

Abstract
Introduction:
Significant traumatic bone loss in developed countries occurs in a high proportion of open fractures ranging from 11.4% to 40%. However, literature from developing countries such as Uganda scarcely documents the prevalence and patterns of traumatic bone loss. Direct trauma and iatrogenic factors have been associated with traumatic bone loss as possible etiologies.
Objective:
The study was aimed at establishing the prevalence and patterns of traumatic bone loss following open long bone fractures, and identifying factors associated with traumatic bone loss among patients presenting to Mulago Hospital within 24 hours of sustaining the injury up to completion of the initial fracture debridement, reduction, and fixation.
Methodology:
It was a prospective cohort study conducted at Mulago Hospital. A total of 136 open long bone fractures were registered and physically examined for traumatic bone loss. Patients who consented were recruited consecutively to participate in the study. Data on the patients’ sociodemographics and fracture patterns were collected using pretested questionnaires and analyzed using Stata version 12.
Results:
From 123 patients, a total of 136 open long bone fractures were registered. The prevalence of traumatic bone loss following open long bone fractures was 26.5%. Of the 36 open long bone fractures with traumatic bone loss, the more common pattern (61.1%) was significant traumatic bone loss (≥ 2.5 cm long). Commercial motorcycle riders (22.0%) and traders (20.3%) were the most common occupations associated with open long bone fractures. Gunshot injuries were the leading cause of traumatic bone loss in open long bone fractures.
Conclusion:
Our setting has a high prevalence of traumatic bone loss among open long bone fractures with the majority occurring in Gustilo type IIIB injuries of the tibia. The likelihood of traumatic bone loss is higher in open fractures caused by gunshots.
Keywords: nonsignificant traumatic bone loss, open long bone fractures, significant traumatic bone loss, traumatic bone loss
1. INTRODUCTION
In developing countries, open fractures are common and are mostly due to the ever increasing number of vehicular road traffic crashes, communal clashes, and civilian gunshot injuries.[1,2] These open fractures may be complicated by bone defects and bone loss which can result directly from the acute trauma or as a necessary treatment component of surgical debridement.[3] The bone defects that arise often have severe negative long-term impact on patients’ lives and present complex treatment challenges.[3–5]
In Uganda, the prevalence of trauma patients who are admitted at Mulago Hospital with open long bone fractures as well the patterns of open long bone fractures presenting with traumatic bone loss is unknown. Furthermore, the extent of bone loss resulting from surgical debridement as part of the standard treatment regimen is also unknown. It is therefore difficult to understand the magnitude of the problem. Since the published literature does not clearly define the worldwide prevalence of traumatic bone loss,[6,7] a study on traumatic bone loss in Uganda could inform the international trauma community about the potential prevalence of bone loss in other countries and the kind of occupations that are associated with open long bone fractures with traumatic bone loss. These data would encourage more research and resource allocation by policy makers internationally toward better management of this condition.
The objectives of this study are to estimate the prevalence of traumatic bone loss following open long bone fractures among patients presenting to Mulago Hospital, and to describe and analyze the clinical patterns of open long bone fractures with traumatic bone loss among patients admitted at Mulago Hospital within 24 hours of sustaining the injury up to completion of the initial fracture debridement, reduction, and fixation.
2. Methods
We carried out a prospective cohort study of traumatic bone loss in open long bone fractures that presented to Mulago Hospital in Kampala, Uganda, from October 2013 to January 2014. All study participants were counselled about the nature of the study procedure and the need for additional assessment that would prolong the surgical procedure. Any risks involved due to the prolonged surgical time such as prolonged anaesthesia, risk of infection, and risk of additional blood loss were explained to the participants.
