

This cohort study investigates the mortality and functional outcomes of individuals who received a prehospital dose of tranexamic acid for suspected severe traumatic brain injury.
Key Points
Question
Is there an association between prehospital tranexamic acid administration and outcomes after severe traumatic brain injury (TBI)?
Findings
In this multicenter cohort study of 1827 patients, prehospital administration of tranexamic acid was associated with a statistically significant increase in the odds of mortality in patients with isolated severe TBI. No evidence of an association was observed in the overall cohort, including in patients with combined intracranial and extracranial injuries.
Meaning
Results of this study suggest that prehospital administration of tranexamic acid could lead to increased mortality in patients with isolated severe TBI.
Abstract
Importance
The development and expansion of intracranial hematoma are associated with adverse outcomes. Use of tranexamic acid might limit intracranial hematoma formation, but its association with outcomes of severe traumatic brain injury (TBI) is unclear.
Objective
To assess whether prehospital administration of tranexamic acid is associated with mortality and functional outcomes in a group of patients with severe TBI.
Design, Setting, and Participants
This multicenter cohort study is an analysis of prospectively collected observational data from the Brain Injury: Prehospital Registry of Outcome, Treatments and Epidemiology of Cerebral Trauma (BRAIN-PROTECT) study in the Netherlands. Patients treated for suspected severe TBI by the Dutch Helicopter Emergency Medical Services between February 2012 and December 2017 were included. Patients were followed up for 1 year after inclusion. Data were analyzed from January 10, 2020, to September 10, 2020.
Exposures
Administration of tranexamic acid during prehospital treatment.
Main Outcomes and Measures
The primary outcome was 30-day mortality. Secondary outcomes included mortality at 1 year, functional neurological recovery at discharge (measured by Glasgow Outcome Scale), and length of hospital stay. Data were also collected on demographic factors, preinjury medical condition, injury characteristics, operational characteristics, and prehospital vital parameters.
Results
A total of 1827 patients were analyzed, of whom 1283 (70%) were male individuals and the median (interquartile range) age was 45 (23-65) years. In the unadjusted analysis, higher 30-day mortality was observed in patients who received prehospital tranexamic acid (odds ratio [OR], 1.34; 95% CI, 1.16-1.55; P < .001), compared with patients who did not receive prehospital tranexamic acid. After adjustment for confounders, no association between prehospital administration of tranexamic acid and mortality was found across the entire cohort of patients. However, a substantial increase in the odds of 30-day mortality persisted in patients with severe isolated TBI who received prehospital tranexamic acid (OR, 4.49; 95% CI, 1.57-12.87; P = .005) and after multiple imputations (OR, 2.05; 95% CI, 1.22-3.45; P = .007).
Conclusions and Relevance
This study found that prehospital tranexamic acid administration was associated with increased mortality in patients with isolated severe TBI, suggesting the judicious use of the drug when no evidence for extracranial hemorrhage is present.
Introduction
Severe traumatic brain injury (TBI) is a leading cause of trauma-related mortality and disability worldwide,1 affecting about 5.5 million people annually.2 Severe TBI is commonly associated with the development of intracranial hemorrhage. The occurrence of bleeding by itself and the volume of blood are associated with mortality and poor outcomes.3 Thus, interventions associated with decreased bleeding could potentially reduce mortality and morbidity.
In this context, tranexamic acid has been shown to decrease mortality in injured patients with severe hemorrhage,4 and so it has become the standard of care in many emergency medical systems. The advantages of tranexamic acid in trauma patients mainly seem to derive from prevention of exsanguination.5 However, exsanguination is usually not a primary concern in TBI, particularly not in isolated TBI, and the association of tranexamic acid administration with TBI outcomes remains unclear. Recently, the CRASH-3 (Effects of Tranexamic Acid on Death, Disability, Vascular Occlusive Events and Other Morbidities in Patients With Acute Traumatic Brain Injury) randomized placebo-controlled trial did not find a statistically significant effect of tranexamic acid on mortality either in the overall study population of patients with all TBI severities or in the subgroup of patients with severe TBI.6 Treatment was initiated in the hospital, and it is possible that no advantage was observed in patients with severe TBI because they may have already developed major intracranial hemorrhage before the treatment was initiated.6 Rowell et al7 recently reported the results of a randomized clinical trial of the prehospital administration of tranexamic acid; they found no evidence of the effects on neurological outcome or mortality. The trial by Rowell et al7 included patients with moderate and severe TBI as well as patients with and without extracranial injuries. Neither of these trials,6,7 therefore, can definitively confirm the absence of advantages or harms in prehospital tranexamic acid administration in patients with severe (isolated) TBI. In this cohort study, we aimed to assess whether prehospital administration of tranexamic acid is associated with mortality and functional outcomes in a group of patients with severe TBI.
Methods
The medical research ethics boards of the Amsterdam University Medical Center and Erasmus MC Rotterdam reviewed the study protocol and concluded that the research did not fall under the Dutch Medical Research Involving Human Subjects Act; hence, study approval and informed consent were waived. We followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline.8
In this cohort study, we performed a retrospective analysis of prospectively collected observational data from the database of the Brain Injury: Prehospital Registry of Outcome, Treatments and Epidemiology of Cerebral Trauma (BRAIN-PROTECT) study. A detailed protocol of the study has been published previously.9 Briefly, BRAIN-PROTECT is a multicenter observational study of the prehospital treatment of patients with severe TBI in the Netherlands. It included patients with suspected severe TBI (based on a trauma mechanism or clinical findings suggestive of severe TBI and a prehospital Glasgow Coma Scale [GCS] score of 8 or lower) who were treated by 1 of the 4 Dutch physician-staffed Helicopter Emergency Medical Services (HEMS)10 from February 2012 through December 2017. Inclusion was based on suspected rather than confirmed TBI because prehospital treatment, including administration of tranexamic acid, is typically based on clinical suspicion rather than on definitive diagnosis. Given that prehospital treatment recommendations are vague and based on low-quality evidence, a marked heterogeneity exists in the prehospital treatment of patients with severe TBI.9 This heterogeneity allows for investigation of the association of different treatments with outcomes while adjusting for confounders. In 9 participating trauma centers (8 level I trauma centers and 1 level II trauma center with neurosurgery facilities), patients were followed up, and in-hospital and outcome data were collected up to 1 year after inclusion (up to December 2018).
