

Abstract
Introduction.
Alternative high school (AHS) students typically report higher levels of alcohol and other drug use compared to students attending traditional high schools. Greater use of such drugs as heroin, methamphetamines, and cocaine in this at-risk population may be driven, in part, by a greater latitude of acceptance toward substance use in general, which may accelerate the transition from gateway drugs to hard drugs.
Methods.
777 adolescents (mean age 16.6; 56% female) were recruited from alternative high schools throughout Southern California. To understand the factors that may lead AHS students to use hard drugs, a model was tested in order to determine if AHS students’ latitude of acceptance towards substance use was a mediator between the relationship of past use of gateway drugs and future use of hard drugs.
Results:
Latitude of acceptance was found to be a statistically significant mediator of future hard drug use (b = 0.03, 95% Confidence Intervals = 0.01 to 0.05) among gateway drug users.
Conclusions:
An individual’s latitude of acceptance to various drug use behaviors may be consistent with societal norms. However, after exposure to, or use of, gateway drugs, attitudes that are more permissive toward hard drug use may be encountered, the acceptance of hard drugs may expand, and the use of hard drugs may escalate. Interventions designed to reduce the use of hard drugs among at-risk youth may be more persuasive by crafting messages that are within the latitude of acceptance of the target population and prevent the acceptance of hard drug use.
Keywords: Adolescence, tobacco use, alcohol use, marijuana use, latitude of acceptance, hard drug use, alternative high school, Social Judgment Theory
Introduction
Adolescent substance use remains an area of major concern in public health. Early initiation of these behaviors can cause increased vulnerability to alterations in brain functioning, cognition, and behavior (Ames et al., 2013; Bava et al., 2010; Volkow et al., 2014). Adolescent substance use has been linked to decreased working memory capacity, poor academic performance, impaired memory function, and altered judgement and emotional functioning (Grant et al., 1997; Grenard et al., 2008; Hanson et al., 2014; King et al., 2007; Miller et al., 2007; Squeglia et al., 2009; Sussman, 2001; Volkow et al., 2014). Further, the risk of becoming dependent on substances is greater among adolescents than adults (Deas et al., 2000; Sussman et al., 2008) and the risk of experiencing problems related to drug dependence is greater among individuals who begin using drugs during adolescence (Chen et al., 2009). Despite these known risks, the prevalence of drug use among high school students remains high. A national sample of 44,900 youth found 49% of 12th graders, 46% of 10th graders, and 21% of 8th graders had used an illicit drug in their lifetime (Johnston, 2016).
Individuals who attend alternative high schools (AHS) are typically those who have left traditional high schools (THS) due to any number of negative behaviors, including excessive truancy, poor academic performance, substance use, violence, emotional, or functional problems (Rohrbach et al., 2005; Sussman et al., 1995). The California Legislative Analyst’s Office estimates that about 7% of California high school students are enrolled in an alternative high school program. These students typically come from diverse and underserved backgrounds, and are more commonly identified as low income and English learners compared to students attending traditional high schools. Specifically, enrollment data indicates that students are more likely to be Hispanic (65 percent compared to 51 percent at THS) or black (10 percent compared to 6 percent at THS) (LAO, 2015), or in foster care (de Velasco et al., 2017). A relatively high prevalence of negative health related behaviors has been documented among youth from AHS (Sussman et al., 2014), including higher levels of potential risk factors for engaging in substance use (Johnson, K. et al., 2012), emotional and physical abuse, exposure to violence, and other occurrences that cause them to feel disconnected from mainstream society (Zweig, 2003). Indeed, AHS students were three times more likely than their 11th grade peers in THS to have been in four or more physical fights at school. Nine percent reported being threatened or injured with a weapon more than once, over double the rate of 11th graders statewide (de Velasco et al., 2008).
While no recent national data exists for alcohol, nicotine, and marijuana use among AHS students (Sussman et al., 2014), investigations conducted among these students have shown especially high drug use prevalence rates (Ames et al., 2007; Grenard et al., 2008; Sussman et al., 2014; Sussman et al., 1997; Sussman et al., 2002). For example, prior investigations have found lifetime alcohol (64.9% vs 50.8%), cigarette (70.1% vs 36.3%), and marijuana (53.9% vs 26.2%) use to occur at much higher levels among AHS students than among THS students (Grunbaum et al., 2001). A more recent study conducted among Minnesota alternative and traditional high schools found disparate rates of cigarette (71.6% vs. 37.7%), marijuana (43.9% vs 15.9%), and alcohol use (76.1% vs 57.9%) (Johnson et al., 2013). Similar results among California AHS youth have also been found (Newcomb et al., 1988; Saunders et al., 2001). An investigation by de Velasco and colleagues found that rates of regular and heavy alcohol and drug use were at least two times higher among continuation school students than 11th-grade students in traditional high schools (de Velasco et al., 2008). To better understand and address substance use among this diverse and understudied population, it is important to examine the factors that may influence AHS students’ decision to engage in substance use and to transition from gateway drugs to other illicit substances.
Gateway drugs are substances, such as alcohol, nicotine, and marijuana, that when used by adolescents are thought to increase the risk of transitioning to hard drugs, such as opioids and amphetamines (Kandel, 1975). While the term ‘gateway drug’ and ‘hard drug’ are scientifically imprecise (Janik et al., 2017), previous research has documented a sequence in which tobacco, alcohol, or marijuana are typically used prior to the use of other illicit drugs (Fergusson et al., 2006). While some have investigated the inclusion of other substances (e.g. ecstasy) as a gateway drug (Reid et al., 2007), alcohol, tobacco, and marijuana nevertheless continue to be among the first substances adolescents will experiment with (Johnston et al., 2019). Further, while there is little agreement on what constitutes a ‘hard drug’ (Janik et al., 2017), this work will group all psychoactive substances other than alcohol, tobacco, and marijuana under the category ‘hard drug’ (described in detail in the methods section). Past investigations have found a link between early alcohol (Barry et al., 2016; Kirby et al., 2012), nicotine (Kandel et al., 2014), and marijuana use, and the use of hard drugs later in life (Degenhardt et al., 2010). This transition is of particular concern as the use of these substances typically increases as children progress through adolescence. Among all high school students, the prevalence of past 30-day alcohol use steadily rose from 23.4% of 9th graders to 42.4% of 12th graders (Kann, 2015), and the prevalence of using marijuana within the past 30 days increased from 15.2% of 9th graders to 27.6% of 12th graders (Kann, 2015). Although there is evidence of a causal link between the use of gateway drugs and hard drugs, approximately 75% of teenagers will mature out of drug use in early adulthood (Rohrbach et al., 2005). This may suggest an unknown mechanism mediating the relationship between the use of gateway drugs in adolescence and the future use of hard drugs. To our knowledge, no research conducted among AHS students has used longitudinal data to examine a possible mechanism that may be associated with this transition in substance use, such as attitudes concerning the types of drugs that are socially acceptable.
