

Abstract
Anterior cruciate ligament reconstruction failure remains a commonly seen outcome despite advances in technique and graft options. Recent studies have shown that the declination of the tibial plateau slope in the sagittal plane affects the in situ stress on the anterior cruciate ligament. The native posterior tibial slope has been described to range from 7° to 10°. However, several authors have suggested that a posterior tibial slope >12° should be considered pathologic. Given the recent evidence, our institution has begun performing a tibial tubercle–sparing anterior closing wedge proximal tibial osteotomy with cross screw fixation to decrease sagittal plane tibial slope.
Technique Video
This video details a tibial tubercle anterior wedge osteotomy to correct a pathologic posterior tibial slope with cross-screw fixation. The patient should be positioned supine on a radiolucent flat top table. The C-arm should be placed on the contralateral side of the operative extremity. Radiolucent triangles are helpful for positioning. The incision is typically 6 to 8 cm beginning at the tibial tubercle and proceeds distally. The osteotomy start point is just distal to the tibial tubercle aiming toward the proximal tibiofibular joint on the lateral radiograph. Breakaway pins and a parallel guide are used to guide the trajectory of the proximal and distal pins. The use of fluoroscopy is recommended to ensure the pins are coplanar on the lateral view. The distal pins are then inserted in a similar fashion to the proximal pins based on preoperative measurements of the necessary osteotomy size. The tips of the distal pins should intersect the proximal pins. The posterior cortex should not be violated. The breakaway pins are then broken off and the pins are used as a cutting guide for the osteotomy. After the bone wedge is removed, the knee should be extended to close the osteotomy gap. K-wires are then used to guide the trajectory of the 4.5mm cannulated crossing screws for fixation. A 3.2-mm drill is used to drill bicortically, followed by a 4.5-mm tap to facilitate screw passage. An anterior trajectory of the screws is recommended.
Anterior cruciate ligament (ACL) reconstruction failure remains a commonly seen outcome despite advances in technique and graft options. Risk factors for ACL reconstruction failure include the use of allograft in young patients, female sex, improper tunnel positioning, and greater body mass index.
Recent studies have shown that the declination of the tibial plateau slope in the sagittal plane affects the in situ stress on the ACL. Giffin et al.1 demonstrated that an increased posterior tibial slope under load resulted in anterior displacement of the tibia relative to the femur. Follow-up studies have confirmed that increased tibial slope leads to a significantly increased amount of in situ stress on both the native ACL and an ACL graft.1 The native posterior tibial slope has been described to range from 7° to 10°. Several authors have suggested that a posterior tibial slope >12° should be considered pathologic.2, 3, 4 Investigations by Salmon et al.2,3 showed that adolescents with a tibial slope of >12° were 11 times more likely to sustain an ACL graft failure. In addition, adults in this study with a tibial slope of >12° were 7 times more likely to sustain an ACL graft failure.3
Given the recent evidence, the senior author at our institution has begun performing an anterior closing wedge proximal tibial osteotomy to decrease sagittal plane tibial slope. The purpose of this Technical Note is to describe the senior author's preferred technique and indications for an anterior closing wedge osteotomy.
Indications and Contraindications
Indications for performing an anterior closing wedge proximal tibia osteotomy include at least one previous ACL reconstruction failure and a posterior tibial slope of 12° or more. Contraindications include posterior cruciate ligament incompetence, genu recurvatum deformity, and primary ACL reconstruction.
Preoperative Planning
Care must be taken when assessing the posterior tibial slope on radiographs. First, ensure that measurements are taken on a near-perfect lateral radiograph with the femoral condyles superimposed. A standard knee radiograph is frequently insufficient for templating, since it does not reveal enough tibial shaft to obtain an accurate measurement. We recommend obtaining a lateral tibia radiograph for templating. Measurement of tibial slope has been addressed in previous publications, but we prefer to use the method described by Kızılgöz et al.5,6 The surgeon chooses 2 points in the tibial diaphysis, distal to the tibial tubercle, and separated by 10 cm to create the longitudinal axis. The points should be placed halfway between the anterior and posterior cortices (Fig 1). The planned resection can then be determined by subtracting the normal posterior tibial slope from the measured slope; a normal posterior slope is 7-9° (Fig 2).7 Magnetic resonance imaging and computed tomography may be useful to identify concomitant injuries and to assess bone tunnel widening from previous ACL reconstructions. This procedure may be performed in conjunction with ACL reconstruction or as a staged procedure with bone tunnel grafting if there is excessive tunnel widening.
