

Abstract
Purpose
To develop population norms for the EQ-5D-5L questionnaire based on a representative sample of Moscow citizens.
Methods
We used quota sampling accounting for sex, age group and administrative district of residence. Respondents in randomly selected outdoor and indoor locations were surveyed with the official Russian paper-and-pencil version of the EQ-5D-5L questionnaire and a set of socio-demographic questions. We estimated four types of EQ-5D results: the distribution of limitations according to EQ-5D-5L dimensions, the perception of the health-related quality of life (HRQoL) with a visual analogue scale (EQ VAS), the unweighted score for a respondent’s health state (Level Sum Score, LSS) and the Russian health preferences-based weighted score (EQ index). In order to estimate the EQ-5D-5L index, we used a newly developed Russian EQ-5D-3L value set, together with EuroQol Group cross-over methodology.
Results
A total of 1020 respondents (18–93 years old) from the general Moscow adult population completed the EQ-5D-5L questionnaire. HRQoL domains with the largest number of identified health limitations were pain/discomfort (48.6%) and anxiety/depression (44.1%). Two hundred seventy-nine respondents (27.0%) did not report any health restrictions. The mean EQ VAS and EQ-5D-5L index were 74.1 (SD 17.3) and 0.907 (0.106) respectively. Multivariate analysis showed that female sex, advanced age and lack of access to the Internet had a negative influence on HRQoL, whereas residence in certain districts had a positive impact.
Conclusions
The study provides population norms of health-related quality of life in Moscow, measured according to the EQ-5D-5L questionnaire. These reference values can be used to optimise the effectiveness of resource allocation in healthcare.
Electronic supplementary material
The online version of this article (10.1007/s11136-020-02705-0) contains supplementary material, which is available to authorised users.
Keywords: Health-related quality of life, Patient-reported outcomes, Normative values, Reference values, EQ-5D, Russia
Introduction
Over the past few years, health technology assessment (HTA) has been implemented in most Central and Eastern European (CEE) countries—based on international standards or through developments to the original HTA system, as in post-Soviet countries [1]. Russia, being the largest country in the world and the world’s ninth most populous country, implemented HTA into federal law in 2014 [2]. In spite of this, local healthcare decision-makers do not commonly use health-related quality of life (HRQoL) in outcome measurement and resource allocation.
When measuring HRQoL, one can choose between generic and disease-specific instruments [3]. Generic instruments focus on general health status, including physical, functional, and emotional domains. They apply to every health state and may be useful for comparisons between unrelated medical technologies. In some specific diseases, their use may be limited by a lack of sensitivity. One of them, the EQ-5D, is by far the most commonly used instrument for calculating utility scores, both in the CEE region [1] and all over the world [4]. The main advantages of EQ-5D are its widespread use, brevity and simplicity of administration [5]. Official versions are available for over 200 languages, so the data collected with EQ-5D can be successfully utilised for international comparisons. A five-level version of the EQ-5D (EQ-5D-5L) was developed, to improve the sensitivity of the original, three-level version (EQ-5D-3L), by adding two intermediate answer options to all of the dimensions [6, 7].
Population reference data for a specific country or region (sometimes called population norm data or simply population norms), can be used to compare profiles for patients with particular conditions with data for the average person in the general population from a similar age and gender group. Additionally, population norms enable comparison of the burden of the disease with the general population’s health, as well as the measurement of health inequalities [8].
Moscow has one of the largest municipal economies in Europe, which also accounts for more than one-fifth of the country’s gross domestic product. In Russia, Muscovites are in second place in terms of life expectancy, second only to inhabitants of the Republic of Ingushetia [9]. Although there is a long tradition of health surveys in Moscow, none of them has involved instruments from the EQ-5D family.
Our study aimed to develop population norms for HRQoL in Moscow, based on the EQ-5D-5L questionnaire. Bearing in mind the size of Russia, and knowing that most of the pilot projects are carried out firstly in Moscow before encompassing other regions, we have decided to start from the capital.
Methods
Sample
To make our study representative, we used quota sampling. Quotas accounted for sex, age group and the district of residence (okrug). The official division of Moscow in place until 2012, with ten administrative areas, was used. Seven age strata were distinguished (18–24, 25–34, 35–44, 45–54, 55–65, 64–75 and 75+ years). Quotas were built based on the Russian Statistics Office (ROSSTAT) data from 2014 [10].
Survey
The official Russian paper-and-pencil version of the EQ-5D-5L was used. The EQ-5D-5L consists of two parts: a descriptive system (a report of symptoms and abilities) and a visual analogue scale (EQ VAS). The descriptive system includes five dimensions: mobility (MO), self-care (SC), usual activities (UA), pain/discomfort (PD), and anxiety/depression (AD). EQ-5D-5L dimensions comprise five levels of severity: no problems, slight problems, moderate problems, severe problems, and extreme problems [4]. Responses for all the five dimensions can be combined to form a five-digit number describing the respondent’s health state (from “11111”, meaning “no problems at all”, to “55555”, meaning “extreme problems” in all five dimensions). A total of 3125 possible health states are defined in this way. The EQ-5D health states may be converted into a single summary index by applying a formula that attaches values to each of the levels in each dimension (EQ Index) [11]. To estimate the EQ-5D-5L index, we used a newly developed Russian EQ-5D-3L value set [12], together with EuroQol Group cross-over methodology [13]. We also calculated unweighted Level Sum Scores (LSS) of the health states, a crude measure of severity of EQ-5D profiles, which may be a useful tool for performing comparisons among different populations.
The additional socio-demographic questionnaire included questions about: respondents’ age, level of education, monthly income, smoker/non-smoker and Internet access and usage. The question about the education provided nine possible answers. For data analysis, the responses were aggregated into three levels: primary (up to 9 years of education), secondary (up to 11 years of teaching, secondary vocational, incomplete higher) or higher education (bachelor’s degree, master’s degree or higher).
Data collection
Two researchers (MH, AT) approached randomly selected respondents in randomly chosen locations, including parks, bus stops, transport hubs, car washes, malls, markets, restaurants, cafes and universities. The respondents were asked to fill in the EQ-5D-5L on their own but were guided by the interviewer if necessary. Answers to questions concerning demographic characteristics were collected by the interviewers. Items were read by the interviewer a maximum three times, and no additional comments were provided. A total of 10% of the interviews were subjected to data input quality control (the data of every tenth questionnaire in the paper form were verified with the data entered in the electronic database). Interviewers’ cross-validation was performed (MH carried out control of the data from the questionnaires entered by AT and vice versa).