We excluded patients from the BRAIN-PROTECT database who were not transported to a participating trauma center (no follow-up data were available) and patients who were undergoing prehospital traumatic cardiopulmonary resuscitation (inherently very high mortality, regardless of treatment). All other patients were included in the present analysis.
Prehospital data were collected on the basis of the Utstein template for uniform reporting of data after major trauma,11 and these data included patient and trauma characteristics, injuries, vital parameters, as well as prehospital treatments and interventions as described previously.9 The collected outcome data included mortality at 30 days (primary outcome) and at 1 year as well as functional neurological outcome (Glasgow Outcome Scale [GOS]; score range: 1-5, with the highest score indicating good recovery with at most minor neurological or psychological deficits) at discharge, and length of hospital stay (secondary outcomes).
Statistical Analysis
The targeted sample size was 2500 patients from the overall BRAIN-PROTECT database.9 Published a priori calculations have shown that subanalyses of the data set (as presented in this study) with a sample size of 2000 patients provide 80% power to detect an absolute 5.6% mortality reduction, with α = .05; similarly, a sample size of 1500 patients has 80% power to detect a 6.4% decrease in mortality, and a sample of 1000 patients has 80% power to detect a 7.8% decrease in mortality.9
Data were analyzed from January 10, 2020, to September 10, 2020, using Stata, version 16.1 (StataCorp LLC), and all hypothesis tests were 2-sided. The distribution of continuous data was assessed with quantile-quantile plots, histograms, and Shapiro-Wilk tests. Data are presented here as mean (SD), median (interquartile range [IQR]), or numbers (percentages) as appropriate.12 Crude differences between patients who received and those who did not receive tranexamic acid in the prehospital setting were explored with 2-sample, unpaired, 2-tailed t tests, Mann-Whitney tests, and χ2 tests.
The association between tranexamic acid and mortality at 30 days was examined using logistic regression.13 In all of the regression modeling performed, the SEs were adjusted for 9 participating trauma centers to account for potential nonindependence of patients treated in the same hospital.14
After unadjusted logistic regression analyses, a multivariable model was built to account for potential confounders, including confounding by indication.15,16 Control variables were all simultaneously added to the model according to theoretical considerations and previous literature17 and included demographic factors (ie, age and sex), preinjury medical condition and medications (ie, American Society of Anesthesiologists Physical Status Classification System score and use of anticoagulant drugs), injury characteristics and severity (ie, trauma mechanism, Injury Severity Score [score range: 1-75, with the highest score indicating critical injury in at least 3 body regions or any unsurvivable injury], and initial GCS score [score range: 3-15, with the highest score indicating that the patient opens the eyes spontaneously, is oriented, and obeys commands]), operational characteristics (ie, involved HEMS provider and distance from the accident scene to the trauma center), and first recorded vital parameters at arrival of HEMS (ie, systolic blood pressure, heart rate, and oxygen saturation as measured by pulse oximetry). Numerical independent variables were modeled using restricted cubic splines to relax the assumption of a linear association between the variable and the logit of mortality. Calibration was assessed with a Hosmer-Lemeshow test, and discrimination was quantified by the area under the receiver operating characteristic curve.18 To address bias and loss of power attributed to listwise deletion in the regression analyses, we also analyzed the data after multiple imputations of missing values.19 Twenty data sets were imputed using chained equations with an imputation model that included the outcome variables, all independent variables in the analysis models, and auxiliary variables.
For planned subgroup analyses, patients were stratified into confirmed severe TBI and isolated severe TBI cohorts. Patients were characterized as having confirmed TBI if the Head Abbreviated Injury Score (AIS) was 3 or higher. Isolated TBI was characterized as a Head AIS of 3 or higher, with neck, spine, thorax, abdomen, extremities, and external AIS of 2 or lower. Because the hypotheses on the association between tranexamic acid and mortality were thus tested in 3 groups of patients (full cohort, confirmed severe TBI cohort, and isolated severe TBI cohort), a Bonferroni-corrected significance threshold of 0.05/3 = 0.017 was used to protect the type I error rate.20
As a planned sensitivity analysis, the actual survival time was analyzed using a Cox proportional hazards regression model.21 A total of 16 additional post hoc sensitivity analyses were performed, as described in eTable 6 in Supplement 1.
Secondary outcomes were analyzed using logistic regression (mortality at 1 year), ordinal logistic regression (GOS score at discharge), and zero-truncated negative binomial regression (hospital length of stay in patients who survived until discharge) adjusted for all control variables. For secondary outcomes and sensitivity analyses, a 2-sided P < .05 was considered statistically significant.