Fig 1.
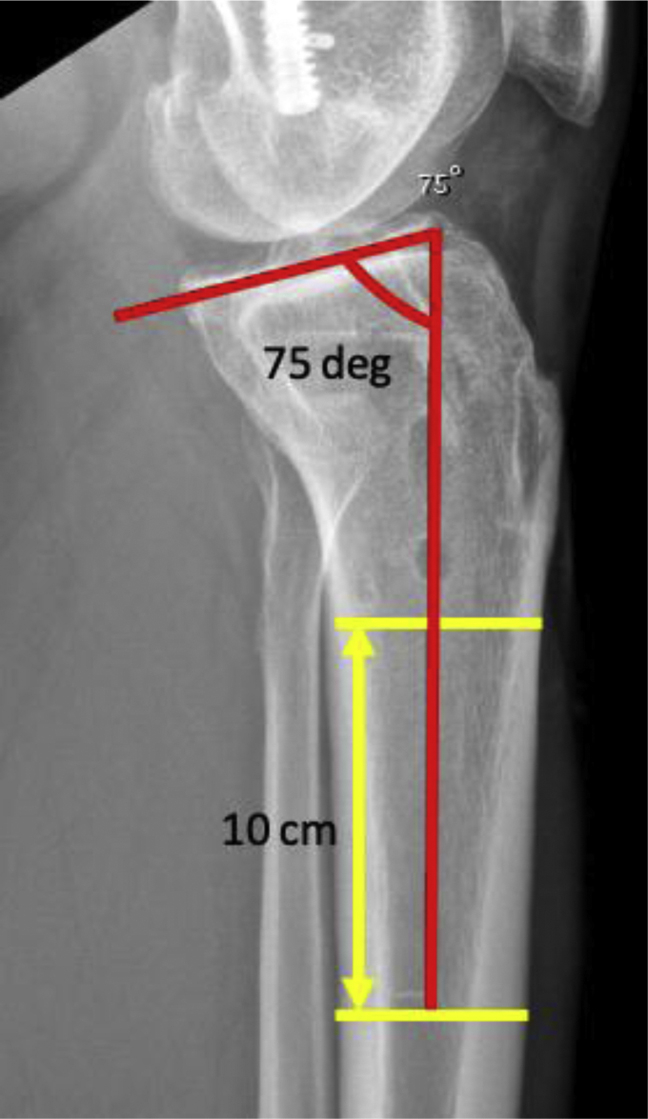
Full-length lateral tibia radiograph (cropped) with measured posterior tibial slope.
Fig 2.

Templated osteotomy resection, determined by subtracting the desired postoperative posterior tibial slope (7°) from the measured slope in Figure 1. The proximal cut start point is distal to the tibial tubercle and the trajectory is in-line with the proximal tibiofibular joint. The distal cut should intersect the proximal cut posteriorly without violating the posterior cortex. The width of resected anterior cortex should be measured based on this preoperative template radiograph.
Positioning
The patient should be positioned supine on a radiolucent table. A lateral post should be placed on the operating table for use during the arthroscopic portions of the procedure. The C-arm should be positioned opposite the operative leg. Radiolucent triangles can be helpful during the osteotomy portion of the procedure.