Latitude of Acceptance
At its most basic, an attitude is an individual’s response, favorable to unfavorable, regarding some sort of object, concept, or behavior (Ajzen et al., 2000). According to seminal work conducted by Fishbein and Azjen, attitude is described as affect or feelings toward a behavior or object – specifically conceptualized as a value-expectancy model (Ajzen et al., 1977, 1980). For example, a person with a positive view toward heroin use, as well as a positive belief regarding the outcome of use, is more likely to engage in that behavior compared to someone with a negative view toward the behavior or a negative belief regarding the outcome of use (Ajzen et al., 1977). Under this framework, only beliefs that are salient to the individual will have a causal impact on attitude, which in turn will exert an influence over behavior (Ajzen, 1985; Ajzen et al., 1980; Fishbein et al., 1974).
The concept of latitude of acceptance used in this work stems from Social Judgement Theory (SJT) and postulates that an individual’s attitude is not based on feelings or affect toward an object or behavior, but instead on the acceptability or unacceptability of the object or behavior. Attitude can range anywhere from completely favorable to completely unfavorable and will change when exposed to new information (i.e. persuasive communication). Along this favorable/unfavorable continuum are categories of positions that can be divided into three distinct regions (Hovland et al., 1957; Sherif et al., 1961). Those attitude positions along the spectrum that an individual rated as acceptable are within the latitude of acceptance, positions rated as objectionable are within the latitude of rejection, and all remaining positions are called the latitude of noncommitment. A key point to this concept of attitude is that as people evaluate new incoming information (persuasive communications), they immediately determine the latitude in which information belongs, and will shift their attitude toward or away that new information accordingly (Sherif et al., 1965). For example, those who hold favorable views of gateway drug use may judge new information received on other drug use as favorable as well, and place this behavior somewhere on their latitude of acceptance spectrum. Additionally, the size of an individuals’ latitude of acceptance/rejection/noncommitment is based on personal involvement one has toward the specific behavior. The more involved an individual is in a behavior, the wider their acceptance spectrum may be toward similar behaviors.
After judging new information as favorable or unfavorable, and placing it somewhere along their acceptance or rejection spectrums, individuals are then thought to attempt to minimize the difference between their own attitude and the attitudes of others that they have judged to fall within their latitude of acceptance (Atkins et al., 1967). In other words, if new information falls within an individual’s own latitude of acceptance, they will perceive it as closer to their own judgement than it actually is, and begin to shift their attitude to align with this new behavior. Thus, if a current gateway drug user is exposed to information regarding hard drug use, they could place this new drug information within their wider latitude of acceptance spectrum, and begin to shift their attitude along the acceptance spectrum in order to minimize the gap between their initial judgement and this new behavior.
Overall, an individual’s acceptance (or rejection) of an opinion or behavior is based on the content, presentation, and the presenter of a message. If an opinion or behavior will be evaluated by someone viewed as a trusted or valued source, the individual will evaluate the statement favorably and may be positively influenced, thus shifting their attitude along their acceptance spectrum (Hovland et al., 1957). Taken together, an individual's attitude toward various drugs may initially be formed consistent with societal norms, but after use of gateway drugs and exposure to new positive communications about other substance use in general, their attitude toward hard drugs may shift.
The primary aim of this study was to assess whether AHS students’ use of gateway drugs and their subsequent use of hard drugs was mediated by their self-reported latitude of acceptance toward drug use (Figure 1). Specifically, it was hypothesized that the use of gateway drugs at the baseline assessment (Time 1) would affect latitude of acceptance one year later (Time 2), which would be associated with hard drug use reported at a two-year follow-up (Time 3).
Figure 1:
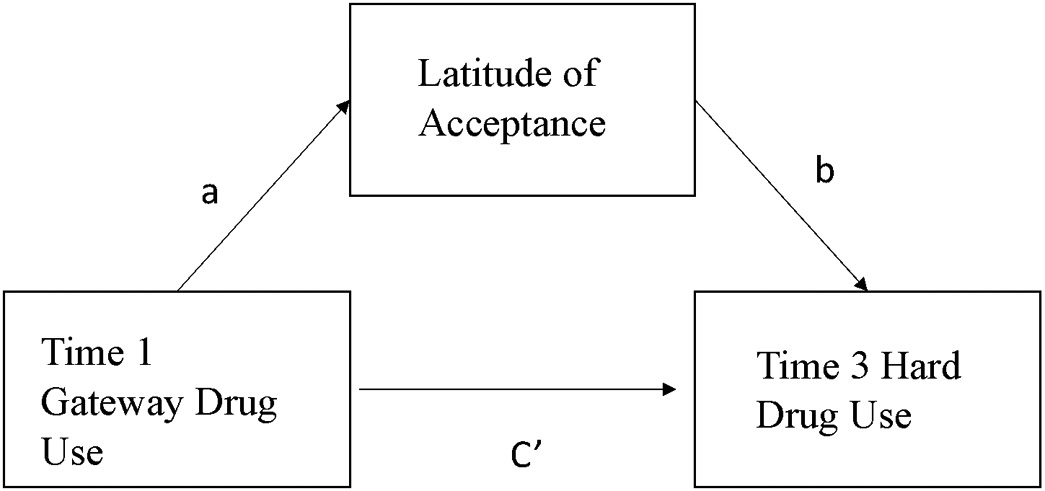
Longitudinal mediation model
Methods
Students from 37 randomly selected alternative high schools located in Southern California were recruited into the study. The composition of AHS consisted of 28 continuation high schools attended by students at risk of not graduating, 6 alternative schools of choice that endeavor to provide students more flexibility in their education, and 3 community day schools that serve high-risk youth including those referred following expulsion or probation (California Department of Education, 2020). All students attending each school were invited to participate. Written assent was obtained from each participating student and consent was obtained from their parent or guardian in accordance with procedures approved by the Claremont Graduate University Institutional Review Board. Participants and parents were informed the study concerned health behaviors, that participants may be asked about potentially illegal actions, and that the study was confidential and voluntary. Students were assessed once per year over three years. A total of 777 students completed the first assessment1. More than half of the students were male (56.1%) and nearly two-thirds were Hispanic (65.2%). Of the remaining participants, 13.6% identified as white, 3.4% identified as black, and 16.3% identified as multiple ethnicities. At baseline, 79.8% of participants had used a gateway drug at least once in the past year and 45.9% had used a hard drug in the past year. The mean age of participants upon enrollment was 16.6 years old (Table 1).
