

Abstract
The aims of this study were to translate the International Skin Tear Advisory Panel (ISTAP) classification system for skin tears into Swedish and to validate the translated system. The research process consisted of two phases. Phase I involved the translation of the classification system, using the forward‐back translation method, and a consensus survey. The survey dictated that the best Swedish translation for “skin tear” was “hudfliksskada.” In Phase 2, the classification system was validated by health care professionals attending a wound care conference held in the spring of 2017 in Sweden. Thirty photographs representing three types of skin tear were presented to participants in random order. Participants were directed to classify the skin tear types in a data collection sheet. The results indicated a moderate level of agreement on classification of skin tears by type. Achieving moderate agreement for the ISTAP skin tear tool is an important milestone as it demonstrates the validity and reliability of the tool. Skin tear classification typing is a complex skill that requires training and time to develop. More education is required for all health care specialists on the classification of skin tears.
Keywords: classification system, skin tears, validation
1. INTRODUCTION
Skin tears are acute wounds caused by shear forces, friction, and/or other blunt trauma to the skin, which results in the skin's layers being separated from each other. A skin tear can either be partial—that is, the epidermis is separated from the dermis—or it may be a full‐bodied injury, where both the epidermis and dermis are separated from underlying structures.1, 2 Common complications of these wounds are pain and infection, and the risk of delayed wound healing is high.3 In a recently published systematic literature review, it was shown that the most prevalent risk factors for skin tears are old age, followed by impaired mobility, falls and accidental injuries, previous skin tears, cognitive deficit/dementia, and dependence in transfer.4
The presence of skin tears is underreported but is believed to be as, or even more, common than pressure ulcers.1 Among elderly nursing home residents, the prevalence of skin tears has been reported to be 22%5 and between 6% and 11%6, 7 in acute care. Carville et al. followed patients in elderly care over time and found an incidence of 10.6%.8
As with all wound types, skin tears should be assessed and documented in a consistent manner to enable the follow up of wound healing and evaluation of given treatment. Through consistent documentation, the extent and consequences of these types of injury can be mapped and interventions evaluated.3 However, until recently, there has been no uniform definition and classification of skin tears. To increase awareness of this largely unheeded health care issue, the International Skin Tear Advisory Panel (ISTAP) established consensus statements on the prevention, identification, assessment, and treatment of skin tears and developed a validated skin tear classification system.2, 9 The ISTAP Skin Tear Classification System includes three skin tear types: no skin loss, partial skin loss, or complete skin loss (Figure 1A). The system was developed in English9 and has been translated into Danish and validated.10 LeBlanc et al. (2018) report that the translation and validation of the system is underway in French, Italian, Chinese, Portuguese, Spanish, and Czech (Personal correspondence with Kimberly LeBlanc, February 29, 2018). Using the ISTAP classification could also be valuable in Sweden, but just as in other countries, it needs to be translated into the local language and validated before being used.
Figure 1.
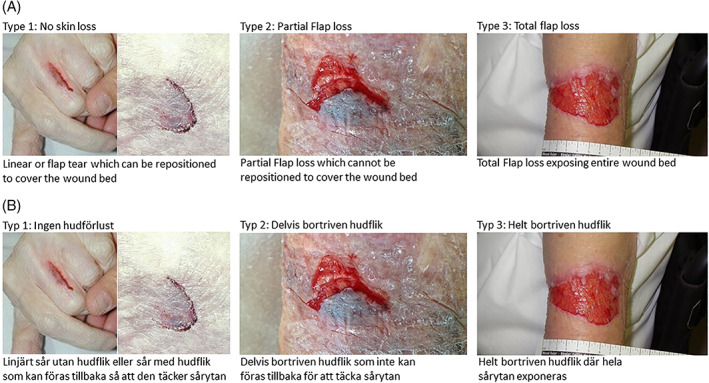
ISTAP skin tear classification system in English and Swedish. A, ISTAP skin tear classification. B, ISTAPs‐klassificering av hudfliksskada (laceration) [Colour figure can be viewed at wileyonlinelibrary.com]
1.1. Aim
The aims of this study were to translate the ISTAP classification system for skin tears into Swedish and to validate the translated system.
