

Abstract
To (i) introduce the technical notes of a novel full‐endoscopic foraminotomy with a large endoscopic trephine for the treatment of severe degenerative lumbar foraminal stenosis at L5S1 level; (ii) assess the primary clinical outcomes of this technique; (iii) compare the effectiveness of this full‐endoscopic foraminotomy technique and other previous techniques for lumbar foraminal stenosis. From January 2019 to August 2019, a retrospective study of L5S1 severe degenerative lumbar foraminal stenosis was performed in our center. All patients who were diagnosed with severe foraminal stenosis at L5S1 level and failed conservative treatment for at least 6 weeks were identified. Patients with segmental instability or other coexisting contraindications were excluded. A total of 21 patients were enrolled in the study. All patients were treated by full‐endoscopic foraminotomy using large endoscopic trephine. The visual analogue scale (VAS) and Oswestry disability index (ODI) were evaluated preoperatively and at 1, 3, 6 months, and 1 year after the surgery, and the modified MacNab criteria were used to evaluate clinical outcomes at the last follow‐up. There were 10 males and 11 females with a mean age of 66.38 ± 9.51 years. Five patients had a history of lumbar surgery. The mean operative time was 63.57 ± 25.74 min. The mean follow‐up time was 13.29 ± 1.38 months. The mean postoperative hospital stay time was 1.29 ± 0.56 days. The mean preoperative VAS score significantly decreased from 7.38 ± 1.02 to 2.76 ± 1.09 (t = 19.759, P < 0.01), 2.25 ± 1.02 (t = 21.508, P < 0.01), 1.60 ± 1.05 (t = 31.812, P < 0.01), and 1.45 ± 1.10 (t = 25.156, P < 0.01) at 1 month, 3 months, 6 months, and 1 year after the operation. The mean preoperative ODI score significantly decreased from 64.66% ± 4.91% to 30.69% ± 4.59% (t = 33.724, P < 0.01), 29.44% ± 4.50% (t = 32.117, P < 0.01), 24.22% ± 4.14% (t = 33.951, P < 0.01), and 22.44% ± 4.94% (t = 30.241, P < 0.01) at 1 month, 3 months, 6 months, and 1 year after the operation. At the last follow‐up, 19 patients (90.48%) got excellent or good outcomes. One patient suffered postoperative dysesthesia, and the symptoms were controlled by conversion treatment. One patient took revision surgery due to the incomplete decompression. There were no other major complications. Percutaneous endoscopic decompression is minimally invasive spine surgery. However, the application of endoscopic decompression for L5S1 foraminal stenosis is relatively difficult due to the high iliac crest and narrow foramen. Full‐endoscopic foraminotomy with the large endoscopic trephine is an effective and safe technique for the treatment of degenerative lumbar foraminal stenosis.
Keywords: Endoscopic trephine, Foraminal stenosis, Full‐endoscopic foraminotomy, Lumbar spinal stenosis

We described an advanced percutaneous endoscopic lumbar foraminotomy by using a specially designed endoscopic trephine. The hard bony decompression was performed directly under endoscopic observation. It combined the efficiency of trephine and the safety of the instruments guided by the endoscope. A safe and effective full‐range decompression of the exiting nerve root was achieved by this technique.
Introduction
Degenerative lumbar spinal stenosis results from gradual degenerative changes in the lumbar spine and can significantly affect mobility, function, and quality of daily life. Degenerative lumbar spinal stenosis is a common disease among the geriatric population and the most frequent indication for spinal surgery. Lumbar foraminal stenosis is a special type of lumbar spinal stenosis.
The lumbar intervertebral foramina is a round, oval, or inverted teardrop zone lateral to the spinal canal. The anatomical boundaries of the lumbar foramina are as below: the upper boundary is the superior vertebral pedicle; the lower boundary is the inferior vertebral pedicle; the anterior boundary is the intervertebral disc, the posteroinferior part of the upper vertebral body, and the posterosuperior part of the lower vertebral body; the posterior boundary is the facet joint and the ligamentum flavum (LF). The normal area of lumbar foramina ranges from 40 to 160 mm2, and the height of lumbar foramina ranges from 20 to 23 mm. The exiting nerve root and dorsal root ganglia through the lumbar foramina are surrounded by radicular vessels and fat. The nerve runs in the anterosuperior part of the foramina, which is between the superior transforaminal ligaments and the inferior transforaminal ligament 1 . The ratio of the exiting nerve root and dorsal root ganglia to the foraminal area could reach 30% 2 .