Table 1.
Descriptive statistics for longitudinal cohort of alternative high school students (n=777) assessed over a three-year period.
| All | Male | Female | p value | |
|---|---|---|---|---|
| Sex N(%) | 777(100%) | 436(56.1%) | 341(43.9%) | |
| Age M(SD) | 16.62(1.04) | 16.72(1.06) | 16.49(0.99) | 0.002 |
| Ethnicity N(%) | 0.29 | |||
| Native American/Alaska Native | 3(0.4%) | 3(0.7%) | 0(0) | |
| Asian | 4(0.5%) | 3(0.7%) | 1(0.3%) | |
| Black | 26(3.44%) | 12(2.83%) | 14(4.22%) | |
| Native Hawaiian/Pacific Islander | 4(0.5%) | 4(0.9%) | 0(0) | |
| White | 103(13.6%) | 54(12.7%) | 49(14.8%) | |
| Mixed | 123(16.3%) | 72(16.9%) | 51(15.4%) | |
| Hispanic | 493(65.2%) | 276(65.1%) | 217(65.4%) | |
| W1 Gateway Drug Use Past Year M(SD) | 2.57(2.83) | 2.83(2.97) | 2.24(2.61) | 0.0042 |
| W1 Hard Drug Use Past Year M(SD) | 0.42(1.07) | 0.44(1.14) | 0.39(0.97) | 0.61 |
| W3 Hard Drug Use Past Year M(SD) | 0.36(1.08) | 0.41(1.12) | 0.31(1.04) | 0.38 |
| W2 Latitude of Acceptance M(SD) | −1.68(1.22) | −1.51(1.29) | −1.86(1.10) | 0.0016 |
Procedure
The first assessment was completed at participating schools using a computerized survey administered via portable laptops. Students who completed consent forms were invited to take a computer-based assessment, requiring an average of two hours to complete. Items were ordered so that direct questions about drug use appeared during the latter portion of the assessment. Follow-up assessments were conducted using portable laptop, telephone, and web-based surveys. During the second assessment 283 (60.3%) students completed a survey on a laptop, 110 (23.5%) students completed an automated telephone survey, and 76 (16.2%) students completed a web-based survey. The third assessment comprised 50 (11.1%) laptop-based surveys, 147(32.7%) phone-based surveys, and 253 (56.2%) web-based surveys. Procedures ensured no names appeared on any of the computerized instruments or on the server used to store collected data. Follow-up reminders began approximately 1 year after baseline assessment, and each year thereafter. Participants were mailed a “pre-call” letter informing them that a representative from this project would be calling them within the next couple of weeks. Participants were contacted to remind them to complete the next assessment through mail, email, text message, and phone calls (McCuller et al., 2002). Upon completion, participants received monetary compensation in the form of movie tickets at Time 1 and 2, and a $50 gift card at Time 3.
Measures
Latitude of acceptance.
The measure of latitude of acceptance was adapted from a scale developed by Hovland and colleagues (Hovland et al., 1957). Participants were presented with the statement “How much is it not okay or okay for youth your age to…’. This was followed by a list of options including ‘try smoking cigarettes’, ‘try drinking beer coolers’, and ‘take amphetamine (Adderall, Ritalin) without a doctor’sprescription’. For each drug, students were asked to select from the response options ‘not ok’, ‘neutral’, and ‘ok’. The mean of the total-item scale was computed for each student.
Use of gateway and hard drugs.
Drug use was assessed with a validated measure (Graham et al., 1984; Stacy, 1997; Stacy et al., 1990) previously used to evaluate AHS students’ use of alcohol (Ames et al., 2017), nicotine (Beleva et al., 2019; Pike et al., 2019), and marijuana (Ames et al., 2017). Questions asked about the frequency with which students used ten different substances in the past year. Alcohol, nicotine, and marijuana were classified as gateway drugs while methamphetamines, non-prescribed stimulants (e.g. Ritalin/Aderall), ecstasy, hallucinogens, cocaine/crack, tranquilizers, heroin, and inhalants were classified as hard drugs. The response options for each drug were ‘0 times’, ‘1–10 times’, ‘11–20 times’, ‘21–30 times’, ‘31–40 times’, ‘41–50 times’, ‘51–60 times’, ‘61–70 times’, ‘71–80 times’, ‘81–90 times’, and ‘91+ times’. The mean of the 11-point scale was calculated for the three gateway drugs and the seven hard drugs.
Data Analysis
Descriptive statistics were generated in SAS v9.4. The mediation analysis was performed using the PROCESS macro (Hayes, 2018). A 10,000 iteration bias-corrected bootstrap was selected when estimating the indirect effect because this nonparametric approach has consistently proven to be a powerful test of mediation (Fritz et al., 2007; Mackinnon et al., 2004). In all subsequent analyses, the primary predictor was gateway drug use (tobacco, alcohol, and marijuana) at baseline, the primary outcome was hard drug use (methamphetamines, ecstasy, hallucinogens, cocaine/crack, tranquilizers, heroin, and inhalants) at the three-year follow-up. The mediation variable under investigation was latitude of acceptance at time 2– defined as the participants’ view of various drugs rated on a positive to negative scale. Covariates included in the model consisted of age, any hard drug use at baseline, latitude of acceptance at time 1, and gender. Hard drug use at baseline was included in the model to ensure any epiphenomenon or spurious associations between hard drug use, the mediator, and the outcome variable were properly accounted for (Hayes, 2009; Hayes, 2018; Hayes et al., 2013). These present threats to validity, and can call into question the underlying causal claim of the mediation pathway (Hayes, 2018). Mean values of gateway drug use, hard drug use, and latitude of acceptance were calculated to use as variables in the model. Model analysis followed mediation procedures with bias-corrected bootstrap confidence intervals of mediation effects described by Hayes (Hayes, 2018). The PROCESS macro (Hayes, 2018) does not output a t-statistic or p-value for the indirect effect, but bootstraps the indirect effect and outputs a 95% confidence interval. If the interval does not include zero, then the indirect effect is statistically significant at the .05 level. Bootstrap confidence intervals have been used to calculate significance as they better respect the irregularity of the sampling distribution of the product term reflecting the indirect effect, yield inferences that are more likely to be accurate, and have higher power than most alternatives (Hayes, 2018; Mackinnon et al., 2004).
