi: 10.1038/s41467-020-15421-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Lin BD, Alkema A, Peters T, et al. Assessing causal links between metabolic traits, inflammation and schizophrenia: a univariable and multivariable, bidirectional Mendelian-randomization study. Int J Epidemiol. 2019;48(5):1505-1514. doi: 10.1093/ije/dyz176 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Wishart DS, Knox C, Guo AC, et al. DrugBank: a comprehensive resource for in silico drug discovery and exploration. Nucleic Acids Res. 2006;34(Database issue):D668-D672. doi: 10.1093/nar/gkj067 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Gaulton A, Hersey A, Nowotka M, et al. The ChEMBL database in 2017. Nucleic Acids Res. 2017;45(D1):D945-D954. doi: 10.1093/nar/gkw1074 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Võsa U, Claringbould A, Westra H-J, et al. Unraveling the polygenic architecture of complex traits using blood eQTL meta-analysis. Posted online October 19, 2018. bioRxiv. doi: 10.1101/447367 [DOI]
- 13.Pardiñas AF, Holmans P, Pocklington AJ, et al. ; GERAD1 Consortium; CRESTAR Consortium . Common schizophrenia alleles are enriched in mutation-intolerant genes and in regions under strong background selection. Nat Genet. 2018;50(3):381-389. doi: 10.1038/s41588-018-0059-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Stahl EA, Breen G, Forstner AJ, et al. ; eQTLGen Consortium; BIOS Consortium; Bipolar Disorder Working Group of the Psychiatric Genomics Consortium . Genome-wide association study identifies 30 loci associated with bipolar disorder. Nat Genet. 2019;51(5):793-803. doi: 10.1038/s41588-019-0397-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Howard DM, Adams MJ, Clarke T-K, et al. ; 23andMe Research Team; Major Depressive Disorder Working Group of the Psychiatric Genomics Consortium . Genome-wide meta-analysis of depression identifies 102 independent variants and highlights the importance of the prefrontal brain regions. Nat Neurosci. 2019;22(3):343-352. doi: 10.1038/s41593-018-0326-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Zhu Z, Zhang F, Hu H, et al. Integration of summary data from GWAS and eQTL studies predicts complex trait gene targets. Nat Genet. 2016;48(5):481-487. doi: 10.1038/ng.3538 [DOI] [PubMed] [Google Scholar]
- 17.Evangelou E, Warren HR, Mosen-Ansorena D, et al. ; Million Veteran Program . Genetic analysis of over 1 million people identifies 535 new loci associated with blood pressure traits. Nat Genet. 2018;50(10):1412-1425. doi: 10.1038/s41588-018-0205-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Zhu Z, Zheng Z, Zhang F, et al. Causal associations between risk factors and common diseases inferred from GWAS summary data. Nat Commun. 2018;9(1):224. doi: 10.1038/s41467-017-02317-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Chung C-M, Wang R-Y, Chen J-W, et al. A genome-wide association study identifies new loci for ACE activity: potential implications for response to ACE inhibitor. Pharmacogenomics J. 2010;10(6):537-544. doi: 10.1038/tpj.2009.70 [DOI] [PubMed] [Google Scholar]
- 20.Villar-Cheda B, Costa-Besada MA, Valenzuela R, Perez-Costas E, Melendez-Ferro M, Labandeira-Garcia JL. The intracellular angiotensin system buffers deleterious effects of the extracellular paracrine system. Cell Death Dis. 2017;8(9):e3044. doi: 10.1038/cddis.2017.439 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Deddish PA, Marcic B, Jackman HL, Wang HZ, Skidgel RA, Erdös EG. N-domain-specific substrate and C-domain inhibitors of angiotensin-converting enzyme: angiotensin-(1-7) and keto-ACE. Hypertension. 1998;31(4):912-917. doi: 10.1161/01.HYP.31.4.912 [DOI] [PubMed] [Google Scholar]
- 22.Bernstein KE, Khan Z, Giani JF, Cao D-Y, Bernstein EA, Shen XZ. Angiotensin-converting enzyme in innate and adaptive immunity. Nat Rev Nephrol. 2018;14(5):325-336. doi: 10.1038/nrneph.2018.15 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Khandaker GM, Cousins L, Deakin J, Lennox BR, Yolken R, Jones PB. Inflammation and immunity in schizophrenia: implications for pathophysiology and treatment. Lancet Psychiatry. 2015;2(3):258-270. doi: 10.1016/S2215-0366(14)00122-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Mazaheri H, Saadat M. Association between insertion/deletion polymorphism in angiotension converting enzyme and susceptibility to schizophrenia. Iran J Public Health. 2015;44(3):369-373. [PMC free article] [PubMed] [Google Scholar]
- 25.Song GG, Lee YH. The insertion/deletion polymorphism in the angiotensin-converting enzyme and susceptibility to schizophrenia or Parkinson’s disease: a meta-analysis. J Renin Angiotensin Aldosterone Syst. 2015;16(2):434-442. doi: 10.1177/1470320313495909 [DOI] [PubMed] [Google Scholar]
- 26.Mohite S, de Campos-Carli SM, Rocha NP, et al. Lower circulating levels of angiotensin-converting enzyme (ACE) in patients with schizophrenia. Schizophr Res. 2018;202:50-54. doi: 10.1016/j.schres.2018.06.023 [DOI] [PubMed] [Google Scholar]
