

Key Points
Question
Is the Ad26.COV2.S vaccine immunogenic in humans, how quickly does it raise antibody responses, and what types of immune responses are elicited?
Findings
This randomized, double-blind, placebo-controlled phase 1 clinical trial of Ad26.COV2.S enrolled 25 participants. Antibodies were detected in vaccine recipients by day 8 and were observed in all vaccine recipients by day 57 after a single immunization. T-cell responses were also generated in vaccine recipients.
Meaning
In this phase 1 study, a single immunization with Ad26.COV2.S induced rapid binding and neutralization antibody responses as well as cellular immune responses.
Abstract
Importance
Control of the global COVID-19 pandemic will require the development and deployment of safe and effective vaccines.
Objective
To evaluate the immunogenicity of the Ad26.COV2.S vaccine (Janssen/Johnson & Johnson) in humans, including the kinetics, magnitude, and phenotype of SARS-CoV-2 spike-specific humoral and cellular immune responses.
Design, Setting, and Participants
Twenty-five participants were enrolled from July 29, 2020, to August 7, 2020, and the follow-up for this day 71 interim analysis was completed on October 3, 2020; follow-up to assess durability will continue for 2 years. This study was conducted at a single clinical site in Boston, Massachusetts, as part of a randomized, double-blind, placebo-controlled phase 1 clinical trial of Ad26.COV2.S.
Interventions
Participants were randomized to receive 1 or 2 intramuscular injections with 5 × 1010 viral particles or 1 × 1011 viral particles of Ad26.COV2.S vaccine or placebo administered on day 1 and day 57 (5 participants in each group).
Main Outcomes and Measures
Humoral immune responses included binding and neutralizing antibody responses at multiple time points following immunization. Cellular immune responses included immunospot-based and intracellular cytokine staining assays to measure T-cell responses.
Results
Twenty-five participants were randomized (median age, 42; age range, 22-52; 52% women, 44% male, 4% undifferentiated), and all completed the trial through the day 71 interim end point. Binding and neutralizing antibodies emerged rapidly by day 8 after initial immunization in 90% and 25% of vaccine recipients, respectively. By day 57, binding and neutralizing antibodies were detected in 100% of vaccine recipients after a single immunization. On day 71, the geometric mean titers of spike-specific binding antibodies were 2432 to 5729 and the geometric mean titers of neutralizing antibodies were 242 to 449 in the vaccinated groups. A variety of antibody subclasses, Fc receptor binding properties, and antiviral functions were induced. CD4+ and CD8+ T-cell responses were induced.
Conclusion and Relevance
In this phase 1 study, a single immunization with Ad26.COV2.S induced rapid binding and neutralization antibody responses as well as cellular immune responses. Two phase 3 clinical trials are currently underway to determine the efficacy of the Ad26.COV2.S vaccine.
Trial Registration
ClinicalTrials.gov Identifier: NCT04436276
This randomized trial compares the immunogenicity of a SARS-CoV-2 Ad26.COV2.S vaccine at high vs low vs no dose (placebo) in humans, including the kinetics, magnitude, and phenotype of coronavirus spike-specific humoral and cellular immune responses.
Introduction
Vaccination represents a key strategy to control the COVID-19 pandemic. Previous studies have demonstrated that an adenovirus serotype 26 (Ad26) vector1 expressing a stabilized SARS-CoV-2 spike (S),2,3 termed Ad26.COV2.S, effectively protected rhesus macaques against infection and hamsters against severe disease following SARS-CoV-2 challenge.4,5 Interim results of a phase 1/2a clinical trial in 810 participants describing the safety and immunogenicity of single-shot and 2-shot regimens of Ad26.COV2.S in humans have recently been reported.6
In this randomized, double-blind, placebo-controlled clinical trial of Ad26.COV2.S, 25 participants were enrolled at a single clinical site in Boston, Massachusetts, for detailed descriptive immunogenicity studies. Participants were randomized to receive single-shot and 2-shot vaccine regimens with either 5 × 1010 or 1 × 1011 viral particles of Ad26.COV2.S or placebo in healthy adults 18 to 55 years of age. This study reports the kinetics, magnitude, and diversity of humoral and cellular immune responses elicited by Ad26.COV2.S (Janssen/Johnson & Johnson).
