

Dear Editors,
Tattoing has been practiced for centuries in many cultures, and has become increasingly popular in Western countries since the 1970s, with a parallel increase in adverse reactions. It is well established that tattooes may be associated not only with different skin diseases, like transient acute inflammatory reactions at the site of needling, but also with serious medical complications such as allergic contact dermatitis, contact urticaria, photodermatitis and other dermatoses like psoriasis, Systemic Lupus Erythematosus (SLE), sarcoidosis, lichen planus or localisation of skin cancer in the area of the tattoo. The reason for this occurrence has not been fully elucidated, but a locus minoris resistentiae or the isomorphism of Koebner has been hypothesised.
Herein, we describe a case of a 26‐year‐old woman who presented to our clinic for an itchy overgrowing reaction at the tattoo site on the posterior side of her right leg. The tattoo had been placed about 6 months prior to spotting the lesion and contained purple, green and blue‐black pigment. Cutaneous examination showed a verrucous plaque limited to the purple area of the tattoo, where the patient had applied different topical antibiotic and corticosteroid ointments, without any benefit (Figure 1).
Figure 1.

Clinical picture of hyperplastic epidermal reaction localised only to the red pigmented area.
Cultural examinations of the lesion were done to exclude an infective pathogenesis and showed negative results.
A diagnosis of tattoo granuloma was considered and a cutaneous biopsy was performed. Microscopically, it has: hyperkeratosis, parakeratosis and striking pseudoepitheliomatous hyperplasia (PEH) (Figure 2), with marked perivascular and periadnexial mononuclear inflammatory infiltrate in the dermis and superficial epidermis, composed primarily of lymphocytes and histiocytes (Figure 3A–C). Dermal blackish pigment was also noted (Figure 4A, B).
Figure 2.
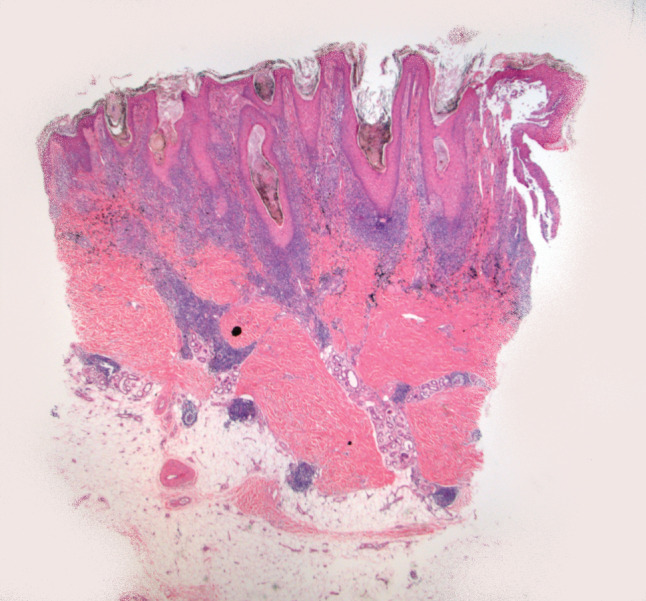
Hematoxylin and eosin, 100× magnification. The figure shows the hyperkeratosis, parakeratosis and pseudoepitheliomatous hyperplasia.
Figure 3.
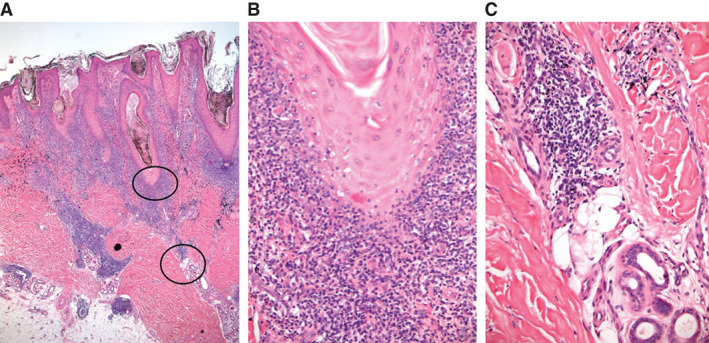
(A) Hematoxylin and eosin, 100× magnification; (B) inflammatory infiltrate at the dermoepidermal junction, 200× magnification and (C) periadnexial inflammatory infiltrate, 200× magnification.
Figure 4.
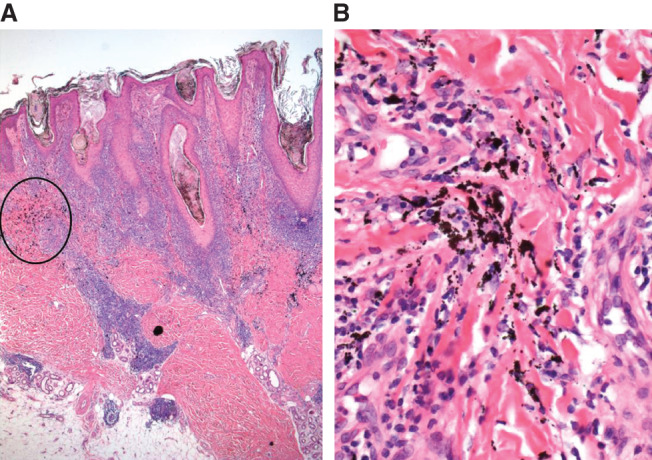
(A) Hematoxylin and eosin, 100× magnification: dermal blackish pigment and (B) dermal blackish pigment at higher magnification 200×.