Arthroscopy
The extremity is exsanguinated with gravity and standard arthroscopy portals are used. Initial assessment of the ACL graft and treatment of meniscal or chondral pathology can be performed before the osteotomy. If a staged procedure is planned, grafting of bone tunnels can be performed at this time. If reconstruction is to be performed concomitantly, ACL tunnels should be made before the osteotomy. This avoids accidentally making the osteotomy through the tunnel trajectory. If there is inadequate space available, an all-inside ACL reconstruction can be performed. Placement and fixation of the graft is done after the osteotomy to avoid disturbing the graft.
Osteotomy
The incision should be midline on the tibia from the tibial tubercle to 6 to 8 cm distal, preferably allowing access to the tibial ACL tunnel and the osteotomy through one incision. Create full-thickness skin flaps medially and laterally. Dissect subperiosteally to allow passage of a radiolucent retractor posteromedially and a Hohmann retractor laterally. The osteotomy start point is just distal to the tibial tubercle and the ACL tunnel, aiming toward the proximal tibiofibular joint on the lateral radiograph. Take care that the trajectory is not too close to the tibial joint surface, so as to avoid an iatrogenic tibial plateau fracture. Breakaway pins are used as a parallel guide (Arthrex, Naples, FL) to guide the proximal and distal trajectory pins. The first breakaway pin is placed midline at the proximal starting point and aims towards the proximal tibiofibular joint on the lateral radiograph (Fig 3). An adjacent medial and lateral breakaway pin should be inserted with a parallel trajectory using the parallel guide (Fig 4). Fluoroscopy is used to ensure that the pins are co-planar on the lateral view, to avoid creating a multiplanar osteotomy that would lead to varus or valgus malalignment (Fig 3). Based on preoperative estimates of the desired resection, the 3 distal pins can then be placed in the same fashion. The tips of the distal pins should intersect with the tips of the proximal pins. The pins should not pass through the posterior cortex. Preservation of the posterior cortex for is critical to maintain structural rigidity and to avoid neurovascular injury. The pins are then broken off at the level of the osteotomy cutting guide (Fig 5). Next, using the osteotomy cutting guide, and while maintaining the retractors in a safe position, an oscillating saw is used to make the proximal cut. Fluoroscopy should be used in the lateral position to ensure that the posterior cortex is not violated. An osteotome can be used when within a few centimeters of the posterior cortex; do not violate the posterior cortex (Fig 6). The distal cut can then be made in the same fashion. Use the osteotome to completely perforate the medial and lateral cortices so that the wedge of bone is easily removed (Figs 7 and 8). Once the wedge has been resected, slowly extend the knee until the gap closes. Next, k-wires are used for the 4.5 partially threaded screws (DePuy-Synthes, Warsaw, IN) to pass medially and laterally in a crossing configuration. The starting point for each k-wire should be slightly distal to the joint line, and slightly anterior to midline. Maintain a more anterior trajectory as the tendency is to aim posterior. A 3.2-mm drill bit is then used to drill bicortically and follow with a 4.5 tap for the proximal cortex. Insert the two 4.5 screws with washers and carefully compress the osteotomy (Fig 9). Check fluoroscopic views carefully to ensure that the posterior cortex did not fracture and that the tibial plateau is intact. If fracture does occur through the posterior cortex or tibial plateau, the two 4.5 screws will likely be insufficient fixation. Consideration should be given to lateral and/or medial periarticular plate fixation. In addition, an InternalBrace (Arthrex) can be used to supplement fixation.
Fig 3.