Methods
Study Design
This study was conducted at a single site at Beth Israel Deaconess Medical Center in Boston. The protocol (Supplement 1) was approved by the Beth Israel Deaconess Medical Center institutional review board. All participants gave written informed consent and successfully completed an assessment of understanding before the initiation of study procedures. This descriptive study (cohort 1b) was performed as part of a larger multicenter, randomized, double-blind, placebo-controlled phase 1/2a trial to evaluate the safety, reactogenicity, and immunogenicity of Ad26.COV2.S at 5 × 1010 or 1 × 1011 viral particles administered intramuscularly as single-shot or 2-shot vaccine schedules, 56 days apart, in healthy adults. Cohort 1b enrolled adults 18 to 55 years of age (N = 25), and included visits and sampling of serum, plasma, and peripheral blood mononuclear cells to allow for investigation of exploratory end points. For the cohorts not reported here, cohort 1a enrolled adults 18 to 55 years of age (N = 375) and focused on collecting primary safety and immunogenicity end points. Cohort 3 (N = 375) enrolled participants who were older than 65 years and tested the same regimens as evaluated in cohort 1. Cohort 2 comparing different dosing intervals has not yet been reported.
Participants
Eligible participants were 18 to 55 years old (inclusive) and negative for SARS-CoV-2 infection by screening nasopharyngeal polymerase chain reaction and serum immunoglobulin testing. Eligible participants also had a body mass index of 30 or less (calculated as weight in kilograms divided by height in meters squared); were healthy, in the investigator’s clinical judgment, as confirmed by medical history, physical examination, clinical laboratory assessments, and vital signs performed at screening; and did not have comorbidities related to an increased risk of severe COVID-19. Participants who were of child-bearing potential were required to use highly effective contraception and could not be pregnant or breastfeeding. Race and ethnicity were based on participant reporting with fixed categories and were recorded to provide demographic information on the study population. Participants were excluded if they were currently working in an occupation with a high risk of exposure to SARS-CoV-2 or considered at the investigator’s discretion to be at increased risk to acquire COVID-19 for any other reason. Full eligibility criteria are described in the study protocol (Supplement 1).
Randomization
Randomization was done by an Interactive Web Response System using randomly permuted blocks of 5. The sponsor, clinical staff, investigators, participants, and laboratory personnel were blinded to assignment. Sponsor and statisticians were group-unblinded to immunogenicity group summaries without participant identifiers for the interim analysis when all participants completed the day 29 and day 71 visits or discontinued earlier. The pharmacist with primary responsibility for study product preparation and dispensing was not blinded to group assignment. To preserve blinding, they placed an overlay on the syringes.
The participants were randomly allocated to 1 of 5 experimental groups (n = 5/group): (1) 5 × 1010 viral particles of Ad26.COV2.S (low-dose) on day 1 and day 57 (low-dose/low-dose); (2) low-dose on day 1 and placebo on day 57 as a single-shot vaccine (low-dose/placebo); (3) 1 × 1011 viral particles of Ad26.COV2.S (high-dose) on day 1 and day 57 (high-dose/high-dose); (4) high-dose on day 1 and placebo on day 57 as a single-shot vaccine (high-dose/placebo); or (5) placebo on day 1 and day 57 (placebo/placebo).
Intervention
Ad26.COV2.S is a recombinant, replication-incompetent Ad26 vector encoding the full length and stabilized SARS-CoV-2 S protein derived from the first clinical isolate of the Wuhan strain (Wuhan, 2019, whole-genome sequence NC_045512). Ad26.COV2.S was supplied at a concentration of 1 × 1011 viral particles/mL as a suspension in single-use vials, with an extractable volume of 0.5 mL. Formulation buffer was supplied as 15-mM citrate, 5% (wt/wt) hydroxypropyl-β-cyclodextrin, 0.4% (wt/wt) ethanol, 0.03% (wt/wt) polysorbate 80, 75-mM sodium chloride, and pH of 6.2 and placebo was 0.9% sodium chloride. For blinding purposes, the same volume (1 mL) was administered to all participants. Study vaccine was administered by intramuscular injection into the deltoid muscle, preferably of the nondominant arm. Placebo consisted of 1 mL of 0.9% sodium chloride solution.
Outcomes
Immunogenicity end points included enzyme-linked immunosorbent assays (ELISA), pseudovirus neutralization assays, interferon (IFN)-γ, and IL-4 enzyme-linked immunospot (ELISPOT) assays to measure cellular immune responses, and intracellular cytokine staining (ICS) assays to measure CD4+ and CD8+ T-cell responses (eMethods in Supplement 2). Within the full randomized clinical trial, these end points were considered secondary. Exploratory immunogenicity end points included Ad26 neutralization assays, systems serology assays, and electrochemiluminescence assays (ECLA) (eMethods in Supplement 2).
