

Abstract
Radiotherapy produces both acute and delayed effects on mucosal tissues, disturbing their healing. This report shows a successful treatment with laser phototherapy (LPT) on a delayed wound healing in oral mucosa previously submitted to radiotherapy with a follow up of 3 years. A 47‐year‐old patient treated 6 months earlier for tongue squamous cell carcinoma by surgery and radiotherapy presented with a mass in the operated area. Biopsy showed chronic inflammatory infiltrate around a residual polyglactin suture. After 2 months there was a painful mucosal dehiscence on the biopsy site. LPT was performed using a semiconductor laser with 660‐nm wavelength (InGaAlP) and spot size of 0·04 cm2. The parameters applied were 40 mW, 4 Jcm2/point, 0·16 J/point, 2·4 J/session. The irradiation was performed punctually, through contact mode in 15 points (4 seconds/point), on top of and around the lesion, during ten sessions. The wound healed completely after ten sessions. This treatment proved to be conservative and effective, inducing healing of a chronic wound in a tissue previously submitted to radiotherapy.
Keywords: Healing, Laser, Squamous cell carcinoma
INTRODUCTION
Head and neck cancers have mainly two ways of treatment: radiotherapy and surgery. External radiotherapy is an established cancer treatment that uses doses of high‐energy X‐rays to destroy neoplastic cells. The main problem in this area is the induced side effects, either during or after irradiation. The side effects and potential complications of this type of treatment include dry mouth, sore throat, difficulty swallowing, tissue fibrosis and changes in small blood vessels 1, 2. Its effect on microcirculation causes a severe harm to tissue, especially in the healing process. At the cellular level, the literature reports a decrease in fibroblasts proliferation, as well as deficiency in its attachment (2). In addition, oral mucositis is a dose‐limiting and painful side effect of radiation and/or chemotherapy cancer patients. It occurs in almost all patients undergoing radiotherapy for treatment of head and neck cancers and represents the major limitation to continuous, uninterrupted radiotherapy and concurrent chemotherapy in the management of head and neck cancer (3). Strategies for reducing oral mucositis include laser phototherapy (LPT) with great results on wound healing and pain relief (4).
After 1971, when Mester (5) first reported the use of LPT in improving wound healing, it was established as an alternative, non invasive method to enhance healing of chronic wounds, modulate the inflammatory process and promote pain relief 6, 7, 8, 9, 10. At the cellular level the absorption of light by specific chromophore photoreceptors occurs, and once absorbed, the light can modulate cell biochemical reactions and stimulate mitochondrial respiration (11) that will result in secondary reactions such as increase in ATP synthesis, collagen production, increase in cell proliferation and migration 12, 13, 14.
The application of LPT using a He–Ne laser (λ = 632·8 nm) in the treatment of recalcitrant radiation ulcers in skin has been described in literature by a few authors 15, 16, 17, as well as the use of LPT in the prevention and treatment of mucositis is well established by several publications 4, 18, 19.
This case reports the use of LPT in the treatment of a deficient wound in the tongue of a patient previously submitted to head and neck radiotherapy.
CASE REPORT
A 47‐year‐old male, who had never smoked, presented to a Head and Neck surgeon in October 2006, with an asymptomatic ulcerated lesion with elevated, indurate margins and fixed to the underlying tissues on the right lateral border of the tongue, measuring 1·2 × 1·52 cm (Figure 1A). The incisional biopsy showed squamous cell carcinoma. The oncologic treatment included surgical removal (Figure 1B), neck dissection and radiotherapy (70 Gy in 30 fractions). Six months later the patient returned to the office, showing a hard submucosal mass in the region of the operated area. Incisional biopsy was performed and showed a chronic inflammatory infiltrate around a residual polyglactin (Vicryl®, Johnson & Johnson, São Paulo, Brazil) suture. Two months later, a painful mucosal dehiscence could be observed and the chosen treatment was LPT in the dehiscence area (Figure 1C). Laser therapy was performed using a semiconductor laser (MMOPTICS®) with 660‐nm wavelength (InGaAlP) and spot size of 0·04 cm2. The power and fluence used was 40 mW and 4 Jcm2/point, respectively. Energy applied was 0·16 J/point and 2·4 J per session. Before and after each LPT session, the power output of the equipment was measured by a power meter (PM 600, Molectron, Portland, OR).
