

Dear Editors,
Burn injury can be fatal, disfiguring and incapacitating. Therefore, well‐timed and appropriate management could be more than helpful, which primarily consists of debridement cleaning and dressings. These are important aspects of wound care because they can prevent the formation of eschar, which is a moist and protein‐rich avascular substance that encourages microbial growth. Inferentially, debridement cleaning can forbid bacterial growth (infection), as well as promote migration of immune cells and distribution of systemically administered antibiotics.
Irrigation to the burn injury wound can achieve effective debridement cleaning (Figure 1); its ‘micro‐debridement’ effect to shed devitalised tissue can be maximised by tap water with a pressure of about 45 psi, which is superior to antibacterial solutions in removing debris and bacteria 1 .
Figure 1.
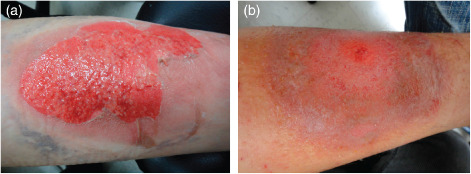
Irrigation scald injury wound on left anterior tibia with tap water. (A) The wound started to be irrigated with warm tap water on fifth day. (B) 5 days after warm tap water irrigation.
Accordingly, we used tap water with temperature lower than individual body temperature to irrigate the wounds twice a day for 5 minutes from the first to the fourth day, followed by warm water, which was 2°C higher than body temperature, until the wounds healed.
Higher irrigation pressure can slough off debris and prevent eschar formation. Cold water irrigation for the first few days prevents the wounds from secondary burn injury, while warm water ameliorates local circulation 2; thus, the overall procedure boosts wound healing and protects the wound from the ongoing inflammatory process. Both cold and warm water work accordingly to accelerate the healing process.
Undeniably, tap water may contain low concentrations of potentially pathological bacteria and varying amounts of small particulate matter. But it has been proven that wounds become infected when they contain more than 105 bacteria per gram of tissue 3. According to the latest updated data from the Taiwan Water Corporation, microbiological cultures of tap water samples in Taichung city are reported to have bacterial counts <1 CFU/ml and the concentration of Escherichia coli is <1 CFU/100 ml. Tap water contains insufficient number of bacteria to cause wound infection and also fits the requirement of the United States Environmental Protection Agency (EPA) for drinking water quality. In conclusion, wound lavage using tap water is an excellent alternative because of its cost‐effectiveness and convenience.
Presuppose that indicated surgical debridement is not delayed (such as for circumferential burn), using alternating cycles of cold and warm tap water irrigation as an adjuvant treatment for burn injury wound has advantages that outweigh its disadvantages and therefore is worth to be promoted.
Kian‐Yong Than, MD1,2,3 & Tzong‐Shiun Li, MD, PhD1,2,3
1Department of Plastic Surgery, China Medical University Beigang Hospital, Taiwan R.O.C.
2Department of Plastic Surgery, China Medical University Hospital, Taiwan R.O.C.
3School of Medicine, China Medical University, Taichung, Taiwan R.O.C.
li.tsa2@msa.hinet.net
Acknowledgements
Both authors do not have any conflict of interest.
References
- 1. Stone S, Carter W. Wound preparation. In: Tintinalli JE, Kelen G, Stapczynski J, editors. Emergency medicine: a comprehensive study guide, 5th edn. New York: McGraw‐Hill, 2000:284–7. [Google Scholar]
- 2. Petrofsky J, Paluso D, Anderson D, Swan K, Yim JE, Murugesan V, Chindam T, Goraksh N, Alshammari F, Lee H, Trivedi M, Hudlikar AN, Katrak V. The contribution of skin blood flow in warming the skin after the application of local heat; the duality of the Pennes heat equation. Med Eng Phys 2011;33:325–9. [DOI] [PubMed] [Google Scholar]
- 3. Riyat MS, Quinton DN. Tap water as a wound cleansing agent in accident and emergency. J Accid Emerg Med 1997;14:165–6. [DOI] [PMC free article] [PubMed] [Google Scholar]