

Abstract
Complete radial tears of the meniscus render the entirety of the meniscus functionally incompetent (known as an ameniscal state); therefore, attempts at repair are essential. Although various techniques have been described, repair failures continue to frequently occur, especially with the medial meniscus. Inside-out repair and anchoring of the preserved meniscus to both the capsule and tibia may offer the advantage of a more robust repair. The objective of this Technical Note is to describe a method of repair for complete radial tears of the medial meniscus using a combination of inside-out sutures and secondary reinforcement to the tibia using all-suture knotless anchors.
Technique Video
A step-by-step video illustration describing a method of medial meniscus radial tear repair using a combination of inside-out sutures and secondary reinforcement to the tibia using all-suture knotless anchors.
The critical role of the meniscus and the consequences of subtotal meniscectomy have been well documented in recent years.1, 2, 3 Loss of the circumferential hoop fibers of the meniscus can occur through either damage to a meniscal root attachment or with a radial split tear of the meniscus. Both of these injuries lead to compartment pressures similar to that of a total meniscectomy.1, 2, 3 Due to the significant repercussions of a nonfunctional meniscus, such as persistent pain and rapid progression of arthritis, research has focused on new techniques for meniscal repair and preservation.4,5 Meniscal root repairs have gained traction due to new adoption of technology and the ability to restore the hoop stress to the native meniscus. As opposed to meniscectomy, these techniques have led to lower rates of arthritis and higher functional scores.4, 5, 6 Although meniscal root repairs have increased in popularity, the repair of a radial split tear in the body of the meniscus remains controversial.
Radial split tears in the body of the medial and lateral menisci represent significant injuries due to the inherent loss of meniscal function. This is caused by complete disruption of the circumferential hoop fibers, which renders an ameniscal state. Because of the poor vascularity in the medial and lateral region of the meniscus, traditional repair methods with all-inside or inside-out techniques have had a low rate of healing.7 Recent techniques have sought to augment traditional repairs by adding additional fixation at the tear site.8,9 LaPrade et al.6 described transosseous fixation with tibial bone tunnels entering at the undersurface of the meniscus tear. While this fixation is robust, it is technically demanding, and risks damage to the articular surface of the tibial plateau. A less well-described technique for augmenting radial split meniscus tears is to add suture anchor fixation along the peripheral edge of the tibial plateau. This, in theory, anchors the meniscus to the peripheral edge of the tibial plateau and restores the meniscotibial ligaments, thereby reinforcing the repair construct and decreasing the risk of meniscal extrusion. This technique is less technically demanding and highly reproducible.
In this report, we describe an innovative surgical technique for repair of a compete medial meniscus tear in the middle third. After traditional sutures are passed in an inside-out fashion, 2 knotless, all-suture, self-tensioning suture anchors are placed along the medial tibial plateau at the junction of the articular cartilage and secured with the vertical suturing into the red-red zone of the meniscus on both sides of the radial tear. These suture anchors act to reinforce the meniscal repair and prevent meniscal extrusion. This technique can be directly applied to complex radial split tears of the medial and lateral menisci, in which traditional fixation methods are insufficient.
Technique
Preoperative Planning
In cases of meniscus pathology, the authors obtain standard knee radiographs, including long-leg standing alignment films in addition to magnetic resonance imaging, before surgical management. Any significant alignment abnormalities, chondral lesions, and ligamentous injuries are addressed in a single stage to provide an optimal biomechanical milieu for meniscus repair.
In the case presented in Video 1, the patient is an active man who had an acute injury to his medial meniscus that resulted in a full-thickness midbody tear. The remainder of his medial cartilaginous surfaces were demonstrated to be intact by 3 Tesla magnetic resonance imaging. He was indicated for a medial meniscus repair using an outside-in technique in addition to anchoring to the tibia by means of all-suture anchors.
Diagnostic Arthroscopy
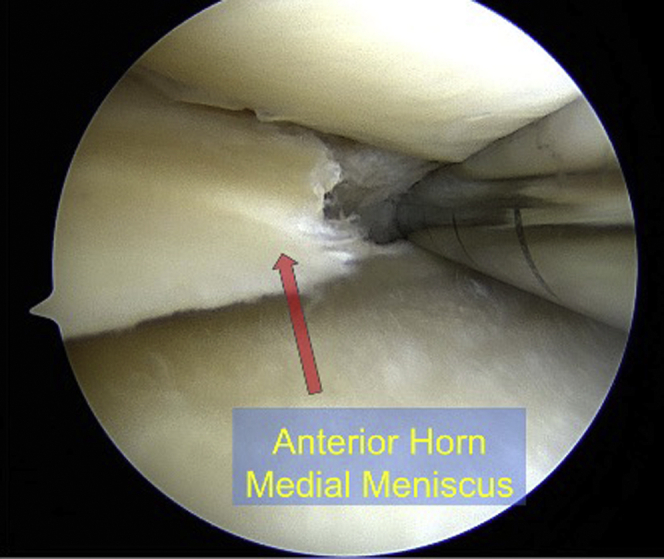
The procedure begins with a complete diagnostic arthroscopy using a 30-degree arthroscope. In the present case, a full-thickness radial tear of the medial meniscus is visualized (Fig 1). An arthroscopic torpedo shaver (Arthrex, Naples, FL, U.S.A.) is used to debride the meniscus tear edges back to a healthy, stable rim (Fig 2). For improved access to the medial meniscus, an 18-gauge spinal needle is used to lightly “piecrust” the medial collateral ligament under valgus stress.
Fig 1.

