

Abstract
Study design: A retrospective hospital-based study.
Objective: To describe the epidemiological profile of traumatic spinal cord injury (TSCI) in Guangdong Province.
Setting: Two hospitals within Guangdong Province, China.
Methods: Medical records of patients diagnosed with TSCI admitted to Foshan Hospital of Traditional Chinese Medicine and Zhujiang Hospital of South Medical University from 1 January 2011 to 31 December 2015 were retrospectively reviewed. Epidemiological characteristics, such as age, sex, occupation, etiology, neurological level of injury, American Spinal Injury Association Impairment Scale at admission, death and cause of death during the acute hospitalization and concomitant injuries.
Results: During the study period, 482 cases were identified. Male-to-female ratio was 3.4:1, with a mean age of 41.5 ± 12.6 years old. The leading cause was falls (49.3%), followed by motor vehicle collisions (MVCs) (34.8%). The most common injury site was the cervical spinal cord, especially C4–C6, accounting for 39.8%.
Conclusion: The number of TSCI patients in Guangdong Province is large and is exhibiting a rising trend. The leading causes were falls and MVCs. The low-falls (height < 1 m) group has expanded over this period. With China entering an ageing society, more appropriate preventative measures should be implemented for fall-related injuries among the elderly.
Keywords: Traumatic spinal cord injury, Epidemiology, Prevention
Introduction
Traumatic spinal cord injury is considered to be the second cause after traumatic brain injury in terms of morbidity and disability.1 This type of injury is a catastrophic event which is associated with devastating physical, psychological and economic consequences. Even though the research is progressing, there is still no breakthrough for treatment as of yet; therefore, primary prevention is the best strategy. Gaining insight into the demographic characteristics of this injury is essential to help direct safety precautions and health care planning.2
The estimated amount of TSCI can vary drastically depending on each country, it ranges from 3.6 per million in Canada to 195.4 per million in Ireland.3–6 This is associated with the different levels of economic development of each country and time period. A review of global epidemiological studies from the years spanning from 1990 to 2009 demonstrated that the incidence rates of TSCI in developed countries dropped from 52.2 to 13.1 per million people. In the meantime, among developing countries, the incidence rates ranged from 12.7 to 29.7 per million people.7 In China, Li and Ning reported a recent annual incidence rate of 23.7 per million population in Tianjin and 60.6 per million in Beijing.8,9
Guangdong Province is located in the south of China. It is one of China’s economic powerhouses and the most populous province in China. To our knowledge, there have been few hospital-based studies focused on epidemiological features of TSCI in Guangdong Province.10 This study presents epidemiologic data on SCI patients who were treated at two institutions in Guangdong Province from 1 January 2011 to 31 December 2015.
Patients and methods
Medical records during 2011–2015 in Foshan Hospital of Traditional Chinese Medicine and Zhujiang Hospital of South Medical University were retrospectively reviewed, using the International Classification of Disease Version 10(ICD-10) and diagnostic code of TSCI. The data that was extracted for this study included age, sex, occupation, etiology, level of injury, severity of injury, American Spinal Injury Association (ASIA) Impairment Scale (AIS), death and cause of death during the acute hospitalization and concomitant injuries. The inclusion criteria for the study were spinal cord injuries or cauda equina injuries, caused by trauma that originally occurred in Guangdong, and patients who were admitted to Foshan Hospital of Traditional Chinese Medicine and Zhujiang Hospital of South Medical University at the time of trauma. Exclusion criteria were intervertebral disc disease, vertebral fractures in the absence of TSCI, and fatally injured people who were never hospitalized. Medical records with uncertain diagnoses and incomplete medical records were also excluded.
In this study, the patients were divided into six age groups with 15 year intervals: 0–15, 16–30, 31–45, 46–60, 61–75, and ≥76 years old. Cause of injury were categorized as motor vehicle collisions (MVCs), low falls (height < 1 m), high falls (height ≥ 1 m), being struck by an object, sports and other. According to the anatomical identity of the level of the lesion, the spinal cord is classified as having cervical, thoracic, lumbar, and sacral segments injuries. Occupations included peasants, laborers, drivers, civil servants, students and others. These verity of the injury was evaluated by American Spinal Injury Association (ASIA) Impairment Scale in line with the 2011 revision of the International Standards for Neurological Classification of Spinal Cord Injury, and the severity of injury was also classified as complete or incomplete tetraplegia and complete or incomplete paraplegia according to the AIS scale.11 The data was collected in a Microsoft Excel spreadsheet and statistical analysis was analyzed by using SPSS 12.0 (SPSS Inc., Chicago, IL, USA).