Results
The BRAIN-PROTECT data set included 2589 patients, of whom 2117 (82%) were transported to participating trauma centers. After exclusion of 290 patients with prehospital cardiopulmonary resuscitation, 1827 patients (71%) were deemed eligible for analysis (eFigure in Supplement 1). Of these patients, 1283 (70%) were male and 541 (30%) were female individuals with a median (IQR) age of 45 (23-65) years. The confirmed TBI cohort comprised 1375 patients, and 719 patients composed the isolated TBI cohort. Demographic and injury data are shown in Table 1 and eTables 1 and 2 in Supplement 1.
Table 1. Characteristics of Patients With and Without Tranexamic Acid Exposure.
| Characteristic | No. (%)a | P value | Missing, No. (%) | ||
|---|---|---|---|---|---|
| Overall (N = 1827) | Patients who received tranexamic acid (n = 693) | Patients who did not receive tranexamic acid (n = 1134) | |||
| Demographic and injury data | |||||
| Age, median (IQR), y | 45 (23-65) | 47 (25-66) | 45 (22-65) | .03 | 20 (1.1) |
| Male sex | 1283 (70) | 486 (70) | 797 (70) | .94 | 3 (0.2) |
| Mechanism of injury | |||||
| Motor vehicle injury | 317 (18) | 130 (19) | 187 (17) | .05 | 29 (1.6) |
| Motorcycle injury | 167 (9) | 66 (10) | 101 (9) | ||
| Bicycle injury | 399 (22) | 169 (25) | 230 (21) | ||
| Pedestrian injury | 126 (7) | 52 (8) | 74 (7) | ||
| Other traffic injury | 56 (3) | 25 (4) | 31 (3) | ||
| Fall from height | 625 (35) | 208 (30) | 417 (37) | ||
| Firearm or stab injury | 34 (2) | 13 (2) | 21 (3) | ||
| Other | 74 (4) | 22 (3) | 52 (5) | ||
| ISS, median (IQR) | 26 (18-34) | 27 (21-38) | 26 (17-34) | <.001 | 208 (11.3) |
| Prehospital vital parameters at HEMS arrivalb | |||||
| GCS score, median (IQR) | 4 (3-7) | 4 (3-6) | 5 (3-7) | <.001 | 0 (0) |
| Systolic blood pressure, mm Hg | 143 (36) | 142 (38) | 143 (35) | .40 | 253 (13.8) |
| Heart rate, min−1 | 94 (29) | 98 (28) | 92 (29) | <.001 | 100 (5.5) |
| SpO2, median (IQR), % | 97 (93-99) | 97 (93-99) | 98 (94-99) | .40 | 273 (14.9) |
| In-hospital data | |||||
| Hospital LOS, median (IQR), dc | 16 (6-32) | 17 (7.5-35) | 15 (5-31) | .007 | 11 (1.0) |
| GOS score at discharge | |||||
| Death | 573 (31) | 250 (39) | 323 (32) | .001 | 170 (9.3) |
| Vegetative state | 38 (2) | 19 (3) | 19 (2) | ||
| Severe disability | 599 (33) | 214 (34) | 385 (38) | ||
| Moderate disability | 177 (10) | 70 (11) | 107 (10) | ||
| Good recovery | 270 (15) | 80 (13) | 190 (19) | ||
| Primary outcome | |||||
| Death at 30 d | 563 (33) | 241 (37) | 322 (30) | .005 | 113 (6.2) |
Abbreviations: GCS, Glasgow Coma Scale; GOS, Glasgow Outcome Scale; HEMS, Helicopter Emergency Medical Services; IQR, interquartile range; ISS, Injury Severity Score; LOS, length of stay; SpO2, oxygen saturation as measured by pulse oximetry.
Percentages are column percentages, may not necessarily add up to 100% because of rounding error, and may not necessarily use the total No. of the respective column as the denominator because of missing data (see Missing column).
Prehospital vital parameters represent the first documented values after the arrival of HEMS.
Hospital LOS was calculated only for patients who were known to survive to discharge.
A total of 693 patients (38%) received prehospital tranexamic acid. Of the 680 patients in whom the tranexamic acid dose was documented, most patients (615 [90%]) received a dose of 1 g and only 4 patients (1%) received more than 2 g. Of the 27 patients who received a dose of less than 1 g, 18 were children (67%). Table 1 shows the demographic and clinical characteristics of patients, stratified by tranexamic acid exposure. Patients who received prehospital tranexamic acid vs those who did not receive the drug were older (median [IQR] age, 47 [25-66] years vs 45 [22-65] years; P = .03), had a higher Injury Severity Score (median [IQR], 27 [21-38] vs 26 [17-34]; P < .001), had a lower prehospital GCS score (median [IQR], 4 [3-6] vs 5 [3-7]; P < .001), and had a higher heart rate at HEMS arrival (mean [SD], 98 [28] min–1 vs 92 [29] min–1; P < .001). Patients who received prehospital tranexamic acid showed a higher 30-day mortality vs those who did not receive the drug (37% [n = 241] vs 30% [n = 322]; P = .005) (Table 1).
In the unadjusted logistic regression analysis, 30-day mortality was statistically significantly higher in patients in the full cohort who received tranexamic acid compared with patients who did not receive the drug (odds ratio [OR], 1.34; 95% CI, 1.16-1.55; P < .001), patients with confirmed TBI (OR, 1.34; 95% CI, 1.15-1.56; P < .001), and patients with isolated TBI (OR, 1.74; 95% CI, 1.33-2.27; P < .001) (Table 2). After adjustment for potential confounders, no evidence of increased mortality was observed in the full cohort and in patients with confirmed TBI. However, substantially increased odds of mortality were observed in patients with isolated TBI (OR, 4.49; 95% CI, 1.57-12.87; P = .005) (eTables 3, 4, and 5 in Supplement 1; Table 2). The adjusted model showed appropriate calibration and good discrimination (area under the receiver operating characteristic curve, 0.90 for the full cohort; 0.89 for the confirmed TBI cohort; and 0.93 for the isolated TBI cohort). The analysis using multiple imputations consistently suggested a marked (albeit less pronounced) increase in mortality after tranexamic acid administration in patients with isolated TBI (OR, 2.05; 95% CI, 1.22-3.45; P = .007). Survival analyses also consistently showed an increased mortality in patients with isolated severe TBI after tranexamic acid administration, as shown in Table 2 and the Figure. In additional post hoc sensitivity analyses, a statistically significant association between tranexamic acid and increased mortality in patients with isolated TBI was consistently shown in 15 of 16 analyses, and in 1 analysis the P value was above the significance threshold (OR, 1.42; 95% CI, 0.95-2.14; P = .09) (eTable 6 in Supplement 1).