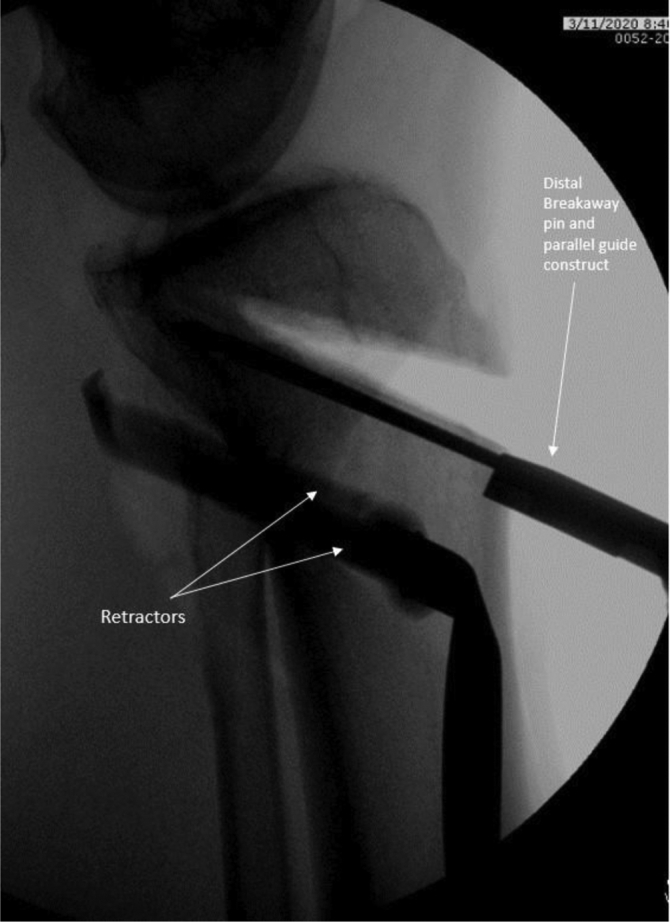
Proximal pin placement. The well positioned lateral radiograph ensures that the pins are collinear and avoids a multi-planar osteotomy.
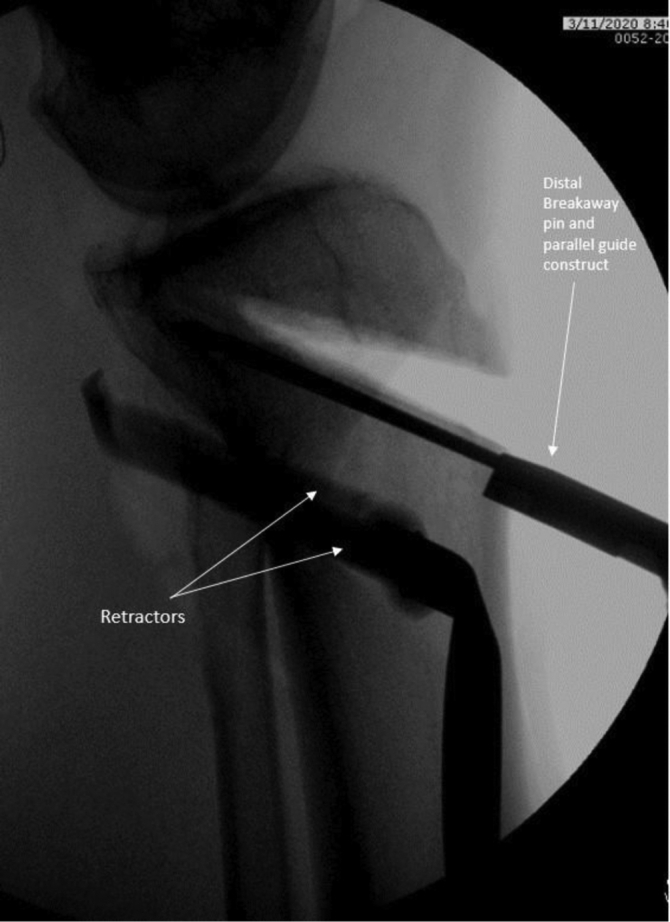
Fig 4.

Parallel guide used for proximal and distal pin placement.
Fig 5.

Osteotomy cutting guide placed on superior pins, with posteromedial and lateral retractors in place.
Fig 6.

After the majority of the proximal cut has been completed with the oscillating saw, the osteotome is used to complete the cut up to, but not through, the posterior cortex.
Fig 7.
Lateral radiograph of osteotomy after resection of bone wedge. Note that the distal pins and osteotomy cutting guide are still in place.
Fig 8.

Wedge of bone removed from proximal tibia, before closure and screw fixation.
Fig 9.