Results
From 1 January 2011 to 31 December 2015, 533 TSCI cases were identified and 51 were excluded from the study (intervertebral disc disease 11; spinal column fracture without SCI 22; incomplete medical records or uncertain diagnosis 18). Finally, the medical records of 482 TSCI patients were collected. As shown in Fig. 1, the number of TSCI admissions increased over the 5 years of study (2011: 79, 2012: 84, 2013: 98, 2014: 103, 2015: 118). Although the total number of ward beds in the hospitals research remained unchanged over this period, the frequency of TSCI admissions increased steadily, with a growth rate of 10.6% on average. Guangdong’s population growth rate was 0.77% during the corresponding period.
Figure 1.
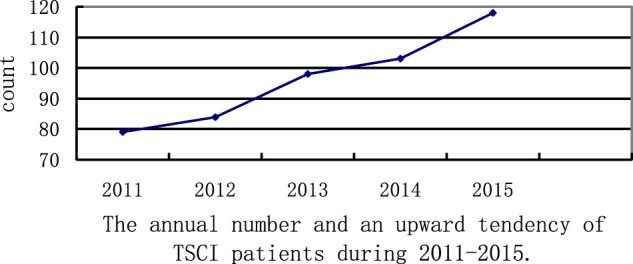
The annual number and an upward tendency of TSCI patients during 2011–2015.
Age and sex
Among 482 patients with TSCI identified, 384 were male and 112 were female with a male/female ratio of 3.42:1. The mean age of TSCI was 41.5 ± 12.6 years (men 42.4 ± 14.8 years, women 47.6 ± 13.8 years), with a range of 15–82 years. Furthermore, the age group 45–60 years was the largest (41.7%), followed by 31–45 years (23.8%). The count of patients with TSCI is shown in Table 1.
Table 1. Characteristics of patients with TSCI from 2011 to 2015.
| Years | 2011 | 2012 | 2013 | 2014 | 2015 | Total |
|---|---|---|---|---|---|---|
| Number of cases | 79 | 84 | 98 | 103 | 118 | 482 |
| Age | ||||||
| 0–15 | 1(1.2%) | 0(0) | 0(0) | 1(0.9%) | 1(0.8%) | 3(0.6%) |
| 16–30 | 14(17.7%) | 16(19.0%) | 15(15.3%) | 19(18.4%) | 23(19.4%) | 87(18.0%) |
| 31–45 | 21(26.5%) | 23(27.3%) | 29(29.5%) | 23(22.3%) | 19(16.1%) | 115(23.8%) |
| 46–60 | 36(45.5%) | 34(40.4%) | 39(39.7%) | 43(41.7%) | 49(41.5%) | 201(41.7%) |
| 61–75 | 5(6.3%) | 9(0.7%) | 12(12.2%) | 11(10.6%) | 22(18.6%) | 59(12.2%) |
| ≥76 | 2(2.5%) | 2(2.3%) | 3(3.0%) | 6(5.8%) | 4(3.3%) | 17(3.5%) |
| Average | 43.22 | 44.84 | 43.45 | 46.73 | 45.36 | 45.21 |
| Sex | ||||||
| Male | 61(77.2%) | 67(79.8%) | 84(85.8%) | 80(77.7%) | 92(78.0%) | 384(78.0%) |
| Female | 18(22.8%) | 17(20.2%) | 14(14.2%) | 23(22.3%) | 26(22.0%) | 98(20.0%) |
| Occupation | ||||||
| Peasant | 33(41.7%) | 31(36.9%) | 36(36.7%) | 40(38.8%) | 48(40.6%) | 188(39.0%) |
| Laborer | 25(31.6%) | 37(44.0%) | 31(31.6%) | 39(37.8%) | 47(39.8%) | 179(37.1%) |
| Drivers | 5(6.3%) | 4(4.7%) | 3(3%) | 5(4.8%) | 4(3.3%) | 21(4.3%) |
| Student | 1(1.2%) | 2(2.3%) | 1(1%) | 1(0.9%) | 2(1.6%) | 7(1.4%) |
| Civil servant | 3(3.7%) | 3(3.5%) | 5(5.1%) | 2(1.9%) | 3(3.3%) | 16(3.3%) |
| Other | 12(15.1%) | 7(8.3%) | 22(22.4%) | 16(15.5%) | 14(11.8%) | 71(14.7%) |
| Etiology | ||||||
| MVCs | 34(43.0%) | 31(36.9%) | 35(35.7%) | 34(33.0%) | 34(28.8%) | 168(34.8%) |
| Low fall | 11(13.9%) | 15(17.8%) | 19(19.3%) | 21(20.3%) | 25(21.1%) | 91(18.8%) |