Degenerative lumbar foraminal stenosis is defined as neural foraminal narrowing caused by the diminishment of the foraminal height, hypertrophy of the facet joint and ligamentum flavum (LF), subluxation of the superior articular process (SAP), osteophytes, and lateral disc herniations 3 . Far lateral disc herniation, foraminal height decrease, and posterolateral osteophytes could compress the exiting nerve root to the superior pedicle, which results in the vertical stenosis of the foramen. Hypertrophic LF and facet joint, subluxation of the SAP, and bony spurs could compress the exiting nerve root which leads to the transverse stenosis of the foramen. A combination of vertical stenosis and transverse stenosis could cause the circumferential stenosis of the foramen. The nerve will be compressed severely in the circumferential foraminal stenosis that most of this area may need surgical treatment. The buckling of the LF caused by foraminal height decrease also contributes to the circumferential foraminal stenosis. A previous study pointed out that foraminal height less than 15 mm and posterior disc height less than 4 mm will result in significant nerve compression.
Lumbar foraminal stenosis tends to occur in the lower lumbar levels. A previous study reported that 75% of lumbar foraminal stenosis occurred in the L5S1 level 4 . The reason may be related to the following factors. First, the diameter of the L5 dorsal root ganglia is the biggest (8.3 mm) and could occupy nearly 51.2% of the available foraminal area. Second, the LF coverage ratio of the foraminal area was largest in the L5S1 level 5 . This also indicates the LF is more likely to buckle and compress the nerve when L5S1 foraminal height decreases. Finally, the lumbosacral junction level, the mobility, and loading of the L5S1 level are larger than other levels. This also makes L5S1 level tend to occur degeneration, which result in disc herniation, disc height loss, facet joint, and LF hypertrophy.
Lumbar exiting nerve root and dorsal root ganglia could be compressed by lumbar foraminal stenosis, and result in low back pain and radicular symptoms. The incidence of lumbar foraminal stenosis was reported as 8%–11% 4 , 6 . The previous study pointed out that nearly 60% of failed back surgery syndromes were caused by unrecognized and incomplete decompression of lumbar foraminal stenosis 7 .
Conventional open paraspinal foraminotomy or foraminoplasty has been considered as the golden standard treatment for lumbar foraminal stenosis 8 , 9 . However, open surgery would have more surgical trauma and take a longer time for postoperative recovery 10 . Moreover, some patients suffered postoperative radicular pain or dysesthesia, which was attributed to the excessive manipulation of the dorsal root ganglion or incomplete decompression 9 , 11 .
To solve these problems, minimally invasive spine surgery including percutaneous endoscopic foraminal discectomy or foraminoplasty was developed 12 , 13 , 14 , 15 . These techniques had many advantages including less bleeding, minor surgical trauma, a shorter hospital stay, and a rapid postoperative functional recovery 16 , 17 , 18 . However, most of these minimally invasive techniques used were limited to the soft disc and to mild or moderate foraminal stenosis due to a lack of effective decompression tools. For bony and severe foraminal stenosis especially at L5S1 level, where the obstruction of the high iliac crest and L5 transverse process exist 19 , a safe, complete, and effective decompression remains a great challenge.
In the present study, we performed endoscopic foraminotomy by using the large endoscopic trephine for degenerative lumbar foraminal stenosis at the L5S1 level, which placed the procedure of bony decompression directly under endoscopic observation. The objective of the present study was to: (i) describe the technical notes of this full‐endoscopic foraminotomy with a novel large endoscopic trephine for the treatment of severe degenerative lumbar foraminal stenosis at L5S1 level; (ii) assess the primary clinical outcomes of this technique; (iii) compare the effectiveness of this full‐endoscopic foraminotomy technique and other previous techniques for lumbar foraminal stenosis.
Methods and Materials
Inclusion and Exclusion Criteria
The inclusion criteria were as follow: (i) patients with radicular symptoms caused by L5S1 foraminal stenosis; (ii) conservative treatment failed for at least 6 weeks; (iii) preoperative magnetic resonance imaging (MRI) and computed tomography (CT) showed severe foraminal stenosis (nerve root collapse) 20 ; (iv) underwent full‐endoscopic foraminotomy surgery; (v) followed up for 12 months.
