

Dear Editors,
1.
Historically, in 1973, after Karydakis had operated a Greek army of 1687 soldiers, he defined pilonidal sinus disease (PSD) as having “no raphe, no wound and scar at the depth”.1 Pilonidal sinus disease, today, remains one of the most commonly encountered diseases at the anogenital region, with density of hair, grooming, and hygiene affecting the development of the disease.
There are several treatment modalities, and each of them have their own, unique recurrence rates. Open drainage procedures are rarely used currently. Approaching PSD simply is the best approach for primary disease. In cases of abscess, the infection should be treated, and the definitive operation can be performed after 2 weeks of infection resolution. In the absence of an abscess, simple closure, fibrin glue, and endoscopic management can be successful. However, in recurrent cases, the major goal must be the decreasing of the length of natal sulcus by converting the natal line angle using flap techniques. Various flap techniques can be used. Conserving the vitality of the flap tissues is the major goal. As seen in a 20‐year‐old patient who had recurrent pilonidal disease with multiple sinuses (Figure 1), excision and V‐Y advancement flap were performed (Figures 2, 3, and 4). Below is the algorithm for the management of pilonidal sinus diseases (Figure 5).
Figure 1.

Recurrent pilonidal disease with multiple sinuses
Figure 2.
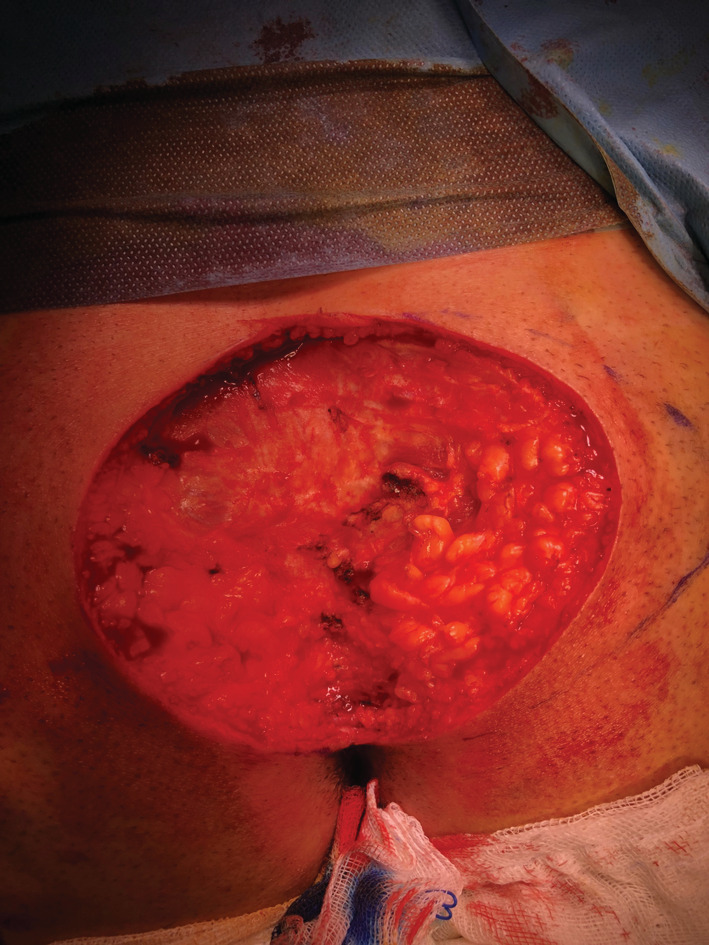
After excision
Figure 3.
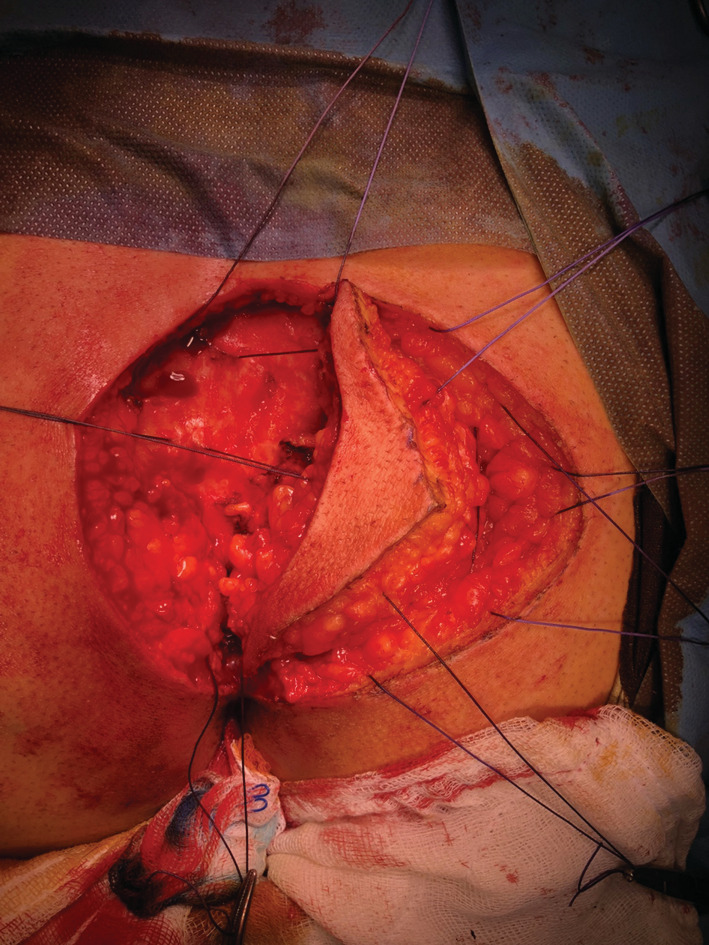
V‐Y advancement flap
Figure 4.