| High fall | 22(27.8%) | 27(32.1%) | 31(31.6%) | 33(32.0%) | 34(28.8%) | 147(30.4%) |
| Struck by object | 6(7.5%) | 7(8.3%) | 5(5.1%) | 7(6.7%) | 9(7.6%) | 34(7.0%) |
| Sports | 1(1.2%) | 2(2.3%) | 1(1%) | 3(2.9%) | 2(1.6%) | 9(1.8%) |
| Others | 5(6.3%) | 2(2.3%) | 7(7.1%) | 5(4.8%) | 14(11.8%) | 33(6.8%) |
| Level of injury | ||||||
| Cervical | 32(40.5%) | 35(41.6%) | 44(44.8%) | 47(45.6%) | 57(48.3%) | 215(44.6%) |
| Thoracic | 26(32.9%) | 29(34.5%) | 35(35.7%) | 33(32.0%) | 36(30.5%) | 159(32.9%) |
| Lumbar | 21(26.5%) | 20(23.8%) | 19(19.3%) | 23(22.3%) | 25(21.1%) | 108(22.4%) |
| Impairment Scale (AIS) | ||||||
| A | 26(32.9%) | 30(35.7%) | 35(35.7%) | 43(41.7%) | 49(41.5%) | 183(37.9%) |
| B | 5(6.3%) | 8(9.5%) | 11(11.2%) | 9(8.7%) | 10(8.4%) | 43(8.9%) |
| C | 15(18.9%) | 18(21.4%) | 20(20.4%) | 25(24.2%) | 23(19.4%) | 101(20.9%) |
| D | 33(41.7%) | 28(33.3%) | 32(32.6%) | 26(25.2%) | 36(30.5%) | 155(32.1%) |
Cause of injury
The causes of TSCI are summarized in Table 1. According to the results, falls were the leading cause of injury, in which low falls and high falls comprised 18.8% and 30.4%, respectively. High falls usually occurred in the ages from 31 to 60. In contrast, in low falls group, the occurrence rate of TSCI steadily increased and was more common in the age >61 years old. MVCs were the second most common cause (34.8%), followed by injury from being struck by objects (7.0%), 1.8% of sport-related injury and other causes (6.8%) – none of the injuries involved gunshot or violence Fig. 2.
Figure 2.
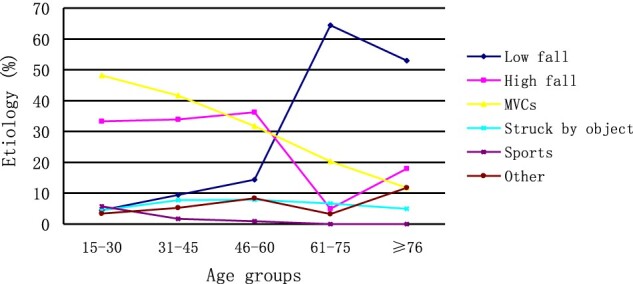
Percentages of TSCI according to age-groups by cause of injury, Guangdong, China from 2011 to 2015.
Neurological level and severity of injury
As revealed in Fig. 3, a bimodal distribution of level of TSCI was observed in this study. Injury to the cervical area formed the first peak, which accounted for 44.6% of all cases, thoracolumbar region injury constitutes the second peak. Percentages of AIS from injuries A, B, C, and D were 183 (37.9%), 43 (8.9%), 101 (20.5%), and 155 (32.1%) during this period, the AIS scale is shown in Table 1. The cases of TSCI was measured by the neurological level of injury (tetraplegia or paraplegia) and injury extent (complete or incomplete). Among patients (30.9%) presented with incomplete paraplegia, followed by incomplete tetraplegia (28.2%), complete paraplegia (24.4%) and (16.3%) complete tetraplegia.
Figure 3.

Distribution histogram of the injury level of the 482 patients.
Concomitant injuries
The detailed review of medical records revealed the most common concomitant injuries were head injuries (66 patients), followed by limb or pelvic fractures (50 patients), fractures of ribs (43 patients), and other injuries, such as lung contusion, hemopneumothorax, MVCs and high falls were more likely to result in concomitant injuries in TSCI patients compared with the other causes.