A 30-degree arthroscopic image of a right knee while viewing through an anteromedial portal demonstrating the full-thickness radial tear evaluated with probing.
Fig 2.
A 30-degree arthroscopic image of a right knee while viewing through an anteromedial portal demonstrating an arthroscopic torpedo shaver (Arthrex, Naples, FL, U.S.A.) used to debride the meniscus tear edges back to a healthy, stable rim.
Meniscus Repair
Following diagnostic arthroscopy and debridement, an open approach to the joint capsule is used. A 3-cm incision distal to the medial epicondyle to the anteromedial tibia is sharply made. Dissection is carried down to the sartorial fascia, which is incised in line with the skin incision with care to avoid injury to the saphenous nerve or the underlying pes anserine tendons. The interval between the medial head of the gastrocnemius tendon and the semimembranosus is developed bluntly, which is layer 2 of the medial side of the knee. A Henning retractor is then placed for safe deflection of the inside-out meniscus repair needles.
Next, the arthroscope is placed in the anteromedial portal while the inside-out needle Meniscal Zone Navigator (Arthrex) is placed through the anterolateral portal (Fig 3). First, 2 vertical mattress sutures using No. 0 fiberwire nonabsorbable suture are passed, with one on each leaflet of the tear approximately 2 to 3 mm from the tear edge to serve as rip-stops for bridging sutures across the tear (Fig 4). These sutures are then tied extracapsularly with the knee in 90 degrees of flexion.
Fig 3.

A 30-degree arthroscopic image of a right knee while viewing through an anteromedial portal demonstrating the inside-out needle Meniscal Zone Navigator (Arthrex, Naples, FL, U.S.A.) placed through the anterolateral portal. Sutures were then passed from outside in on either side of the radial tear.
Fig 4.

A 30-degree arthroscopic image of a right knee while viewing through an anteromedial portal demonstrating 2 vertical mattress sutures using No. 0 fiberwire nonabsorbable suture, each passed with one on each leaflet of the tear approximately 2 to 3 mm from the tear edge to serve as rip stops for bridging sutures across the tear.
Next, the first of 2 bridging sutures is passed across the tear and tied (Fig 5). Two oblique mattress inside-out sutures are then passed on each side of the tear. These are not tied but are instead left in place to later be used as a shuttling sutures to pass the 1.5-mm meniscal suture tape from each of the 2 tibial all-suture anchors.
Fig 5.

A 30-degree arthroscopic image of a right knee while viewing through an anteromedial portal demonstrating the ripstop configuration was used where one suture was placed on either end of the tear and then oblique mattress-style sutures are placed on either side of the rip stop. After these 14 inside-out meniscal sutures were tied, 2 additional sutures were placed inside out and passed obliquely, one on the anterior portion of the meniscus and the other on the posterior side for use as shuttling sutures.
Through the same open incision for the inside-out repair, two 2.6-mm all-suture knotless FiberTAK anchors (Arthrex) (Fig 6) are placed on the superior tibia at positions both anteriorly and posteriorly, corresponding to both sides of the radial tear (Table 1). The previously passed oblique mattress sutures passed in an inside-out fashion are used to shuttle the suture tape from the anchor through the meniscus (Table 1). Once the suture tape from each anchor is passed through the meniscus, the anchor shuttling stitch is used to pass the suture tape back through the knotless mechanism in the anchor (Fig 7). Finally, with the knee in slight flexion, the suture tape is cinched to reapproximate and anchor the meniscus periphery to the proximal tibia.
Fig 6.