Lateral and AP radiographs of the anterior proximal tibia osteotomy after fixation. Note that there is a retained screw in the femur from a previous failed ACL reconstruction, a metallic TightRope button on the lateral femur from the current ACL reconstruction, as well as a superomedial outflow portal on the AP fluoroscopic view. (ACL, anterior cruciate ligament; ACLR, anterior cruciate ligament reconstruction; AP, anteroposterior.)
ACL Reconstruction
Once the osteotomy fixation has been completed, the ACL reconstruction may be addressed. ACL reconstruction may need to be staged with bone grafting if there is significant tunnel bone loss. A standard ACL reconstruction can be performed if there is sufficient space for tunnel placement proximal to the tibial osteotomy. However, some cases may require an all-inside ACL reconstruction to avoid traversing the osteotomy. In this case, we have performed an all-inside reconstruction with allograft using a FlipCutter (Arthrex) to create our femoral and tibial tunnels. A TightRope (Arthrex) can then be used for femoral fixation (Figs 9 and 10) and a biocomposite RetroScrew (Arthrex) for tibial fixation (Fig 11). Careful attention must be given to avoid graft–tunnel mismatch. A graft that is too short could prevent appropriate fixation or if too long would prevent tensioning.
Fig 10.

Viewing from the anterolateral portal, a RetroScrew fixation with an anteriorly placed RetroScrew diver and large curette used to provide downward force on the screw. A nitinol wire is used to guide the anterior position of the RetroScrew driver. (BTA, bone-tendon autograft.)
Fig 11.

Fixated bone-tendon autograft ACL reconstruction with femoral Tightrope and tibial RetroScrew viewed from the anterolateral portal. (ACL, anterior cruciate ligament; BTA, bone-tendon autograft.)
Rehabilitation
The patient is made nonweight-bearing for a total of 4 weeks. Range of motion is not restricted starting the first postoperative day. At 4 weeks, the patient is progressed to weight-bearing as tolerated.
Discussion
An anterior closing wedge osteotomy to reduce posterior tibial slope has become increasingly recognized and performed to reduce the risk of further revision ACL reconstruction graft failure. Several authors have suggested that a posterior tibial slope of >12° should be considered pathologic.1, 2, 3, 4 This is due to increased anterior tibial translation, which increases the force experienced by the native ACL and ACL graft.1 Therefore, correction of posterior tibial slope is recommended by several authors.4,5,8 At our institution, an anterior wedge closing osteotomy is only performed in the revision ACL reconstruction setting.
Previous studies have demonstrated that an anterior wedge closing osteotomy effectively reduces the risk of ACL reconstruction graft failure.4,8 Sonnery-Cottet et al.8 reported on 5 patients at 32 months postoperatively from a slope-reducing anterior closing wedge osteotomy in combination with an ACL reconstruction. They concluded that an ACL reconstruction in combination with a proximal anterior closing-wedge osteotomy can restore stability and function of the knee as well as prevent re-rupture.
There are several important advantages to our described technique. First, the tibial tubercle is not disrupted and therefore the effect on patellofemoral kinematics is minimized. Breakaway pins allow for the use of a guide, which allows for a precise osteotomy and slope correction. The cross-screw fixation provides a stable construct, which allows for early weight-bearing. The potential risks of this technique include perforation of the posterior cortex. If the posterior cortex is perforated, a plate construct is recommended. Care must be taken to avoid a multiplanar osteotomy, resulting in varus/valgus instability. As with most osteotomies around the knee, the posterior neurovascular structures are in close proximity and must be protected.
Our experience is consistent with previous studies. To date, patients who have undergone an anterior wedge osteotomy with single-stage ACL reconstruction have demonstrated restored knee stability with no cases of re-rupture. Included in this Note are tables that display the advantages and disadvantages of our technique (Table 1) as well as pearls and pitfalls (Table 2). Also included is a video describing our technique (Video 1).
Table 1.