In-hospital mortality
A total of 11 patients (2.2% of admissions) died during hospitalization, and the average time from admission to death was 15 days. Nine were male and two were female. Eight patients had been operated on. Among the 11 patients, 4 (36.3%) were 60 or older, 10 had cervical TSCI and one had thoracic TSCI. In the end, 8 died from respiratory failure, 2 died of multiple organ failure and one died from acute pulmonary embolism.
Discussion
As there is no regional population-based registry system in Guangdong Province, the method used in the current study may be the only means of determining the epidemiology in a given area. The similarity of the results obtained in the past five consecutive years indicates high reliability. In the present study, the sex distribution (male/female) of TSCI was nearly 4:1, which is in concordance with the results of a similar study from the United States and two studies from China.8,9,12 This phenomenon can be explained by the fact that like most countries, men are more likely involved in hazardous work, while few women are engaged in heavy physical activities, such as working in the construction industry. In addition, the results showed that the mean age of patients with TSCI was 41.5 years old with a peak at the 30 to 45-year old age group, accounting for 41.7%. This is in accordance with the recent report from other countries.13–16 People within this age range are active and socially productive members of society. A disability such as TSCI would put both economic and social burdens on the patients and their families.
The level of injury took on bimodal distribution in the current study, which was similar to other reports from China.9,17 Spinal injury to the cervical area accounted for more than 40%, especially C4–C6 (39.8%), and was often associated with dislocation. Thoracic and lumbar spine traumas accounted for 85% of injuries in the 60 to 80-year old group, which was much higher than that of other age groups. This finding correlates with the aging population of China and the higher incidence of age-related osteoporosis in recent years.18 Disability in the older population would entail considerable social and economic consequences; the total cost for the treatment could be a heavy burden, with a significant impact on the healthcare system.
In most developed countries, MCVs have been the leading cause of SCI traditionally.19–21 On the contrary, in this study, falls were the most common accident mechanism for TSCI, accounting for 49.2%. This finding is in accordance with a previous study on TSCI conducted in Guangdong Province.10 This has similarly been seen in the United States where falls have become the leading cause of SCI since 2008.22 However, in the present study, MVCs were the second most common cause of TSCI (34.7%). Falls and MVCs were the two main causes of TSCI, and this was also demonstrated in other studies.23–26 The majority of high falls leading to TSCI occurred in the construction industry. This should be attributed to the accelerated industrialization process and the flourishing large-scale infrastructure projects in China. Therefore fall prevention strategies in the construction industry must be further strengthened. We also noted that the low falls accounted for 18.8% of the cases in this study, the results are not in agreement with those of a 2017 report form Guangdong Province, which found that only 1.5% of all cases with TSCI were caused by low falls.10 Further research is required to explain those differences between our data and previously reported data. Drunk driving used to be a serious social problem and posed a serious threat to public safety in China several years ago. With improved campaigns to prevent traffic accidents along with improvements in roads and more aggressive charges for drunk driving, this problem has been improving greatly in recent years. This may explain why the MVCs was not the leading cause of TSCIs. In addition, no gunshot injuries were reported, which could be attributed to a more stringent gun control than in other countries.
Regarding spinal cord injury severity, AIS A injury was the most common type of SCI in the present study. AIS D was the most common amongst those with a partial injury. AIS A and D injuries comprised the majority of TSCI cases. This finding was in agreement with other series.12,27,28 Complete injuries were mainly associated with MVCs and high falls, while incomplete injuries were associated with low falls in elderly people. Although low falls are low-impact, elderly people are vulnerable to spinal cord injuries due to degenerative changes of the cervical spine, osteoporosis and sensory deterioration.
Several limitations of our study needed be acknowledged. First, the present study was a hospital-based descriptive report, which identified only a small fraction of all cases with TSCI; In addition, Guangdong Province does not currently have a SCI registered system, therefore, the true prevalence rate could not be calculated. Second, this study was a retrospective study, some data was not accurately recorded at registration. Third, patients who died at the time of the accident or on the way to hospital were not considered, which also could lead to an underestimation of the incidence rate.
Conclusion
The number of TSCI patients in Guangdong Province is large and takes on a growing trend. The leading causes were falls and MVCs. The low-falls group tended to expand over this period. This data indicates that the preventive programs should focus on falls and traffic accidents. With China entering an ageing society, more appropriate preventative measures should be implemented for fall-related injuries among the elderly.