A total of 123 patients with open long bone fractures who presented to Mulago Hospital during the study period consented and were included in the study. We excluded patients with closed fractures, previous pathological disease conditions, and previous open fractures of the fractured and/or the contralateral long bone that had complications such as chronic infection, nonunion and malunion. We also excluded physiologically unstable moribund patients who first required management in the intensive care unit within 24 hours of their injuries because they could not tolerate anaesthesia during their initial surgery and measurement of bone loss. We also excluded patients with bilateral segmental or circumferential traumatic bone loss that resulted in bilateral limb shortening thereby eliminating use of the contralateral long bone as an accurate reference point for restoring of the original length the affected bone, and finally uncooperative patients who had unclear identification and causative circumstances surrounding their injury (Fig. 1).
Figure 1.
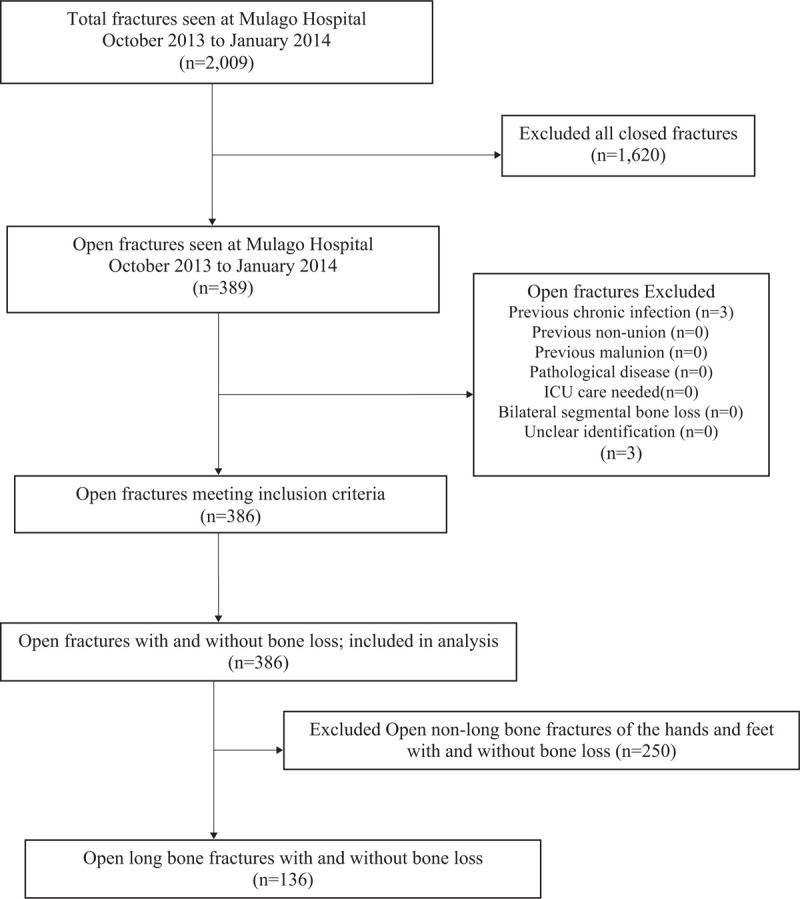
Screening profile for open long bone fractures with traumatic bone loss seen at Mulago Hospital.
Prospective enrollment of study participants was done consecutively for all patients with open long bone fractures who reported to the accident and emergency unit and 3B emergency surgical ward who met the selection criteria. Their data were collected within 24 hours after the injury initially at the time of admission and after each patient's initial fracture debridement, reduction, and fixation. This was later followed by analysis.
Following resuscitation, all patients who provided consent or assent to participate in the study were enrolled and data were then collected using a questionnaire. Questionnaires used had previously been pretested and piloted by the principal investigator and 2 of his research assistants to test for reliability and internal validity (alpha >80).
The participants’ histories were taken and physical examination of their injuries was done. Preoperative plain radiographs of the affected long bones were taken in anteroposterior and lateral views and assessed with the orthopaedic team on duty, in preparation for irrigation and debridement and open reduction and fixation of the open long bone fractures.
After thorough irrigation and debridement, the patients’ open long bone fractures were assessed and classified according to the Gustilo classification.[8,9] Subsequent open reduction and fixation of the fractures was then done.