Analysis
We estimated four types of EQ-5D results: (1) the distribution of limitations according to EQ-5D-5L dimensions, (2) the perception of the health-related quality of life with EQ VAS, (3) the unweighted score for the respondent’s health state—the Level Sum Score (LSS), and (4) the weighted score for the health state—the EQ-5D-5L index. For continuous variables, we calculated the following descriptive statistics: mean, standard deviation and 95% confidence interval. Estimations were presented for the whole sample, as well as for the seven predefined age groups, in the EuroQol Group’s standardised format, to facilitate comparative research. We used multiple linear regression to examine the associations of socio-demographic characteristics with the EQ-5D-5L index and EQ VAS scores. All variables, including age, were entered into the models as categorical variables. Regression coefficients were presented together with information about the level of statistical significance. The analysis was carried out using Microsoft Excel and StatsDirect software, version 2.8.0 (StatsDirect Ltd, England).
Results
From February to October 2017, a total of 1020 respondents from Moscow completed the EQ-5D-5L questionnaire. The sample approximated to the general adult Moscow population in terms of age, gender and district of residence (see Table 1 for details). The respondents were aged 18–93 years (mean 44.8, SD 19.0). The sample was characterised by a relatively high level of education (nearly 60% holding a university degree; only 0.5% with just primary level education). A substantial percentage of respondents (21.6%) refused to disclose their income.
Table 1.
Study sample characteristics and comparison with Moscow general adult population (n = 11,815,393)
| Study sample n (%) |
General adult population* % |
|
|---|---|---|
| N | 1020 (100.0) | |
| Sex | ||
| Female | 555 (54.4) | 54.0 |
| Male | 465 (45.6) | 46.0 |
| Age groups, years | ||
| 18–24 | 184 (18.0) | 18.3 |
| 25–34 | 190 (18.6) | 17.6 |
| 35–44 | 170 (16.7) | 16.4 |
| 45–54 | 150 (14.7) | 15.0 |
| 55–64 | 126 (12.4) | 12.8 |
| 65–74 | 106 (10.4) | 10.4 |
| ≥ 75 | 94 (9.2) | 9.5 |
| Moscow District | ||
| Central | 69 (6.8) | 6.4 |
| East | 126 (12.4) | 12.6 |
| North | 98 (9.6) | 9.7 |
| North-East | 118 (11.6) | 11.8 |
| North-West | 88 (8.6) | 8.2 |
| South | 148 (14.5) | 14.9 |
| South-East | 116 (11.4) | 11.4 |
| South-West | 121 (11.9) | 11.9 |
| West | 116 (11.4) | 11.1 |
| Zelenograd | 20 (2.0) | 1.9 |
| Education | ||
| Primary | 6 (0.5) | 6.4 |
| Secondary | 411 (40.5) | 51.3 |
| Higher | 599 (59.0) | 42.1 |
| No education | 0 (0) | 0.2 |
| Income, RUB | ||
| ≤ 15,000 | 102 (10.0) | [≤ 14,000 RUB]: 5.3 |
| 15,001–30,000 | 246 (24.1) | [14,000–27,000]: 17.1 |
| 30,001–50,000 | 174 (17.1) | [27,000–45,000]: 23.7 |
| 50,001–80,000 | 147 (14.4) | [45,000–60,000]: 14.7 |
| > 80,000 | 131 (12.8) | [> 60,000 RUB]: 39.2 |
| Refused | 220 (21.6) | – |
| Smoking status (current) | ||
| No | 736 (72.2) | 72.5 |
| Yes | 276 (27.1) | 27.0 |
| Refused | 8 (0.8) | 0.5 |
| Internet usage | ||
| Everyday | 785 (77.9) | 89.2 |
| Minimum once a week | 81 (8.0) | |
| No | 142 (14.1) | 10.8 |
Table 2 presents the results of the EQ-5D-5L descriptive system according to gender and age group. The health-related quality of life domains with the most significant number of identified health restrictions were pain/discomfort (48.6%) and anxiety/depression (44.1%), with the lowest being self-care (11.5%). The most significant number of severe and extreme health limitations was identified in the mobility dimension (3.7%), followed by anxiety/depression (3.2%).
Table 2.
Prevalence of EQ-5D-5L responses by age group and gender (%)
| Level | Mobility | Self-care | Usual activities | Pain/discomfort | Anxiety/depression | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | Male | Female | Total | Male | Female | Total | Male | Female | Total | Male | Female | Total | Male | Female | |
| All | n = 1020 | n = 465 | n = 555 | ||||||||||||
| 1 | 64.3 | 68.2 | 61.1 | 88.5 | 89.5 | 87.7 | 68.0 | 73.3 | 63.6 | 51.4 | 58.5 | 45.4 | 55.9 | 61.3 | 51.4 |
| 2 | 23.1 | 22.4 | 23.8 | 9.0 | 9.0 | 9.0 | 23.9 | 19.1 | 27.9 | 36.8 | 31.8 | 40.9 | 30.6 | 27.1 | 33.5 |
| 3 | 8.8 | 8.0 | 9.5 | 1.5 | 1.1 | 1.8 | 5.8 | 5.6 | 5.9 | 9.4 | 8.6 | 10.1 | 10.4 | 9.7 | 11.0 |
| 4 | 3.6 | 1.5 | 5.4 | 1.0 | 0.4 | 1.4 | 1.9 | 1.5 | 2.2 | 2.1 | 1.1 | 2.9 | 2.4 | 1.9 | 2.7 |
| 5 | 0.1 | 0.0 | 0.2 | 0.0 | 0.0 | 0.0 | 0.4 | 0.4 | 0.4 | 0.4 | 0.0 | 0.7 | 0.8 | 0.0 | 1.4 |
| Any problems | 35.7 | 31.8 | 38.9 | 11.5 | 10.5 | 12.3 | 32.0 | 26.7 | 36.4 | 48.6 | 41.5 | 54.6 | 44.1 | 38.7 | 48.6 |
| 18–24 years | n = 184 | n = 85 | n = 99 | ||||||||||||
| 1 | 87.0 | 88.2 | 85.9 | 95.7 | 98.8 | 92.9 | 76.6 | 82.4 | 71.7 | 62.0 | 80.0 | 46.5 | 54.3 | 71.8 | 39.4 |