2. MATERIALS AND METHODS
The ISTAP Skin Tear Classification System was translated into Swedish using a forward‐back translation method according to Wild et al.10 The research process in the present study consisted of two phases as described here.
2.1. Phase I—Translation into Swedish
2.1.1. Ia—Translation of the ISTAP classification system
The ISTAP classification system was translated into Swedish using the forward‐back translation method described by Wild et al.11 First, the ISTAP classification system was translated from English into Swedish by an independent professional translator. Two of the authors of this study (UK and CB) reviewed the translation, initially independently of each other and then together, to subsequently agree on a version. The final Swedish version was thereafter translated back into English by a different independent professional translator. The revised English version was then finally compared with the original and was approved by the ISTAP co‐chairs (KLB) (Figure 1B).
2.1.2. Ib—Consensus regarding Swedish translation of the word “skin tear”
During the translation process, it became clear that the term “skin tear” was not easily translated into Swedish. This led to us conducting a survey among wound care specialists around Sweden to find the best Swedish translation of the term. First, a web questionnaire was sent by e‐mail to: (1) physicians in the Swedish Society for Dermatology and Venereology Dermatology, (2) registered nurses (RN) in the society of the Swedish Dermatology and Venerology Nurses Association, and (3) RN in the Swedish Wound Care Nurses Association. The primary question was: do you agree or disagree that “hudflikslesion” is an appropriate translation for “skin tear”? If not, what do you suggest instead? In total, 145 health care professionals participated in this online survey—44 physicians and 101 RN. The majority thought that “hudflikslesion” was not the best translation (60.7%, n = 88). For this reason we conducted a second web questionnaire by e‐mail to the same societies, asking their members to instead select the best translation for “skin tear” from the list of terms that were most frequently suggested in the first survey. These included “hudreva”, “hudfliksskada,” and “hudskada med hudflik.” In this second web questionnaire the participants were also asked for some background data such as age, gender, workplace, and wound care and skin tear experience. A total of 137 people participated (36 physicians, 93 RNs, and eight other professionals), all of whom had extensive experience of wound care (93.4%). The majority of the participants were women (87.5%), and their mean age was 50 years (SD 11.6). The most frequently selected translation of “skin tear” into Swedish was “hudfliksskada,” with 56.9% (n = 78) of participants selecting it.
2.2. Phase II—Validation of the ISTAP classification system
Health care professionals attending the Wound Care Conference held in the spring of 2017 in Sweden were invited to participate in the validation phase of the study. Those who accepted the invitation received a short educational session (approximately 25 minutes) related to skin tear prediction, prevention, assessment, and management prior to the test. The definition of each skin tear type, as classified by ISTAP, was presented to the participants in a standardised way. A set of 30 photographs of skin tears, derived from ISTAP,9 was thereafter presented to them as a PowerPoint presentation, with all skin tear types in a random order. The participants were directed to classify the skin tear types in a data collection sheet without consulting each other and without referring to the classification document. Participants also included their background data such as age, gender, workplace, and wound care and skin tear experience. All together, 84 people participated in the validation phase.
2.3. Statistical analysis
Descriptive data are presented using frequencies, means, and standard deviations. An inter‐reliability analysis using the Fleiss’ kappa statistical measure was performed to determine consistency between participants. Kappa can take values from 1 to −1. Values between 1 and 0 indicate agreement that is better than chance, a value of 0 indicates a level of agreement that could have been achieved by chance, and values between 0 and −1 indicate levels of agreement that are lower than chance. Landis and Koch propose the following interpretation of Kappa: < 0 “poor,” 0–20 “slight,” 21–40 “fair,” 41–60 “moderate,” 61–80 “substantial,” and 81–100 “almost perfect.”12 The analyses were performed using IBM SPSS statistics 22.0 and SAS/STAT 9.4 software.
2.4. Ethical considerations
In accordance with Swedish legislation concerning the Ethical Review of Research Involving Humans (2003:460), this study needed no further approval. The study was conducted in compliance with the ethical principles derived from the Declaration of Helsinki.13 Completing and submitting the survey (web questionnaire) for phase Ib implied consent, and anonymity was guaranteed. Before the validation study started (phase II), the participants gave their consent by entering the room and choosing to participate in the study. They received verbal information about the study, including the aim and procedures involved, that it was voluntary, and that they could withdraw at any time without explanation. They were also informed that the data would be treated confidentially and that no names or workplaces would be mentioned in the text.