Solicited adverse events (AEs), collected through a diary, were recorded for each vaccination from the time of vaccination until 7 days after vaccination. All other unsolicited AEs and special reporting situations, whether serious or nonserious, were reported for each vaccination from the time of vaccination until 28 days after vaccination. Unsolicited AEs with the onset date outside the timeframe defined above (>28 days after previous study vaccination), which were ongoing on the day of the subsequent vaccination, were recorded as such. All serious AEs and AEs leading to participant discontinuation (regardless of the causal relationship) were reported for all participants from the moment of first vaccination until completion of the participant’s last study-related procedure, which may include contact for safety follow-up. All AEs were followed until resolution or until clinically stable. An internal data review committee, consisting of members who were not directly involved in the study conduct, data management, or statistical analysis, was established and will monitor data to ensure the continued safety of the participants enrolled in this study.
Sample Size and Statistical Analysis
No formal statistical hypothesis for safety or immunogenicity was tested. The number of participants was chosen for this study to provide a preliminary safety and immunogenicity assessment. Placebo recipients were included for blinding and safety purposes and to provide additional control specimens for immunogenicity assays. The full analysis set includes all participants with at least 1 vaccine administration documented. The per-protocol immunogenicity population included all randomized and vaccinated participants for whom immunogenicity data were available excluding participants with major protocol deviations expecting to affect the immunogenicity outcomes. In addition, samples obtained after missed vaccinations or participants with natural infection occurring after screening (if applicable) were excluded from the analysis set. No formal statistical testing of safety data was planned. Safety data were analyzed descriptively by vaccine group. No formal hypothesis on immunogenicity was tested. Descriptive statistics were calculated for continuous immunologic parameters at all available time points. Immunogenicity analyses were performed on the per-protocol immunogenicity population. Analysis of immunologic data was performed using GraphPad Prism version 8.4.2 (GraphPad Software). Comparison of data between groups was performed using 2-sided Mann-Whitney U tests. Correlations were assessed by 2-sided Spearman rank-correlation tests. Two-sided P values of less than .05 were considered significant. This study reports an interim analysis that includes data through day 71 of the study.
Results
Study Design
Among 28 participants who were screened between July 27, 2020, and August 7, 2020, 2 participants were ineligible due to positive diagnostic test results for SARS-CoV-2 at screening and 1 was ineligible due to body mass index greater than 30 (Figure 1). Twenty-five participants received the following doses (N = 5/group): (1) 5 × 1010 viral particles of Ad26.COV2.S (low-dose) on day 1 and day 57 (low-dose/low-dose); (2) low-dose on day 1 and placebo on day 57 as a single-shot vaccine (low-dose/placebo); (3) 1 × 1011 viral particles of Ad26.COV2.S (high-dose) on day 1 and day 57 (high-dose/high-dose); (4) high-dose on day 1 and placebo on day 57 as a single-shot vaccine (high-dose/placebo); or (5) placebo on day 1 and day 57 (placebo/placebo). Demographics of the study population are shown in the Table. Safety data from these 25 participants have been reported separately.6
Figure 1. Participant Recruitment, Randomization, and Follow-up in a Study of Ad26.COV2.S Vaccine.

BMI indicates body mass index (calculated as weight in kilograms divided by height in meters squared); PCR, polymerase chain reaction; and vp, viral particles.
Table. Summary of Demographics and Baseline Characteristics.
| No. (%) | ||||
|---|---|---|---|---|
| Ad26.COV2.S, 5 × 1010 vp | Ad26.COV2.S, 1 × 1011 vp | Placebo | All participants | |
| No. | 10 | 10 | 5 | 25 |
| Age, y | ||||
| Mean (SD) | 43.7 (8.2) | 35.4 (7.7) | 40.8 (12.0) | 39.8 (9.3) |
| Median (range) | 45.0 (24.0-52.0) | 34.5 (26.0-47.0) | 42.0 (22.0-52.0) | 42.0 (22.0-52.0) |
| 18-40 | 2 (20) | 6 (60) | 2 (40) | 10 (40) |
| 41-55 | 8 (80) | 4 (40) | 3 (60) | 15 (60) |
| Sex | ||||
| Female | 5 (50) | 5 (50) | 3 (60) | 13 (52) |
| Male | 5 (50) | 4 (40) | 2 (40) | 11 (44) |
| Undifferentiateda | 0 | 1 (10) | 0 | 1 (4) |
| Race | ||||
| White | 8 (80) | 9 (90) | 5 (100) | 22 (88) |
| Asian | 2 (20) | 0 | 0 | 2 (8) |
| Multiple | 0 | 1 (10) | 0 | 1 (4) |
| Ethnicity | ||||
| Hispanic or Latino | 0 | 1 (10) | 1 (20) | 2 (8) |
| Not Hispanic or Latino | 9 (90) | 9 (90) | 4 (80) | 22 (88) |
| Not reported | 1 (10) | 0 | 0 | 1 (4) |
| Weight, kg | ||||
| Mean (SD) | 67.6 (13.0) | 71.2 (10.0) | 73.7 (10.5) | 70.2 (11.2) |
| Median (range) | 65.3 (46.7-90.5) | 68.8 (56.5-85.0) | 70.3 (61.7-89.0) | 68.9 (46.7-90.5) |
| Height, cm | ||||
| Mean (SD) | 171.1 (11.3) | 166.6 (10.7) | 171.8 (3.6) | 169.4 (9.9) |
| Median (range) | 175.3 (157.0-185.7) | 166.1 (146.0-182.6) | 172.5 (167.0-176.7) | 169.9 (146.0-185.7) |
| BMI | ||||
| Mean (SD) | 23.0 (3.4) | 25.7 (2.8) | 24.9 (3.0) | 24.5 (3.2) |
| Median (range) | 23.5 (18.8-27.1) | 25.6 (21.4-29.9) | 23.9 (22.1-29.9) | 24.8 (18.8-29.9) |
Abbreviations: BMI, body mass index (calculated as weight in kilograms divided by height in meters squared); vp, viral particles.