Table 2. Analyses of the Association Between Tranexamic Acid Exposure and Mortality.
| Analysis | Full cohort | P value | Confirmed TBI cohort | P value | Isolated TBI cohort | P value |
|---|---|---|---|---|---|---|
| Unadjusted analysis, OR (95% CI)a | ||||||
| Unadjusted logistic regression | 1.34 (1.16-1.55) | <.001 | 1.34 (1.15-1.56) | <.001 | 1.74 (1.33-2.27) | <.001 |
| Adjusted analysis, OR (95% CI)a | ||||||
| Confounder-adjusted logistic regression, original data set | 1.18 (0.73-1.90) | .51 | 1.27 (0.68-2.35) | .45 | 4.49 (1.57-12.87) | .005 |
| Confounder-adjusted logistic regression, after multiple imputations | 1.17 (0.84-1.65) | .35 | 1.19 (0.92-1.53) | .19 | 2.05 (1.22-3.45) | .007 |
| Sensitivity analysis, HR (95% CI)b | ||||||
| Confounder-adjusted survival analysis, original data set | 1.10 (0.92-1.31) | .30 | 1.10 (0.90-1.35) | .35 | 1.66 (1.08-2.54) | .02 |
| Confounder-adjusted survival analysis, after multiple imputations | 1.01 (0.90-1.14) | .81 | 1.00 (0.91-1.11) | .97 | 1.34 (1.16-1.55) | <.001 |
Abbreviations: HR, hazard ratio; OR, odds ratio; TBI, traumatic brain injury.
Logistic regression analyses were performed for the association between prehospital administration of tranexamic acid and 30-day mortality. All analyses, including the unadjusted, adjusted for clustering within trauma centers. Adjusted analyses also controlled for demographic factors, preinjury medical condition, injury characteristics and severity, operational characteristics, and first recorded vital parameters at Helicopter Emergency Medical Services arrival.
Sensitivity analyses were performed by modeling survival time using Cox proportional hazards regression model instead of dichotomizing mortality at 30 days.
Figure. Adjusted Survival Probability.
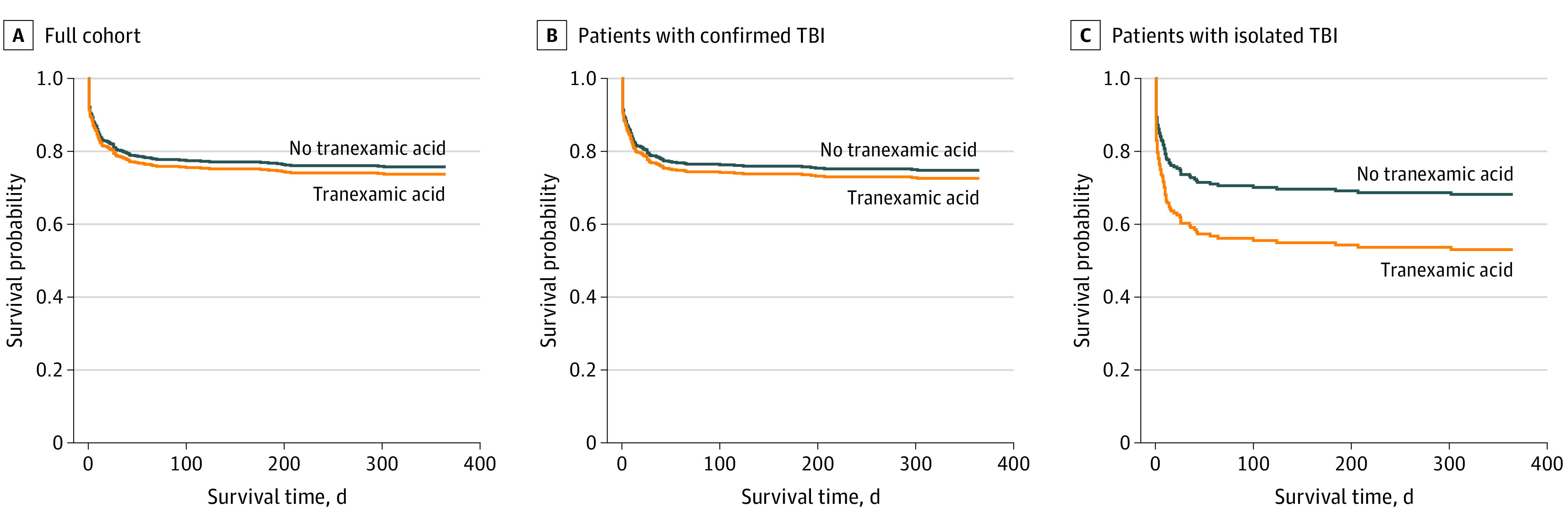
Cox proportional hazards regression model was used to estimate the adjusted survival probability for patients who received vs patients who did not receive tranexamic acid during prehospital treatment. Because the estimated survival function depends on the values and levels of all covariates, the depicted absolute values are just illustrative examples but are less relevant than the difference between the lines. In the full cohort (A) and the confirmed traumatic brain injury (TBI) cohort (B), tranexamic acid had a minimal and statistically nonsignificant association with survival (curves lie close to each other). In contrast, a marked association was observed in patients with isolated TBI after rigorous adjustment for potential confounders (C).