3. RESULTS
In phase II, the Swedish translation of the ISTAP classification system was tested on 84 participants: 59 RNs, 24 non‐RNs, and one with an unknown profession. The mean age of the participants was 51.8 years (SD 11.18, range 23–70 years); 78 were women, and six were men. Respondents’ experience of wound care ranged from reasonable to extensive (Table 1).
Table 1.
Background information about the participants in study phase II (n = 84)
| Question/results | n | % |
|---|---|---|
| Gender | ||
| Women | 78 | 92.9 |
| Men | 6 | 7.1 |
| Were do you work? | ||
| Hospital care | 52 | 61.9 |
| Primary health care | 15 | 17.9 |
| Municipal health care | 5 | 6.0 |
| Other | 11 | 13.2 |
| Missing | 1 | 1.2 |
| What is your professional role? | ||
| Registered nurse | 59 | 71.1 |
| Assistant nurse | 18 | 21.4 |
| Other | 6 | 7.1 |
| Missing | 1 | 1.2 |
| How do you rate your experience of wound care? | ||
| No experience | 1 | 1.2 |
| Little experience | 3 | 3.6 |
| Some experience | 14 | 16.7 |
| Reasonable experience | 31 | 36.9 |
| Extensive experience | 33 | 39.3 |
| Missing | 2 | 2.4 |
| Have you met any patient with this type of wound (skin tear) in the clinic? | ||
| No, never | 2 | 2.4 |
| Yes, but very rarely | 6 | 7.1 |
| Yes, but not often | 20 | 23.8 |
| Yes, quite often | 34 | 40.5 |
| Yes, very often | 21 | 25.0 |
| Missing | 1 | 1.2 |
The overall agreement of the classification system was 68.4%. A moderate level of agreement was demonstrated for the total group (Fleiss’ к 0.500) as well as for the RN group and the non‐RN group (Fleiss’ к = 0.489 and Fleiss’ к = 0.549, respectively). In addition, a moderate level of agreement was also found between health care staff with little experience of wound care and extensive experience of wound care (Fleiss’ к = 0.517 and Fleiss’ к = 0.505, respectively) (Table 2).
Table 2.
The statistical analysis of the level of agreement among participants in study phase II
| Group | Number of participants | Fleiss’ kappa | Strength of agreement |
|---|---|---|---|
| All participants | 84 | 0.500 | Moderate |
| Registered nurses | 59 | 0.489 | Moderate |
| Assistant nurses or others | 24 | 0.549 | Moderate |
| Little experience of wound care | 18 | 0.517 | Moderate |
| Extensive experience of wound care | 64 | 0.505 | Moderate |
| Met patients with skin tears quite rarely | 28 | 0.490 | Moderate |
| Met patients with skin tears quite often | 55 | 0.512 | Moderate |
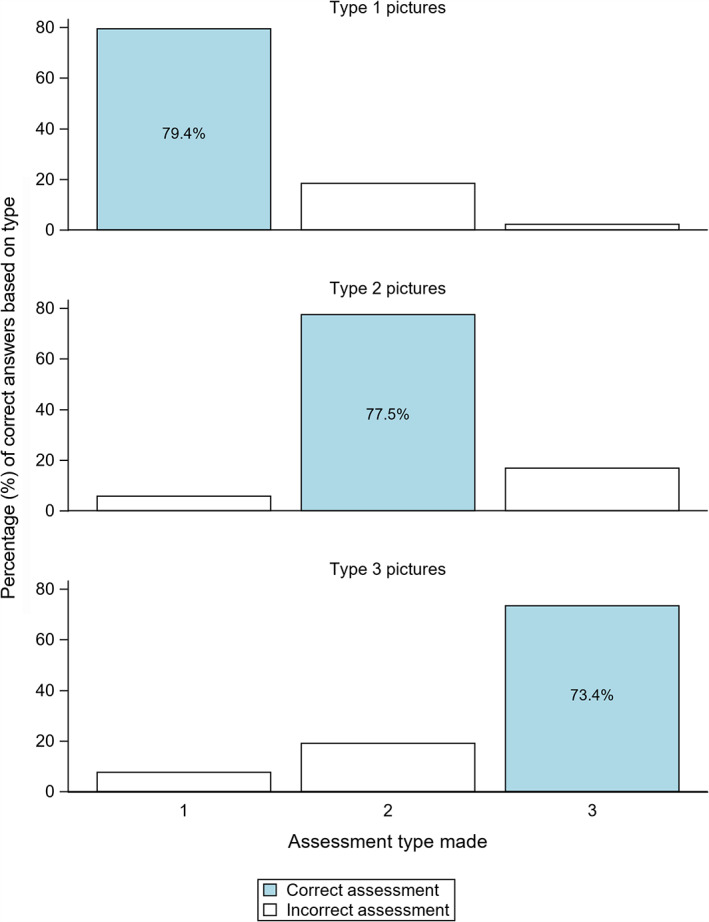
Participants correctly classified skin tear type 1 in 79.4% of the photographs, skin tear type 2 in 77.5% of the photographs, and skin tear type 3 in 73.4% of the photographs (Figure 2).