Finally, measurement of the length of the bone defect caused by the injury and/or surgical debridement was done intraoperatively using a vernier caliper to determine the significance of the bone loss. The longest dimension of the defect that was parallel to the anatomical axis of the long bone was measured using a vernier caliper and taken as the length of the bone defect in centimeters.
2.1. Sample size
Using a sample size formula by Daniel (1999),[10] the sample size calculated was 380 fractures.
N = Z2P (1 – P)/d2
where N= sample size,
Z = Standard normal deviate at 95% confidence interval corresponding to 1.96
P = expected prevalence or proportion of the condition of interest: results of a pilot study conducted in the Accident and Emergency department at Mulago Hospital, open long bone fractures and nonlong bone fractures of the hands and feet, so P = 34%
1–P = the probability of not having an open fracture, so 1–P = 66%
d = precision or degree of accuracy= 0.05.
Substituting for the formula above,
=344.8220
N=345
We added 10% of the calculated sample size to compensate for any loss or non-response, which made it 0.1 × 345 = 34.5
Total sample size was 345 + 34.5 = 379.5
Sample size N was 380 fractures.
The numerator was the number of open long bone fractures and nonlong bone fractures of the hands and feet with traumatic bone loss and the denominator included all open long bone and nonlong bone fractures of the hands and feet.
This sample size was calculated for all open long bone fractures and nonlong bone fractures of the hands and feet. However for purposes of this study, we analyzed only open long bone fractures, which were 136.
Sociodemographic characteristics such as age, gender, and occupation at the time of acquiring the open long bone fracture were predictor variables. The type of long bone as well as the causes of injury categorized as a binary variable, that is high-energy or low energy trauma, were also predictor variables. The type of open long bone fracture based on the Gustilo classification was a multicategorical variable.
The outcome variable was traumatic bone loss following open long bone fractures (≥0.1 cm in length) measured within 24 hours of the injury after the initial fracture debridement.
With the help of medical statisticians, all questionnaires were double entered into a computer using EpiData version 3.1, with range, consistency, and validation checks embedded that aided data cleaning.
Stata version 12 was used for all data analysis. A descriptive analysis of the baseline characteristics of the study population was done. Frequencies and proportions of traumatic loss following open long bone fractures and the distribution of clinical presentations among patients were computed taking the total number of study participants as the denominator. Results were presented in frequency tables and text.
2.2. Ethical considerations
Permission to conduct the study was granted from the Department of Orthopaedics, the School of Medicine Research and Ethics Committee, and Mulago Hospital Ethics and Research committee.
Informed consent was obtained from all adult patients ≥18years. Informed consent was also obtained from caretakers of children < 7 years. All children aged ≥ 7 years were included in the study after they had assented to take part in it.
3. Results
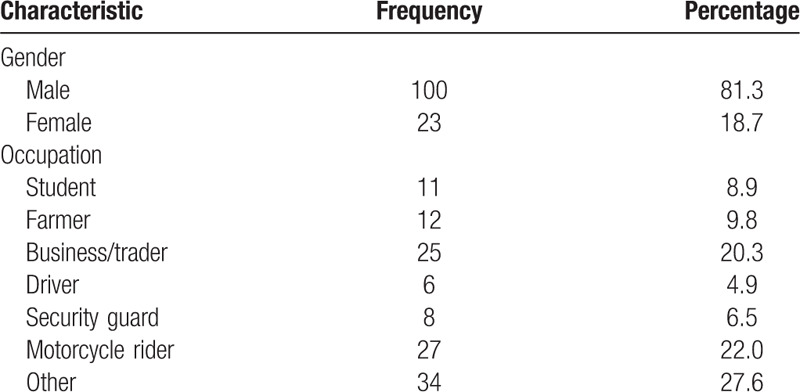
A total of 123 patients consented and participated in the study. The male-to-female ratio was 4:1. The majority of patients with open long bone fractures were commercial motorcycle riders (22.0%) and traders (20.3%) (Table 1). Occupations represented by others were individually of a low percentage (range 1%–4%). The most affected age group was between 20 and 29 years (48.0%), and the mean age was 30.8 ± 11 years.