The exclusion criteria were as follows: (i) segmental instability; (ii) isthmic lumbar spondylolisthesis or degenerative lumbar spondylolisthesis greater than I degree; (iii) coexisting contraindications such as infection and tumor.
Patient Population
Between January 2019 and August 2019, 21 patients with L5S1 foraminal stenosis treated by full‐endoscopic foraminotomy were enrolled in our study according to the inclusion and exclusion criteria. All procedures were approved by the Ethics Committee of our institution.
Surgical Technique
A Novel Large Endoscopic Trephine System
A special and novel instrument named large endoscopic trephine system was designed for full‐endoscopic foraminotomy (Fig. 1A,B). The outside diameter (OD) and inside diameter (ID) of the trephine was 7.5 mm and 6.5 mm. The OD of the endoscope was 6.3 mm and the ID of the working cannula was 7.6 mm (Endo‐Surgi/Standard, Joimax, German). Endoscopic trephine could be inserted between the working cannula and endoscope, and could remove the bone under endoscopic observation.
Fig. 1.

Endoscopic trephine system. (A, B): Specially designed instruments of endoscopic trephine system. (A) Special trephine (left), working cannula (medial), secondary bevel‐ended working cannula (right). (B) Schematic illustration of the endoscopic trephine system. Endoscopic trephine was inserted between the working cannula and endoscope, which could remove the bone under endoscopic observation.
All surgeries were performed by experienced endoscopy surgeons. The surgical procedures could be summarized into the following three steps: (i) a safe extraforaminal approach to the lateral side of the SAP; (ii) a safe and effective bony decompression including hypertrophied SAP, ventral side of the isthmus, and inferior side of the superior pedicle; (iii) soft tissue decompression including thickened LF and foraminal ligament (Fig. 2A–E).
Fig. 2.

Schematic illustration of the foraminotomy by using the endoscopic trephine. (A) A flow chart of the key steps for full‐endoscopic foraminotomy surgery. (B) The initial decompression started at the shoulder of SAP, and the working cannula was placed in contact with the surface of SAP. (C) The procedure of bony decompression was from outside to inside and from caudal to cranial. (D) Decompression cranially to the partial ventral side of the isthmus and inferior side of superior pedical until the cranial attachment of foraminal ligamentum flavum exposed. (E) Removed thickened LF, nucleus pulposus fragments and foraminal ligament, the decompression was completed. Upper was coronal illustration, and the lower was sagittal illustration. LF was figured in gray, dura and nerve root were figured in yellow, disc and nucleus fragments were figured in blue, bony structure was figured in light yellow.
Patient Preparation and Approach
All operations were performed under local anesthesia. The patient was placed in the lateral position on a radiolucent table (Fig. 3A). The entry point was located 7 to 9 cm lateral from the midline (depending on the iliac crest, the L5 transverse process, and the L5S1 disc space) (Fig. 3B). The direction of the approach should be parallel to the L5S1 disc space. The main target point was the shoulder of the SAP (Fig. 3B–D). To identify an adequate approach trajectory, preoperative radiography and intraoperative fluoroscopy should be carefully checked.
Fig. 3.

Placement of working cannula. (A) The patient was placed in the lateral position. The entry point was located 8 cm lateral from midline. (B) Reconstructed 3D illustration showed the cannula was placed parallel to L5S1 disc space, and targeted at the shoulder of the SAP. (C, D) Intraoperative radiography showed the extraforaminal placement of the working cannula. (E) The endoscopic views of the SAP. (F) The endoscopic trephine was inserted for bony decompression. SAP, superior articular process; Endo, endoscopic.
The procedure of the approach was performed in the following steps: (i) once the entry point and direction were confirmed, local anesthesia (2% lidocaine 15 mL, 1% ropivacaine 10 mL, and saline 20 mL) was performed on soft tissue and facet joint; (ii) an 18‐gauge spinal needle was inserted into the shoulder of SAP by the guidance of fluoroscopy, and then a guidewire was passed to replace the spinal needle; (iii) a skin incision was made, a series of obturators were inserted through the guidewire; (iv) a bevel‐ended working cannula was inserted through the obturator, and the cannula was put in contact with the surface of SAP; (v) the endoscopic trephine and endoscope were inserted, and the surface of SAP could viewed by the endoscope (Fig. 3E,F).