To ascertain whether the association of tranexamic acid with mortality depended on the use of anticoagulant medication before the injury, we performed an unplanned post hoc analysis in which the interaction between tranexamic acid use and anticoagulant use was modeled. No evidence of an interaction was found.
For secondary outcomes, the unadjusted analysis suggested higher 12-month mortality (OR, 1.29; 95% CI, 1.10-1.50; P = .001), lower GOS score at discharge (OR, 0.70; 95% CI, 0.65-0.76; P < .001), and longer hospital length of stay (incidence rate ratio, 1.17; 95% CI, 1.08-1.26; P < .001) in patients in the full cohort who received tranexamic acid. After adjustment for confounding, a statistically significant increase in 12-month mortality persisted in patients with isolated TBI after tranexamic acid exposure (OR, 3.31; 95% CI, 1.20-9.16; P = .02) (Table 3).
Table 3. Secondary Outcomes.
| Outcome | Cohort | Effect size (95% CI) | P value |
|---|---|---|---|
| Unadjusted analyses | |||
| Hospital LOS, IRR | Full | 1.17 (1.08-1.26) | <.001 |
| Confirmed TBI | 1.12 (1.03-1.22) | .009 | |
| Isolated TBI | 0.91 (0.75-1.10) | .32 | |
| GOS score at discharge, OR | Full | 0.70 (0.65-0.76) | <.001 |
| Confirmed TBI | 0.72 (0.63-0.82) | <.001 | |
| Isolated TBI | 0.61 (0.48-0.78) | <.001 | |
| 12-mo Mortality, OR | Full | 1.29 (1.10-1.50) | .001 |
| Confirmed TBI | 1.28 (1.07-1.53) | .007 | |
| Isolated TBI | 1.74 (1.34-2.25) | <.001 | |
| Adjusted analyses, original data set | |||
| Hospital LOS, IRR | Full | 0.92 (0.81-1.04) | .17 |
| Confirmed TBI | 0.89 (0.77-1.03) | .11 | |
| Isolated TBI | 0.71 (0.54-0.95) | .02 | |
| GOS score at discharge, OR | Full | 1.05 (0.81-1.37) | .71 |
| Confirmed TBI | 0.97 (0.72-1.30) | .83 | |
| Isolated TBI | 0.68 (0.25-1.90) | .47 | |
| 12-mo Mortality, OR | Full | 1.08 (0.66-1.76) | .76 |
| Confirmed TBI | 1.04 (0.60-1.79) | .89 | |
| Isolated TBI | 3.31 (1.20-9.16) | .02 | |
| Adjusted analyses, after multiple imputations | |||
| Hospital LOS, IRR | Full | 1.05 (0.92-1.20) | .44 |
| Confirmed TBI | 1.04 (0.88-1.22) | .65 | |
| Isolated TBI | 0.88 (0.69-1.11) | .27 | |
| GOS score at discharge, OR | Full | 0.97 (0.78-1.21) | .79 |
| Confirmed TBI | 0.86 (0.72-1.04) | .13 | |
| Isolated TBI | 0.69 (0.42-1.14) | .15 | |
| 12-mo Mortality, OR | Full | 0.99 (0.77-1.29) | .96 |
| Confirmed TBI | 0.99 (0.75-1.30) | .93 | |
| Isolated TBI | 1.78 (1.13-2.80) | .01 |
Abbreviations: GOS, Glasgow Outcome Scale; IRR, incidence rate ratio; LOS, length of stay; OR, odds ratio; TBI, traumatic brain injury.
Discussion
In this multicenter cohort study, we observed increased mortality among patients with isolated severe TBI who had received prehospital tranexamic acid, whereas no evidence of an association between tranexamic acid exposure and mortality was observed in the other 2 cohorts after controlling for potential confounders.
Tranexamic acid is an antifibrinolytic agent that inhibits plasminogen activation by competitive binding at the plasminogen lysine binding sites.22 The drug is widely used in hospitals to prevent surgical or postpartum blood loss.23,24 In patients with traumatic injury and bleeding, tranexamic acid has been shown in a randomized clinical trial to reduce mortality4 and has been widely used in prehospital and in-hospital trauma care. However, it remains unclear whether tranexamic acid is similarly advantageous for patients with severe TBI.
Intracranial hemorrhage is detrimental to outcome, and TBI itself is associated with coagulopathy,25 which may further aggravate bleeding and increase mortality.26 Therefore, it is tempting to assume that antifibrinolytic drugs will limit intracranial hemorrhage and thus improve outcomes. However, coagulation disorders after TBI are associated with the complex interplay between coagulopathy, fibrinolysis, and hypercoagulability.27,28 Hypercoagulability may promote cerebral intravascular microthrombi or systemic disseminated intravascular coagulation,27 and patients with severe TBI are at considerable risk of thromboembolic events from deep vein thrombosis.29 Drugs that alter the delicate balance between coagulation and fibrinolysis might, therefore, not be advantageous and could theoretically have detrimental implications for outcomes.