Table 1.
Demographic characteristics of the respondents presenting with open long bone fractures.
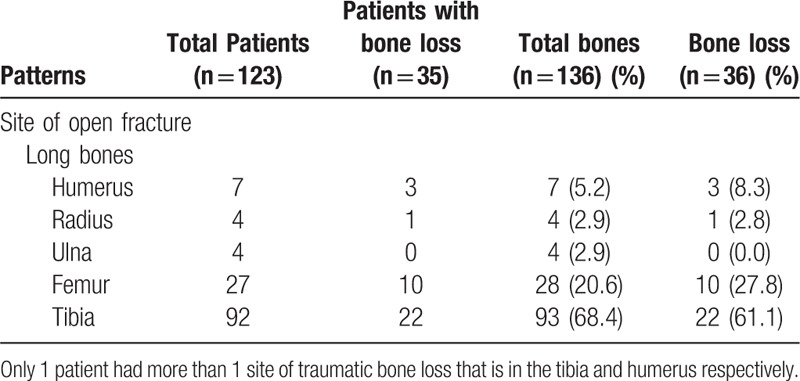
The most frequent site of open long bone fractures among patients was the tibia (93/136) and the least frequent were the radius and ulna (Table 2). The tibia, femur, and humerus were the most reported bones with open long bone fractures accounting for 68.4%, 20.6%, and 5.2%, respectively. There were 136 open long bone fractures registered in the 123 patients. Of the 136 open long bone fractures, 36 had traumatic bone loss giving a prevalence of 26.5%. The mean length of traumatic bone loss was 4.8 cm (SD 5.5 cm) and ranged from 1.0 to 29.0 cm. The mean lengths of traumatic bone loss by site were tibia 5.8 cm (SD 5.7 cm), femur 3.8 cm (SD 2.4 cm), and humerus 2.7 cm (SD 0.6 cm), respectively. The most frequent site of bone loss was the tibia (Table 2).
Table 2.
Site of open long bone fractures.
We had 123 patients with open long bone fractures. Of the 123 patients, 112 had 1 open long bone fracture, 9 patients had 2 open long bone fractures, and 2 had 3 open long bone fractures. Similarly 114 out of 123 patients had 1 open long bone fracture per extremity, 7 patients had 2 open long bone fractures per extremity, and 2 had 3 open long bone fractures per extremity.
In total, we had 35 patients with bone loss but of those 1 had more than one site of bone loss.
3.1. Patterns of traumatic bone loss
Significant traumatic bone loss (2.5 cm or more in length) was the most common pattern (61.1%) compared to nonsignificant traumatic bone loss that is bone loss of less than 2.5 cm in length (38.9%).
Out of 136 open long bone fractures, the majority were caused by motorcycle—motor vehicle accidents (40 accidents, 29.4%). Other common causes of injury included; 20 motor vehicle-pedestrian accidents (14.7%), 17 motorcycle—motorcycle accidents (12.1%), 15 gunshot injuries (11.0%), and 25 other causes of injury (18.4%).
Of the 35 patients with traumatic bone loss, 9 resulted from gunshot injuries, 8 resulted from motorcycle—motor vehicle accidents, and 9 resulted from other causes of injury including assault, self-inflicted injuries.
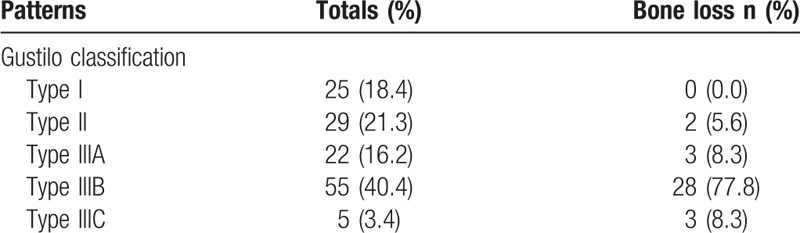
The majority of open fractures were Gustilo type IIIB at 55 (40.4%), and the least were Gustilo type IIIC at 5 (3.4%) (Table 3).