After the operation
Figure 5.
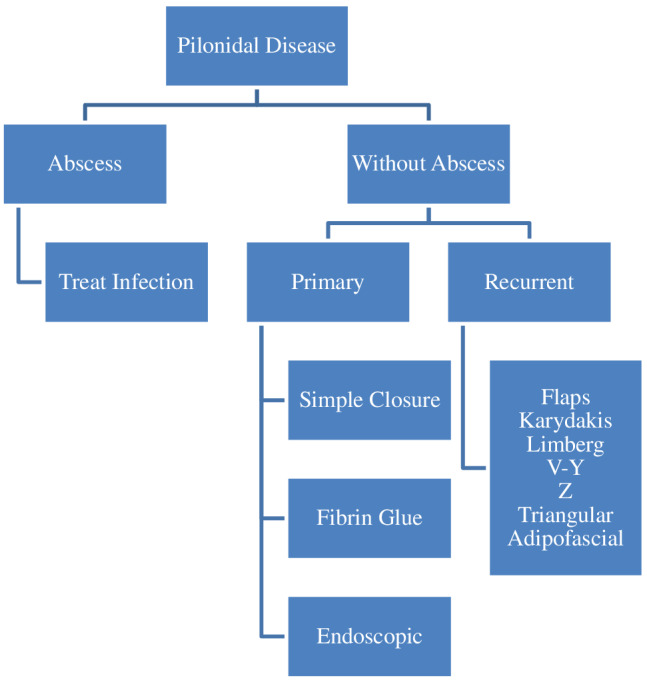
The algorithm for the management of pilonidal sinus diseases
Drain usage is another area of controversy as it can be associated with infections and increased hospital stay. Drains can be safely omitted by encouraging patients to lay supine for the first few postoperative days to diminish seroma occurrence.2, 3
REFERENCES
- 1. Karydakis GE. New approach to the problem of pilonidal sinus. Lancet. 1973;2(7843):1414‐1415. [DOI] [PubMed] [Google Scholar]
- 2. Isik A, Eryılmaz R, Okan I, et al. The use of fibrin glue without surgery in the treatment of pilonidal sinus disease. Int J Clin Exp Med. 2014;7(4):1047‐1051. [PMC free article] [PubMed] [Google Scholar]
- 3. Isik A, Idiz O, Firat D. Novel approaches in pilonidal sinus treatment. Prague Med Rep. 2016;117(4):145‐152. [DOI] [PubMed] [Google Scholar]