Due to the nested nature of data, intraclass correlations (ICC) were estimated to determine the degree of variability in drug use within a school compared to variability across schools. Analysis indicated that ICCs were relatively low for both gateway drug use and hard drug use, which suggests that school-level effects did not need to be incorporated into the mediation model (Murray et al., 2004). Specifically, ICCs for Time 1, 2, and 3 gateway drug use were .026, .001, and .011, and for Time 1, 2 and 3 hard drug use were .000, .008, and .021 respectively. An analysis of missing data revealed that students who did not complete the second or third assessment were significantly older at the first assessment (16.8 vs 16.4 , p < .01) and reported greater alcohol use in the past year (3.7 vs 3.2, p = .04), but were not significantly different on other indicated measures. To avoid biased parameter estimates, multiple imputation methods were implemented with PROC MI (Allison, 2001) and used to generate 40 imputed data sets (Graham et al., 2007; Schlomer et al., 2010). Imputed data was included in the mediation analysis and results were summarized with PROC MIANALYZE.
Results
Parameter estimates from the first mediation model (Table 2) indicated that the direct effect of gateway drug use on subsequent hard drug use was not statistically significant (b = 0.01, 95% Confidence Intervals [95% CI] = −0.02 to 0.04). However, the indirect effect was statistically significant (b = 0.03, 95% CI = 0.01 to 0.05) as was the total effect (b = 0.04, 95% CI = 0.01 to 0.07)2. This suggest that students’ latitude of acceptance toward drug use at the second assessment fully mediated the relationship between gateway drug use at the first assessment and hard drug use at the third assessment. As a sensitivity analysis, the mediation analyses were rerun with non-imputed data. Results from a complete case analysis indicated the mediation pathway was statistically significant (b = 0.03; 95% CI: 0.00 to 0.06).
Table 2:
Parameter estimates from model examining mediation effect of latitude of acceptance.
| Parameter Estimate |
SE | 95% CI | |
|---|---|---|---|
| Total Effect | 0.04 | 0.02 | 0.01-0.07 |
| Direct Effect | 0.01 | 0.02 | −0.02-0.04 |
| Indirect Effect | 0.03 | 0.01 | 0.01-0.05 |
Note: Age, gender, LOA scores and hard drug use at the first assessment were included in the model as covariates.
Discussion
The current study is the first to investigate whether latitude of acceptance towards substance use mediated the relationship between past use of gateway drugs and future use of hard drugs among a population of AHS students. The results showed that the predictive effect of gateway drug use on hard drug use was fully mediated by the construct of latitude of acceptance.
The results from the current investigation suggests that an individual’s position on an attitude dimension (Hovland et al., 1957; Sherif et al., 1961) may have a significant association with future behavior. Although only a limited number of studies have explored this theory of attitude in relation to substance use, there is previous evidence compatible with the current findings. For example, a study by Atkins and colleagues (Atkins et al., 1967) investigated college students and their attitude toward the introduction of a fraternity system on campus. Results indicated that participants who perceived a persuasive communication as falling within their latitude of acceptance showed significantly greater change of their own position in the direction of the communication. Another study conducted by Deaux and Bieri tested attitudes toward masculinity and femininity among college students. This work suggested that participants who judged another individual to be within their latitude of acceptance on masculine and feminine constructs changed their own position significantly more than participants who judged the individual to be outside their latitude of acceptance (Deaux et al., 1967). A more recent investigation conducted by Smith and colleagues (Smith et al., 2006) used a tailored message based on individuals’ latitudes of acceptance and noncommitment to significantly reduce the number of drinks consumed at college parties. Specifically, they found that messages that fell within an individual’s latitude of noncommitment were successfully able to alter attitudes related to perception of peer alcohol consumption. Finally, a study conducted to measure the effects message quality had on attitude change found that individuals with wide latitudes of acceptance (i.e. low involvement in message content), were more likely to be persuaded by experimental messaging, and thus shift attitudes toward the topic, than those with narrow latitudes of acceptance (i.e. high involvement in message content) (Park et al., 2007).
Research into cognitive processing of information may provide various explanations as to why an adolescent would develop an increased acceptance of drug use. Data indicates early gateway drug use may affect the formation of drug-relevant associations in memory through repeated positive experience (Ames et al., 2017; Barrett et al., 2004; Grenard et al., 2008; Wiers et al., 2006). The more strongly these associations are linked in memory, the easier they are to activate and drive behavior when cues, contexts, or outcomes related to the behavior are experienced or considered (Ames et al., 2017). This effect has been demonstrated in several previous studies across a range of populations and for several types of drugs (Ames et al., 2006; McCusker, 2001; Rooke et al., 2008; Stacy et al., 2010; Wiers et al., 2006). Adolescents with positive drug cognitions may come to view additional drugs more favorably, which in turn could affect future susceptibility to pro-drug messaging from peers. Existing models of drug use behavior have also found peer and family opinions and attitudes to have great influence over adolescent drug use behavior (Allen et al., 2012; Garnier et al., 2002). If students perceived alcohol, nicotine, or marijuana use in their school to be common, they may be more accepting of those behaviors (Eisenberg et al., 2014; Gilreath et al., 2012; Spijkerman et al., 2004), and if these students had a wide latitude of acceptance toward these drugs it could alter their attitude of other, harder substances.