Endoscopic Foraminal Decompression
The bony decompression was performed using endoscopic trephine (Fig. 1A,B). The key points of bony decompression by endoscopic trephine were as follows. First, the endoscopic trephine should be firmly in contact with the surface of the bone to prevent slipping. Second, the trephine should be rotated to remove the bone. The movement of the bone was observed under endoscopy that when the trephine rotated in the opposite direction, it indicated that the bone had been resected enough. Sometimes, a layer of fragile cortical bone preserved on the ventral side should be removed gently. Finally, the direction of the bony decompression was from outside to inside and from caudal to cranial. Large bones could be resected in several parts. The range of cranial decompression should expose the cranial attachment of foraminal ligamentum flavum.
The procedure of foraminal decompression was performed using the following steps: (i) after the capsule and soft tissue were removed, the surface of SAP bone was exposed (Fig. 4A,B); (ii) endoscopic trephine was used to remove partial hypertrophied SAP shoulder, tip, and osteophyte. After this procedure, the foraminal structures including exiting nerve root, foraminal ligament, and LF appeared clearly (Fig. 4C,D); (iii) the partial ventral side of the inferior articular process and isthmus were removed by endoscopic trephine. We carefully continued cranial bony decompression until the cranial attachment of foraminal LF was exposed (usually the transition zone of the inferior and posterolateral side of the pedicle and the base of the transverse process). We removed the attachment of foraminal LF. Thus, the thickened foraminal LF was en‐bloc removed (Fig. 4E); (iv) the secondary bevel‐ended working cannula was inserted to replace the endoscopic trephine. An exploration of foramen could be performed. Preserved bone debris, ligaments, and possibly existed redundant disc could be removed by endoscopic graspers and punches. The decompression was completed when the exiting nerve root could be mobilized freely by straight leg raising test or flexible probe (Fig. 4F).
Fig. 4.
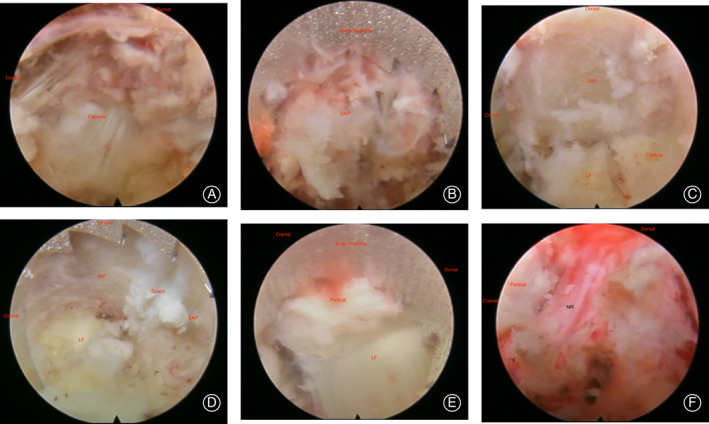
Intraoperative endoscopic views of the decompression by endoscopic trephine. (A) The facet joint capsule was exposed. (B) Endoscopic trephine was inserted to remove the shoulder of SAP. (C) Partial SAP was removed by endoscopic trephine, and a layer of fragile cortical bone preserved on the ventral side. It could prevent the injury of the nerve root. (D) LF and joint space were exposed after partial SAP and IAP was removed. (E) The cranial attachment of foraminal LF was exposed. It should be removed carefully. (F) The complete full‐range decompression of the exiting nerve root.
We withdrew the endoscopy system and closed the skin incision with a 1‐point subcutaneous suture. Patients were permitted to be discharged when they could walk without complications.
Outcome Evaluation
The operation time, postoperative hospital stay time, and complications were recorded. Clinical outcomes measurements were evaluated preoperatively and at 1, 3, 6 months, and 1 year after the operation. Modified MacNab criteria was used to evaluate the overall clinical outcomes at the last follow‐up. Patients' clinical data were collected by chart reviews and patient‐based outcome questionnaires or telephone interviews.
Clinical Outcomes Measurements
Visual Analog Scale (VAS)
VAS was used to evaluate low back pain and leg pain. VAS divided the degree of pain from 0 to 10: 0 represented no pain, 1 to 3 represented mild pain, 4 to 6 represented moderate pain, 7 to 9 represented severe pain that patient could not tolerate, and 10 represented the most pain 21 .