- 27.Gadelha A, Vendramini AM, Yonamine CM, et al. Convergent evidences from human and animal studies implicate angiotensin I-converting enzyme activity in cognitive performance in schizophrenia. Transl Psychiatry. 2015;5:e691. doi: 10.1038/tp.2015.181 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Schizophrenia Working Group of the Psychiatric Genomics Consortium . Mapping genomic loci prioritises genes and implicates synaptic biology in schizophrenia. Posted September 13, 2020. medRxiv. doi: 10.1101/2020.09.12.20192922 [DOI]
- 29.Nelson MR, Tipney H, Painter JL, et al. The support of human genetic evidence for approved drug indications. Nat Genet. 2015;47(8):856-860. doi: 10.1038/ng.3314 [DOI] [PubMed] [Google Scholar]
- 30.King EA, Davis JW, Degner JF. Are drug targets with genetic support twice as likely to be approved? Revised estimates of the impact of genetic support for drug mechanisms on the probability of drug approval. PLoS Genet. 2019;15(12):e1008489. doi: 10.1371/journal.pgen.1008489 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Minikel EV, Karczewski KJ, Martin HC, et al. ; Genome Aggregation Database Production Team; Genome Aggregation Database Consortium . Evaluating drug targets through human loss-of-function genetic variation. Nature. 2020;581(7809):459-464. doi: 10.1038/s41586-020-2267-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Qi T, Wu Y, Zeng J, et al. ; eQTLGen Consortium . Identifying gene targets for brain-related traits using transcriptomic and methylomic data from blood. Nat Commun. 2018;9(1):2282. doi: 10.1038/s41467-018-04558-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Harris MJ, Jeste DV. Late-onset schizophrenia: an overview. Schizophr Bull. 1988;14(1):39-55. doi: 10.1093/schbul/14.1.39 [DOI] [PubMed] [Google Scholar]
- 34.Doane J, Stults B. Visual hallucinations related to angiotensin-converting enzyme inhibitor use: case reports and review. J Clin Hypertens (Greenwich). 2013;15(4):230-233. doi: 10.1111/jch.12063 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Gillman MA, Sandyk R. Reversal of captopril-induced psychosis with naloxone. Am J Psychiatry. 1985;142(2):270. doi: 10.1176/ajp.142.2.270a [DOI] [PubMed] [Google Scholar]
- 36.Ahmad S. Enalapril-induced acute psychosis. Ann Pharmacother. 1991;25(5):558-559. doi: 10.1177/106002809102500518 [DOI] [PubMed] [Google Scholar]
- 37.Ahmad S. Losartan and reversible psychosis. Cardiology. 1996;87(6):569-570. doi: 10.1159/000177156 [DOI] [PubMed] [Google Scholar]
- 38.Tarlow MM, Sakaris A, Scoyni R, Wolf-Klein G. Quinapril-associated acute psychosis in an older woman. J Am Geriatr Soc. 2000;48(11):1533. doi: 10.1111/jgs.2000.48.11.1533 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eMethods. MR Analysis
eFigure 1. Multi-SNP MR for ACE Protein Levels and Schizophrenia Risk
eFigure 2. Summary of Results From Sensitivity Analyses of the Effect of ACE Gene Expression or Protein Levels on Schizophrenia Risk
eFigure 3. MR Analysis of Systolic Blood Pressure as Exposure With Schizophrenia Risk
eTable 15. Estimates of bxy Under the Null With Selection Bias
eTable 16. Estimates of bxy Under the Causality With Selection Bias
eTable 17. Association Between ACE Brain Expression and Schizophrenia Risk
eTable 18. Association Between Blood Gene Expression and Schizophrenia Risk
eTable 19. Association Between Blood Gene Expression and Bipolar Disorder
eTable 20. Association Between Blood Gene Expression and Major Depression
eReferences.
eTable 1. Expression Quantitative Trait Loci (eQTL) Datasets
eTable 2. Genome-wide Association Studies Used in Mendelian Randomization Analysis
eTable 3. Target Genes for Antihypertensive Drug Classes Identified Using DrugBank and ChEMBL Databases
eTable 4. MR Association Between Drug Target Gene Expression in Blood and Systolic Blood Pressure
eTable 5. MR Association Between Drug Target Gene Expression in Blood and Schizophrenia Risk
eTable 6. MR Association Between Drug Target Gene Expression in Blood and Bipolar Disorder Risk
eTable 7. MR Association Between Drug Target Gene Expression in Blood and Major Depressive Disorder Risk
eTable 8. MR Association Between ACE Gene Expression in Blood and Prefrontal Cortex With Schizophrenia Risk
eTable 9. Association Between ACE eQTL SNV in Blood (rs4277405) With Expression of Other Nearby Genes
eTable 10. MR Association Between Expression in Blood of Genes Surrounding ACE and Schizophrenia Risk
eTable 11. MR Analysis Using rs4343 as an Instrument for ACE Expression in Blood and Psychiatric Disorders as Outcome
eTable 12. MR Association Between Expression of Renin-Angiotensin Pathway Genes in Brain and Schizophrenia Risk
eTable 13. Effect of Schizophrenia Risk on ACE Plasma and CSF Levels
eTable 14. Causal Estimates From Different MR Methods for the Association of Systolic Blood Pressure With Schizophrenia Risk