

Abstract
Arthroscopic long head of biceps tenotomy is an established technique for addressing shoulder pain associated with long head of biceps pathology. Arthroscopic techniques, compared with open surgery, have demonstrated improvements in outcomes for patients including rapid recovery, but either regional or general anesthesia is required, which is associated with complications. We describe a novel technique using a Nanoscope needle arthroscopy system that allows for long head of biceps tenotomy to be performed under local anesthetic in the outpatient or office setting.
Technique Video
The video illustrates the procedural steps. It starts with patient setup, shows the portals used, and continues with intraoperative footage of long head of biceps tenotomy.
Shoulder pain due to pathology affecting the long head of the biceps (LHB) is common. Frequently it is due to partial-thickness tears, hourglass biceps,1 biceps instability, or dislocation. Arthroscopic assessment of the shoulder is commonly performed, and arthroscopic LHB tenotomy has been shown to produce significant benefits to the patient which are sustained.2,3 However, patients undergoing these procedures often have medical comorbidities that increase the risk of anesthesia owing to the cardiorespiratory effects of either regional anesthesia (from diaphragmatic paralysis during interscalene blockage) or general anaesthesia.4
Arthroscopic surgery allows the whole shoulder joint to be inspected, and concomitant pathologies, such as rotator cuff tears, can be treated in the same sitting. It is unclear, however, how much additional benefit is gained from this over and above a simple LHB tenotomy.2,3
We describe a surgical technique using a Nanoscope (Arthrex, Naples, FL) to perform a nanoscopic assessment of the shoulder and nanoscopic LHB tenotomy under local anesthetic. This has been made possible by the reduction in size of the instruments and is a procedure that is well tolerated and accepted by patients.
Surgical Technique
Fig 1, Fig 2, Fig 3, Fig 4, Fig 5, Fig 6 to Fig 1, Fig 2, Fig 3, Fig 4, Fig 5, Fig 6 and the Video 1 show the surgical technique.
Fig 1.

Patient setup for local anesthetic procedure in an operating theater setting. Left shoulder in beach-chair position.
Fig 2.

Nanoportal placement for shoulder nanoscopy shown here on the left shoulder.
Fig 3.

Nanoscope and fluid management cannula.
Fig 4.
Diagnostic nanoscope view from the glenohumeral joint of the right shoulder, showing rotator cuff tear and hourglass biceps.
Fig 5.

Nanoscope and instrument in the left shoulder, picture taken from above.
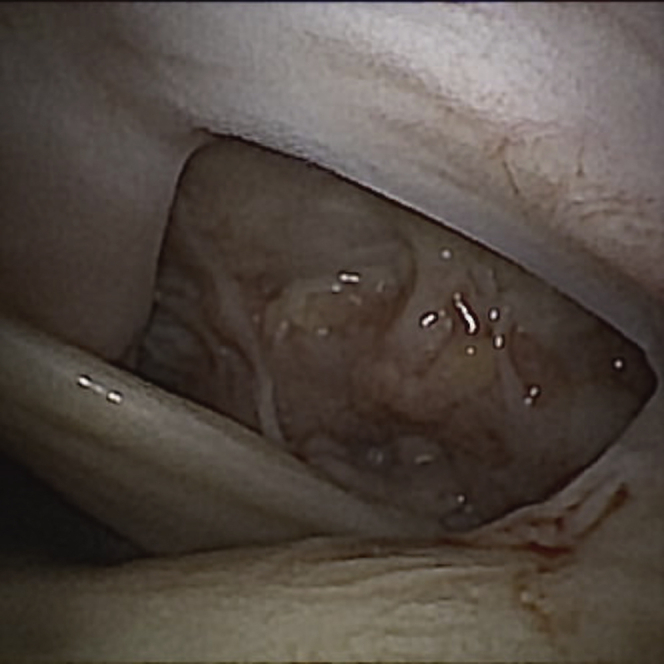
Fig 6.