Undifferentiated: nonbinary sex.
Kinetics and Magnitude of Binding and Neutralizing Antibody Responses
By day 8 following immunization, binding antibodies were observed in 65% (13 of 20) of vaccine recipients against full-length S protein (Figure 2A and B; eFigure 1A in Supplement 2; P = .02, comparing undetectable geometric mean titer [GMT] at day 1 vs GMT of 41 on day 8) and in 90% (18 of 20) of vaccine recipients against the S receptor binding domain (RBD) (Figure 2A and B; eFigure 1B in Supplement 2; P = .003, comparing undetectable GMT at day 1 vs GMT of 41 on day 8 responses by ELISA). Virus-neutralizing antibodies were observed in 25% (5 of 20) of vaccine recipients (Figure 2C and D; eFigure 1C in Supplement 2) by a luciferase-based pseudovirus-neutralizing antibody assay.5,7,8
Figure 2. Kinetics and Magnitude of Binding and Neutralizing Antibodies (NAb) Following Ad26.COV2.S Vaccination.

Spike- and receptor binding domain (RBD)–specific binding antibodies by enzyme-linked immunosorbent assay (ELISA) (A and B) and SARS-CoV-2 pseudovirus neutralizing antibody (psVNA) and Ad26 virus neutralizing antibody (Ad26 VNA) (C and D) responses following Ad26.COV2.S vaccination. Symbols represent different dosing groups postprime and postboost. The red bars indicate geometric mean titers and the dotted lines indicate lower limits of quantitation (LLOQ).
By day 15, S-specific and RBD-specific binding antibodies were observed in 100% (20 of 20) of vaccine recipients (Figure 2A and B), and neutralizing antibodies were observed in 85% (17 of 20) of vaccine recipients (Figure 2C and D). Binding and neutralizing antibodies continued to increase on days 29, 57, and 71. By days 57 and 71, 100% (20 of 20) of vaccine recipients showed neutralizing antibodies as well as S- and RBD-specific binding antibodies. On day 71, the GMTs of S-specific binding antibodies were 2432, 3249, 5729, 2852, and 20; the GMTs of RBD-specific binding antibodies were 1018, 2023, 3666, 2372, and 21; and the GMTs of neutralizing antibodies were 242, 375, 449, 387, and 13 in the low-dose/low-dose, low-dose/placebo, high-dose/high-dose, high-dose/placebo, and placebo/placebo groups, respectively (Figure 2).
The boost immunization on day 57 increased binding antibody titers by a mean of 2.56-fold (range, 1.58-3.04) and neutralizing antibody titers by a mean of 4.62-fold (range, 3.56-5.68) in the low-dose/low-dose and high-dose/high-dose groups on day 71. The immunologic response to the boost was also manifested by an increase in Ad26 vector–specific neutralizing antibodies in the low-dose/low-dose and high-dose/high-dose groups on day 71 (Figure 2C and D).
S-specific and RBD-specific binding antibody titers on day 29 strongly correlated with each other (R = 0.98, P < .001; eFigure 2 in Supplement 2), and both correlated with neutralizing antibody titers on day 29 (R = 0.88, P < .001; and R = 0.86, P < .001, respectively; eFigure 2 in Supplement 2).