A 2.6-mm all-suture knotless FiberTAK anchor loaded with suture tape.
Table 1.
Pearls and Pitfalls of Full-Thickness Radial Medial Meniscus Tear Fixation With Inside-Out Technique With Tibial Knotless Suture Anchors
| Pearls | Pitfalls |
|---|---|
| In young and active patients with an overall healthy meniscus, in the setting of an acute radial tear, a side-to-side repair of the radial tear should be attempted. | Avoid overtensioning of the sutures to the anchors in order to facilitate normal meniscal translation. |
| The combination of an oblique mattress configuration and ripstop method allows a stronger construct. | Not appropriately preparing the meniscus may impede its healing. |
| Marrow venting is a useful adjuvant to enhance biology and facilitate healing. | Tension inside-out sutures at 90° of knee flexion to avoid overconstraint. |
| An adequate number of sutures are required for a solid repair. | The knotless anchor suture is passed in vertical configuration in the red-red zone of the meniscus and brought out to the edge of the capsule at the tibial rim to avoid overconstraint. |
| Knotless suture anchors enable ability to dial in tension. | Ensure the suture anchors are inserted right at the meniscus-capsule junction and avoid the tibia cartilage. |
Fig 7.

Image of the open surgical procedure on the medial aspect of a right knee demonstrating suture shuttling from the proximal medial tibia. After shuttling sutures were placed from inside out, the anterior and posterior aspects of the tibia were then identified and two 2.9-mm Knotless FiberTaks (Arthrex, Naples, FL, U.S.A.) were placed. The shuttling sutures were then used to shuttle the sutures through the meniscus in an oblique mattress fashion, and the knotless mechanism was used to affix the sutures down to the inferior tibia to re-create the meniscal tibial attachment.
The arthroscope is then reinserted into the joint to reveal a repaired, stable meniscus (Fig 8). Finally, for optimization of the physiologic environment to aid in healing, marrow venting of the notch is performed (Table 1). Then, 8 cc of platelet-rich plasma, which had been drawn preoperatively, is injected outside in with a 22-guage needle targeting the red-red and red-white zone of the meniscus.
Fig 8.