Taken together, these studies suggest that the larger one’s latitude of acceptance the more likely it is the individual will accept persuasive arguments as compatible with their own attitudes, and thus shift their attitude toward the new position. Among AHS students, this may cause adolescents to modify their attitude toward the use of hard drugs and move further along the acceptance spectrum to align with that of peers and family members who use, as well as the perceived norms and use rates of their schools and neighborhoods (Eisenberg et al., 2014; Ennett et al., 2010; Hoffman et al., 2006). When presented with a persuasive message that falls within their current latitude of acceptance, the individual will perceive the new position as closer to their own attitude than it actually is, and thus form a new more positive attitude toward the new behavior (Sherif et al., 1965). These persuasive messages may take many forms, including personal exposure to peer, family, or community use, discussions on the topic with friends or family, as well as estimations of community use or acceptance of use. It is possible this measure of attitude may capture information not typically assessed with other attitudinal frameworks, and help inform new prevention programming aimed at reducing adolescent substance use. For example, future interventions attempting to change behavior may be able to tailor messages so that they fall within the latitude of acceptance, thus being more likely to be viewed as compatible with current attitudes, and thus influence participant behavior. This would be in contrast to attempts to change attitude by modifying values or outcome expectancies. Indeed, when a message that advocates a specific position (e.g. adolescent alcohol use is lower than is commonly believed) falls within the receiver’s latitude of acceptance, it will be viewed more subjectively similar to the receiver’s position, and persuade attitude and behavior change beyond what would have occurred from an objective assessment of the message’s content (Dillard et al., 2007). Interestingly, the reverse would be true as well; if an intervention’s content falls within an individual’s latitude or rejection, it may be deemed as unbelievable or irrelevant, and otherwise dismissed. This may account for some of the failures of past anti-drug interventions that use fear tactics to persuade behavior change. Messages are deemed unbelievable, falling within the latitude of rejection, thus failing to change attitude or behavior.
Limitations
Although the theoretical foundations of the concept of a latitude of acceptance are well-established in Social Judgement Theory, and the practical utility of the theory is promising, several limitations to the current investigation should be noted. First, AHS students constitute an at-risk population with numerous mental and behavioral health issues which limits generalizability to other, at-risk populations (Johnson, K.E. et al., 2012). Second, as AHS typically have students enrolled for less than a year, as well as the high-risk nature of this population, high levels of attrition (41.7%) were observed which may have impacted observations between each year long assessment period. While extensive follow-up and tracking procedures (McCuller et al., 2002) and the use of standard techniques for handling missing data (Allison, 2001) were employed, parameter estimates may have been biased by the dropout among participants who were older at the baseline assessment and therefore may have reported different levels of hard drug use at subsequent follow-up assessments. Further investigation among this population may be warranted in order to enhance generalizability to other diverse, at-risk populations. Third, use of this theoretical framework has not been studied in depth among diverse adolescent populations at-risk for substance use. Therefore, it remains possible that other unknown mechanisms may be involved which influence adolescent attitudes toward substance use. Further, under this construct it is assumed that persuasive communication is inherent to attitude change, however this construct was not measured directly in this work. Yet, the theory under study has shown predictive utility in past investigations of attitude change and behavior in a variety of populations and therefore may have relevance to understanding and addressing adolescent substance use. Future research could measure specific types of communication adolescents receive, as well as where specifically a behavior falls along their acceptance or rejection spectrum. Finally, the effect sizes observed were small. Still, given the addictive properties of such hard drugs as heroin, methamphetamines, and cocaine, even a small increase in use may have detrimental consequences on long-term health behaviors of adolescents. Further research into the relationship between latitude of acceptance and drug use behavior among AHS students is warranted given the potential for enhancing the efficacy of large-scale interventions that may lead to a substantial improvement in population-level health outcomes.
Conclusion
This study examined the mediating effect of latitude of acceptance on the relationship between past gateway drug use and future hard drug use among a population of at-risk adolescents. The analyses suggest that a wider acceptance of substance use, in conjunction with prior use of gateway drugs, may play a significant role in the subsequent use of hard drugs, including opioids and stimulants. Given the rising rates of hard drug use in the United States, this study may assist in the development of intervention strategies that can reduce the risk for substance use disorders by tapping into a key component of attitude change.
Acknowledgments
Role of Funding Sources
This research was supported by grants from the National Institute on Drug Abuse (DA023368, DA024659, DA024772) and the National Institute on Alcohol Abuse and Alcoholism (AA017996). NIDA and NIAAA had no role in the design of the study, collection, analysis and interpretation of data, or in the writing of the report.
Footnotes
Disclosure of potential conflicts of interest
The authors declare that they have no conflict of interest.
Research involving Human Participants and/or Animals
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Claremont Graduate University Institutional Review Board (IRB00001114) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study
447 participants completed the Time 2 assessment and 449 participants completed the Time 3 assessment.
Results are substantively similar when analysis with imputed dataset excludes students who reported hard drug use at baseline (BootCI: 0.009-0.015).
Publisher's Disclaimer: This Author Accepted Manuscript is a PDF file of a an unedited peer-reviewed manuscript that has been accepted for publication but has not been copyedited or corrected. The official version of record that is published in the journal is kept up to date and so may therefore differ from this version.