Figure 1.
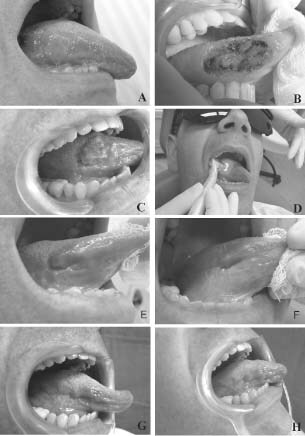
(A) Squamous cell carcinoma on right lateral border of tongue (October 2006). (B) Immediately after the surgical removal of the squamous cell carcinoma (December 2006). (C) Painful mucosal dehiscence (14 November 2007). (D) First session of ten of laser phototherapy (LPT) (27 November 2007). (E) Aspect of wound healing after seven sessions of LPT (4 December 2007). (F) Final aspect of the wound after ten sessions of LPT. The wound healed completely (7 December 2007). (G) Follow up of 4 months after the end of LPT treatment (April 2008). (H) Follow up of 3 years after the end of LPT treatment (November 2010).
The saliva present on the tongue was always dried with gauze pads before irradiation. The irradiation was performed punctually, through contact mode in 15 points (4 seconds/point) on top of and around the lesion, during ten sessions (Figure 1D). The laser therapy was applied daily, exception of Sunday, reaching 10 days. No concomitant topical or systemic medication was used by the patient during the treatment.
The patient was asked to number the pain score from 0 to 10. Before the beginning of LPT, the patient reported score 8, after the first session of LPT, the pain was completely reverted and after ten sessions, the wound healed completely (Figure 1F). The wound healing was analysed clinically and through the photographs taken. No side effects of LPT were detected or related to the patient, such as erythema, oedema or blooding. In addition, any symptoms as fever, itch, pain, burning and paresthesia were observed. The follow up of 4 months and 3 years after the end of LPT showed neither signs nor symptoms in the previous dehiscence area (Figure 1G and H, respectively).
DISCUSSION
This case report showed an LPT successful treatment inducing closure of a chronic wound in the tongue previously submitted to head and neck radiotherapy. Although we supposed that some surgical approach would be necessary to complete the closure of the wound, the treatment was started with LPT to relieve the patient's pain. After the first session of LPT, the pain was completely controlled and the ulcer healing exhibited extraordinary improvement. The improvement of the wound healing and pain control by LPT is reported by several studies in the literature through modulation of inflammation 6, 8, 9, 10, fibroblast proliferation (20), keratinocyte migration and proliferation 21, 22, increased microcirculation (23), growth factor release (24) and collagen synthesis 14, 20. The application of LPT (HeNe 632 nm) in the treatment of recalcitrant radiation ulcers in skin has been described in literature by a few authors 15, 16, 17, as well as using 780‐nm diode laser (23). Schindl et al. (16), in a brief communication, published a case report of a 64‐year‐old woman with a painful chronic ulcerous lesion on the left sole. Fifty years earlier the patient had received five sessions of X‐ray therapy on treat three plantar with unreported dose. The author used a He–Ne laser, 632·8 nm, with 5 mm spot size diameter and fluence of 31·5 J/cm2. The beam was diverged by the instrument's scanner to cover the upper edge of the ulcer (total area of 20 mm2) and irradiation was applied twice a week. After the fourth session, the patient reported marked pain relief. During the next sessions, granulation and subsequent epithelisation of the wound were noted. After 20 sessions, the ulcer had healed completely. Despite the difference of parameters used as higher fluence (16), the pattern of results were similar to the present case report, with firstly pain relief and wound completely healed after some sessions. Schindl et al. (15) also showed a beneficial effect on impaired wound healing in three patients with chronic radiation ulcers in skin. The author used higher fluence (30 J/cm2) in comparison with this study with a He–Ne laser. Shaffer et al. (23) applied LPT in patients suffering from painful mastitis after breast ionising radiation and in patients with radiogenic ulcers (780 nm, 5 J/cm2, 5× week during 5 weeks), and through magnetic resonance imaging it was verified that all patients showed complete clinical remission. All the studies in the literature using LPT in the treatment of side effect of radiotherapy in skin and mucosa show beneficial results 15, 16, 17, 23, 25. To the best of our knowledge, no case reported that LPT applied in recalcitrant ulcers in oral mucosa has been described so far.