Oswestry Disability Index (ODI)
ODI was wildly used to evaluate the limitations of daily activities caused by spinal diseases. The ODI contains 10 questions, including pain intensity, self‐care, lifting, walking, sitting, standing, sleep, sex, social, travel. Each question score range was from 0 to 5 points. We summarized each question the patients answered and converted them into a percentage score as follows: (total score/(5 × number of questions answered)) × 100%. The percentages reflected pain as follows: 0% to 20% represented mild dysfunction, 21% to 40% represented moderate dysfunction, 41% to 60% represented severe dysfunction, and 61% to 80% represented disability, 81% to 100% represented long‐term bedridden or exaggerating the influence of the pain 22 .
Modified MacNab Criteria
Modified MacNab criteria were used to evaluate the overall effectiveness of the surgery, including four grades. Excellent: No restriction of mobility, return to normal work and level of activity. Good: Relief of presenting symptoms, able to return to modified work. Fair: Some improved functional capacity, still handicapped. Poor: No relief of symptoms.
Statistical Analysis
Continuous variables were expressed as means ± SD, preoperative, and postoperative clinical outcomes were compared using paired t‐test. P value <0.05 was considered significant. Statistical analysis was performed by SPSS 20.0 (SPSS. Chicago, IL, USA).
Result
Demographics and Operative Data
There were 10 males and 11 females with a mean age of 66.38 ± 9.51 years (ranged from 52 to 85 years). Five patients had a history of lumbar surgery. Three of them underwent open discectomy and fusion surgery at the adjacent level, two patients underwent endoscopic discectomy at the operative level. The mean operative time was 63.57 ± 25.74 min (ranged from 33 to 114 min). The mean follow‐up time was 13.29 ± 1.38 months (ranged from 12 to 16 months). The mean postoperative hospital stay time was 1.29 ± 0.56 days (ranged from 0 to 2 days).
Clinical Outcomes
VAS and ODI
The mean preoperative VAS score significantly decreased from 7.38 ± 1.02 to 2.76 ± 1.09 (t = 19.759, P < 0.01), 2.25 ± 1.02 (t = 21.508, P < 0.01), 1.60 ± 1.05 (t = 31.812, P < 0.01), and 1.45 ± 1.10 (t = 25.156, P < 0.01) at 1 month, 3 months, 6 months, and 1 year after the operation. The mean preoperative ODI score significantly decreased from 64.66% ± 4.91% to 30.69% ± 4.59% (t = 33.724, P < 0.01), 29.44% ± 4.50% (t = 32.117, P < 0.01), 24.22% ± 4.14% (t = 33.951, P < 0.01), and 22.44% ± 4.94% (t = 30.241, P < 0.01) at 1 month, 3 months, 6 months, and 1 year after the operation (Fig. 5).
Fig. 5.

VAS and ODI were improved significantly after the surgery. (A) VAS before surgery (pre‐op) and at 1 month, 3 months, 6 months, and 1 year after surgery. (B) ODI before surgery (pre‐op) and at 1 month, 3 months, 6 months, and 1 year after surgery.
Modified MacNab Criteria
At the last follow‐up, according to the modified MacNab criteria, 12 patients got an excellent outcome, seven patients got a good outcome, one patient got a fair outcome, and one patient got a poor outcome. The successful rate (excellent and good outcomes) reached 90.48% in our study.
One patient suffered postoperative dysesthesia, and the symptoms were controlled by conversion treatment. One patient took revision surgery due to the incomplete decompression. There were no other major complications.
Discussion
Difference with the Traditional Endoscopic Trephine
For past decades, the application of trephine for endoscopic decompression was guided by fluoroscopy 13 , 23 , 24 . With the development of technology, the endoscopic trephine guided under endoscopic visualization was used for endoscopic decompression 14 . However, the diameter of this traditional endoscopic trephine was relatively small, and it was inserted inside the endoscope. The efficiency of this traditional endoscopic trephine for bony compression was low 14 .
The overall decompression procedure performed by the endoscopic trephine in this study could be monitored under endoscopic view, which reduced the occurrence of potential neurovascular injury. Furthermore, the large diameter of the endoscopic trephine in this study could provide efficient and sufficient decompression.