Table 3.
Classification of open fractures.
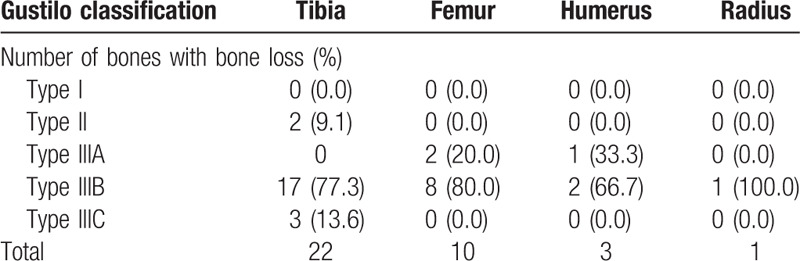
Among open long bone fractures of the lower extremities with bone loss, 17 (77.3%) of the tibias were of Gustilo type IIIB and 8 (80.0%) of the femurs were of Gustilo type IIIB, respectively (Table 4).
Table 4.
Gustilo classification of open fractures of the tibia, femur, humerus, and radius with bone loss.
4. Discussion
This study found a high estimated prevalence of traumatic bone loss following open long bone fractures at Mulago Hospital in Kampala, Uganda. It also found that significant traumatic bone loss was common in our setting. Gunshot injuries were the leading cause of traumatic bone loss in open long bone fractures in our setting. Most open long bone fractures in this study were Gustilo grade IIIB injuries due to the large volume of high-energy trauma that we see at Mulago Hospital.
4.1. Limitations
Subjective errors might have arisen when reading the preoperative radiographs and a lesion might have been missed.
Small fragments of bone that were lost in comminuted fractures might have been missed during the intraoperative assessment of the open long bone fractures.
Some types of injuries sustained, seasonal effects on the frequency, and patient outcome information were missed due to the short period of data collection.
This study did not differentiate between the amount of bone loss present presurgery versus postdebridement; hence no conclusion could be made as to relative contribution of extensive surgical treatment versus the extent of bone loss present immediately following the traumatic event.
4.2. Relation to previous research
In this study, the prevalence of traumatic bone loss was 26.5%, which is higher than the prevalence of 11.4% found in Edinburgh, Scotland,[6] and that found in Finland at 4%.[11] However, Robinson et al[7] reported that worldwide the overall prevalence of traumatic bone loss in open fractures ranged from 17% to 40%, in which range our prevalence lies. In developed countries, the low prevalence of traumatic bone loss in open long bone fractures as shown in the literature was most likely due to fewer high-energy injuries experienced by the populations of these countries. These injuries usually resulted from sports injuries such as skiing and road traffic accidents in cars as opposed to motorcycles. The low incidence of gunshot-related injuries of the limbs among the populations of these developed countries further contributed to their low prevalence of traumatic bone loss in open fractures.[12–14] However, in this study the high prevalence of traumatic bone loss reflected a high incidence of open long bone fractures and high-energy injuries among the population of this developing country, commonly caused by motorcycle accidents, motor vehicle accidents and civilian gunshot injuries.
Wound debridement also contributed to bone loss as it was done in all patients.
Surgical debridement is a standard of care for open fractures that follows a protocol that was also used in this study that involves removal of devitalised segments of bone.[15] Some studies have identified debridement as a cause of traumatic bone loss.[3,6,15–18]
The mean length of traumatic bone loss in open long bone fractures that was found in this study was similar to that of studies done in Turkey and India, where the mean lengths of the traumatic bone defects were 6.8 cm and 8.9 cm, respectively.[17,19] This similar finding resulted from the common site of open fractures with bone loss that was the tibia and the common cause of injury that was high-velocity gunshot injuries in these studies. The range of traumatic bone loss in long bones that was reported in this study was larger than that of studies done in Turkey and India where the ranges of the traumatic bone defects in long bones were 4 to 16 cm and 5 to 17 cm, respectively.[17,19] These differences in ranges of length of traumatic bone loss in long bones might have been due to the smaller number of patients with traumatic bone loss that were assessed in the Turkish and Indian studies that were 19 and 25 patients, respectively.[17,19]
This study noted findings similar to those documented by Kigera and Shamim[20] in Kampala who reported that the majority of open fractures of the extremities were sustained in road traffic crashes (96%), of which motorcycles (52.1%) dominated motorcars (43.8%). They further reported that most of the victims were pedestrians (37.5%).[20] In our study, the variety of road users who were prone to open long bone fractures reflected a low public awareness on safe road use.