The interaction of laser light with living tissues may lead to different results depending upon several factors, such as wavelength, dose, power and physiologic status of the cell at the irradiation time (26). The red wavelength was chosen in this case because of its superficial absorption (26) promoting epithelial‐cell proliferation. One of the factors that lead to the success of the treatment was probably associated with the schedule of the irradiations adopted. Several studies in the literature show that a single LPT irradiation is not as effective as successive ones 27, 28. Transitory effects in cells resulted by LPT were also shown in the literature, suggesting that the number of sessions is important to maintain laser effect on cells (29). The fluence is also of importance. The use of high doses of energy has been considered a potential inhibitor of cellular proliferation within a narrow band of energy and density (26). According to the literature, tissues and cells that present a reduced physiological state respond better to LPT in comparison to healthy ones 20, 26, 30, 31. In the case described here, the patient received head and neck ionising radiation which produces both acute and delayed effects on mucosal tissues, disturbing their healing (32). Radiotherapy induces acute degenerative changes in basement membranes and increases vascular permeability. Changes in vasculature may include decreased number of capillary vessels, stasis and occlusion, oedema of vascular walls, thrombosis and reduction of neovascularisation, contributing to healing deficiency (33). Fibroblasts may also be permanently altered by radiation, resulting in alterations of collagen synthesis that can lead to atrophy, contraction and fibrosis of the tissue (34). In this context, radiation therapy for cancer may interrupt the normal wound healing mechanisms, increasing the likelihood of postoperative wound infection, which increases the risk of wound dehiscence and subsequent failure (33). In thepresent case, we observed that the combination of the parameters and number of LPT irradiations adopted was effective in promoting the wound healing.
The effect of laser therapy on the stimulation of cell lines of tumour cells remains a controversial topic. The LPT effect on tumour cell proliferation has been shown to be inhibitory, proliferative, as well as neutral, depending on cell type, wavelength, dosage and schedule of irradiation 34, 35, 36, 37, 38, 39, 40. In the present case, a previous biopsy confirmed the absence of malignant cells. The patient can therefore be considered norm reactive, with no more malignant cells, which allows the safe use of LPT in the treatment of the wound. Although LPT under certain conditions appears to be able to stimulate malignant cells, this has so far only been documented in vitro. In the in vivo situation, the presence of the immune system changes the conditions and the laser stimulation of the immune response may be higher than the stimulation of the tumour cells. This was documented already in 1965 by McGuff et al. (41), where different types of tumours were implanted into the oral pouches of hamsters and irradiated by varying doses of ruby and helium‐neon lasers. Matching, Kitsmaniuk et al. (25), used Helium–Neon and Cooper vapour laser for prevention and treatment of postoperative and irradiation complications in 195 patients with locally advanced head and neck carcinoma and found that LPT of skin fields improved skin tolerance to the neutron beam. The study did not show any tumour growth stimulation by the laser irradiation in terms of recurrence and metastasis development.
It was concluded that LPT offers a promising conservative therapy for the treatment of postoperative and irradiation‐related dehiscence. A follow up of at least 1 year was recommended, not just because of the side effect of radiotherapy but also because of the potential recurrence of the oral squamous cell carcinoma. Figure 1G shows the clinical aspect after 4 months of laser therapy, as well as Figure 1H shows the aspect after 3 years, when complete healing of the wound and acceptable scar remodelling could be observed. This case report confirmed that LPT could be an effective, economic and non invasive treatment for dehiscence tissue resulted from radiotherapy, with the advantages of safety and tolerability.