Diversity and Specificity of Antibody Responses
Assessment of binding and functional profiles of vaccine-elicited antibodies on day 29 by systems serology9 showed that Ad26.COV2.S induced S- and RBD-specific IgA1, IgA2, IgG1, IgG2, IgG3, IgG4, and IgM subclasses; FcγR2a, FcγR2b, FcγR3a, and FcγR3b binding; and antibody-dependent complement deposition, antibody-dependent neutrophil phagocytosis, antibody-dependent cellular phagocytosis, and antibody-dependent NK cell activation functional antiviral responses (Figure 3; eFigures 3 and 4 in Supplement 2). A similar diversity of antibody responses was observed to the S1 and S2 subdomains of the S protein (eFigures 5, 6, and 7 in Supplement 2).
Figure 3. Systems Serology Following Ad26.COV2.S Vaccination.

Polar plots showing the diversity of induced SARS-CoV-2 antibody characteristics and functions. The mean percentile of the spike- and receptor binding domain (RBD)–specific antibody features in each group are shown on day 29. Distance from the origin reflects the effect size. Each wedge represents a SARS-CoV-2 antibody feature, and the size of the wedge indicates the magnitude of the value. The colors represent the type of feature: orange, antibody Ig isotypes and subclasses; gray, Fc receptor (FcR) binding levels; and blue, antibody functions including antibody-dependent complement deposition (ADCD), antibody-dependent neutrophil phagocytosis (ADNP), antibody-dependent cellular phagocytosis (ADCP), and antibody-dependent NK cell activation (ADNKA).
An ECLA was used to evaluate the specificity of the antibody responses to SARS-CoV-2, SARS-CoV-1, CoV-229E, CoV-HKU1, CoV-NL63, and CoV-OC43. Ad26.COV2.S vaccination induced SARS-CoV-2 S-specific antibodies by ECLA (Figure 4) that appeared comparable to ELISA (Figure 2). Cross-reactive responses were observed to the S protein from SARS-CoV-1 at approximately 10-fold lower magnitude than SARS-CoV-2 (Figure 4). High background levels of antibodies were observed at baseline for the S proteins from the common cold coronaviruses CoV-229E, CoV-HKU1, CoV-NL63, and CoV-OC43, with no clear increase in these responses following vaccination (eFigure 8 in Supplement 2).
Figure 4. Antibody Cross-Reactivity Following Ad26.COV2.S Vaccination.

Electrochemiluminescence assay (Meso Scale Discovery SARS-CoV-2 IgG Panel 2; K15369U-2) assessing binding antibody responses to the spike proteins from SARS-CoV-2 and SARS-CoV-1 following Ad26.COV2.S vaccination. The red bars indicate geometric mean responses.
Cellular Immune Responses
S-specific cellular immune responses were assessed by IFN-γ and IL-4 ELISPOT assays in peripheral blood mononuclear cells of all participants, as well as multiparameter ICS assays in a subset of participants for which sufficient peripheral blood mononuclear cells were available. IFN-γ ELISPOT responses were observed in 65% (13 of 20) of vaccine recipients by day 15 and in 84% (16 of 19) of vaccine recipients by day 71, with no clear differences among groups (Figure 5A and B). No IL-4 responses were observed, indicating a TH1-biased cellular immune response. Multiparameter ICS assays confirmed the induction of central memory CD27+/CD45RA−/CD4+ and CD8+ T-cell responses in all but 1 vaccine recipient studied (Figure 5C). IFN-γ ELISPOT responses correlated with S-specific binding antibody titers (R = 0.55, P = .005), RBD-specific binding antibody titers (R = 0.54, P = .006), and neutralizing antibody titers (R = 0.57, P = .003) on day 29 (eFigure 9 in Supplement 2).
Figure 5. Kinetics and Magnitude of Cellular Immune Responses Following Ad26.COV2.S Vaccination.