Nanobiter performing long head of biceps tenotomy in a left shoulder. The humeral head is seen below the Nanobiter.
Patient Setup
The procedure can be performed in a procedure room or operating theater, depending on local facilities. The patient is placed in a sitting position so that the posterior, lateral, and anterior aspects of the shoulder are unimpeded. Draping is used to ensure a sterile field. The arm is supported on a rest so that the arm is in ∼30° forward flexion, and the patient can relax the limb to ensure the rotator cuff muscles do not contract and prevent entry to the glenohumeral joint (Fig 1).
Portal Selection
The Nanoscope has a 0° view; therefore, portals should be placed slightly away from a standard portal for a 30° arthroscope. In patients with a suspected or confirmed rotator cuff tear, entry to the glenohumeral joint can be made posterolaterally directly into the joint via the standard posterior entry diagnostic (SPED) portal, which is more laterally placed than a standard soft spot portal. Alternatively an anterolateral diagnostic and inspection (ALDI) portal can be used to visualize the rotator cuff and bursa and the joint through the rotator cuff tear if present (Fig 2). This portal is higher and more anterior than a standard anterolateral portal. We have found that the ALDI portal is more commonly used as the initial portal for diagnostics. Portal selection is important, as local anesthetic infiltration will be used in the skin and subcutaneous tissue relevant to the portal location.
Local Anesthetic
Local anesthetic, 40 ml with adrenaline, is used, based on safe dosage calculation related to the patient’s weight. First, 5 ml is infiltrated around the intended portal sites, and the remaining anesthetic is injected into the joint with sufficient time left to ensure adequate onset of action.
Fluid Management
A 3-way tap is set up to connect to a 1-liter bag of normal saline, a 50-ml luer lock syringe, and a giving set connected to the nanoscope. This allows an assistant to control fluid flow into or out of the shoulder (Fig 1).
Diagnostic Nanoscopy
A 2.2-mm cannula is inserted, and the 1.9-mm nanoscope is inserted through the cannula (Fig 3). Diagnostic nanoscopy is performed to diagnose or confirm relevant pathology in the shoulder (Fig 4; Video 1). Pictures and videos can be obtained and saved on the portable console.
Procedure Portal
The anterior BICeptor procedure portal is located so that it allows the instrument to cross at a perpendicular to the LHB to carry out the LHB tenotomy (Fig 2). A needle is used to localize the portal and additional anesthetic infiltration is used if necessary. A small stab incision is used to insert a 2-mm Nanobiter instrument (Arthrex) into the joint (Fig 4). The LHB tenotomy is completed (Fig 5).
Postoperative Care
The patient has waterproof dressings applied over the needle incisions. They are observed by the clinic nurse for a short period of time after the procedure. Direct discharge home from the procedure or waiting room is made. The patient is given an information leaflet containing exercise to mobilize the shoulder to prevent stiffness.
Discussion
This nanoscopic technique demonstrates that the technology available now is capable of allowing surgeons to perform local anesthetic procedures in the outpatient or operating theater setting with high-quality images to aid visualization. This simple 2-portal technique minimizes soft tissue trauma and fluid extravasation to ensure postoperative pain is kept to a minimum. Other reports have shown that the view with a Nanoscope is sufficient to safely carry out other surgical procedures in the shoulder.5,6
Isolated arthroscopic tenotomy of the LHB has been shown to have a significant improvement in patient and clinician-reported outcomes measures.7 However, many of these patients are elderly with medical comorbidities, and general anesthesia is not without risk. Therefore, this local anesthetic procedure described has significant advantages in excluding those anesthetic risks in a technique that is well tolerated by patients.
In the setting of a rotator cuff tear, there are many additional procedures described to improve outcomes for patients. With improvements in arthroscopic techniques and medical devices, we hypothesize that it is most convenient for surgeons to carry out all necessary procedures at the same sitting, e.g., LHB tenotomy and rotator cuff repair, despite the possibility that the expensive and time-consuming rotator cuff repair may have minimal additional pain-relieving benefits for the patient. It may be the fear of failure of the patient to improve with an isolated LHB tenotomy, thus needing a further procedure, that promotes this philosophy in treatment. However, with a simple local anesthetic procedure to complete the LHB tenotomy, it is likely that many patients will not need to undergo further procedures in the future, particularly in the case of dislocation of the long head of biceps.