| 2 | 12.0 | 9.4 | 14.1 | 4.3 | 1.2 | 7.1 | 19.6 | 14.1 | 24.2 | 33.7 | 17.6 | 47.5 | 34.2 | 23.5 | 43.4 |
| 3 | 1.1 | 2.4 | 0.0 | 0.0 | 0.0 | 0.0 | 1.6 | 1.2 | 2.0 | 2.2 | 2.4 | 2.0 | 9.2 | 3.5 | 14.1 |
| 4 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 1.1 | 1.2 | 1.0 | 1.6 | 0.0 | 3.0 | 1.6 | 1.2 | 2.0 |
| 5 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 1.1 | 1.2 | 1.0 | 0.5 | 0.0 | 1.0 | 0.5 | 0.0 | 1.0 |
| Any problems | 13.0 | 11.8 | 14.1 | 4.3 | 1.2 | 7.1 | 23.4 | 17.6 | 28.3 | 38.0 | 20.0 | 53.5 | 45.7 | 28.2 | 60.6 |
| 25–34 years | n = 190 | n = 83 | n = 107 | ||||||||||||
| 1 | 85.3 | 88.0 | 83.2 | 96.3 | 96.4 | 96.3 | 74.7 | 72.3 | 76.6 | 62.6 | 62.7 | 62.6 | 58.9 | 62.7 | 56.1 |
| 2 | 12.1 | 8.4 | 15.0 | 3.2 | 3.6 | 2.8 | 17.4 | 16.9 | 17.8 | 29.5 | 26.5 | 31.8 | 29.5 | 27.7 | 30.8 |
| 3 | 2.6 | 3.6 | 1.9 | 0.5 | 0.0 | 0.9 | 5.8 | 7.2 | 4.7 | 7.9 | 10.8 | 5.6 | 8.9 | 8.4 | 9.3 |
| 4 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 1.6 | 2.4 | 0.9 | 0.0 | 0.0 | 0.0 | 1.6 | 1.2 | 1.9 |
| 5 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.5 | 1.2 | 0.0 | 0.0 | 0.0 | 0.0 | 1.1 | 0.0 | 1.9 |
| Any problems | 14.7 | 12.0 | 16.8 | 3.7 | 3.6 | 3.7 | 25.3 | 27.7 | 23.4 | 37.4 | 37.3 | 37.4 | 41.1 | 37.3 | 43.9 |
| 35–44 years | n = 170 | n = 76 | n = 94 | ||||||||||||
| 1 | 74.7 | 80.3 | 70.2 | 95.9 | 98.7 | 93.6 | 81.2 | 88.2 | 75.5 | 60.0 | 68.4 | 53.2 | 54.7 | 60.5 | 50.0 |
| 2 | 18.8 | 15.8 | 21.3 | 4.1 | 1.3 | 6.4 | 15.9 | 6.6 | 23.4 | 36.5 | 28.9 | 42.6 | 35.9 | 28.9 | 41.5 |
| 3 | 6.5 | 3.9 | 8.5 | 0.0 | 0.0 | 0.0 | 2.9 | 5.3 | 1.1 | 2.9 | 1.3 | 4.3 | 8.8 | 10.5 | 7.4 |
| 4 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.6 | 1.3 | 0.0 | 0.0 | 0.0 | 0.0 |
| 5 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.6 | 0.0 | 1.1 |
| Any problems | 25.3 | 19.7 | 29.8 | 4.1 | 1.3 | 6.4 | 18.8 | 11.8 | 24.5 | 40.0 | 31.6 | 46.8 | 45.3 | 39.5 | 50.0 |
| 45–54 years | n = 150 | n = 69 | n = 81 | ||||||||||||
| 1 | 66.0 | 75.4 | 58.0 | 93.3 | 97.1 | 90.1 | 68.7 | 81.2 | 58.0 | 48.0 | 55.1 | 42.0 | 61.3 | 62.3 | 60.5 |
| 2 | 24.0 | 17.4 | 29.6 | 5.3 | 2.9 | 7.4 | 28.0 | 17.4 | 37.0 | 44.0 | 39.1 | 48.1 | 24.7 | 23.2 | 25.9 |
| 3 | 6.7 | 5.8 | 7.4 | 1.3 | 0.0 | 2.5 | 3.3 | 1.4 | 4.9 | 6.7 | 4.3 | 8.6 | 10.7 | 10.1 | 11.1 |
| 4 | 3.3 | 1.4 | 4.9 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 1.3 | 1.4 | 1.2 | 3.3 | 4.3 | 2.5 |
| 5 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| Any problems | 34.0 | 24.6 | 42.0 | 6.7 | 2.9 | 9.9 | 31.3 | 18.8 | 42.0 | 52.0 | 44.9 | 58.0 | 38.7 | 37.7 | 39.5 |
| 55–64 years | n = 126 | n = 59 | n = 67 | ||||||||||||
| 1 | 53.2 | 64.4 | 43.3 | 89.7 | 91.5 | 88.1 | 65.9 | 71.2 | 61.2 | 45.2 | 55.9 | 35.8 | 60.3 | 66.1 | 55.2 |
| 2 | 32.5 | 27.1 | 37.3 | 8.7 | 6.8 | 10.4 | 27.8 | 23.7 | 31.3 | 43.7 | 37.3 | 49.3 | 29.4 | 27.1 | 31.3 |
| 3 | 11.9 | 6.8 | 16.4 | 0.8 | 1.7 | 0.0 | 5.6 | 5.1 | 6.0 | 9.5 | 6.8 | 11.9 | 7.1 | 6.8 | 7.5 |
| 4 | 2.4 | 1.7 | 3.0 | 0.8 | 0.0 | 1.5 | 0.8 | 0.0 | 1.5 | 1.6 | 0.0 | 3.0 | 3.2 | 0.0 | 6.0 |
| 5 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| Any problems | 46.8 | 35.6 | 56.7 | 10.3 | 8.5 | 11.9 | 34.1 | 28.8 | 38.8 | 54.8 | 44.1 | 64.2 | 39.7 | 33.9 | 44.8 |
| 65–74 years | n = 106 | n = 50 | n = 56 | ||||||||||||
| 1 | 27.4 | 28.0 | 26.8 | 76.4 | 72.0 | 80.4 | 57.5 | 64.0 | 51.8 | 37.7 | 42.0 | 33.9 | 49.1 | 52.0 | 46.4 |
| 2 | 43.4 | 54.0 | 33.9 | 18.9 | 24.0 | 14.3 | 32.1 | 30.0 | 33.9 | 39.6 | 44.0 | 35.7 | 30.2 | 30.0 | 30.4 |
| 3 | 17.0 | 14.0 | 19.6 | 1.9 | 2.0 | 1.8 | 6.6 | 4.0 | 8.9 | 16.0 | 12.0 | 19.6 | 15.1 | 16.0 | 14.3 |
| 4 | 12.3 | 4.0 | 19.6 | 2.8 | 2.0 | 3.6 | 3.8 | 2.0 | 5.4 | 5.7 | 2.0 | 8.9 | 3.8 | 2.0 | 5.4 |
| 5 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.9 | 0.0 | 1.8 | 1.9 | 0.0 | 3.6 |
| Any problems | 72.7 | 72.0 | 73.2 | 23.6 | 28.0 | 19.6 | 42.5 | 36.0 | 48.2 | 62.3 | 58.0 | 66.1 | 50.9 | 48.0 | 53.6 |
| 75+ years | n = 94 | n = 43 | n = 51 | ||||||||||||
| 1 | 12.8 | 9.3 | 15.7 | 50.0 | 46.5 | 52.9 | 27.7 | 32.6 | 23.5 | 21.3 | 18.6 | 23.5 | 47.9 | 41.9 | 52.9 |
| 2 | 38.3 | 51.2 | 27.5 | 34.0 | 44.2 | 25.5 | 39.4 | 39.5 | 39.2 | 34.0 | 41.9 | 27.5 | 27.7 | 32.6 | 23.5 |
| 3 | 30.9 | 32.6 | 29.4 | 6.4 | 7.0 | 11.8 | 22.3 | 20.9 | 23.5 | 35.1 | 34.9 | 35.3 | 17.0 | 18.6 | 15.7 |
| 4 | 17.0 | 7.0 | 25.5 | 9.6 | 2.3 | 9.8 | 9.6 | 7.0 | 11.8 | 7.4 | 4.7 | 9.8 | 5.3 | 7.0 | 3.9 |
| 5 | 1.1 | 0.0 | 2.0 | 0.0 | 0.0 | 0.0 | 1.1 | 0.0 | 2.0 | 2.1 | 0.0 | 3.9 | 2.1 | 0.0 | 3.9 |
| Any problems | 87.2 | 90.7 | 84.3 | 50.0 | 53.5 | 47.1 | 72.3 | 67.4 | 76.5 | 78.7 | 81.4 | 76.5 | 52.1 | 58.1 | 47.1 |
Health restrictions grew with age group (Fig. 1). This was particularly evident in terms of the mobility domain. The only dimension that followed a different pattern was anxiety/depression, where the level of limitations was generally high (> 40%) and relatively stable across age groups.