This study noted findings similar to those of Kesemenli et al[17] who noted that traumatic bone defects developed in the majority of patients (68%) as a result of high-velocity gunshot injuries. In Beirut, Lebanon, the results from a study by Dagher and Roukoz[21] showed that gunshot injuries (56%) were similarly the major cause of traumatic bone loss in open fractures.
High-velocity missile injuries are caused by bullets fired from weapons with a muzzle velocity exceeding 300 m/s such as the AK 47 assault rifle. This rifle is common in our environment, has a muzzle velocity of 2300 feet per second (701 m/s), and a rate of fire of 600 rounds per minute.[18] The fracture caused by such a missile is due to the high-energy transfer which occurs at a small area of impact causing shattering of bone and cavitation of the soft tissues.[18,22] As a result of this extensive damage, most of these fractures belong to Gustilo grade III injuries.[8,18] The gunshot injuries reported in this study were therefore high-energy injuries, which is in agreement with other studies in Italy, Lebanon, Turkey, Cote d’Ivoire, and Scotland and were shown to produce open long bone fractures with traumatic bone loss.[6,17,21,23–25]
Open fractures have traditionally been classified by the Gustilo and Anderson classification.[8,9,20] This study reported similar findings to those of Keating et al[6] in Scotland and Yazar et al[26] in China who found that bone loss in open long bone fractures mostly occurred in the tibia (68% and 79%, respectively) and the majority of injuries were Gustilo grade IIIB. These findings were attributed to the subcutaneous position of the tibia, which predisposes it to open fractures and easy extrusion of bone. Other studies with similar findings included Kesemenli et al[17] in Turkey (63%), El-Sayed et al[27] in Egypt (67%), and Lawal et al[28] in Nigeria (83%).
The short period of data collection was noted as a limitation to the study as patient outcome information following treatment was missed.
4.3. Implications
The orthopaedic team at Mulago Hospital should be trained to have a high index of suspicion for traumatic bone loss when handling open long bone fractures due to the high prevalence observed.
Significant traumatic bone loss contributes to reoperation and functional, physical, and socioeconomic issues.[29–31] We have identified a significant rate of high-energy fractures from both gunshot injuries and road traffic accidents including a high proportion involving motorcycles.[32–36] There is a need to conduct awareness campaigns concerning safety rules that are targeted at high-risk groups to reduce the incidence of traumatic bone loss due to gunshot injuries and road traffic accidents.
A further study is necessary to determine if bone loss in long bones was in the shaft or metaphyseal region.
5. Conclusion
Our setting has a high prevalence of traumatic bone loss among open long bone fractures with the majority occurring in Gustilo type IIIB injuries of the tibia. The likelihood of traumatic bone loss is higher in open long bone fractures caused by gunshots.
Acknowledgments
Participated in writing or technical editing of the manuscript.
Nathan Evaniewd, Brad A. Petrisord, Peter. J. O’Briene, Yunia Mayanjaf. dDivision of Orthopaedics, McMaster University, Hamilton, ON, Canada. eVancouver General Hospital and Health Sciences Center, Division of Orthopaedic Trauma, Vancouver, British Columbia, Canada V5Z 4E3. fScientist at MRC/UVRI and LSHTM Uganda Research Unit.