References
- Ajzen I (1985). From Intentions to Actions: A Theory of Planned Behavior. In Kuhl J & Beckmann J (Eds.), Action Control (pp. 11–39). Berlin, Heidelberg: Springer Berlin Heidelberg. [Google Scholar]
- Ajzen I, & Fishbein M (1977). Attitude-behavior relations: A theoretical analysis and review of empirical research. Psychological Bulletin, 84(5), 888–918. doi: 10.1037/0033-2909.84.5.888 [DOI] [Google Scholar]
- Ajzen I, & Fishbein M (1980). Understanding attitudes and predicting social behavior: Prentice-Hall. [Google Scholar]
- Ajzen I, & Fishbein M (2000). Attitudes and the Attitude-Behavior Relation: Reasoned and Automatic Processes. European Review of Social Psychology, 11(1), 1–33. doi: 10.1080/14792779943000116 [DOI] [Google Scholar]
- Allen JP, Chango J, Szwedo D, Schad M, & Marston E (2012). Predictors of susceptibility to peer influence regarding substance use in adolescence. Child Dev, 83(1), 337–350. doi: 10.1111/j.1467-8624.2011.01682.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Allison PD (2001). Missing Data. Thousand Oaks, CA: Sage University. [Google Scholar]
- Ames SL, Franken IH, & Coronges K (2006). Implicit cognition and drugs of abuse. In Wiers RW & Stacy AW (Eds.), Handbook of implicit cognition and addiction (pp. 363–378). Thousand Oaks: SAGE Publications. [Google Scholar]
- Ames SL, Grenard JL, Stacy AW, Xiao L, He Q, Wong SW, … Bechara A (2013). Functional imaging of implicit marijuana associations during performance on an Implicit Association Test (IAT). Behav Brain Res, 256, 494–502. doi: 10.1016/j.bbr.2013.09.013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ames SL, Grenard JL, Thush C, Sussman S, Wiers RW, & Stacy AW (2007). Comparison of indirect assessments of association as predictors of marijuana use among at-risk adolescents. Exp Clin Psychopharmacol, 15(2), 204–218. doi: 10.1037/1064-1297.15.2.218 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ames SL, Xie B, Shono Y, & Stacy AW (2017). Adolescents at risk for drug abuse: a 3-year dual-process analysis. Addiction, 112(5), 852–863. doi: 10.1111/add.13742 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Atkins AL, Deaux KK, & Bieri J (1967). Latitude of acceptance and attitude change: empirical evidence for a reformulation. J Pers Soc Psychol, 6(1), 47–54. doi: 10.1037/h0024527 [DOI] [PubMed] [Google Scholar]
- Barrett LF, Tugade MM, & Engle RW (2004). Individual differences in working memory capacity and dual-process theories of the mind. Psychol Bull, 130(4), 553–573. doi: 10.1037/0033-2909.130.4.553 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barry AE, King J, Sears C, Harville C, Bondoc I, & Joseph K (2016). Prioritizing Alcohol Prevention: Establishing Alcohol as the Gateway Drug and Linking Age of First Drink With Illicit Drug Use. J Sch Health, 86(1), 31–38. doi: 10.1111/josh.12351 [DOI] [PubMed] [Google Scholar]
- Bava S, & Tapert SF (2010). Adolescent brain development and the risk for alcohol and other drug problems. Neuropsychol Rev, 20(4), 398–413. doi: 10.1007/s11065-010-9146-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beleva Y, Pike JR, Miller S, Xie B, Ames SL, & Stacy AW (2019). Share of Advertising Voice at the Point-of-Sale and Its Influence on At-Risk Students' Use of Alternative Tobacco Products. Nicotine Tob Res, 21(7), 903–910. doi: 10.1093/ntr/nty152 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chen CY, Storr CL, & Anthony JC (2009). Early-onset drug use and risk for drug dependence problems. Addict Behav, 34(3), 319–322. doi: 10.1016/j.addbeh.2008.10.021 [DOI] [PMC free article] [PubMed] [Google Scholar]
- de Velasco JR, Austin G, Dixon D, Johnson J, McLaughlin M, & Perez L (2008). Alternative education options: A descriptive study of California continuation high schools. San Diego: California Alternative Education Research Project, San Diego University. [Google Scholar]
- de Velasco JR, & Gonzales D (2017). Accountability for Alternative Schools in California. Retrieved from Sacramento, CA: [Google Scholar]
- Deas D, Riggs P, Langenbucher J, Goldman M, & Brown S (2000). Adolescents Are Not Adults: Developmental Considerations in Alcohol Users. Alcoholism: Clinical and Experimental Research, 24(2), 232–237. doi: 10.1111/j.1530-0277.2000.tb04596.x [DOI] [PubMed] [Google Scholar]
- Deaux KK, & Bieri J (1967). Latitude of acceptance in judgments of masculinity-femininity1. Journal of Personality, 35(1), 109–117. doi: 10.1111/j.1467-6494.1967.tb01418.x [DOI] [PubMed] [Google Scholar]
- Degenhardt L, Dierker L, Chiu WT, Medina-Mora ME, Neumark Y, Sampson N, … Kessler RC (2010). Evaluating the drug use "gateway" theory using cross-national data: consistency and associations of the order of initiation of drug use among participants in the WHO World Mental Health Surveys. Drug Alcohol Depend, 108(1-2), 84–97. doi: 10.1016/j.drugalcdep.2009.12.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dillard JP, Shen L, & Vail RG (2007). Does Perceived Message Effectiveness Cause Persuasion or Vice Versa? 17 Consistent Answers. Human Communication Research, 33(4), 467–488. doi: 10.1111/j.1468-2958.2007.00308.x [DOI] [Google Scholar]
- Eisenberg ME, Toumbourou JW, Catalano RF, & Hemphill SA (2014). Social norms in the development of adolescent substance use: a longitudinal analysis of the International Youth Development Study. J Youth Adolesc, 43(9), 1486–1497. doi: 10.1007/s10964-014-0111-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ennett ST, Foshee VA, Bauman KE, Hussong A, Faris R, Hipp JR, & Cai L (2010). A social contextual analysis of youth cigarette smoking development. Nicotine Tob Res, 12(9), 950–962. doi: 10.1093/ntr/ntq122 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fergusson DM, Boden JM, & Horwood LJ (2006). Cannabis use and other illicit drug use: testing the cannabis gateway hypothesis. Addiction, 101(4), 556–569. doi: 10.1111/j.1360-0443.2005.01322.x [DOI] [PubMed] [Google Scholar]
- Fishbein M, & Ajzen I (1974). Attitudes towards objects as predictors of single and multiple behavioral criteria. Psychological Review, 81(1), 59–74. doi: 10.1037/h0035872 [DOI] [Google Scholar]