Fig. 1.
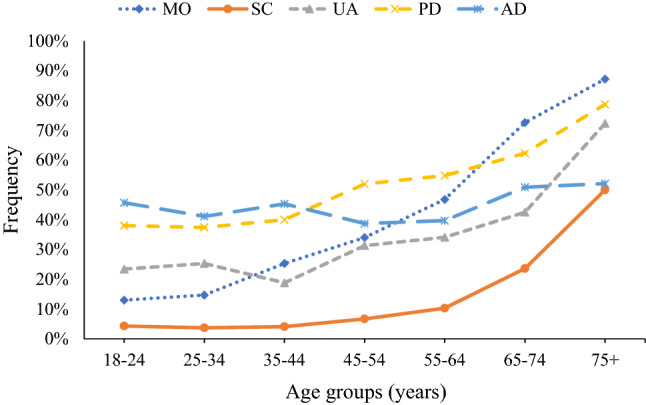
Prevalence of health limitations (any level of severity) for EQ-5D-5L dimensions according to age group
Analysing five EQ-5D-5L dimensions within seven age groups, we can state that, in general, females are characterised by expressing a lower health-related quality of life (in 29 out of 35 comparisons). The most striking difference concerned the youngest age group (18–24 years), and the domains pain/discomfort and anxiety/depression, where the absolute difference between the frequency of problems reported by women and men was 33.5% and 32.4%, respectively (Supplemental Fig. 1).
In total, we observed 170 different health states (out of the 3125 possible defined by EQ-5D-5L). The five most common health states accounted for 50.7% of cases, while the ten most common accounted for 60.8% of cases (Table 3). Two hundred seventy-nine respondents (27.4%) did not report any health restrictions (health state ‘11111’).
Table 3.
Most common EQ-5D-5L health states among the Moscow population
| Health state | n | % | Mean EQ-5D-5L Index | Mean EQ VAS | n males | n females | ||
|---|---|---|---|---|---|---|---|---|
| All | Males | Females | ||||||
| 11111 | 279 | 27.4 | 1.000 | 84.9 | 85.2 | 84.6 | 154 | 125 |
| 11112 | 85 | 8.3 | 0.967 | 82.6 | 81.2 | 83.8 | 40 | 45 |
| 11121 | 55 | 5.4 | 0.947 | 77.7 | 77.5 | 78.0 | 27 | 28 |
| 11122 | 54 | 5.3 | 0.915 | 77.2 | 81.0 | 75.9 | 14 | 40 |
| 21121 | 44 | 4.3 | 0.913 | 72.5 | 73.5 | 71.8 | 20 | 24 |
| 21122 | 25 | 2.5 | 0.881 | 67.7 | 74.0* | 63.5* | 10 | 15 |
| 11222 | 21 | 2.1 | 0.856 | 67.0 | 69.4 | 65.3 | 9 | 12 |
| 21111 | 21 | 2.1 | 0.966 | 73.3 | 71.0 | 75.5 | 10 | 11 |
| 11211 | 19 | 1.9 | 0.941 | 78.3 | 80.0 | 76.4 | 10 | 9 |
| 11212 | 17 | 1.7 | 0.909 | 78.0 | 81.0 | 75.2 | 8 | 9 |
| 11123 | 16 | 1.6 | 0.906 | 70.5 | 72.6 | 68.9 | 7 | 9 |
| 11221 | 16 | 1.6 | 0.889 | 73.1 | 71.0 | 74.1 | 5 | 11 |
| 21222 | 16 | 1.6 | 0.822 | 71.2 | 76.3 | 69.5 | 4 | 12 |
| 11113 | 12 | 1.2 | 0.959 | 70.0 | 69.0 | 75.0 | 10 | 2 |
| 11213 | 12 | 1.2 | 0.900 | 70.8 | 63.3 | 73.3 | 3 | 9 |
| 21112 | 12 | 1.2 | 0.934 | 73.6 | 70.8 | 76.3 | 6 | 6 |
| 21221 | 12 | 1.2 | 0.922 | 67.3 | 63.7 | 70.8 | 6 | 6 |
*p < 0.05 males vs females, Mann–Whitney test
The whole sample distribution of the EQ-5D-5L index, EQ VAS and LSS is presented in Supplemental Fig. 2 (parallel chart created in IBM Watson Studio Cloud). As in other general population studies, the health-related quality of life of Moscow residents measured according to the EQ-5D-5L index or LSS, clustered around the highest values, whereas when measured by EQ VAS it was far from the top.
Detailed characteristics of the EQ-5D-5L index and EQ VAS, according to gender and age group, are shown in Table 4. Similar data summary concerning LSS is presented in Supplemental Table 1.
Table 4.