Acknowledgements
We are deeply grateful to the colleagues of study hospital’s medical record statistics room for help in the collection record data.
Disclaimer statements
Contributors None.
Funding None.
Conflict of interest The authors declare no conflict of interest.
References
- 1.Polinder S, Meerding WJ, Mulder S, Petridou E, van Beeck E.. EUROCOST reference group. Assessing the burden of injury in six European countries. Bull World Health Organ. 2007;85(1):27–34. doi: 10.2471/BLT.06.030973 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Lenehan B, Boran S, Street J, Higgins T, McCormack D, Poynton AR.. Demographics of acute admissions to a national spinal injuries unit. Eur Spine J. 2009;18(7):938–42. doi: 10.1007/s00586-009-0923-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Tator CH, Duncan EG, Edmonds VE, Lapczak LI, Andrews DF.. Changes in epidemiology of acute spinal cord injury from 1947 to 1981. SurgNeurol. 1993;40(3):207–15. [DOI] [PubMed] [Google Scholar]
- 4.Roche SJ, Sloane PA, McCabe JP.. Epidemiology of spine trauma in an Irish regional trauma unit: a 4-year study. Injury. 2008;39(4):436–42. doi: 10.1016/j.injury.2007.12.012 [DOI] [PubMed] [Google Scholar]
- 5.Jazayeri SB, Beygi S, Shokraneh F, Hagen EM, Rahimi-Movaghar V.. Incidence of traumatic spinal cord injury worldwide: a systematic review. Eur Spine J. 2015;24:905–18. doi: 10.1007/s00586-014-3424-6 [DOI] [PubMed] [Google Scholar]
- 6.Kumar R, Lim J, Mekary RA, Rattani A, Dewan MC, Sharif SY, et al. Traumatic spinal injury: global epidemiology and worldwide volume. World Neurosurg. 2018;S1878–S8750(18):30303–6. [DOI] [PubMed] [Google Scholar]
- 7.Chiu WT, Lin HC, Lam C, Chu SF, Chiang YH, Tsai SH.. Epidemilogy of traumatic spinal cord injury: comprisons between developed and developing countries. Asia Pac J Public Health. 2010;22(1):9–18. doi: 10.1177/1010539509355470 [DOI] [PubMed] [Google Scholar]
- 8.Li J, Liu G, Zheng Y, Hao C, Zhang Y, Wei B, et al. The epidemiological survey of acute traumatic spinal cord injury (ATSCI) of 2002 in Beijing municipality. Spinal Cord. 2011;49(7):777–82. doi: 10.1038/sc.2011.8 [DOI] [PubMed] [Google Scholar]
- 9.Ning GZ, Yu TQ, Feng SQ, Zhou XH, Ban DX, Liu Y, et al. Epidemiology of traumatic spinal cord injury in Tianjin, China. Spinal Cord. 2011;49(3):386–90. doi: 10.1038/sc.2010.130 [DOI] [PubMed] [Google Scholar]
- 10.Yang R, Guo L, Huang L, Wang P, Tang Y, Ye J, et al. Epicemiological characteristics of traumatic spinal cord injury in Guangdong, China. Spine (Phila Pa 1976). 2017;42(9):555–61. doi: 10.1097/BRS.0000000000001896 [DOI] [PubMed] [Google Scholar]
- 11.Kirshblum SC, Waring W, Biering-Sorensen F, Burns SP, Johansen M, Schmidt-Read M, et al. Reference for the 2011 revision of the international standards for neurological classification of spinal cord injury. J Spinal Cord Med. 2011;34(6):547–54. doi: 10.1179/107902611X13186000420242 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Devivo MJ. Epidemiology of traumatic spinal cord injury: trends and future implications. Spinal Cord. 2012;50(5):365–72. doi: 10.1038/sc.2011.178 [DOI] [PubMed] [Google Scholar]
- 13.Amin A, Bernard J, Nadarajah R, Davies N, Gow F, Tucker S.. Spinal injuries admitted to a specialist centre over a 5-year period: a study to evaluate delayed admission. Spinal Cord. 2005;43(7):434–7. doi: 10.1038/sj.sc.3101734 [DOI] [PubMed] [Google Scholar]
- 14.Divanoglou A, Levi R.. Incidence of traumatic spinal cord injury in Thessaloniki, Greece and Stockholm, Sweden: a prospective population-based study. Spinal Cord. 2009;47(11):796–801. doi: 10.1038/sc.2009.28 [DOI] [PubMed] [Google Scholar]