References
- 1.Chalya PL, Mabula JB, Dass RM, et al. Injury characteristics and outcome of road traffic crash victims at Bugando Medical Centre in Northwestern Tanzania. J Trauma Manag Outcomes. 2012;6:1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Ifesanya A, Omololu A, Ogunlade S, et al. The burden of open fractures of the tibia in a developing economy. Nig J Plast Surg. 2010;6:32–39. [Google Scholar]
- 3.DeCoster TA, Gehlert RJ, Mikola EA, et al. Management of posttraumatic segmental bone defects. J Am Acad Orthop Surg. 2004;12:28–38. [DOI] [PubMed] [Google Scholar]
- 4.O’Hara NN, Mugarura R, Potter J, et al. Economic loss due to traumatic injury in Uganda: the patient's perspective. Injury. 2016;47:1098–1103. [DOI] [PubMed] [Google Scholar]
- 5.Semaya AE, Badawy E, Hasan M, et al. Management of post-traumatic bone defects of the tibia using vascularised fibular graft combined with Ilizarov external fixator. Injury. 2016;47:969–975. [DOI] [PubMed] [Google Scholar]
- 6.Keating JF, Simpson AH, Robinson CM. The management of fractures with bone loss. J Bone Joint Surg Br. 2005;87:142–150. [DOI] [PubMed] [Google Scholar]
- 7.Robinson CM, McLauchlan G, Christie J, et al. Tibial fractures with bone loss treated by primary reamed intramedullary nailing. J Bone Joint Surg Br. 1995;77:906–913. [PubMed] [Google Scholar]
- 8.Gustilo RB, Anderson JT. Prevention of infection in the treatment of one thousand and twenty-five open fractures of long bones: retrospective and prospective analyses. J Bone Joint Surg Am. 1976;58:453–458. [PubMed] [Google Scholar]
- 9.Neubauer T, Bayer GS, Wagner M. Open fractures and infection. Acta Chir Orthop Traumatol Cech. 2006;73:301–312. [PubMed] [Google Scholar]
- 10.Naing L, Winn T, Rusli B. Practical issues in calculating the sample size for prevalence studies. Arch OrofacSci. 2006;1:9–14. [Google Scholar]
- 11.Ristiniemi J, Lakovaara M, Flinkkila T, et al. Staged method using antibiotic beads and subsequent autografting for large traumatic tibial bone loss: 22 of 23 fractures healed after 5–20 months. Acta Orthop. 2007;78:520–527. [DOI] [PubMed] [Google Scholar]
- 12.Mäkitie I, Mattila VM, Pihlajamäki H. Severe vascular gunshot injuries of the extremities: a ten-year nation-wide analysis from Finland. Scand J Surg. 2006;95:49–54. [DOI] [PubMed] [Google Scholar]
- 13.Chalya P, Mchembe M, Gilyoma J, et al. Gunshot injuries: a Tanzanian experience in a Teaching hospital in the Lake Zone. East Cent Afr J Surg. 2011;16:1. [Google Scholar]
- 14.Mohammed A, Edino S, Ochicha O, et al. Epidemiology of gunshot injuries in Kano, Nigeria. Nigerian J Surg Res. 2005;7:296–299. [Google Scholar]
- 15.Hossain N. B. M. Focus on Management of Traumatic Bone Loss. 2011. Available at: http://www.boneandjoint.org.uk/content/management-traumatic-bone-loss. [Google Scholar]
- 16.Griffith MH, Gardner MJ, Blyakher A, et al. Traumatic segmental bone loss in a pediatric patient treated with bifocal bone transport. J Orthop Trauma. 2007;21:347–351. [DOI] [PubMed] [Google Scholar]
- 17.Kesemenli C, Subasi M, Kirkgoz T, et al. Treatment of traumatic bone defects by bone transport. Acta Orthop Belg. 2001;67:380–386. [PubMed] [Google Scholar]
- 18.Khan MA, Hussain R, Khan SH, et al. Open fractures caused by high velocity missiles: the outcome of treatment of 39 fractures followed for 1–3 years. J Pak Med Assoc. 1997;47:274–278. [PubMed] [Google Scholar]
