

ABSTRACT
We present the case of a 58‐year‐old man who presented to our wound care centre with a 7 ‐month history of a progressive unilateral leg ulcer. He reported intermittent, heavy bleeding at the ulcer. The duplex sonography showed a bilateral incompetence of the saphenofemoral junctions and the entire course of the great saphenous veins and, surprisingly, also a bilateral reversed arterial‐like pulsating flow in the great and small saphenous veins as well as in the deep veins of the lower extremities. During cardiac examination by auscultation and echocardiography, we detected a previously undescribed severe tricuspid insufficiency with strongly reduced systolic ejection of both the left and the right ventricle and repercussions on the peripheral venous system as a cause for the pulsating veins. This case report highlights that, although infrequent, the presence of pulsating varicose veins points to the presence of cardiac abnormalities, especially severe tricuspid insufficiency, and should direct clinicians to initiate a thorough cardiological examination. Our case highlights that consequent compression therapy can be sufficient for wound healing in such cases and should be initially considered. These patients are at risk of severe bleeding, and therefore, interventions should be carefully planned.
Keywords: Chronic wound, Incompetence of the great saphenous veins, Severe bleeding, Tricuspid insufficiency
Introduction
Chronic venous insufficiency is a common disease and one of the most important reasons for leg ulcers 1. In most cases, the vein varicosis is primary; it is secondary only in 5–20% due to conditions such as deep vein thrombosis, pelvic tumours or arteriovenous fistulas 2. The presence of pulsating varicose veins is an uncommon finding, which is rarely reported in the literature and has been attributed to right heart failure 3, 4.
Case report
We present the case of a 58‐year‐old man who presented to our wound care centre with a 7 ‐month history of a progressive unilateral leg ulcer. He reported intermittent, heavy bleeding at the ulcer. He was otherwise well, but a dilated cardiomyopathy with severe heart failure following prolonged infection had been diagnosed years ago, and a secondary mitral regurgitation had been treated with the percutaneous MitraClip device. The physical examination revealed a superficial leg ulcer about 4 cm in diameter at the right medial calf and minor lower leg oedema (Figure 1A). The duplex sonography showed a bilateral incompetence of the saphenofemoral junctions and the entire course of the great saphenous veins and, surprisingly, also a bilateral reversed arterial‐like pulsating flow in the great and small saphenous veins, as well as in the deep veins of the lower extremities (Figure 1B).
Figure 1.
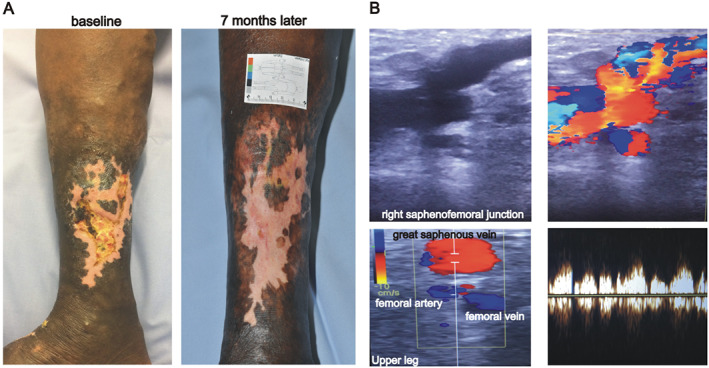
A leg ulcer with pulsating varicose veins. (A) The patient has a lower leg ulcer of about 4 cm in diameter at the right medial calf. Please note the varicose veins above the ulcer. Healing of the wound was achieved within 7 months after presentation of the patient. (B) Duplex sonography reveals incontinence of the saphenofemoral junction with reversed arterial‐like pulsating flow during the whole course of the great saphenous vein. At the upper leg, both the femoral vein and great saphenous veins show reversed arterial‐like pulsating flow. The Duplex image displays phasic wave forms in the great saphenous vein of the upper leg.
During cardiac examination by auscultation and echocardiography, we detected a previously undescribed severe tricuspid insufficiency with strongly reduced systolic ejection of both the left and the right ventricle and repercussions on the peripheral venous system as a cause for the pulsating veins. In the phlebodynamometric examination, arterial‐like pulsations even at the distal veins of the back of the feet were found. We detected a pressure reduction during deactivation of the great saphenous vein; thus, a surgical intervention to reduce venous hypertension in the superficial peripheral veins appears to be a therapeutic option. However, because of the high pressure in the deep veins, a relapse of the great saphenous vein by stripping or, preferably, endovenous laser or radiofrequency treatment soon after surgical treatment is highly likely. Therefore, because of the significant cardiac risk factors in our patient, in agreement with the cardiologists, we initially decided on a conservative treatment by optimising the heart failure therapeutic regime, prescribing compression therapy with class 3 graduated elastic stockings and improvement of wound dressings. The implantation of a CardioMEM‐Sensor for continuous monitoring of the pulmonary artery pressure and fine tuning of the diuretics was also recommended. With these adjustments, reduction of the ulcer size was achieved rapidly.
Discussion
Pulsating varicose veins have been rarely reported in the literature 3, 4. The most common misdiagnosis of arteriovenous malformation can lead to unnecessary surgical exploration without considering the diagnosis of severe heart failure. Severe right heart failure is associated with increased systemic venous pressure, which might be reflected by distension of the jugular veins or an enlarged and pulsatile liver, which is caused by reversed blood flow during systole. In rare cases, right heart failure is also causal for back pressure in the deep veins of the lower limbs, which secondarily also affects the superficial veins of the legs. The heightened pressure within the veins results in their dilatation and valve insufficiency. Thus, right heart failure should be considered an aetiological factor for chronic venous insufficiency and leg ulcers 5.
This case report highlights that, although infrequent, the presence of pulsating varicose veins points to the presence of cardiac abnormalities, especially severe tricuspid insufficiency, and should direct clinicians to initiate a thorough cardiological examination. Our case highlights that consequent compression therapy can be sufficient for wound healing in such cases and should be initially considered. These patients are at risk of severe bleeding, and therefore, interventions should be carefully planned.
Acknowledgements
We thank the patient for providing permission to share his information. We thank Dr. Tsakiris Leonidas for valuable advice regarding the cardiological condition of the patient.
The authors have no conflicts of interest to disclose.
References
- 1. Pannier‐Fischer F, Rabe E. Epidemiology of chronic venous diseases. Hautarzt 2003;54(11):1037–44. [DOI] [PubMed] [Google Scholar]
- 2. Comerota A, Lurie F. Pathogenesis of venous ulcer. Semin Vasc Surg März 2015;28(1):6–14. [DOI] [PubMed] [Google Scholar]
- 3. Dalla Vestra M, Grolla E, Bonanni L, Dorrucci V, Presotto F, Rigo F. From the veins to the heart: a rare cause of varicose veins. Case Rep Vasc Med 2015;2015:849408. 10.1155/2015/849408 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Rispoli P, Varetto G, Santovito D, Castagno C, Tallia C. A severe cause of pulsating varicose veins. Lancet Lond Engl 2011;378(9809):2138. [DOI] [PubMed] [Google Scholar]
- 5. Augey F, Pinet A, Renaudier P. Heart failure and stasis ulcer: a significant association (prospective study of 100 cases). Ann Dermatol Venereol Mai 2010;137(5):353–8. [DOI] [PubMed] [Google Scholar]