- Fritz MS, & Mackinnon DP (2007). Required sample size to detect the mediated effect. Psychol Sci, 18(3), 233–239. doi: 10.1111/j.1467-9280.2007.01882.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Garnier HE, & Stein JA (2002). An 18-year model of family and peer effects on adolescent drug use and delinquency. Journal of Youth and Adolescence, 31(1), 45–56. doi: 10.1023/a:1014085016511 [DOI] [Google Scholar]
- Gilreath TD, Chaix B, King G, Matthews S, & Flisher AJ (2012). Multi-level influence of school norms on tobacco use in South Africa: an ecometric consideration of group differences. Cancer Causes Control, 23 Suppl 1, 27–36. doi: 10.1007/s10552-012-9908-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- Graham JW, Flay BR, Johnson CA, Hansen WB, Grossman L, & Sobel JL (1984). Reliability of self-report measures of drug use in prevention research: Evaluation of the Project SMART questionnaire via the test-retest reliability matrix. J Drug Educ, 14(2), 175–193. [DOI] [PubMed] [Google Scholar]
- Graham JW, Olchowski AE, & Gilreath TD (2007). How many imputations are really needed? Some practical clarifications of multiple imputation theory. Prev Sci, 8(3), 206–213. doi: 10.1007/s11121-007-0070-9 [DOI] [PubMed] [Google Scholar]
- Grant BF, & Dawson DA (1997). Age at onset of alcohol use and its association with DSM-IV alcohol abuse and dependence: results from the national longitudinal alcohol epidemiologic survey. Journal of Substance Abuse, 9, 103–110. doi: 10.1016/s0899-3289(97)90009-2 [DOI] [PubMed] [Google Scholar]
- Grenard JL, Ames SL, Wiers RW, Thush C, Sussman S, & Stacy AW (2008). Working memory capacity moderates the predictive effects of drug-related associations on substance use. Psychol Addict Behav, 22(3), 426–432. doi: 10.1037/0893-164X.22.3.426 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grunbaum JA, Lowry R, & Kann L (2001). Prevalence of health-related behaviors among alternative high school students as compared with students attending regular high schools. Journal of Adolescent Health, 29(5), 337–343. doi: 10.1016/s1054-139x(01)00304-4 [DOI] [PubMed] [Google Scholar]
- Hanson KL, Thayer RE, & Tapert SF (2014). Adolescent marijuana users have elevated risk-taking on the balloon analog risk task. J Psychopharmacol, 28(11), 1080–1087. doi: 10.1177/0269881114550352 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hayes AF (2009). Beyond Baron and Kenny: Statistical Mediation Analysis in the New Millennium. Communication Monographs, 76(4), 408–420. doi: 10.1080/03637750903310360 [DOI] [Google Scholar]
- Hayes AF (2018). Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach (Second Edition ed.). New York, NY: Guilford Publications. [Google Scholar]
- Hayes AF, & Scharkow M (2013). The relative trustworthiness of inferential tests of the indirect effect in statistical mediation analysis: does method really matter? Psychol Sci, 24(10), 1918–1927. doi: 10.1177/0956797613480187 [DOI] [PubMed] [Google Scholar]
- Hoffman BR, Sussman S, Unger JB, & Valente TW (2006). Peer influences on adolescent cigarette smoking: a theoretical review of the literature. Subst Use Misuse, 41(1), 103–155. doi: 10.1080/10826080500368892 [DOI] [PubMed] [Google Scholar]
- Hovland CI, Harvey OJ, & Sherif M (1957). Assimilation and contrast effects in reactions to communication and attitude change. The Journal of Abnormal and Social Psychology, 55(2), 244–252. doi: 10.1037/h0048480 [DOI] [PubMed] [Google Scholar]
- Janik P, Kosticova M, Pecenak JP, & Turcek M (2017). Categorization of psychoactive substances into "hard drugs" and "soft drugs": a critical review of terminology used in current scientific literature. Am J Drug Alcohol Abuse, 43(6), 636–646. doi: 10.1080/00952990.2017.1335736 [DOI] [PubMed] [Google Scholar]
- Johnson K, & Taliaferro L (2012). Health behaviors and mental health of students attending alternative high schools: a review of the research literature. J Spec Pediatr Nurs, 17(2), 79–97. doi: 10.1111/j.1744-6155.2011.00311.x [DOI] [PubMed] [Google Scholar]
- Johnson KE, McMorris BJ, & Kubik MY (2013). Comparison of health-risk behaviors among students attending alternative and traditional high schools in Minnesota. J Sch Nurs, 29(5), 343–352. doi: 10.1177/1059840512469409 [DOI] [PubMed] [Google Scholar]
- Johnson KE, & Taliaferro LA (2012). Health behaviors and mental health of students attending alternative high schools: A review of the research literature. Journal for Specialists in Pediatric Nursing, 17(2), 79–97. [DOI] [PubMed] [Google Scholar]
- Johnston LD, Miech RA, O’Malley PM, Bachman JG, Schulenberg JE, & Patrick ME (2019). Monitoring the Future national survey results on drug use 1975-2018: Overview, key findings on adolescent drug use. Retrieved from Ann Arbor, Michigan: [Google Scholar]
- Johnston LD, O’Malley PM, Miech RA, Bachman JG, & Schulenberg JE (2016). Monitoring the Future national survey results on drug use, 1975-2015: Overview, key findings on adolescent drug use. Retrieved from Ann Arbor: [Google Scholar]
- Kandel D (1975). Stages in adolescent involvement in drug use. Science, 190(4217), 912–914. doi: 10.1126/science.1188374 [DOI] [PubMed] [Google Scholar]
- Kandel ER, & Kandel DB (2014). Shattuck Lecture. A molecular basis for nicotine as a gateway drug. N Engl J Med, 371(10), 932–943. doi: 10.1056/NEJMsa1405092 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kann LM,T; Harris WA; et al. (2015). Youth Risk Behavior Surveillance — United States. Retrieved from [Google Scholar]
- King KM, & Chassin L (2007). A Prospective Study of the Effects of Age of Initiation of Alcohol and Drug Else on Young Adult Substance Dependence*. Journal of Studies on Alcohol and Drugs, 68(2), 256–265. doi: 10.15288/jsad.2007.68.256 [DOI] [PubMed] [Google Scholar]
- Kirby T, & Barry AE (2012). Alcohol as a gateway drug: a study of US 12th graders. J Sch Health, 82(8), 371–379. doi: 10.1111/j.1746-1561.2012.00712.x [DOI] [PubMed] [Google Scholar]
- LAO. (2015). Next Steps for Improving State Accountability for Alternative Schools. Retrieved from Sacramento, CA: [Google Scholar]
- Mackinnon DP, Lockwood CM, & Williams J (2004). Confidence Limits for the Indirect Effect: Distribution of the Product and Resampling Methods. Multivariate Behav Res, 39(1), 99. doi: 10.1207/s15327906mbr3901_4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCuller WJ, Sussman S, Holiday K, Craig S, & Dent CW (2002). Tracking procedures for locating high-risk youth. Eval Health Prof, 25(3), 345–362. doi: 10.1177/0163278702025003006 [DOI] [PubMed] [Google Scholar]