Previous studies have not provided a definitive answer on whether or not tranexamic acid should be used in patients with TBI.6,7,30,31 A 2019 meta-analysis reported that tranexamic acid was associated with decreased hemorrhage growth, but it found no statistically significant association with mortality.31 In addition, the CRASH-3 trial found no statistically significant effects of tranexamic acid on mortality in the overall population of patients with TBI.6 Although the authors observed decreased head injury–related mortality in the subgroup of patients with mild to moderate TBI when tranexamic acid was administered in the hospital within 3 hours after the injury, no such evidence was found for patients with severe TBI.6 This finding suggests that the treatment effect of tranexamic acid may depend on the severity of TBI and the timing of tranexamic acid administration, and tranexamic acid could plausibly alter the outcomes when it is administered in the earliest phase of treatment (ie, during prehospital treatment). Prehospital tranexamic acid administration was recently examined in a randomized clinical trial by Rowell et al.7 In a heterogenous population of patients with moderate to severe TBI, with and without extracranial injuries, Rowell et al7 found that tranexamic acid had no statistically significant effect on neurological recovery or mortality. Given that tranexamic acid seems to protect from exsanguination,5 it is plausible that its treatment effects may depend not only on TBI severity and timing of tranexamic acid administration but also on whether a patient is at risk for major extracranial hemorrhage. Therefore, we specifically addressed the association between prehospital tranexamic acid administration and outcomes in patients with severe TBI, particularly isolated severe TBI.
In unadjusted analyses, we observed a statistically significant increase in mortality across all patient subgroups when tranexamic acid was administered. However, the treatment was not randomly assigned. Patients who received tranexamic acid systematically differed from those who did not receive the drug, and in turn such differences may explain the differences in outcomes (eg, more severely injured patients received tranexamic acid more often, and injury severity is known to be associated with outcomes).15,16 After adjustment for potential confounders, the association between tranexamic acid administration and increased mortality vanished across the total cohort of patients, including patients with and without extracranial injuries; this finding was similar to the results observed by Rowell et al7 in their heterogenous patient population. However, the association persisted in the group of patients with isolated severe TBI. Similarly, adjusted 12-month mortality was also higher in patients with isolated severe TBI, and sensitivity analyses provided consistent evidence of increased mortality after tranexamic acid administration in patients with isolated severe TBI.
The findings in this cohort study highlight the possibility that tranexamic acid could lead to increased mortality in patients with isolated severe TBI. The observational data did not allow causal inferences or conclusions to be made about the mechanism by which tranexamic acid might be detrimental to survival, but this drug may induce a shift of the coagulation system toward hypercoagulability, perhaps involving microthrombi with impairment of the cerebral microcirculation and oxygenation. Other properties of tranexamic acid, such as modulation of inflammatory responses or promotion of seizure activity,22 may also play a role. Moreover, transient hypotension after rapid tranexamic acid administration, which can be detrimental to outcomes in patients with TBI,32 has been described. In patients with combined intracranial and extracranial injuries, adverse effects of tranexamic acid may have offset the advantages on extracranial bleeding that have been previously described in other studies and could explain why no evidence of advantages or adverse effects of tranexamic acid has been found in the heterogenous overall population of patients.
In the absence of higher-level evidence to support the universal use of tranexamic acid for all patients with severe TBI, the data suggest that tranexamic acid should be used judiciously in the prehospital setting. The data do not suggest abandoning the current practice of using tranexamic acid in those patients with extracranial injuries and substantial blood loss. Given the available evidence that tranexamic acid can prevent death from exsanguination in trauma patients with severe hemorrhage, it seems prudent to follow the current protocols for such patients. However, in patients with isolated severe TBI, tranexamic acid administration seems detrimental to survival. This observation suggests that tranexamic acid should be avoided in patients with severe TBI when major extracranial trauma is not suspected. We acknowledge that the findings from this study cannot be implemented 1 to 1 in prehospital practice, given that AIS scores are used to differentiate between suspected and confirmed TBI and to identify isolated severe TBI. These AIS scores are not available during prehospital treatment, and health care practitioners are, as always in prehospital care, faced with having to make treatment decisions based on limited information. Nonetheless, using tranexamic acid cautiously seems prudent when best clinical judgment suggests that a patient has isolated severe TBI (based on GCS score ≤8 in combination with other suggestive clinical findings) without evidence of relevant extracranial injuries.
Limitations
This study has several limitations. Although the data did not allow causal inferences to be made about the outcomes of tranexamic acid, we rigorously adjusted for confounders and performed several sensitivity analyses. Nonetheless, residual confounding (eg, associated with unobserved factors) could not be excluded. Moreover, missing data are inevitable in observational research and were addressed by multiple imputations in this study. The estimates varied considerably between the original and imputed analyses, suggesting that missing data had implications for the analysis results. However, although the numbers differed, the analysis of imputed data sets provided consistent evidence of an association between tranexamic acid administration and increased mortality in patients with isolated TBI. Other limitations include the potential for selection bias or information bias, and the BRAIN-PROTECT study protocol describes in detail how such bias was minimized.9
Furthermore, we did not address the association between the administered tranexamic acid dose and outcomes because almost all patients received a dose of 1 g. This dose is recommended by the Dutch national ambulance protocol and is commonly used internationally during prehospital treatment.33,34,35,36,37 We, however, cannot exclude the possibility that a different dose of tranexamic acid would have other outcomes. Moreover, the findings generated in a physician-based HEMS environment of a high-income country with relatively short distances to trauma centers may not necessarily readily generalize to settings with different demographic, geographic, or logistic characteristics.