All these findings were consistent with the diagnosis of PEH at the tattoo site. The patient was treated with monthly intralesional triamcinolone injections and she is currently in follow‐up.
Although inflammatory reactions to tattoos are uncommon, more and more cases are being documented as tattooing becomes increasingly popular in today's society. Different cutaneous delayed reaction patterns have been described, usually secondary to red pigment injection – the most common are allergic and lichenoid reactions, but granulomatous, pseudolymphomatous and morpheiform reactions can also occur 1, 2
The development of cutaneous cancer has been rarely described in the area of a tattoo, but it could be coincidental 3, 4, 5.
PEH is a cutaneous reaction pattern associated with numerous clinical injuries, such as trauma, lymphedema, chronic dermopathies, cutaneous infections and infestations. It can occur also in patients with cutaneous neoplasms, such as melanoma and T‐cell lymphoma 6.
Due to the exuberant epidermal proliferation, PEH may clinically resemble a cutaneous neoplasm (keratoacanthoma, squamous cell carcinoma and basal cell carcinoma); therefore, histologic examination is the main diagnostic tool to prevent misdiagnosis and consequent over‐treatment 2.
PEH is a very rare cutaneous reaction pattern arising at tattoo sites; it was first described in 1967 by Goldstein and since then, very few cases have been reported in literature 7, 8, 9, 10, 11.
Our case underlines the importance of recognising this unusual reaction pattern to tattoo: we therefore suggest that all physicians need to be aware of this entity, in order to easily rule out the possibility of a disguised neoplastic process.
Antonella Tammaro1, Claudia Abruzzese1,
Alessandra Narcisi1, Giorgia Cortesi1, Elena Fontana2,
Severino Persechino1, Roberto Salmaso3 & Mauro Salvatore
Alessandro Alaibac2
1UOC Dermatology, NESMOS Department
University of Rome Sapienza
Rome, Italy
2Department of Medicine
University of Padova
Padova, Italy
3UOC Histopathology
Hospital of Padova
Padova, Italy
tammaroantonella@gmail.com
References
- 1. Jacob CI. Tattoo‐associated dermatoses: a case report and review of the literature. Dermatol Surg 2002;28:962–5. [DOI] [PubMed] [Google Scholar]
- 2. Cui W, McGregor DH, Stark SP, Ulusarac O, Mathur SC. Pseudoepitheliomatous hyperplasia‐an unusual reaction following tatoo: report of a case and review of the literature. Int J Dermatol 2007;46:743–5. [DOI] [PubMed] [Google Scholar]
- 3. Goldenberg G, Patel S, Patel MJ, Williford P, Sangueza O. Eruptive squamous cell carcinomas, keratoacanthoma type, arising in a multicolor tatoo. J Cutan Pathol 2003;35:62–4. [DOI] [PubMed] [Google Scholar]
- 4. Cinotti E, Fausti V, Parodi A, Rongioletti F. Dermatomyofibroma arising in a tattoo. G Ital Dermatol Venereol 2013;148:153–4. [PubMed] [Google Scholar]
- 5. Kluger N, Koljonen V. Tattoos, inks, and cancer. Lancet Oncol 2012;13:e161–8. [DOI] [PubMed] [Google Scholar]
- 6. Weedon D. Tumors of the epidermis. In: Houston MJ, editor. Skin pathology, 2nd edn. London: Churchill Livingstone, 2002:755. [Google Scholar]
- 7. Goldstein N. Mercury‐cadmium sensitivity in tattoos. A photoallergic reaction in red pigment. Ann Intern Med 1967;67:984–9. [DOI] [PubMed] [Google Scholar]
- 8. Breza TS Jr, O'Brien AK, Glavin FL. Pseudoepitheliomatous hyperplasia: an unusual tattoo reaction. JAMA Dermatol 2013;149:630–1. [DOI] [PubMed] [Google Scholar]
- 9. de Roeck A, Joujoux JM, Fournier F, Dandurand M, Meunier L, Stoebner PE. Florid pseudoepitheliomatous hyperplasia related to tattoo: a case report. Int Wound J 2013;10:539–41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Kluger N, Durand L, Minier‐Thoumin C, Plantier F, Cotten H, Berteloot E, Blatière V, Dereure O. Pseudoepitheliomatous epidermal hyperplasia in tattoos: report of three cases. Am J Clin Dermatol 2008;9:337–40. [DOI] [PubMed] [Google Scholar]
- 11. Balfour E, Olhoffer I, Leffell D, Handerson T. Massive pseudoepitheliomatous hyperplasia: an unusual reaction to a tattoo. Am J Dermatopathol 2003 Aug;25:338–40. [DOI] [PubMed] [Google Scholar]