Advantages and Disadvantages of a Tibial Tubercle–Sparing Anterior Closing Wedge Osteotomy
| Advantages | Disadvantages |
|---|---|
| Tibial tubercle not disrupted | Unknown implications of the effect of the osteotomy on the patellofemoral joint |
| Use of a “guide” allows for a precise osteotomy and slope correction | |
| Reliable fixation with the cross-screw fixation technique | |
| Internal brace can be easily used for backup fixation of the wedge |
Table 2.
Pearls and Pitfalls of a Tibial Tubercle–Sparing Anterior Closing Wedge Osteotomy to Correct Pathologic Posterior Tibial Slope.
| Pearls | Pitfalls |
|---|---|
| Position the patient supine with a radiolucent table | Avoid penetrating the posterior cortex |
| Radiolucent triangles can assist with osteotomy | Posterior cortex penetration requires additional fixation |
| Avoid trajectory too close to the tibial plateau to prevent iatrogenic fracture | Unintentional multiplanar osteotomy can lead to varus/valgus malalignment |
| Breakaway pins can be used as a parallel guide for a precise osteotomy | Early weight-bearing can lead to fracture of the posterior cortex |
| The tips of the distal pins should intersect with the tips of the proximal pins | |
| Maintain an anterior trajectory with cross pin K-wire to avoid posterior screw placement |
Footnotes
The authors report that they have no conflicts of interest in the authorship and publication of this article. The views expressed in the manuscript are those of the authors and do not reflect the official poly or position of the Department of the Army, Department of Defense, or the US Government. Full ICMJE author disclosure forms are available for this article online, as supplementary material.
Supplementary Data
This video details a tibial tubercle anterior wedge osteotomy to correct a pathologic posterior tibial slope with cross-screw fixation. The patient should be positioned supine on a radiolucent flat top table. The C-arm should be placed on the contralateral side of the operative extremity. Radiolucent triangles are helpful for positioning. The incision is typically 6 to 8 cm beginning at the tibial tubercle and proceeds distally. The osteotomy start point is just distal to the tibial tubercle aiming toward the proximal tibiofibular joint on the lateral radiograph. Breakaway pins and a parallel guide are used to guide the trajectory of the proximal and distal pins. The use of fluoroscopy is recommended to ensure the pins are coplanar on the lateral view. The distal pins are then inserted in a similar fashion to the proximal pins based on preoperative measurements of the necessary osteotomy size. The tips of the distal pins should intersect the proximal pins. The posterior cortex should not be violated. The breakaway pins are then broken off and the pins are used as a cutting guide for the osteotomy. After the bone wedge is removed, the knee should be extended to close the osteotomy gap. K-wires are then used to guide the trajectory of the 4.5mm cannulated crossing screws for fixation. A 3.2-mm drill is used to drill bicortically, followed by a 4.5-mm tap to facilitate screw passage. An anterior trajectory of the screws is recommended.
References
- 1.Giffin J., Vogrin T., Zantop T., Woo S., Harner C. Effects of increasing tibial slope on the biomechanics of the knee. Am J Sports Med. 2004;32:376–382. doi: 10.1177/0363546503258880. [DOI] [PubMed] [Google Scholar]
- 2.Salmon L.J., Heath E., Akrawi H., Roe J.P., Linklater J., Pinczewski L.A. 20-year outcomes of anterior cruciate ligament reconstruction with hamstring tendon autograft: The catastrophic effect of age and posterior tibial slope. Am J Sports Med. 2018;46:531–543. doi: 10.1177/0363546517741497. [DOI] [PubMed] [Google Scholar]
- 3.Salmon L.J., Refshauge K.M., Russell V.J., Roe J.P., Linklater J., Pinczewski L.A. Gender differences in outcome after anterior cruciate ligament reconstruction with hamstring tendon autograft. Am J Sports Med. 2006;34:621–629. doi: 10.1177/0363546505281806. [DOI] [PubMed] [Google Scholar]
- 4.Dejour D., Saffarini M., Demey G., Baverel L. Tibial slope correction combined with second revision ACL produces good knee stability and prevents graft rupture. Knee Surg Sports Traumatol Arthrosc. 2015;23:2846–2852. doi: 10.1007/s00167-015-3758-6. [DOI] [PubMed] [Google Scholar]