EQ-5D-5L index and EQ VAS according to age group and gender
| Age group (years) | All | Male | Female | |||
|---|---|---|---|---|---|---|
| n | Mean (SD) [95% CI] | n | Mean (SD) [95% CI] | n | Mean (SD) [95% CI] | |
| EQ-5D-5L Index | ||||||
| All ages | 1020 | 0.907 (0.106) [0.900–0.913] | 465 | 0.923 (0.083) [0.918–0.931] | 555 | 0.893 (0.120) [0.883–0.903] |
| 18–24 | 184 | 0.934 (0.090) [0.921–0.947] | 85 | 0.960 (0.056) [0.948–0.972] | 99 | 0.911 (0.106) [0.890–0.933] |
| 25–34 | 190 | 0.937 (0.074) [0.927–0.948] | 83 | 0.937 (0.070) [0.921–0.953] | 107 | 0.937 (0.077) [0.922–0.952] |
| 35–44 | 170 | 0.938 (0.064) [0.929–0.948] | 76 | 0.952 (0.060) [0.938–0.966] | 94 | 0.927 (0.065) [0.914–0.940] |
| 45–54 | 150 | 0.917 (0.081) [0.904–0.930] | 69 | 0.935 (0.075) [0.917–0.953] | 81 | 0.902 (0.083) [0.884–0.921] |
| 55–64 | 126 | 0.908 (0.084) [0.891–0.921] | 59 | 0.928 (0.066) [0.911–0.945] | 67 | 0.886 (0.094) [0.863–0.909] |
| 65–74 | 106 | 0.855 (0.012) [0.834–0.878] | 50 | 0.878 (0.079) [0.856–0.900] | 56 | 0.835 (0.143) [0.797–0.873] |
| 75+ | 94 | 0.778 (0.169) [0.744–0.813] | 43 | 0.802 (0.099) [0.771–0.832] | 51 | 0.759 (0.210) [0.700–0.818] |
| EQ VAS | ||||||
| All ages | 1020 | 74.1 (17.3) [73.0–75.1] | 465 | 75.3 (17.4) [73.7–76.9] | 555 | 73.0 (17.2) [71.6–74.5] |
| 18–24 | 184 | 78.7 (14.8) [76.6–80.9] | 85 | 83.2 (12.1) [80.6–85.8] | 99 | 74.9 (15.9) [71.7–78.0] |
| 25–34 | 190 | 80.2 (13.0) [78.3–82.0] | 83 | 80.2 (13.9) [77.2–83.2] | 107 | 80.2 (12.3) [77.8–79.0] |
| 35–44 | 170 | 77.5 (14.4) [75.3–79.7] | 76 | 79.1 (12.8) [76.1–82.0] | 94 | 76.3 (15.6) [73.1–79.4] |
| 45–54 | 150 | 75.3 (16.8) [72.6–78.0] | 69 | 78.0 (16.9) [73.9–82.0] | 81 | 73.1 (16.6) [69.4–76.7] |
| 55–64 | 126 | 74.2 (15.2) [71.6–76.9] | 59 | 73.2 (15.1) [69.3–77.2] | 67 | 75.1 (15.4) [71.3–78.8] |
| 65–74 | 106 | 62.2 (18.0) [58.7–65.6] | 50 | 62.8 (17.7) [57.7–67.8] | 56 | 61.6 (18.3) [56.7–66.5] |
| 75+ | 94 | 57.4 (20.5) [53.2–61.6] | 43 | 56.4 (21.9) [49.7–63.1] | 51 | 58.3 (19.4) [52.9–63.8] |
In general, lower HRQoL values start to be evident from the age of 45, and the decline in HRQoL accelerates from 65 years old. Women are characterised by worse HRQoL ratings than men, except for two age groups (55–64 years, 75+ years) in EQ VAS.
Electronic Supplementary Material (Supplemental Tables 2–9, Supplemental Figs. 3–8) presents the descriptive analysis of population data, preceding the regression analysis. Better educated respondents tend to report fewer limitations within UA, but more within AD. Young (18–24 years) males with primary or secondary education reported fewer problems within all EQ-5D-5L dimensions, than those with higher education. Young (18–24 years) females with primary or secondary education reported substantially fewer problems within PD and AD dimensions (by 14.7% and 22.1%, respectively), than those with higher education. Better educated women had higher EQ VAS and EQ-5D-5L index scores across all age groups. Relationship between current smoking and HRQoL was unsystematic. Higher income was associated with better EQ VAS and EQ-5D-5L index scores, fewer problems within MO, UA and PD dimensions, but more anxiety and depression.
Table 5 presents the results of multivariate analysis on socio-demographic characteristics, which significantly predicted HRQoL outcomes. Female sex, advanced age (65+ years) and lack of access to the Internet had a negative influence. In contrast, residence in selected districts (Zelenograd, North-West, South-East) had a positive impact on health status, as measured by the EQ-5D-5L index. The results for EQ VAS were similar, although not statistically significant for district-based dependences.
Table 5.
Relation of EQ-5D-5L index and EQ VAS with demographic characteristics of respondents (N = 1020)
| n (%) | EQ Index | EQ VAS | |||
|---|---|---|---|---|---|
| Mean (SD) | Multiple linear regression coefficients | Mean (SD) | Multiple linear regression coefficients | ||
| Intercept | 0.938 | 78.4 | |||
| Gender | |||||
| Male | 465 (45.6) | 0.923 (0.083) | – | 75.3 (17.4) | – |
| Female | 555 (54.4) | 0.893 (0.120) | − 0.034** | 73.0 (17.2) | − 2.5** |
| Age group | |||||
| 18–24 years | 184 (18.0) | 0.934 (0.090) | – | 78.7 (14.8) | – |
| 25–44 years | 360 (35.3) | 0.938 (0.069) | − 0.001 | 78.9 (13.7) | − 0.7 |
| 45–64 years | 276 (27.1) | 0.912 (0.082) | − 0.016 | 74.8 (16.1) | − 3.3** |
| 65+ years | 200 (19.6) | 0.819 (0.149) | − 0.092** | 60.0 (19.3) | − 16.7** |
| Education level | |||||
| Secondary or primary | 417 (41.0) | 0.901 (0.121) | – | 73.2 (19.2) | – |
| Higher | 599 (59.0) | 0.911 (0.094) | 0.011 | 74.6 (15.9) | 2.0* |
| Smoking status | |||||
| No | 736 (72.7) | 0.904 (0.108) | – | 73.2 (17.0) | – |
| Yes | 276 (27.3) | 0.914 (0.101) | − 0.007 | 76.2 (18.1) | 0.9 |
| Internet usage | |||||
| Everyday | 785 (77.9) | 0.927 (0.079) | – | 77.1 (14.8) | – |
| Minimum once a week | 81 (8.0) | 0.883 (0.096) | − 0.011 | 66.3 (18.7) | − 5.0** |
| No | 142 (14.1) | 0.811 (0.170) | − 0.059** | 62.4 (22.6) | − 4.3** |
| District | |||||
| North-East | 118 (11.6) | 0.890 (0.107) | – | 72.3 (17.9) | – |
| Central | 69 (6.8) | 0.903 (0.118) | 0.006 | 74.1 (15.5) | 0.7 |
| East | 126 (12.4) | 0.896 (0.106) | 0.005 | 73.5 (19.9) | 0.8 |
| North | 98 (9.6) | 0.912 (0.114) | 0.020 | 75.5 (15.2) | 2.5 |
| North-West | 88 (8.6) | 0.920 (0.087) | 0.029** | 76.0 (16.7) | 2.8 |
| South | 148 (14.5) | 0.903 (0.131) | 0.010 | 72.4 (16.8) | − 0.7 |
| South-East | 116 (11.4) | 0.916 (0.093) | 0.026** | 73.1 (19.0) | 0.3 |
| South-West | 121 (11.9) | 0.913 (0.086) | 0.020 | 75.6 (15.2) | 2.5 |
| West | 116 (11.4) | 0.908 (0.107) | 0.012 | 74.5 (18.7) | 0.9 |
| Zelenograd | 20 (2.0) | 0.940 (0.060) | 0.044* | 78.5 (11.7) | 5.3 |
*p < 0.1; **p < 0.05
Discussion
To the best of our knowledge, this is the first study to estimate population norms for the descriptive part of the EQ-5D-5L questionnaire, EQ VAS, EQ-5D-5L index and Level Sum Score, among a representative sample of Moscow inhabitants. Norms for the EQ-5D-5L index were obtained through the usage of a recently developed Russian EQ-5D-3L value set and EuroQol Group cross-over methodology. Moscow’s normative data may be used as reference values in future EQ-5D-based studies. We have found that HRQoL is worse in women than in men across almost all age groups, especially in the youngest one (18–24 years).