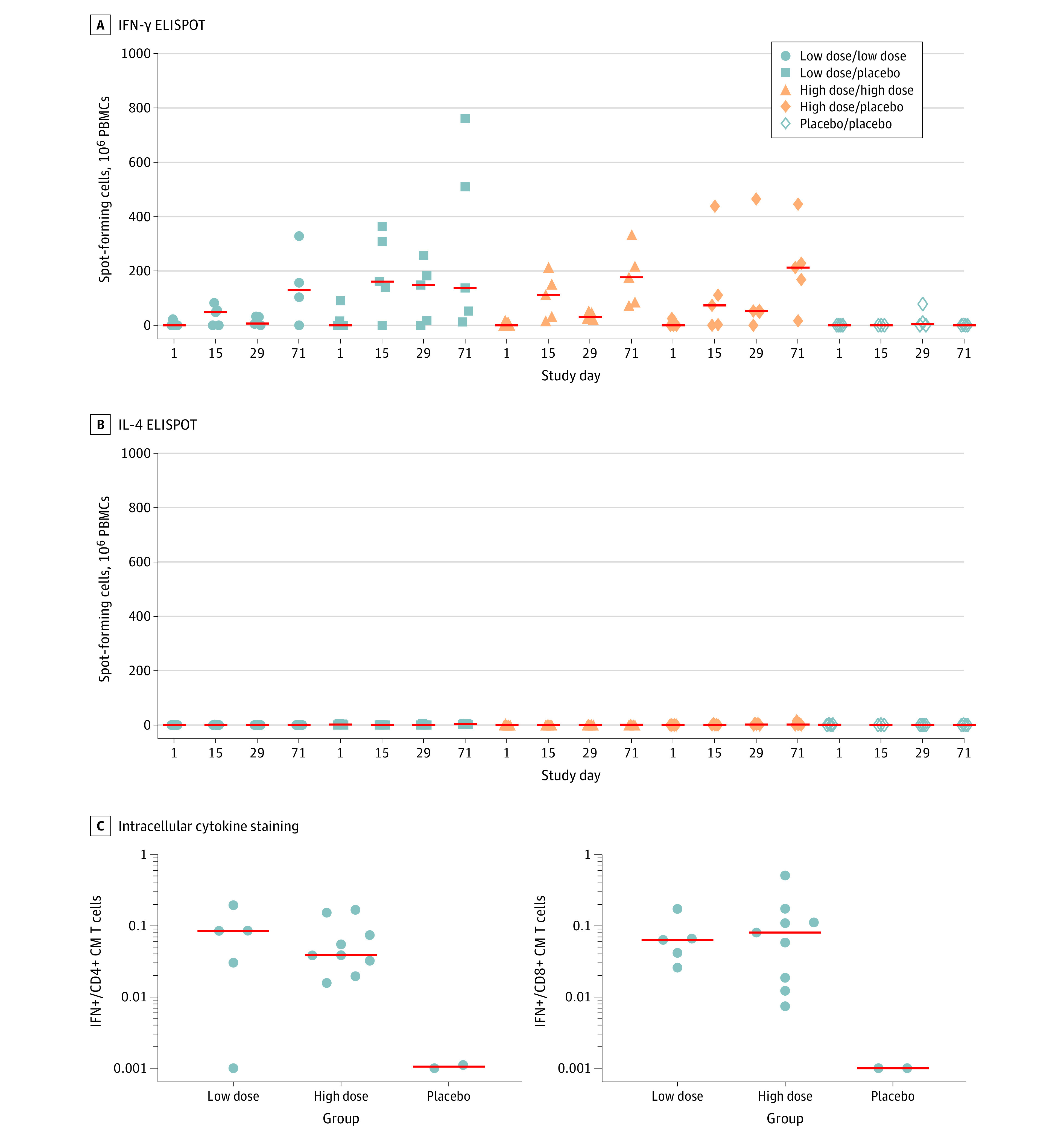
Interferon (IFN)-γ and IL-4 enzyme-linked immunospot (ELISPOT) responses to assess TH1 and TH2 cellular immune responses (A and B) and IFN-γ central memory (CM) CD27+/CD45RA-/CD4+ and CD8+ T-cell responses by intracellular cytokine staining (ICS) assays (C) following Ad26.COV2.S vaccination. ICS assays were performed in a subset of participants with sufficient peripheral blood mononuclear cells (PBMCs) on days 71 and 85. The red bars indicate geometric mean responses.
Discussion
In this study, humoral and cellular immune responses were assessed in 25 individuals who received Ad26.COV2.S or placebo in a phase 1 clinical trial. The findings extend previously reported results6 by showing that a single immunization with Ad26.COV2.S induced rapid binding and neutralization antibody responses as well as cellular immune responses, including induction of RBD-specific binding antibodies in 90% of vaccine recipients by day 8. Moreover, this vaccine induced a diversity of antibody subclasses, FcR binding properties, and antiviral functions. These data demonstrate that Ad26.COV2.S induced rapid and complex antibody responses as well as cellular immune responses.
The immunogenicity of Ad26.COV2.S complements recent reports describing the safety and immunogenicity of other COVID-19 vaccine candidates, including mRNA vaccines,10,11,12,13 Ad vector–based vaccines,14,15,16,17,18 and adjuvanted protein vaccines.19 The mRNA-1273,20 BNT162b2 mRNA,21 and ChAdOx122 vaccines have recently shown robust protective efficacy in phase 3 clinical trials, raising the possibility that additional COVID-19 vaccine candidates may also prove safe and effective in humans.