REFERENCES
- 1. Rudolph R, Arganese T, Woodward M. The ultrastructure and etiology of chronic radiotherapy damage in human skin. Ann Plast Surg 1982;9:282–92. [DOI] [PubMed] [Google Scholar]
- 2. Rudolph R, Vande Berg J, Schneider JA, Fisher JC, Poolman WL. Slowed growth of cultured fibroblasts from human radiation wounds. Plast Reconstr Surg 1988;82:669–77. [DOI] [PubMed] [Google Scholar]
- 3. Russo G, Haddad R, Posner M, Machtay M. Radiation treatment breaks and ulcerative mucositis in head and neck cancer. Oncologist 2008;13:886–98. [DOI] [PubMed] [Google Scholar]
- 4. Simoes A, Eduardo FP, Luiz AC, Campos L, Sa PH, Cristofaro M, Marques MM, Eduardo CP. Laser phototherapy as topical prophylaxis against head and neck cancer radiotherapy‐induced oral mucositis: comparison between low and high/low power lasers. Lasers Surg Med 2009;41: 264–70. [DOI] [PubMed] [Google Scholar]
- 5. Mester E, Spiry T, Szende B, Tota JG. Effect of laser rays on wound healing. Am J Surg 1971;122:532–5. [DOI] [PubMed] [Google Scholar]
- 6. Wedlock P, Shephard RA, Little C, McBurney F. Analgesic effects of cranial laser treatment in two rat nociception models. Physiol Behav 1996;59:445–8. [DOI] [PubMed] [Google Scholar]
- 7. Moore P, Ridgway TD, Higbee RG, Howard EW, Lucroy MD. Effect of wavelength on low‐intensity laser irradiation‐stimulated cell proliferation in vitro. Lasers Surg Med 2005;36:8–12. [DOI] [PubMed] [Google Scholar]
- 8. Shimizu N, Yamaguchi M, Goseki T, Shibata Y, Takiguchi H, Iwasawa T, Abiko Y. Inhibition of prostaglandin E2 and interleukin 1‐beta production by low‐power laser irradiation in stretched human periodontal ligament cells. J Dent Res 1995;74:1382–8. [DOI] [PubMed] [Google Scholar]
- 9. Sakurai Y, Yamaguchi M, Abiko Y. Inhibitory effect of low‐level laser irradiation on LPS‐stimulated prostaglandin E2 production and cyclooxygenase‐2 in human gingival fibroblasts. Eur J Oral Sci 2000;108:29–34. [DOI] [PubMed] [Google Scholar]
- 10. Tam G. Low power laser therapy and analgesic action. J Clin Laser Med Surg 1999;17:29–33. [DOI] [PubMed] [Google Scholar]
- 11. Karu T. Primary and secondary mechanisms of action of visible to near‐IR radiation on cells. J Photochem Photobiol B 1999;49:1–17. [DOI] [PubMed] [Google Scholar]
- 12. Abergel RP, Lyons RF, Castel JC, Dwyer RM, Uitto J. Biostimulation of wound healing by lasers: experimental approaches in animal models and in fibroblast cultures. J Dermatol Surg Oncol 1987;13:127–33. [DOI] [PubMed] [Google Scholar]
- 13. Conlan MJ, Rapley JW, Cobb CM. Biostimulation of wound healing by low‐energy laser irradiation. A review. J Clin Periodontol 1996;23:492–6. [DOI] [PubMed] [Google Scholar]
- 14. de Araujo CE, Ribeiro MS, Favaro R, Zezell DM, Zorn TM. Ultrastructural and autoradiographical analysis show a faster skin repair in He‐Ne laser‐treated wounds. J Photochem Photobiol B 2007;86:87–96. [DOI] [PubMed] [Google Scholar]
- 15. Schindl A, Schindl M, Pernerstorfer‐Schon H, Mossbacher U, Schindl L. Low intensity laser irradiation in the treatment of recalcitrant radiation ulcers in patients with breast cancer–long‐term results of 3 cases. Photodermatol Photoimmunol Photomed 2000;16:34–7. [DOI] [PubMed] [Google Scholar]