Conclusions
To our knowledge, this cohort study is the first to demonstrate an association between tranexamic acid and increased mortality in patients with isolated severe TBI. This finding suggests that administration of tranexamic acid should be avoided in such patients.
eFigure. Patient Flow Diagram
eTable 1. Characteristics of Patients Who Died Versus Survived Within 30 Days
eTable 2. Characteristics of Patients per Subgroup (Confirmed and Isolated TBI)
eTable 3. Results of the Main Analysis: Full Cohort of Patients
eTable 4. Results of the Main Analysis: Confirmed Severe TBI
eTable 5. Results of the Main Analysis: Isolated Severe TBI
eTable 6. Results of Supplemental Sensitivity Analyses
Nonauthor Collaborators. The BRAIN-PROTECT collaborators.
References
- 1.Rubiano AM, Carney N, Chesnut R, Puyana JC. Global neurotrauma research challenges and opportunities. Nature. 2015;527(7578):S193-S197. doi: 10.1038/nature16035 [DOI] [PubMed] [Google Scholar]
- 2.Dewan MC, Rattani A, Gupta S, et al. Estimating the global incidence of traumatic brain injury. J Neurosurg. 2018;130:1-18. [DOI] [PubMed] [Google Scholar]
- 3.Perel P, Roberts I, Bouamra O, Woodford M, Mooney J, Lecky F. Intracranial bleeding in patients with traumatic brain injury: a prognostic study. BMC Emerg Med. 2009;9:15. doi: 10.1186/1471-227X-9-15 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Shakur H, Roberts I, Bautista R, et al. ; CRASH-2 trial collaborators . Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage (CRASH-2): a randomised, placebo-controlled trial. Lancet. 2010;376(9734):23-32. doi: 10.1016/S0140-6736(10)60835-5 [DOI] [PubMed] [Google Scholar]
- 5.Roberts I, Prieto-Merino D, Manno D. Mechanism of action of tranexamic acid in bleeding trauma patients: an exploratory analysis of data from the CRASH-2 trial. Crit Care. 2014;18(6):685. doi: 10.1186/s13054-014-0685-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.CRASH-3 trial collaborators . Effects of tranexamic acid on death, disability, vascular occlusive events and other morbidities in patients with acute traumatic brain injury (CRASH-3): a randomised, placebo-controlled trial. Lancet. 2019;394(10210):1713-1723. doi: 10.1016/S0140-6736(19)32233-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Rowell SE, Meier EN, McKnight B, et al. Effect of out-of-hospital tranexamic acid vs placebo on 6-month functional neurologic outcomes in patients with moderate or severe traumatic brain injury. JAMA. 2020;324(10):961-974. doi: 10.1001/jama.2020.8958 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP; STROBE Initiative . The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. 2007;370(9596):1453-1457. doi: 10.1016/S0140-6736(07)61602-X [DOI] [PubMed] [Google Scholar]
- 9.Bossers SM, Boer C, Greuters S, et al. ; BRAIN-PROTECT collaborators . Dutch prospective observational study on prehospital treatment of severe traumatic brain injury: the BRAIN-PROTECT study protocol. Prehosp Emerg Care. 2019;23(6):820-827. doi: 10.1080/10903127.2019.1587126 [DOI] [PubMed] [Google Scholar]
- 10.Franschman G, Verburg N, Brens-Heldens V, et al. Effects of physician-based emergency medical service dispatch in severe traumatic brain injury on prehospital run time. Injury. 2012;43(11):1838-1842. doi: 10.1016/j.injury.2012.05.020 [DOI] [PubMed] [Google Scholar]
- 11.Ringdal KG, Coats TJ, Lefering R, et al. ; Utstein TCD expert panel . The Utstein template for uniform reporting of data following major trauma: a joint revision by SCANTEM, TARN, DGU-TR and RITG. Scand J Trauma Resusc Emerg Med. 2008;16:7. doi: 10.1186/1757-7241-16-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Schober P, Vetter TR. Descriptive statistics in medical research. Anesth Analg. 2019;129(6):1445. doi: 10.1213/ANE.0000000000004480 [DOI] [PubMed] [Google Scholar]
- 13.Vetter TR, Schober P. Regression: the apple does not fall far from the tree. Anesth Analg. 2018;127(1):277-283. doi: 10.1213/ANE.0000000000003424 [DOI] [PubMed] [Google Scholar]
- 14.Schober P, Vetter TR. Repeated measures designs and analysis of longitudinal data: if at first you do not succeed-try, try again. Anesth Analg. 2018;127(2):569-575. doi: 10.1213/ANE.0000000000003511 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Kyriacou DN, Lewis RJ. Confounding by indication in clinical research. JAMA. 2016;316(17):1818-1819. doi: 10.1001/jama.2016.16435 [DOI] [PubMed] [Google Scholar]
- 16.Schober P, Vetter TR. Confounding in observational research. Anesth Analg. 2020;130(3):635. doi: 10.1213/ANE.0000000000004627 [DOI] [PubMed] [Google Scholar]
- 17.Bossers SM, Boer C, Bloemers FW, et al. ; BRAIN-PROTECT collaborators . Epidemiology, prehospital characteristics and outcomes of severe traumatic brain injury in the Netherlands: the BRAIN-PROTECT study. Prehosp Emerg Care. Published online September 22, 2020. doi: 10.1080/10903127.2020.1824049 [DOI] [PubMed] [Google Scholar]