- 5.DePhillipo N.N., Kennedy M.I., Dekker T.J., Aman Z.S., Grantham W.J., LaPrade R.F. Anterior closing wedge proximal tibial osteotomy for slope correction in failed ACL reconstructions. Arthrosc Tech. 2019;8:e451–e457. doi: 10.1016/j.eats.2019.01.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Kızılgöz V., Sivrioğlu A.K., Ulusoy G.R., Yıldız K., Aydın H., Çetin T. Posterior tibial slope measurement on lateral knee radiographs as a risk factor of anterior cruciate ligament injury: A cross-sectional study. Radiogr Lond Engl 1995. 2019;25:33–38. doi: 10.1016/j.radi.2018.07.007. [DOI] [PubMed] [Google Scholar]
- 7.Utzschneider S., Goettinger M., Weber P. Development and validation of a new method for the radiologic measurement of the tibial slope. Knee Surg Sports Traumatol Arthrosc. 2011;19:1643–1648. doi: 10.1007/s00167-011-1414-3. [DOI] [PubMed] [Google Scholar]
- 8.Sonnery-Cottet B., Mogos S., Thaunat M. Proximal tibial anterior closing wedge osteotomy in repeat revision of anterior cruciate ligament reconstruction. Am J Sports Med. 2014;42:1873–1880. doi: 10.1177/0363546514534938. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
This video details a tibial tubercle anterior wedge osteotomy to correct a pathologic posterior tibial slope with cross-screw fixation. The patient should be positioned supine on a radiolucent flat top table. The C-arm should be placed on the contralateral side of the operative extremity. Radiolucent triangles are helpful for positioning. The incision is typically 6 to 8 cm beginning at the tibial tubercle and proceeds distally. The osteotomy start point is just distal to the tibial tubercle aiming toward the proximal tibiofibular joint on the lateral radiograph. Breakaway pins and a parallel guide are used to guide the trajectory of the proximal and distal pins. The use of fluoroscopy is recommended to ensure the pins are coplanar on the lateral view. The distal pins are then inserted in a similar fashion to the proximal pins based on preoperative measurements of the necessary osteotomy size. The tips of the distal pins should intersect the proximal pins. The posterior cortex should not be violated. The breakaway pins are then broken off and the pins are used as a cutting guide for the osteotomy. After the bone wedge is removed, the knee should be extended to close the osteotomy gap. K-wires are then used to guide the trajectory of the 4.5mm cannulated crossing screws for fixation. A 3.2-mm drill is used to drill bicortically, followed by a 4.5-mm tap to facilitate screw passage. An anterior trajectory of the screws is recommended.
This video details a tibial tubercle anterior wedge osteotomy to correct a pathologic posterior tibial slope with cross-screw fixation. The patient should be positioned supine on a radiolucent flat top table. The C-arm should be placed on the contralateral side of the operative extremity. Radiolucent triangles are helpful for positioning. The incision is typically 6 to 8 cm beginning at the tibial tubercle and proceeds distally. The osteotomy start point is just distal to the tibial tubercle aiming toward the proximal tibiofibular joint on the lateral radiograph. Breakaway pins and a parallel guide are used to guide the trajectory of the proximal and distal pins. The use of fluoroscopy is recommended to ensure the pins are coplanar on the lateral view. The distal pins are then inserted in a similar fashion to the proximal pins based on preoperative measurements of the necessary osteotomy size. The tips of the distal pins should intersect the proximal pins. The posterior cortex should not be violated. The breakaway pins are then broken off and the pins are used as a cutting guide for the osteotomy. After the bone wedge is removed, the knee should be extended to close the osteotomy gap. K-wires are then used to guide the trajectory of the 4.5mm cannulated crossing screws for fixation. A 3.2-mm drill is used to drill bicortically, followed by a 4.5-mm tap to facilitate screw passage. An anterior trajectory of the screws is recommended.