- 15.Couris CM, Guilcher SJ, Munce SE, Fung K, Craven BC, Verrier M, et al. Characteristics of adults with incident traumatic spinal cord injury in Ontario, Canada. Spinal Cord. 2010;48(1):39–44. doi: 10.1038/sc.2009.77 [DOI] [PubMed] [Google Scholar]
- 16.McColl MA, Charlifue S, Glass C, Savic G, Meehan M.. International differences in ageing and spinal cord injury. Spinal Cord. 2002;40(3):128–36. doi: 10.1038/sj.sc.3101264 [DOI] [PubMed] [Google Scholar]
- 17.Feng HY, Ning GZ, Feng SQ, Yu TQ, Zhou HX.. Epidemiological profile of 239 traumatic spinal cord injury cases over a period of 12 years in Tianjin, China. J Spinal Cord Med. 2011;34(4):388–94. doi: 10.1179/2045772311Y.0000000017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Liu P, Yao Y, Liu MY, Fan WL, Chao R, Wang ZG, et al. Spinal trauma in mainland China form 2001 to 2007: an epidemiological study based on a nationwide database. Spine. 2012;37(15):1310–5. doi: 10.1097/BRS.0b013e3182474d8b [DOI] [PubMed] [Google Scholar]
- 19.Van den Berg ME, Castellote JM, Mahillo-Fernandez I, de Pedro Cuesta J.. Incidence of spinal cord injury worldwide: a systematic review. Neuroepidemiology. 2010;34(3):184–92. doi: 10.1159/000279335 [DOI] [PubMed] [Google Scholar]
- 20.Burke DA, Linden RD, Zhang YP, Maiste AC, Shields CB.. Incidence rates and populations at risk for spinal cord injury: a regional study. Spinal Cord. 2001;39(5):274–8. doi: 10.1038/sj.sc.3101158 [DOI] [PubMed] [Google Scholar]
- 21.Albert T, Ravaud JF.. Tetrafigap group. Rehabilitation of spinal cord injury in France: a nationwide multicentre study of incidence and regional disparities. Spinal Cord. 2005;43(6):357–65. doi: 10.1038/sj.sc.3101717 [DOI] [PubMed] [Google Scholar]
- 22.Jain NB, Ayers GD, Peterson EN, Harris MB, Morse L, O’Connor KC, et al. Traumatic spinal cord injury in the United States, 1993–2012. JAMA. 2015 Jun 9;313(22):2236–43. doi: 10.1001/jama.2015.6250 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Wang HF, Yin ZS, Chen Y, Duan ZH, Hou S, He J.. Epidemiological features of traumatic spinal cord injury in Anhui Province, China. Spinal Cord. 2013;51(1):20–2. doi: 10.1038/sc.2012.92 [DOI] [PubMed] [Google Scholar]
- 24.Shin JC, Kim DH, Yu SJ, Yang HE, Yoon SY.. Epidemiologicchange of patients with spinal cord injury. Ann Rehabil Med. 2013;37(1):50–6. doi: 10.5535/arm.2013.37.1.50 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Cripps RA, Lee BB, Wing P, Weerts E, Mackay J, Brown D.. A global map for traumatic spinal cord epidemiology: towards a living data repository for injury prevention. Spinal Cord. 2011;49(4):493–501. doi: 10.1038/sc.2010.146 [DOI] [PubMed] [Google Scholar]
- 26.Lenehan B, Street J, Kwon BK, Noonan V, Zhang H, Fisher CG, et al. The epidemiology of traumatic spinal cord injury in British Columbia, Canada. Spine. 2012;37(4):321–9. doi: 10.1097/BRS.0b013e31822e5ff8 [DOI] [PubMed] [Google Scholar]
- 27.Ning GZ, Mu ZP, Shangguan L, Tang Y, Li CQ, Zhang ZF.. Epidemiological features of traumatic spinal cord injury in Chongqing, China. J Spinal Cord Med. 2016;39(4):455–60. doi: 10.1080/10790268.2015.1101982 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Celani MG, Spizzichino L, Ricci S, Zampolini M, Franceschini M.. Retrospective study group on SCI. Spinal cord injury in Italy: a multicenter retrospective study. Arch Phys Med Rehabil. 2001;82(5):589–96. doi: 10.1053/apmr.2001.21948 [DOI] [PubMed] [Google Scholar]