A 30-degree arthroscopic image of a right knee while viewing through an anteromedial portal demonstrating the final construct after the 14 meniscal sutures were tied and the meniscus was repaired to the tibia with the use of 2 suture anchors.
Rehabilitation
Postoperatively, the patient is placed into a hinged knee brace locked in extension for ambulation and made 20 lb weightbearing. Knee range of motion is restricted to 0 to 90 degrees for 6 weeks. Isometric quadriceps strengthening is initiated on postoperative day 1. After 6 weeks, range of motion and strengthening are progressed to full.
Discussion
This article demonstrates a reproducible technique for augmenting traditional inside-out meniscal repairs. This technique has the advantage of being reproducible with minimal added morbidity to the patient and provides robust fixation at an area traditionally considered difficult to repair. This technique anchors the meniscus to the tibial plateau and may prevent normal meniscal translation on the tibial plateau. However, because of the relatively small amount of normal movement of the medial meniscus relative to the lateral meniscus, this technique is particularly favorable in radial tears of the medial meniscus.
LaPrade et al.6,10 described transosseous fixation of radial split tears of the medial meniscus and reported favorable outcomes with low revision rates. However, this technique is challenging and risks penetration of the articular surface if the guide pin is not placed perfectly. In this technique, an open incision is already used. This minimizes any added patient morbidity or surgical time. It also allows for a reproducible and reliable method of fixation because of the open exposure. It remains to be seen whether anchoring the meniscus at sites other than the meniscal roots has long-term negative consequences on joint health. However, it is our opinion that preserving the meniscal tissue and hoop stress is of far higher importance than ensuring normal meniscal mobility. Future studies are needed to better understand these concepts.
This technique is not without limitations. Given the inside-out nature of the technique, a skilled assistant is required, which may not be available under all circumstances. A second limitation includes the use of a small, all-suture anchor in the proximal tibia, which has the potential for loss of fixation in the thin cortical and osteoporotic bone potentially encountered in older individuals.
In conclusion, we present an innovative technique to augment inside-out meniscal repairs with self-tensioning suture anchors placed along the peripheral tibial plateau. This technique is reproducible and allows for robust fixation. This information can be directly used in the repair of radial split tears of the midbody of the medial or lateral meniscus.
Footnotes
The authors report that they have no conflicts of interest in the authorship and publication of this article. Full ICMJE author disclosure forms are available for this article online, as supplementary material.
Supplementary Data
A step-by-step video illustration describing a method of medial meniscus radial tear repair using a combination of inside-out sutures and secondary reinforcement to the tibia using all-suture knotless anchors.
References
- 1.Allaire R., Muriuki M., Gilbertson L., Harner C.D. Biomechanical consequences of a tear of the posterior root of the medial meniscus: Similar to total meniscectomy. J Bone Joint Surg Am. 2008;90(9):1922–1931. doi: 10.2106/JBJS.G.00748. [DOI] [PubMed] [Google Scholar]
- 2.Padalecki J.R., Jansson K.S., Smith S.D. Biomechanical consequences of a complete radial tear adjacent to the medial meniscus posterior root attachment site in situ pull-out repair restores derangement of joint mechanics. Am J Sports Med. 2013;42(3):699–707. doi: 10.1177/0363546513499314. [DOI] [PubMed] [Google Scholar]
- 3.Tachibana Y., Mae T., Fujie H. Effect of radial meniscal tear on in situ forces of meniscus and tibiofemoral relationship. Knee Surg Sport Traumatol Arthrosc. 2017;25(2):355–361. doi: 10.1007/s00167-016-4395-4. [DOI] [PubMed] [Google Scholar]
- 4.Faucett S.C., Geisler B.P., Chahla J. Meniscus root repair vs meniscectomy or nonoperative management to prevent knee osteoarthritis after medial meniscus root tears: Clinical and economic effectiveness. Am J Sports Med. 2019;47(3):762–769. doi: 10.1177/0363546518755754. [DOI] [PubMed] [Google Scholar]
- 5.Bernard C.D., Kennedy N.I., Tagliero A.J. Medial meniscus posterior root tear treatment: A matched cohort comparison of nonoperative management, partial meniscectomy, and repair. Am J Sports Med. 2020;48(1):128–132. doi: 10.1177/0363546519888212. [DOI] [PubMed] [Google Scholar]
- 6.LaPrade R.F., Matheny L.M., Moulton S.G., James E.W., Dean C.S. Posterior meniscal root repairs: Outcomes of an anatomic transtibial pull-out technique. Am J Sports Med. 2017;45(4):884–891. doi: 10.1177/0363546516673996. [DOI] [PubMed] [Google Scholar]
- 7.Tsujii A., Amano H., Tanaka Y. Second look arthroscopic evaluation of repaired radial/oblique tears of the midbody of the lateral meniscus in stable knees. J Orthop Sci. 2018;23(1):122–126. doi: 10.1016/j.jos.2017.09.023. [DOI] [PubMed] [Google Scholar]
- 8.Bhatia S., Civitarese D.M., Turnbull T.L. A novel repair method for radial tears of the medial meniscus. Am J Sports Med. 2016;44(3):639–645. doi: 10.1177/0363546515615565. [DOI] [PubMed] [Google Scholar]
- 9.Moulton S.G., Bhatia S., Civitarese D.M., Frank R.M., Dean C.S., LaPrade R.F. Surgical techniques and outcomes of repairing meniscal radial tears: A systematic review. Arthroscopy. 2016;32(9):1919–1925. doi: 10.1016/j.arthro.2016.03.029. [DOI] [PubMed] [Google Scholar]
- 10.Cinque M.E., Geeslin A.G., Chahla J., Dornan G.J., Laprade R.F. Two-tunnel transtibial repair of radial meniscus tears produces comparable results to inside-out repair of vertical meniscus tears. Am J Sports Med. 2017;45(10):2253–2259. doi: 10.1177/0363546517704425. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
A step-by-step video illustration describing a method of medial meniscus radial tear repair using a combination of inside-out sutures and secondary reinforcement to the tibia using all-suture knotless anchors.
A step-by-step video illustration describing a method of medial meniscus radial tear repair using a combination of inside-out sutures and secondary reinforcement to the tibia using all-suture knotless anchors.