- McCusker CG (2001). Cognitive biases and addiction: an evolution in theory and method. Addiction, 96(1), 47–56. doi: 10.1080/09652140020016950 [DOI] [PubMed] [Google Scholar]
- Miller JW, Naimi TS, Brewer RD, & Jones SE (2007). Binge drinking and associated health risk behaviors among high school students. Pediatrics, 119(1), 76–85. doi: 10.1542/peds.2006-1517 [DOI] [PubMed] [Google Scholar]
- Murray DM, Varnell SP, & Blitstein JL (2004). Design and Analysis of Group-Randomized Trials: A Review of Recent Methodological Developments. American Journal of Public Health, 94(3), 423–432. doi: 10.2105/ajph.94.3.423 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Newcomb MD, & Bentler PM (1988). The impact of family context, deviant attitudes, and emotional distress on adolescent drug use: Longitudinal latent-variable analyses of mothers and their children. Journal of Research in Personality, 22(2), 154–176. doi: 10.1016/0092-6566(88)90012-8 [DOI] [Google Scholar]
- Park HS, Levine TR, Kingsley Westerman CY, Orfgen T, & Foregger S (2007). The Effects of Argument Quality and Involvement Type on Attitude Formation and Attitude Change: A Test of Dual-Process and Social Judgment Predictions. Human Communication Research, 33(1), 81–102. doi: 10.1111/j.1468-2958.2007.00290.x [DOI] [Google Scholar]
- Pike JR, Shono Y, Tan N, Xie B, & Stacy AW (2019). Retail outlets prompt associative memories linked to the repeated use of nicotine and tobacco products among alternative high school students in California. Addict Behav, 99, 106067. doi: 10.1016/j.addbeh.2019.106067 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reid LW, Elifson KW, & Sterk CE (2007). Ecstasy and gateway drugs: initiating the use of ecstasy and other drugs. Ann Epidemiol, 17(1), 74–80. doi: 10.1016/j.annepidem.2006.07.013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rohrbach LA, Sussman S, Dent CW, & Sun P (2005). Tobacco, Alcohol, and other Drug use among High-Risk Young People: A Five-Year Longitudinal Study from Adolescence to Emerging Adulthood. Journal of Drug Issues, 35(2), 333–356. doi: 10.1177/002204260503500206 [DOI] [Google Scholar]
- Rooke SE, Hine DW, & Thorsteinsson EB (2008). Implicit cognition and substance use: a meta-analysis. Addict Behav, 33(10), 1314–1328. doi: 10.1016/j.addbeh.2008.06.009 [DOI] [PubMed] [Google Scholar]
- Saunders J, & Saunders E (2001). Alternative School Students' Perceptions of Past [Traditional] and Current [Alternative] School Environments. The High School Journal, 85(2), 12–23. [Google Scholar]
- Schlomer GL, Bauman S, & Card NA (2010). Best practices for missing data management in counseling psychology. J Couns Psychol, 57(1), 1–10. doi: 10.1037/a0018082 [DOI] [PubMed] [Google Scholar]
- Sherif CW, Sherif M, & Nebergall RE (1965). Attitude and attitude change: the social judgement-involvement process: Saunders. [Google Scholar]
- Sherif M, & Hovland CI (1961). Social judgment: Assimilation and contrast effects in communication and attitude change. [DOI] [PubMed] [Google Scholar]
- Smith SW, Atkin CK, Martell D, Allen R, & Hembroff L (2006). A Social Judgment Theory Approach to Conducting Formative Research in a Social Norms Campaign. Communication Theory, 16(1), 141–152. doi: 10.1111/j.1468-2885.2006.00009.x [DOI] [Google Scholar]
- Spijkerman R, van den Eijnden RJ, Vitale S, & Engels RC (2004). Explaining adolescents' smoking and drinking behavior: the concept of smoker and drinker prototypes in relation to variables of the theory of planned behavior. Addict Behav, 29(8), 1615–1622. doi: 10.1016/j.addbeh.2004.02.030 [DOI] [PubMed] [Google Scholar]
- Squeglia LM, Jacobus J, & Tapert SF (2009). The influence of substance use on adolescent brain development. Clin EEG Neurosci, 40(1), 31–38. doi: 10.1177/155005940904000110 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stacy AW (1997). Memory activation and expectancy as prospective predictors of alcohol and marijuana use. J Abnorm Psychol, 106(1), 61–73. [DOI] [PubMed] [Google Scholar]
- Stacy AW, Flay BR, Sussman S, Brown SK, Santi S, & Best JA (1990). Validity of alternative self-report indices of smoking among adolescents. Psychological Assessment, 2(4), 442–446. doi: 10.1037/1040-3590.2.4.442 [DOI] [Google Scholar]
- Stacy AW, & Wiers RW (2010). Implicit cognition and addiction: a tool for explaining paradoxical behavior. Annu Rev Clin Psychol, 6(1), 551–575. doi: 10.1146/annurev.clinpsy.121208.131444 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sussman S, Arpawong TE, Sun P, Tsai J, Rohrbach LA, & Spruijt-Metz D (2014). Prevalence and co-occurrence of addictive behaviors among former alternative high school youth. J Behav Addict, 3(1), 33–40. doi: 10.1556/JBA.3.2014.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sussman S, Dent CW, & Galaif ER (1997). The correlates of substance abuse and dependence among adolescents at high risk for drug abuse. Journal of Substance Abuse, 9, 241–255. doi: 10.1016/s0899-3289(97)90019-5 [DOI] [PubMed] [Google Scholar]
- Sussman S, Dent CW, & Stacy AW (2002). Project Towards No Drug Abuse: A Review of the Findings and Future Directions. American Journal of Health Behavior, 26(5), 354–365. doi: 10.5993/ajhb.26.5.4 [DOI] [PubMed] [Google Scholar]
- Sussman S, Skara S, & Ames SL (2008). Substance abuse among adolescents. Subst Use Misuse, 43(12-13), 1802–1828. doi: 10.1080/10826080802297302 [DOI] [PubMed] [Google Scholar]
- Sussman S, Stacy AW, Dent CW, Simon TR, Galaif ER, Moss MA, … Johnson CA (1995). Continuation high schools: youth at risk for drug abuse. J Drug Educ, 25(3), 191–209. doi: 10.2190/HDQH-XD21-GJT0-9G8V [DOI] [PubMed] [Google Scholar]
- Sussman SA, SL;. (2001). The social psychology of drug abuse. Buckingham, GB: Open University Press. [Google Scholar]
- Volkow ND, Baler RD, Compton WM, & Weiss SR (2014). Adverse health effects of marijuana use. N Engl J Med, 370(23), 2219–2227. doi: 10.1056/NEJMra1402309 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wiers RW, & Stacy AW (2006). Implicit cognition and addiction: An introduction. Current Directions in Psychological Science. [Google Scholar]
- Zweig JM (2003). Vulnerable Youth: Identifying Their Need for Alternative Educational Settings. [Google Scholar]