- 18.Vetter TR, Schober P, Mascha EJ. Diagnostic testing and decision-making: beauty is not just in the eye of the beholder. Anesth Analg. 2018;127(4):1085-1091. doi: 10.1213/ANE.0000000000003698 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Schober P, Vetter TR. Missing data and imputation methods. Anesth Analg. 2020;131(5):1419-1420. doi: 10.1213/ANE.0000000000005068 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Schober P, Vetter TR. Adjustments for multiple testing in medical research. Anesth Analg. 2020;130(1):99. doi: 10.1213/ANE.0000000000004545 [DOI] [PubMed] [Google Scholar]
- 21.Schober P, Vetter TR. Survival analysis and interpretation of time-to-event data: the tortoise and the hare. Anesth Analg. 2018;127(3):792-798. doi: 10.1213/ANE.0000000000003653 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Lier H, Maegele M, Shander A. Tranexamic acid for acute hemorrhage: a narrative review of landmark studies and a critical reappraisal of its use over the last decade. Anesth Analg. 2019;129(6):1574-1584. doi: 10.1213/ANE.0000000000004389 [DOI] [PubMed] [Google Scholar]
- 23.WOMAN Trial Collaborators . Effect of early tranexamic acid administration on mortality, hysterectomy, and other morbidities in women with post-partum haemorrhage (WOMAN): an international, randomised, double-blind, placebo-controlled trial. Lancet. 2017;389(10084):2105-2116. doi: 10.1016/S0140-6736(17)30638-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Ker K, Prieto-Merino D, Roberts I. Systematic review, meta-analysis and meta-regression of the effect of tranexamic acid on surgical blood loss. Br J Surg. 2013;100(10):1271-1279. doi: 10.1002/bjs.9193 [DOI] [PubMed] [Google Scholar]
- 25.Dekker SE, Duvekot A, de Vries HM, et al. Relationship between tissue perfusion and coagulopathy in traumatic brain injury. J Surg Res. 2016;205(1):147-154. doi: 10.1016/j.jss.2016.06.023 [DOI] [PubMed] [Google Scholar]
- 26.Talving P, Benfield R, Hadjizacharia P, Inaba K, Chan LS, Demetriades D. Coagulopathy in severe traumatic brain injury: a prospective study. J Trauma. 2009;66(1):55-61. doi: 10.1097/TA.0b013e318190c3c0 [DOI] [PubMed] [Google Scholar]
- 27.Harhangi BS, Kompanje EJ, Leebeek FW, Maas AI. Coagulation disorders after traumatic brain injury. Acta Neurochir (Wien). 2008;150(2):165-175. doi: 10.1007/s00701-007-1475-8 [DOI] [PubMed] [Google Scholar]
- 28.Stein SC, Smith DH. Coagulopathy in traumatic brain injury. Neurocrit Care. 2004;1(4):479-488. doi: 10.1385/NCC:1:4:479 [DOI] [PubMed] [Google Scholar]
- 29.Skrifvars MB, Bailey M, Presneill J, et al. ; EPO-TBI investigators and the ANZICS Clinical Trials Group . Venous thromboembolic events in critically ill traumatic brain injury patients. Intensive Care Med. 2017;43(3):419-428. doi: 10.1007/s00134-016-4655-2 [DOI] [PubMed] [Google Scholar]
- 30.Schober P, Mascha EJ, Loer SA, Schwarte LA, Bossers SM. Tranexamic acid for traumatic brain injury. Lancet. 2020;396(10245):164. doi: 10.1016/S0140-6736(20)30542-0 [DOI] [PubMed] [Google Scholar]
- 31.Weng S, Wang W, Wei Q, Lan H, Su J, Xu Y. Effect of tranexamic acid in patients with traumatic brain injury: a systematic review and meta-analysis. World Neurosurg. 2019;123:128-135. doi: 10.1016/j.wneu.2018.11.214 [DOI] [PubMed] [Google Scholar]
- 32.Manley G, Knudson MM, Morabito D, Damron S, Erickson V, Pitts L. Hypotension, hypoxia, and head injury: frequency, duration, and consequences. Arch Surg. 2001;136(10):1118-1123. doi: 10.1001/archsurg.136.10.1118 [DOI] [PubMed] [Google Scholar]
- 33.Wafaisade A, Lefering R, Bouillon B, Böhmer AB, Gäßler M, Ruppert M; TraumaRegister DGU . Prehospital administration of tranexamic acid in trauma patients. Crit Care. 2016;20(1):143. doi: 10.1186/s13054-016-1322-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Shah Jahan MY, Shamila MA, Nurul Azlean N, et al. Administration of tranexamic acid for victims of severe trauma within pre-hospital care ambulance services (PHCAS) in Malaysia. Med J Malaysia. 2019;74(4):300-306. [PubMed] [Google Scholar]
- 35.Huebner BR, Dorlac WC, Cribari C. Tranexamic acid use in prehospital uncontrolled hemorrhage. Wilderness Environ Med. 2017;28(2S):S50-S60. doi: 10.1016/j.wem.2016.12.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Queensland Ambulance Service . Drug therapy protocols: tranexamic acid. Accessed May 31, 2020. https://www.ambulance.qld.gov.au/docs/clinical/dtprotocols/DTP_Tranexamic%20acid.pdf
- 37.West Midlands Ambulance Service . Trauma management guidelines. Accessed May 31, 2020. https://www.midlandsairambulance.com/media/1292/trauma-management-guidelines-may-2017.pdf
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eFigure. Patient Flow Diagram
eTable 1. Characteristics of Patients Who Died Versus Survived Within 30 Days
eTable 2. Characteristics of Patients per Subgroup (Confirmed and Isolated TBI)
eTable 3. Results of the Main Analysis: Full Cohort of Patients
eTable 4. Results of the Main Analysis: Confirmed Severe TBI
eTable 5. Results of the Main Analysis: Isolated Severe TBI
eTable 6. Results of Supplemental Sensitivity Analyses
Nonauthor Collaborators. The BRAIN-PROTECT collaborators.