Figure 2.
Indicates the number (percent) of pictures the participants were able to answer correctly [Colour figure can be viewed at wileyonlinelibrary.com]
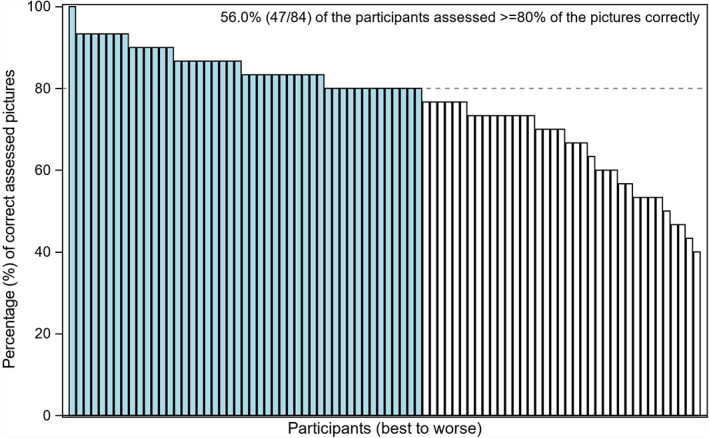
In total, 47 of the 84 participants (56.0%) assessed 80% of the pictures correctly (Figure 3).
Figure 3.
Number (percentage) of correct answers based on type [Colour figure can be viewed at wileyonlinelibrary.com]
4. DISCUSSION
The aims of this study were to culturally adapt the ISTAP skin tear classification system by translating it into Swedish using the forward‐back translation method and then to validate the inter‐reliability of the tool using Fleiss kappa. In the present study, a moderate agreement among RNs and non‐RNs was found. The results of this study support those reported by LeBlanc et al.9 and Skiveren et al.10 LeBlanc et al. reported a substantial level of agreement among the ISTAP panel members in their study, which was attributed to the extensive knowledge that the panel as a collective has on skin tears. Achieving moderate agreement for the ISTAP skin tear tool in this study is an important milestone as it demonstrates the validity of the tool.
It was hypothesised prior to this study that the participants with a higher level of wound care experience would demonstrate a level of agreement similar to the ISTAP panel. The results of this study did not confirm this hypothesis, as shown in Table 2. This suggests that more education is required for all health care staff on the classification of skin tears regardless of experience level of wound care. Skin tear classification is a complex skill that requires training and time to develop.
The participants demonstrated a higher degree of agreement when asked to classify type 1 skin tears than for type 2 and type 3 skin tears. A limitation of this study was that participants were asked to classify skin tears based on photographs, limiting the participants’ ability to complete a thorough wound assessment, which is standard practice in clinical settings. It is hypothesised that a higher level of agreement could have been reached if participants were given the opportunity to examine wounds in real settings. Furthermore, it could have been easier to assess the photos if participants had access to the classification system document as a reference during the validation test, which has been discussed by a previous author.9
This study has contributed by supplying further validity data for the usefulness of the ISTAP classification system of skin tears. Including work performed in previous studies, the classification system has now been validated by 681 health care professionals, the majority of whom are RNs.9, 10 Further validation among physicians and other allied health professionals is required. By validating the skin tear classification system among a wider group of professionals, the awareness of the tool will increase, as will the awareness of skin tears as unique and complex wounds.