- 16. Schindl A, Schindl M, Schindl L. Successful treatment of a persistent radiation ulcer by low power laser therapy. J Am Acad Dermatol 1997;37:646–8 [DOI] [PubMed] [Google Scholar]
- 17. Schindl M, Kerschan K, Schindl A, Schon H, Heinzl H, Schindl L. Induction of complete wound healing in recalcitrant ulcers by low‐intensity laser irradiation depends on ulcer cause and size. Photodermatol Photoimmunol Photomed 1999;15:18–21. [DOI] [PubMed] [Google Scholar]
- 18. Eduardo FP, Bezinelli L, Luiz AC, Correa L, Vogel C, Eduardo CP. Severity of oral mucositis in patients undergoing hematopoietic cell transplantation and an oral laser phototherapy protocol: a survey of 30 patients. Photomed Laser Surg 2009;27:137–44. [DOI] [PubMed] [Google Scholar]
- 19. Schubert MM, Eduardo FP, Guthrie KA, Franquin JC, Bensadoun RJ, Migliorati CA, Lloid CM, Eduardo CP, Walter NF, Marques MM, Hamdi M. A phase III randomized double‐blind placebo‐controlled clinical trial to determine the efficacy of low level laser therapy for the prevention of oral mucositis in patients undergoing hematopoietic cell transplantation. Support Care Cancer 2007;15:1145–54. [DOI] [PubMed] [Google Scholar]
- 20. Pereira AN, Eduardo Cde P, Matson E, Marques MM. Effect of low‐power laser irradiation on cell growth and procollagen synthesis of cultured fibroblasts. Lasers Surg Med 2002;31:263–7. [DOI] [PubMed] [Google Scholar]
- 21. Haas AF, Isseroff RR, Wheeland RG, Rood PA, Graves PJ. Low‐energy helium‐neon laser irradiation increases the motility of cultured human keratinocytes. J Invest Dermatol 1990;94:822–6. [DOI] [PubMed] [Google Scholar]
- 22. Webb C, Dyson M, Lewis WH. Stimulatory effect of 660 nm low level laser energy on hypertrophic scar‐derived fibroblasts: possible mechanisms for increase in cell counts. Lasers Surg Med 1998;22:294–301. [DOI] [PubMed] [Google Scholar]
- 23. Schaffer M, Bonel H, Sroka R, Schaffer PM, Busch M, Sittek H, Reiser M, Duhmke E. Magnetic resonance imaging (MRI) controlled outcome of side effects caused by ionizing radiation, treated with 780 nm‐diode laser – preliminary results. J Photochem Photobiol B 2000;59:1–8. [DOI] [PubMed] [Google Scholar]
- 24. Yu W, Naim JO, Lanzafame RJ. The effect of laser irradiation on the release of bFGF from 3T3 fibroblasts. Photochem Photobiol 1994;59:167–70. [DOI] [PubMed] [Google Scholar]
- 25. Kitsmaniuk ZD, Demochko VB, Popovich VI. [The use of low‐energy lasers for preventing and treating postoperative and radiation‐induced complications in patients with head and neck tumors]. Vopr Onkol 1992;38:980–6. [PubMed] [Google Scholar]
- 26. Karu T. Photobiology of low‐power laser effects. Health Phys 1989;56:691–704. [DOI] [PubMed] [Google Scholar]
- 27. Kreisler M, Christoffers AB, Willershausen B, d’Hoedt B. Effect of low‐level GaAlAs laser irradiation on the proliferation rate of human periodontal ligament fibroblasts: an in vitro study. J Clin Periodontol 2003;30:353–8. [DOI] [PubMed] [Google Scholar]