One of the limitations of our study may be the moderate sample size (about 1000 respondents), which is clearly smaller than, for example, that used in a Spanish study (> 20,000 of respondents) [14, 15]. We would like to point out, however, that the sample size should be correlated with the size of the target population. If we estimate the number of respondents per 1 million of the population (about 86 in the case of our study), this indicator is higher than in most of the EQ-5D-5L population norms studies which we identified—in Germany [16–18], Ireland [19], Uruguay [20], South Korea [21], Japan [22], the USA [23] and Indonesia [24].
Although since July 2012 there has existed a new official administrative division of Moscow (two new districts were added), we decided to limit our study to Moscow’s former division into 10 zones. The two new areas have a suburban character, are distant from the city centre (up to 80 km), less populated, have limited access to the metro system, and the health-related quality of life of people living there could be different than for other Muscovites.
Our sample proved to be representative for the Moscow population in terms of sex, age group and the district of residence. However, we based our study on quota sampling, which is a less optimal solution than the random sampling used in other Central and Eastern European studies, such as in Slovenia or Poland (computer selection of respondents based on phone number or personal identification number) [25, 26].
Although accessibility of the Moscow transportation system for the disabled has improved over the last few years, since the Passenger Mobility Centre was opened in 2013, limitations for handicapped people on Moscow transportation systems remains significant, and we were not able to interview any person with a visible disability. According to official statistics, disabled people constitute about 8.5% of the Russian population [27]. One may wonder whether the results of our study would be different if it had taken the form of a postal survey or a direct interview at the respondent’s home.
Our sample was not perfectly balanced in terms of education. Higher education constitutes 42% in Moscow reference data and 59% in our study group, primary education—6.5% and 0.5%, respectively. In general, the level of education of Muscovites seems high compared to other populations. Our sample was additionally skewed in the direction of higher levels of education. This could be a particular limitation in situations in which Moscow population norms will be used to evaluate health care programmes that affect the less-educated set of beneficiaries, for example, citizens of other Russian regions.
A high percentage of respondents (about 22%) refused to answer the question regarding income. As stated previously, refusal to answer among Russian respondents, particularly in Moscow, is frequently of significant proportions, partly due to high levels of distrust towards strangers [28].
There is a long tradition of health surveys carried out among the Moscow population. In the last 3 decades several have taken place: a postal survey in 1991 (n = 545) [29], the Moscow Health Survey in 2004 (n = 1190) [18, 30, 31] or the Stress, Ageing, and Health in Russia (SAHR) study in 2006–2011 (n = 1800) [32, 33]. In the first two of these, health-related quality of life measurement was based on a single-item self-reported measure; in the last one, it was done using the 36-item Short Form Health Survey (SF-36).
We did not identify any population norms survey, neither in Moscow nor Russia, based on the EQ-5D-5L questionnaire. However, in general, studies including EQ-5D are quite numerous, especially those undertaken in disease-specific populations and published in the Russian language. The Russian version of EQ-5D-5L has been successfully validated in a group of 163 patients with spondylarthritis [34]. Recent years have witnessed attempts to carry out EQ-5D-3L valuation [35, 36], which should soon result in the final publication of a country-specific Russian value set [11]. The availability of validated tools should facilitate international comparisons, which up to now have been based mainly on general economic and social indicators [37–39].
The lower health perceptions among Moscow women was noted in the early nineties in a study comparing them with women from Helsinki [19], and subsequently in a comparison with Danish citizens [40] and in the Moscow Health Study [18, 21]. Similar results were found in a study of women from St. Petersburg, Russia’s second-largest city [41]. Self-rated health was much worse in St. Petersburg than in Estonia or Finland. Housewives, in comparison to employed women, had better self-rated health, unlike in the two other areas [32]. Studies indicate that in Russia, although females outlive men and the difference in life expectancy is one of the world’s most significant [42], they generally report worse health [43, 44]. This phenomenon, known as the male–female health-survival paradox [45], is very pronounced in Moscow [31].
One of the potentially interesting results of our study is the evidence of a particularly low HRQoL in young females, as measured with standardised tools. Among women aged 18–24 years, over 60% reported problems with anxiety/depression and over 53% with pain/discomfort. The assessment of health with EQ VAS was 8.3 points lower than in men from the same age group.
Many different factors could lie behind this phenomenon. The Russian sociologist Elena Varshavskaya [46] writes about the NEET group (Not in Employment, Education or Training) among Russian youth. In 2010, Eurostat adopted the standardised definition of NEET and developed a methodology for the statistical calculation of its level. The NEET group includes young people aged 15–24 years who are unemployed or economically inactive, and at the same time do not study and are not covered by vocational training. According to Varshavskaya [46], the proportion of those who do not work or study is about 5% higher among women than among men (15.5 and 10.4%, respectively). Engagement in fulfilling activities, such as education, training, volunteering or work, contributes to future financial independence and is essential for well-being [47].
HRQoL population norms for Moscow, taking into account the size of the city—over 11.8 million inhabitants, constitute a standalone value. Nevertheless, our study may be treated as a pilot project, preceding a nation-wide survey. Given the geographical extent of the country, the implementation of Russia population norms study can be a challenge but should constitute the next logical stage of research. Current Moscow population norms should be re-estimated, when the directly measured EQ-5D-5L, becomes available.
Conclusions
This study presents population norms for the EQ-5D-5L health questionnaire, based on a representative sample of Moscow inhabitants. These reference values, distinguishing age and gender groups, can be used to optimise the effectiveness of resource allocation in healthcare.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Author contributions
Study design: MHV, AT, DG. Data collection and management: MHV, AT. Data analyses: MHV, AT, DG. All authors were involved in the manuscript preparation and all authors read and approved the final manuscript.
Funding
This study has no funding.
Anonymisation of the data
No data were collected that could identify the respondent.
Data availability
The datasets generated during the current study are available from the corresponding author on reasonable request.
Compliance with ethical standards
Conflict of interest
MHV and AT declare no conflict of interest. DG is a member of the EuroQol Group, a non-profit organisation that develops and distributes instruments that assess and value health. The views expressed in the paper are the authors’ own and do not necessarily represent those of the EuroQol Research Foundation.