The challenge of finding a suitable term to describe skin tears is highlighted in this study. Within English nursing literature, the common term found is “skin tear”; however, this study demonstrates the difficulties encountered when attempting to translate the term into Swedish. Future translation studies are encouraged to conduct a consensus survey to determine the most appropriate means for describing “skin tear” in different languages. In this study, consensus dictated that the best Swedish term for “skin tear” is “hudfliksskada.”
This study has added to the skin tear literature by further validating the ISTAP skin tear classification system and by translating and culturally adapting the tool into Swedish.
ACKNOWLEDGEMENTS
The authors thank the study participants for their contribution during the research project. The authors are also grateful to statistician Mattias Mohlin, from Statistiska Konsultgruppen, Gothenburg, for helping with the statistical analysis and figures. This research project was funded by the Research Council South Älvsborg, Borås, Sweden (VGFOUSA‐674471). The authors state that they have no conflicts of interest to declare.
Källman U, Kimberly LB, Bååth C. Swedish translation and validation of the international skin tear advisory panel skin tear classification system. Int Wound J. 2019;16:13–18. 10.1111/iwj.12975
Funding information Research Council Södra Älvsborg, Borås, Sweden, Grant/Award Number: VGFOUSA‐674471
REFERENCES
- 1. LeBlanc K, Baranoski S, Christensen D, et al. International skin tear advisory panel: a tool kit to aid in the prevention, assessment, and treatment of skin tears using a simplified classification system. Adv Skin Wound Care. 2013;26(10):459‐476. 77–78. [DOI] [PubMed] [Google Scholar]
- 2. LeBlanc K, Baranoski S. Skin tears: state of the science: consensus statements for the prevention, prediction, assessment, and treatment of skin tears. Adv Skin Wound Care. 2011;24:2‐15. [DOI] [PubMed] [Google Scholar]
- 3. LeBlanc K, Baranoski S, Christensen D, et al. The art of dressing selection: a consensus statement on skin tears and best practice. Adv Skin Wound Care. 2016;29(1):32‐46. [DOI] [PubMed] [Google Scholar]
- 4. Strazzieri‐Pulido KC, Peres GR, Campanili TC, de Gouveia Santos VL. Incidence of skin tears and risk factors: a systematic literature review. J Wound Ostomy Continence Nurs. 2017;44(1):29‐33. [DOI] [PubMed] [Google Scholar]
- 5. Leblanc K, Christensen D, Cook J, Culhane B, Gutierrez O. Prevalence of skin tears in a long‐term care facility. J Wound Ostomy Continence Nurs. 2013;40(6):580‐584. [DOI] [PubMed] [Google Scholar]
- 6. Chang YY, Carville K, Tay AC. The prevalence of skin tears in the acute care setting in Singapore. Int Wound J. 2016;13(5):977‐983. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Bermark S, Wahlers B, Gerber AL, Philipsen PA, Skiveren J. Prevalence of skin tears in the extremities in inpatients at a hospital in Denmark. Int Wound J. 2018. April;15(2):212‐217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Carville K, Leslie G, Osseiran‐Moisson R, Newall N, Lewin G. The effectiveness of a twice‐daily skin‐moisturising regimen for reducing the incidence of skin tears. Int Wound J. 2014;11(4):446‐453. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. LeBlanc K, Baranoski S, Holloway S, Langemo D. Validation of a new classification system for skin tears. Adv Skin Wound Care. 2013;26(6):263‐265. [DOI] [PubMed] [Google Scholar]
- 10. Skiveren J, Bermark S, LeBlanc K, Baranoski S. Danish translation and validation of the international skin tear advisory panel skin tear classification system. J Wound Care. 2015;24(8):388‐392. [DOI] [PubMed] [Google Scholar]
- 11. Wild D, Grove A, Martin M, et al. Principles of good practice for the translation and cultural adaptation process for patient‐reported outcomes (PRO) measures: report of the ISPOR task force for translation and cultural adaptation. Value Health. 2005;8(2):94‐104. [DOI] [PubMed] [Google Scholar]
- 12. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33(1):159‐174. [PubMed] [Google Scholar]
- 13. World Medical Association Declaration of Helsinki . Ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191‐2194. [DOI] [PubMed] [Google Scholar]