- 28. Kubasova T, Kovacs L, Somosy Z, Unk P, Kokai A. Biological effect of He‐Ne laser: investigations on functional and micromorphological alterations of cell membranes, in vitro. Lasers Surg Med 1984;4:381–8. [DOI] [PubMed] [Google Scholar]
- 29. Gavish L, Asher Y, Becker Y, Kleinman Y. Low level laser irradiation stimulates mitochondrial membrane potential and disperses subnuclear promyelocytic leukemia protein. Lasers Surg Med 2004;35:369–76. [DOI] [PubMed] [Google Scholar]
- 30. Eduardo FP, Mehnert DU, Monezi TA, Zezell DM, Schubert MM, Eduardo CP, Marques MM. Cultured epithelial cells response to phototherapy with low intensity laser. Lasers Surg Med 2007; 39:365–72. [DOI] [PubMed] [Google Scholar]
- 31. Tuner J, Hode L. It's all in the parameters: a critical analysis of some well‐known negative studies on low‐level laser therapy. J Clin Laser Med Surg 1998;16:245–8. [PubMed] [Google Scholar]
- 32. Bernstein EF, Sullivan FJ, Mitchell JB, Salomon GD, Glatstein E. Biology of chronic radiation effect on tissues and wound healing. Clin Plast Surg 1993;20:435–53. [PubMed] [Google Scholar]
- 33. Tibbs MK. Wound healing following radiation therapy: a review. Radiother Oncol 1997;42:99–106. [DOI] [PubMed] [Google Scholar]
- 34. Drake DB, Oishi SN. Wound healing considerations in chemotherapy and radiation therapy. Clin Plast Surg 1995;22:31–7. [PubMed] [Google Scholar]
- 35. Schaffer M, Sroka R, Fuchs C, Schrader‐Reichardt U, Schaffer PM, Busch M, Duhmke E. Biomodulative effects induced by 805 nm laser light irradiation of normal and tumor cells. J Photochem Photobiol B 1997;40:253–7. [DOI] [PubMed] [Google Scholar]
- 36. Sroka R, Schaffer M, Fuchs C, Pongratz T, Schrader‐Reichard U, Busch M, Schaffer PM, Duhmke E, Baumgartner R. Effects on the mitosis of normal and tumor cells induced by light treatment of different wavelengths. Lasers Surg Med 1999;25:263–71. [DOI] [PubMed] [Google Scholar]
- 37. Coombe AR, Ho CT, Darendeliler MA, Hunter N, Philips JR, Chapple CC, Yum LW. The effects of low level laser irradiation on osteoblastic cells. Clin Orthod Res 2001;4:3–14. [DOI] [PubMed] [Google Scholar]
- 38. Kreisler M, Christoffers AB, Willershausen B., d’Hoedt B. Low‐level 809 nm GaAlAs laser irradiation increases the proliferation rate of human laryngeal carcinoma cells in vitro. Lasers Med Sci 2003;18:100–3. [DOI] [PubMed] [Google Scholar]
- 39. Pinheiro AL, Carneiro NS, Vieira AL, Brugnera A Jr, Zanin FA, Barros RA, Silva PS. Effects of low‐level laser therapy on malignant cells: in vitro study. J Clin Laser Med Surg 2002;20:23–6. [DOI] [PubMed] [Google Scholar]
- 40. Ocaña‐Quero JM, Gomez‐Villamandos R, Moreno‐Millán M, Santisteban‐Valenzuela JM. Effect of Helium‐Neon (HeNe) laser irradiation on dog neoplasm cells in culture. Lasers Med Sci 1998;13:143–7. [DOI] [PubMed] [Google Scholar]
- 41. McGuff PE, Deterling RA Jr, Gottlieb LS. Tumoricidal effect of laser energy on experimental and human malignant tumors. N Engl J Med 1965;273:490–2. [DOI] [PubMed] [Google Scholar]