A central hypothesis for most current COVID-19 vaccine programs is that antibodies against the SARS-CoV-2 S protein are protective. Most programs are therefore focused on strategies that induce virus-specific neutralizing antibodies, although it is possible that other antibody functions may also contribute to protection. Binding, neutralizing, and functional nonneutralizing antibodies correlated with protective efficacy following DNA and Ad26 vaccination in rhesus macaques.5,8 Moreover, adoptive transfer of purified IgG from convalescent macaques protected naive macaques against SARS-CoV-2 challenge in a dose-dependent fashion.7,23 S-specific binding antibody titers of 400, RBD-specific binding antibody titers of 100, and neutralizing antibody titers of 50 represented the thresholds for protection in this preclinical model,23 but correlates of protection have not yet been determined for protection against COVID-19 infection or disease in humans. Nevertheless, the antibody titers induced in humans by Ad26.COV2.S exceeded these thresholds. CD8+ T-cell responses may also contribute to protection, particularly in the setting of waning or borderline antibody responses23 or potentially against viral variants that are partially resistant to antibodies. Two phase 3 clinical trials (NCT04505722 and NCT04614948) are currently underway to determine the efficacy of the Ad26.COV2.S vaccine.
Limitations
This study has several limitations. First, the small size of this study precludes formal statistical comparisons among groups. Second, participants aged 18 to 55 years were enrolled at a single site in Boston, and thus generalizability to elderly individuals and to other regions will require further study. Third, immunogenicity data are shown for 71 days following immunization, and additional follow-up time will be required to define the long-term durability of this vaccine. Fourth, the relevance of antibody responses to protection against COVID-19 infection or disease in humans remains to be proven. Fifth, additional studies will be required to determine whether neutralizing antibody and T-cell responses are diminished against the recently described SARS-CoV-2 variants from the United Kingdom, South Africa, and Brazil.
Conclusions
In this phase 1 study, a single immunization with Ad26.COV2.S induced rapid binding and neutralization antibody responses as well as cellular immune responses. Two phase 3 clinical trials are currently underway to determine the efficacy of the Ad26.COV2.S vaccine.
Trial Protocol
eMethods.
eFigure 1. Rapid Induction of Binding and Neutralizing Antibodies Following Ad26.COV2.S Vaccination
eFigure 2. Correlations of Humoral Immune Responses
eFigure 3. Systems Serology Data for S
eFigure 4. Systems Serology Data for RBD
eFigure 5. Systems Serology Data for S1
eFigure 6. Systems Serology Data for S2
eFigure 7. Systems Serology Summary for RBD, S, S1, and S2
eFigure 8. Antibody Cross-Reactivity Following Ad26.COV2.S Vaccination
eFigure 9. Correlations of Cellular and Humoral Immune Responses
Data Sharing Statement
References
- 1.Abbink P, Lemckert AA, Ewald BA, et al. Comparative seroprevalence and immunogenicity of six rare serotype recombinant adenovirus vaccine vectors from subgroups B and D. J Virol. 2007;81(9):4654-4663. doi: 10.1128/JVI.02696-06 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Wrapp D, Wang N, Corbett KS, et al. Cryo-EM structure of the 2019-nCoV spike in the prefusion conformation. Science. 2020;367(6483):1260-1263. doi: 10.1126/science.abb2507 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Bos R, Rutten L, van der Lubbe JEM, et al. Ad26 vector-based COVID-19 vaccine encoding a prefusion-stabilized SARS-CoV-2 Spike immunogen induces potent humoral and cellular immune responses. NPJ Vaccines. 2020;5:91. doi: 10.1038/s41541-020-00243-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Tostanoski LH, Wegmann F, Martinot AJ, et al. Ad26 vaccine protects against SARS-CoV-2 severe clinical disease in hamsters. Nat Med. 2020;26(11):1694-1700. doi: 10.1038/s41591-020-1070-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Mercado NB, Zahn R, Wegmann F, et al. Single-shot Ad26 vaccine protects against SARS-CoV-2 in rhesus macaques. Nature. 2020;586(7830):583-588. doi: 10.1038/s41586-020-2607-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sadoff J, Le Gars M, Shukarev G, et al. Interim results of a phase 1-2a trial of Ad26.COV2.S COVID-19 vaccine. N Engl J Med. 2021. doi: 10.1056/NEJMoa2034201 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Chandrashekar A, Liu J, Martinot AJ, et al. SARS-CoV-2 infection protects against rechallenge in rhesus macaques. Science. 2020;369(6505):812-817. doi: 10.1126/science.abc4776 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Yu J, Tostanoski LH, Peter L, et al. DNA vaccine protection against SARS-CoV-2 in rhesus macaques. Science. 