Ethical approval
The study was approved by the Bioethical Committee of the Medical University of Warsaw, Warsaw, Poland (AKBE/189/17).
Consent to participate
Verbal informed consent was obtained prior to the interview.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Malwina Hołownia-Voloskova, Email: malwina.holownia@gmail.com.
Aleksei Tarbastaev, Email: AG@Tarbastaev.ru.
Dominik Golicki, Email: dominik.golicki@wum.edu.pl.
References
- 1.Rencz F, Gulácsi L, Drummond M, Golicki D, Prevolnik Rupel V, Simon J, Stolk EA, Brodszky V, Baji P, Závada J, Petrova G, Rotar A, Péntek M. EQ-5D in Central and Eastern Europe: 2000–2015. Quality of Life Research. 2016;25:2693–2710. doi: 10.1007/s11136-016-1375-6. [DOI] [PubMed] [Google Scholar]
- 2.Holownia-Voloskova M, Vorobiev PA, Grinin M, Davydovskaya MV, Ermolaeva TN, Kokushkin KA. Drug policy in the Russian Federation. Value in Health Regional Issues. 2018;16:106–111. doi: 10.1016/j.vhri.2018.09.001. [DOI] [PubMed] [Google Scholar]
- 3.Fayers PM, Hays R. Assessing quality of life in clinical trials. Oxford: Oxford University Press; 2005. [Google Scholar]
- 4.EuroQol Research Foundation: EQ-5D is a recommended tool for use in cost-utility analyses around the globe. https://euroqol.org/eq-5d-is-a-recommended-tool-for-use-in-cost-utility-analyses-around-the-globe/ (2019). Accessed 24 March 2020.
- 5.Brooks R. EuroQol: The current state of play. Health Policy. 1996;37:53–72. doi: 10.1016/0168-8510(96)00822-6. [DOI] [PubMed] [Google Scholar]
- 6.Herdman M, Gudex C, Lloyd A, Janssen M, Kind P, Parkin D, Bonsel G, Badia X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L) Quality of Life Research. 2011;20:1727–1736. doi: 10.1007/s11136-011-9903-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Janssen MF, Pickard AS, Golicki D, Gudex C, Niewada M, Scalone L, Swinburn P, Busschbach J. Measurement properties of the EQ-5D-5L compared to the EQ-5D-3L across eight patient groups: A multi-country study. Quality of Life Research. 2013;22:1717–1727. doi: 10.1007/s11136-012-0322-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Szende A, Janssen B, Cabases J, editors. Self-reported population health: An international perspective based on EQ-5D. Dordrecht Heidelberg New York London: Springer Open; 2014. [PubMed] [Google Scholar]
- 9.Deyev AI. How do Muscovites live longer? Uspekhi gerontologii. 2018;31:851–858. [PubMed] [Google Scholar]
- 10.ROSSTAT, Federal State Statistic Service.: Population of the Russian Federation by municipalities as for-1.01.2014. http://www.gks.ru/wps/wcm/connect/rosstat_main/rosstat/ru/statistics/publications/catalog/afc8ea004d56a39ab251f2bafc3a6fce (2014). Accessed 30 June 2019.
- 11.Golicki D, Jakubczyk M, Graczyk K, Niewada M. Valuation of EQ-5D-5L health states in Poland: The first EQ-VT-based study in Central and Eastern Europe. Pharmacoeconomics. 2019;37:1165–1176. doi: 10.1007/s40273-019-00811-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Omelyanovskiy, V., Musina, N. Z., Ratushnyak, S. S., Bezdenezhnyh, T. P., Fediaeva, V. K., Roudijk, B., Purba, F. D. (2020). Preliminary results of the EQ-5D-3L valuation study in Russia. 4th EuroQol Academy Meeting, Prague, Czech Republic, 2–4 March.
- 13.van Hout B, Janssen MF, Feng YS, Kohlmann T, Busschbach J, Golicki D, Lloyd A, Scalone L, Kind P, Pickard AS. Interim scoring for the EQ-5D-5L: Mapping the EQ-5D-5L to EQ-5D-3L value sets. Value in Health. 2012;15:708–715. doi: 10.1016/j.jval.2012.02.008. [DOI] [PubMed] [Google Scholar]
- 14.Garcia-Gordillo MA, Adsuar JC, Olivares PR. Normative values of EQ-5D-5L: In a Spanish representative population sample from Spanish Health Survey, 2011. Quality of Life Research. 2016;25:1313–1321. doi: 10.1007/s11136-015-1164-7. [DOI] [PubMed] [Google Scholar]
- 15.Hernandez G, Garin O, Pardo Y, Vilagut G, Pont A, Suarez M, Neira M, Rajmil L, Gorostiza I, Ramallo-Farina Y, Cabases J, Alonso J, Ferrer M. Validity of the EQ-5D-5L and reference norms for the Spanish population. Quality of Life Research. 2018;27:2337–2348. doi: 10.1007/s11136-018-1877-5. [DOI] [PubMed] [Google Scholar]
- 16.Hinz A, Kohlmann T, Stobel-Richter Y, Zenger M, Brahler E. The quality of life questionnaire EQ-5D-5L: Psychometric properties and normative values for the general German population. Quality of Life Research. 2014;23:443–447. doi: 10.1007/s11136-013-0498-2. [DOI] [PubMed] [Google Scholar]
- 17.Huber MB, Felix J, Vogelmann M, Leidl R. Health-related quality of life of the general German population in 2015: Results from the EQ-5D-5L. International Journal of Environmental Research and Public Health. 2017;14:426. doi: 10.3390/ijerph14040426. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Grochtdreis T, Dams J, Konig HH, Konnopka A. Health-related quality of life measured with the EQ-5D-5L: Estimation of normative index values based on a representative German population sample and value set. The European Journal of Health Economics. 2019;20:933–944. doi: 10.1007/s10198-019-01054-1. [DOI] [PubMed] [Google Scholar]
- 19.Hobbins A, Barry L, Kelleher D, O’Neill C. The health of the residents of Ireland: Population norms for Ireland based on the EQ-5D-5L descriptive system—a cross sectional study. HRB Open Research. 2018;1:22. doi: 10.12688/hrbopenres.12848.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Augustovski F, Rey-Ares L, Irazola V, Garay OU, Gianneo O, Fernandez G, Morales M, Gibbons L, Ramos-Goni JM. An EQ-5D-5L value set based on Uruguayan population preferences. Quality of Life Research. 2016;25:323–333. doi: 10.1007/s11136-015-1086-4. [DOI] [PubMed] [Google Scholar]
- 21.Kim TH, Jo MW, Lee S, Kim SH, Chung SM. Psychometric properties of the EQ-5D-5L in the general population of South Korea. Quality of Life Research. 2013;22:2245–2253. doi: 10.1007/s11136-012-0331-3. [DOI] [PubMed] [Google Scholar]
- 22.Shiroiwa T, Fukuda T, Ikeda S, Igarashi A, Noto S, Saito S, Shimozuma K. Japanese population norms for preference-based measures: EQ-5D-3L, EQ-5D-5L, and SF-6D. Quality of Life Research. 2016;25:707–719. doi: 10.1007/s11136-015-1108-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Craig BM, Pickard AS, Lubetkin EI. Health problems are more common, but less severe when measured using newer EQ-5D versions. Journal of Clinical Epidemiology. 2014;67:93–99. doi: 10.1016/j.jclinepi.2013.07.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Purba FD, Hunfeld JAM, Iskandarsyah A, Fitriana TS, Sadarjoen SS, Passchier J, Busschbach JJV. Quality of life of the Indonesian general population: Test-retest reliability and population norms of the EQ-5D-5L and WHOQOL-BREF. PLoS One. 2018;13(5):e0197098. doi: 10.1371/journal.pone.0197098. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Klemenc-Ketis Z, Smogavec M, Softic N, Kersnik J. Health-related quality of life: A population based study from Slovenia. Central European Journal of Public Health. 2011;19:7–12. doi: 10.21101/cejph.a3636. [DOI] [PubMed] [Google Scholar]
- 26.Golicki D, Niewada M. EQ-5D-5L Polish population norms. Archives of Medical Science. 2017;13:191–200. doi: 10.5114/aoms.2015.52126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Data of Federal Statistic Bureau of Russian Federation. http://www.gks.ru/wps/wcm/connect/rosstat_main/rosstat/ru/statistics/population/disabilities/#. Accessed 30 June 2019.