- 19.Chaddha M, Gulati D, Singh AP, et al. Management of massive posttraumatic bone defects in the lower limb with the Ilizarov technique. Acta Orthop Belg. 2010;76:811–820. [PubMed] [Google Scholar]
- 20.Kigera J, Shamim M. Antibiotic prescription patterns in the management of open fractures at Mulago Hospital in Kampala. East Cent Afr J Surg. 2012;17:47–50. [Google Scholar]
- 21.Dagher F, Roukoz S. Compound tibial fractures with bone loss treated by the Ilizarov technique. J Bone Joint Surg Br. 1991;73:316–321. [DOI] [PubMed] [Google Scholar]
- 22.Hull JB. Management of gunshot fractures of the extremities. J Trauma. 1996;40 (3 suppl):S193–S197. [DOI] [PubMed] [Google Scholar]
- 23.Lavini F, Dall’Oca C, Bartolozzi P. Bone transport and compression-distraction in the treatment of bone loss of the lower limbs. Injury. 2010;41:1191–1195. [DOI] [PubMed] [Google Scholar]
- 24.Smith WR, Elbatrawy YA, Andreassen GS, et al. Treatment of traumatic forearm bone loss with Ilizarov ring fixation and bone transport. Int Orthop. 2007;31:165–170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Traore M, Kone S, Kouame M, et al. Reconstruction of post-traumatic bone loss (BL) members: our experience about 27 cases. Open J Orthop. 2016;6:139–143. [Google Scholar]
- 26.Yazar S, Lin CH, Wei FC. One-stage reconstruction of composite bone and soft-tissue defects in traumatic lower extremities. Plast Reconstr Surg. 2004;114:1457–1466. [DOI] [PubMed] [Google Scholar]
- 27.El-Sayed M, El-Hadidi M, El-Adl W. Free non-vascularised fibular graft for treatment of post-traumatic bone defects. Acta Orthop Belg. 2007;73:70–76. [PubMed] [Google Scholar]
- 28.Lawal YZ, Garba ES, Ogirima MO, et al. Use of non-vascularized autologous fibula strut graft in the treatment of segmental bone loss. Ann Afr Med. 2011;10:25–28. [DOI] [PubMed] [Google Scholar]
- 29.D’Agostino P, Stassen P, Delloye C. Post-traumatic bone loss of the femur treated with segmental bone allograft and bone morphogenetic protein: a case report. Acta Orthop Belg. 2007;73:396–399. [PubMed] [Google Scholar]
- 30.Court-Brown CM, Rimmer S, Prakash U, et al. The epidemiology of open long bone fractures. Injury. 1998;29:529–534. [DOI] [PubMed] [Google Scholar]
- 31.Woon CY, Chong KW, Wong MK. Induced membranes—a staged technique of bone-grafting for segmental bone loss: a report of two cases and a literature review. J Bone Joint Surg Am. 2010;92:196–201. [DOI] [PubMed] [Google Scholar]
- 32.Naddumba EK. A cross-sectional retrospective study of Boda Boda injuries at Mulago Hospital in Kampala,Uganda. East Cent Afr J Surg. 2004;9:44–47. [Google Scholar]
- 33.Kigera JWM, Naddumba EK. Patterns of injuries after road traffic crashes involving bodabodas. Ann Afr Surg. 2010;5:12–15. [Google Scholar]
- 34.Kigera J, Nguku L, Naddumba EK. The impact of Bodaboda motor crashes on the udget for clinical services at Mulago Hospital. Kampala East Cent Afr J Surg. 2010;15:57–61. [Google Scholar]
- 35.Tumwesigye NM, Atuyambe LM, Kobusingye OK. Factors associated with injuries among commercial motorcyclists: evidence from a matched case control study in Kampala City, Uganda. PLoS One. 2016;11:2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Todt J, Gautam P, Karonga J, et al. Road safety performance review. Uganda: 2018. [Google Scholar]