2020;369(6505):806-811. doi: 10.1126/science.abc6284 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Chung AW, Kumar MP, Arnold KB, et al. Dissecting polyclonal vaccine-induced humoral immunity against HIV using systems serology. Cell. 2015;163(4):988-998. doi: 10.1016/j.cell.2015.10.027 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Walsh EE, Frenck RW Jr, Falsey AR, et al. Safety and immunogenicity of two RNA-based Covid-19 vaccine candidates. N Engl J Med. 2020;383(25):2439-2450. doi: 10.1056/NEJMoa2027906 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Widge AT, Rouphael NG, Jackson LA, et al. ; mRNA-1273 Study Group . Durability of responses after SARS-CoV-2 mRNA-1273 vaccination. N Engl J Med. 2021;384(1):80-82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Anderson EJ, Rouphael NG, Widge AT, et al. ; mRNA-1273 Study Group . Safety and immunogenicity of SARS-CoV-2 mRNA-1273 vaccine in older adults. N Engl J Med. 2020;383(25):2427-2438. doi: 10.1056/NEJMoa2028436 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Jackson LA, Anderson EJ, Rouphael NG, et al. ; mRNA-1273 Study Group . An mRNA vaccine against SARS-CoV-2: preliminary report. N Engl J Med. 2020;383(20):1920-1931. doi: 10.1056/NEJMoa2022483 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Folegatti PM, Ewer KJ, Aley PK, et al. ; Oxford COVID Vaccine Trial Group . Safety and immunogenicity of the ChAdOx1 nCoV-19 vaccine against SARS-CoV-2: a preliminary report of a phase 1/2, single-blind, randomised controlled trial. Lancet. 2020;396(10249):467-478. doi: 10.1016/S0140-6736(20)31604-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ramasamy MN, Minassian AM, Ewer KJ, et al. ; Oxford COVID Vaccine Trial Group . Safety and immunogenicity of ChAdOx1 nCoV-19 vaccine administered in a prime-boost regimen in young and old adults (COV002): a single-blind, randomised, controlled, phase 2/3 trial. Lancet. 2021;396(10267):1979-1993. doi: 10.1016/S0140-6736(20)32466-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Logunov DY, Dolzhikova IV, Zubkova OV, et al. Safety and immunogenicity of an rAd26 and rAd5 vector-based heterologous prime-boost COVID-19 vaccine in two formulations: two open, non-randomised phase 1/2 studies from Russia. Lancet. 2020;396(10255):887-897. doi: 10.1016/S0140-6736(20)31866-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Zhu FC, Guan XH, Li YH, et al. Immunogenicity and safety of a recombinant adenovirus type-5-vectored COVID-19 vaccine in healthy adults aged 18 years or older: a randomised, double-blind, placebo-controlled, phase 2 trial. Lancet. 2020;396(10249):479-488. doi: 10.1016/S0140-6736(20)31605-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Zhu FC, Li YH, Guan XH, et al. Safety, tolerability, and immunogenicity of a recombinant adenovirus type-5 vectored COVID-19 vaccine: a dose-escalation, open-label, non-randomised, first-in-human trial. Lancet. 2020;395(10240):1845-1854. doi: 10.1016/S0140-6736(20)31208-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Keech C, Albert G, Cho I, et al. Phase 1-2 trial of a SARS-CoV-2 recombinant spike protein nanoparticle vaccine. N Engl J Med. 2020;383(24):2320-2332. doi: 10.1056/NEJMoa2026920 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Baden LR, El Sahly HM, Essink B, et al. ; COVE Study Group . Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine. N Engl J Med. 2021;384(5):403-416. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Polack FP, Thomas SJ, Kitchin N, et al. ; C4591001 Clinical Trial Group . Safety and efficacy of the BNT162b2 mRNA COVID-19 vaccine. N Engl J Med. 2020;383(27):2603-2615. doi: 10.1056/NEJMoa2034577 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Voysey M, Clemens SAC, Madhi SA, et al. ; Oxford COVID Vaccine Trial Group . Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: an interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet. 2021;397(10269):99-111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.McMahan K, Yu J, Mercado NB, et al. Correlates of protection against SARS-CoV-2 in rhesus macaques. Nature. 2021;590(7847):630-634. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Trial Protocol
eMethods.
eFigure 1. Rapid Induction of Binding and Neutralizing Antibodies Following Ad26.COV2.S Vaccination
eFigure 2. Correlations of Humoral Immune Responses
eFigure 3. Systems Serology Data for S
eFigure 4. Systems Serology Data for RBD
eFigure 5. Systems Serology Data for S1
eFigure 6. Systems Serology Data for S2
eFigure 7. Systems Serology Summary for RBD, S, S1, and S2
eFigure 8. Antibody Cross-Reactivity Following Ad26.COV2.S Vaccination
eFigure 9. Correlations of Cellular and Humoral Immune Responses
Data Sharing Statement