- 28.Vågerö D, Kislitsyna O, Ferlander S, Migranova L, Carlson P, Rimachevskaya N. Moscow Health Survey 2004—Social surveying under difficult circumstances. International Journal of Public Health. 2008;53:171–179. doi: 10.1007/s00038-008-7052-y. [DOI] [PubMed] [Google Scholar]
- 29.Palosuo H, Uutela A, Zhuravleva I, Lakomova N. Social patterning of ill health in Helsinki and Moscow: Results from a comparative survey in 1991. Social Science and Medicine. 1998;46:1121–1136. doi: 10.1016/s0277-9536(97)10043-0. [DOI] [PubMed] [Google Scholar]
- 30.Ferlander S, Mäkinen IH. Social capital, gender and self-rated health. Evidence from the Moscow Health Survey 2004. Social Science & Medicine. 2009;69:1323–1332. doi: 10.1016/j.socscimed.2009.08.009. [DOI] [PubMed] [Google Scholar]
- 31.Ferlander S, Stickley A, Kislitsyna O, Jukkala T, Carlson P, Mäkinen IH. Social capital—A mixed blessing for women? A cross-sectional study of different forms of social relations and self-rated depression in Moscow. BMC Psychology. 2016;4:37. doi: 10.1186/s40359-016-0144-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Shkolnikova M, Shalnova S, Shkolnikov VM, Metelskaya V, Deev A, Andreev E, Jdanov D, Vaupel JW. Biological mechanisms of disease and death in Moscow: Rationale and design of the survey on Stress Aging and Health in Russia (SAHR) BMC Public Health. 2009;9:293. doi: 10.1186/1471-2458-9-293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Oksuzyan A, Shkolnikova M, Vaupel JW, Christensen K, Shkolnikov VM. Sex differences in biological markers of health in the study of stress, aging and health in Russia. PLoS One. 2015;10:e0131691. doi: 10.1371/journal.pone.0131691. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Akulova AI, Gaydukova IZ, Rebrov AP. Validation of the EQ-5D-5L version in Russia. Nauchno-Prakticheskaya Revmatologiya. 2018;56:351–355. [Google Scholar]
- 35.Kind P, Gerry C. From Russia with love—Valuation of EQ-5D health states using available data. Value in Health. 2017;20:A59. [Google Scholar]
- 36.Khabibullina A, Gerry CJ. Valuing health states in Russia: A first feasibility study. Value in Health Regional Issues. 2019;19:75–80. doi: 10.1016/j.vhri.2019.01.005. [DOI] [PubMed] [Google Scholar]
- 37.Liu Y, Rao K, Fei J. Economic transition and health transition: Comparing China and Russia. Health Policy. 1998;44:103–122. doi: 10.1016/s0168-8510(98)00010-4. [DOI] [PubMed] [Google Scholar]
- 38.Jogerst GJ, Daly JM, Hesli V, Saha C. Comparison of health and effective functioning in Russia and the United States. Clinical Interventions in Aging. 2006;1:189–196. doi: 10.2147/ciia.2006.1.2.189. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Hsieh N. Economic security, social cohesion, and depression disparities in post-transition societies: A comparison of older adults in China and Russia. Journal of Health and Social Behavior. 2015;56:534–551. doi: 10.1177/0022146515611731. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Oksuzyan A, Shkolnikova M, Vaupel JW, Christensen K, Shkolnikov VM. Sex differences in health and mortality in Moscow and Denmark. European Journal of Epidemiology. 2014;29:243–252. doi: 10.1007/s10654-014-9893-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Dubikaytis T, Härkänen T, Regushevskaya E, Hemminki E, Haavio-Mannila E, Laanpere M, Kuznetsova O, Koskinen S. Socioeconomic differences in self-rated health among women: A comparison of St. Petersburg to Estonia and Finland. International Journal for Equity in Health. 2014;13:39. doi: 10.1186/1475-9276-13-39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Field M. Gender gaps in mortality. Dissimilarities in mortality rates: Analysis of standard data. In: Shkolnikov V, Andreev E, Maleva T, editors. Inequality and mortality in Russia. Moscow: Moscow Carnegie Center; 2000. pp. 20–23. [Google Scholar]
- 43.Rose R. How much does social capital add to individual health? A survey study of Russians. Social Science and Medicine. 2000;51:1421–1435. doi: 10.1016/s0277-9536(00)00106-4. [DOI] [PubMed] [Google Scholar]
- 44.Gordeev VS, Goryakin Y, McKee M, Stuckler D, Roberts B. Economic shocks and health resilience: Lessons from the Russian Federation. Journal of Public Health. 2016;38:e409–e418. doi: 10.1093/pubmed/fdv166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Nathanson CA. Illness and the feminine role: A theoretical review. Social Science and Medicine. 1975;9:57–62. doi: 10.1016/0037-7856(75)90094-3. [DOI] [PubMed] [Google Scholar]
- 46.Varshavskaya EA. Rossiyskaya NEET-molodezh': kharakteristiki i tipologiya. Sotsiologicheskiye issledovaniya. 2016;9:31–39. [Google Scholar]
- 47.Office for National Statistics.: Young people’s well-being. https://www.ons.gov.uk/peoplepopulationandcommunity/wellbeing/articles/youngpeopleswellbeingandpersonalfinance/2017 (2017). Accessed 30 May 2020.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
No data were collected that could identify the respondent.
The datasets generated during the current study are available from the corresponding author on reasonable request.