The difficulties that we have experienced using this technique are related to the learning curve of using the 0° scope and the correct placement of the local anesthetic. The learning curve of the 0° scope is minimal and is addressed by adjusting your standard arthroscopic portal, usually in a lateral direction. Calculating the maximum safe volume of local anesthetic before surgery ensures that an adequate volume is available for use without compromising safety (Table 1). The procedures have all been tolerated well on this basis. Also, the active contraction of the rotator cuff can be a challenge, causing difficulty entering the glenohumeral joint. By setting the patient up with an arm rest, with the arm held in slight forward flexion, this contraction of the rotator cuff is reduced. In fact, most sports surgery or shoulder surgery specialists will rarely see the rotator cuff in action. However, local anesthetic nanoscopy shows this marvelous dynamic structure in action, with active movement of the arm compressing the humeral head into the glenoid.
Table 1.
Pearls and pitfalls
| Pearls |
| Alter traditional portals to account for 0° scope |
| Use a 50-ml luer lock syringe and 3-way tap to control fluid |
| Ensure Nanobiter is perpendicular to long head of biceps |
| Pitfalls |
| Attempting interventional procedures before establishing competencies in diagnostic nanoscopy under local anesthetic |
| Not enough local anesthetic volume used |
When performing the LHB tenotomy, it is essential that the Nanobiter is perpendicular to the LHB. The 2-mm size of the instrument is excellent in minimizing soft tissue trauma on entry; however, it will make the tenotomy difficult if it is not brought in perpendicular of the tendon, as the jaws will not engage on the tissue. We find needle localization critical to resolving this issue.
The advantages and disadvantages of wide-awake shoulder nanoscopic long head of biceps tenotomy are outlined in Table 2. The main advantages are the avoidance of general or regional anesthetic, reducing the morbidity associated with these anesthetic techniques. The disadvantage is the learning curve of using a 0° scope; however, it is short and can be learned when performing normal shoulder arthroscopic procedures.
Table 2.
Advantages and disadvantages
| Advantages |
| Avoidance of risks of general anesthetic |
| Avoidance of risks of regional anesthetic |
| Less swelling and pain |
| Reduced postoperative pain |
| Immediate discharge |
| Fully disposable single-use set |
| Disadvantages |
| Additional cost of nanoscope |
| Learning curve with 0° scope |
Shoulder nanoscopy is beginning to become an established field in sports medicine. The visualization technology has sufficiently improved to allow this to become the standard of care. Because of the small size of the instrumentation, there are increasing possibilities for other shoulder soft tissue procedures to be carried out under local anesthetic.
Footnotes
The authors report the following potential conflicts of interest or sources of funding: C.P. reports grants, Arthrex. R.D. reports grants, Arthrex. N.P. reports grants, Arthrex. Full ICMJE author disclosure forms are available for this article online, as supplementary material.
Supplementary Data
The video illustrates the procedural steps. It starts with patient setup, shows the portals used, and continues with intraoperative footage of long head of biceps tenotomy.
References
- 1.Boileau P., Ahrens P.M., Hatzidakis A.M. Entrapment of the long head of the biceps tendon: The hourglass biceps—a cause of pain and locking of the shoulder. J Shoulder Elbow Surg. 2004;13:249–257. doi: 10.1016/j.jse.2004.01.001. [DOI] [PubMed] [Google Scholar]
- 2.Walch G., Edwards T.B., Boulahia A. Arthroscopic tenotomy of the long head of the biceps in the treatment of rotator cuff tears: Clinical and radiographic results of 307 cases. J Shoulder Elbow Surg. 2005;14:238–246. doi: 10.1016/j.jse.2004.07.008. [DOI] [PubMed] [Google Scholar]
- 3.Veen E.J.D., Boeddha A.V., Diercks R.L. Arthroscopic isolated long head of biceps tenotomy in patients with degenerative rotator cuff tears: mid-term clinical results and prognostic factors. Eur J Orthop Surg Traumatol. 2020 doi: 10.1007/s00590-020-02787-z. (online ahead of print) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Shin J.J., Popchak A.J., Musahl V. Complications after arthroscopic shoulder surgery: A review of the American Board of Orthopaedic Surgery Database. J Am Acad Orthop Surg Glob Res Rev. 2018;2:e093. doi: 10.5435/JAAOSGlobal-D-18-00093. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Lavender C., Lycans D., Kopiec A. Nanoscopic single-incision anterior labrum repair. Arthrosc Tech. 2020;9:e297–e301. doi: 10.1016/j.eats.2019.10.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Lavender C., Lycans D., Sina Adil S.A. Single-incision rotator cuff repair with a needle arthroscope. Arthrosc Tech. 2020;9:e419–e423. doi: 10.1016/j.eats.2019.11.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ahmed A.F., Toubasi A., Mahmoud S. Long head of biceps tenotomy versus tenodesis: A systematic review and meta-analysis of randomized controlled trials. Shoulder & Elbow. 2020 doi: 10.1177/1758573220942923. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
The video illustrates the procedural steps. It starts with patient setup, shows the portals used, and continues with intraoperative footage of long head of biceps tenotomy.
The video illustrates the procedural steps. It starts with patient setup, shows the portals used, and continues with intraoperative footage of long head of biceps tenotomy.