The application of the endoscopic trephine technique in patients with severe foraminal stenosis has many advantages. First, the decompression for foramen was from outside to inside. At the beginning of this technique, the cannula was placed at the extraforaminal zone instead of being inserted into the foraminal zone, which could decrease the occurrence of exiting nerve root irritation 13 . In this study, we inserted the endoscopy and trephine when the cannula was contacted with the surface of SAP. This meant the first step of decompression could be guided by the endoscopic view. Second, the endoscopic trephine could resect the bone rapidly under direct endoscopic observation control. This technique offered sufficient decompression of exiting nerve root in foraminal stenosis and minimized the incidence of neural injury and bleeding (Fig. 6). The manipulation of the endoscopic trephine was simple to experienced surgeons. The mean operative time could be shortened to 63 min with the shortest operative time of 33 min. Furthermore, the instruments were easier to acquire without major cost. Overall, it was an efficient and safe technique for foraminal stenosis. Finally, as introduced previously, the approach of our technique was paralleled to the disc space, and the entry point was closer to the midline than those conventional transforaminal approaches, which made it easier to reach L5S1 foraminal. The high iliac crest and L5 transverse process did not obstruct our approach. Meanwhile, the SAP basilar part and most of the SAP body were preserved, and there was no postoperative back pain to affect stability.
Fig. 6.

The case of a 56‐year‐old female patient. (A, B) Preoperative MRI and CT showed the severe foraminal stenosis at the left L5S1 level. (C, D) Postoperative CT showed complete foraminal decompression was achieved. Preoperative (E) and postoperative (F) reconstructed 3D illustrations showed the exiting nerve root was completely decompressed. The gray part was L5 vertebral and structures above L5. The red part was S1 vertebral and structures below S1. The green part was the iliac crest. The orange line was the exiting nerve root. The orange dotted line was the exiting nerve root covered by the bony structures. The hypertrophied SAP, ventral side of the isthmus and the transition zone of the posterolateral side of the superior pedical and the base of the transverse process were removed.
Endoscopic Decompression for Foraminal Stenosis and Clinical Outcomes
For past decades, several percutaneous endoscopic decompression techniques for lumbar foraminal stenosis have been developed. Knight et al. 25 introduced the use of lasers for foraminoplasty, which could ablate discs, ligaments, and osteophytes. However, the effect of the laser for bony stenosis is low and time‐consuming. Ahn et al. 23 reported the foraminotomy by reamer in patients with L5S1 foraminal stenosis. Schubert and Hoogland 24 also described the foraminoplasty by reamer in patients with migrated disc herniation. Reamer could remove the hypertrophied bone effectively. However, the use of reamer was guided by fluoroscopy. The decompression was not visually controlled which could lead to neural injury.
Recently, Ahn et al. 14 described the use of the endoscopic drill for foraminotomy in patients with foraminal stenosis. Choi et al. 13 also reported the foraminoplasty for disc herniation by using an endoscopic drill. The endoscopic drill was a safe and effective technique that could accomplish decompression under endoscopic observation. However, the manipulation of the endoscopic drill is difficult and time‐consuming. Lee et al. 12 demonstrated a biportal endoscopic technique by using pituitary rongeur and Kerrison punch for patients with foraminal stenosis. It could also decompress under endoscopic vision. However, the efficacy for bony stenosis is low and time‐consuming.
In our study, we used endoscopic trephine for foraminotomy in patients with L5S1 foraminal stenosis. This technique provided full decompression of exiting nerve root in bony foraminal stenosis with the control of direct endoscopic observation. The VAS and ODI scores were significantly decreased at 1, 3, 6 months, and 1 year after the operation. The satisfied rate was 90.48% and no major complications occurred at the last follow‐up. Our results were comparable to previous endoscopic decompression techniques (Table 1). These results indicated that the endoscopic trephine technique was safe and effective for foraminal stenosis decompression.
TABLE 1.
Comparison of clinical outcomes with other endoscopic foraminoplasty
| Ref. | No. of patients | Operative Time, min | Pathology | Instrument | Success Rate | Postoperative Hospital Stay | Complication |
|---|---|---|---|---|---|---|---|
| Knight et al., 2001 | 250 | Foraminal stenosis, Disc | Endo Laser | 73% | 1 foot drop, 1 aseptic discitis, 13 revision surgery | ||
| Ahn et al., 2003 | 12 | 73(45–110) | Foraminal Stenosis,L5S1 | Reamer, Endo Laser | 83.3% | 1 open surgery | |
| Ahn et al., 2014 | 33 | 55.6(35–120) | Foraminal Stenosis | Endo drill | 82% | 1.36(1 ‐ 4) | 2 dysesthesia, 1 open surgery |
| Choi et al., 2017 | 36 FG(136) | Disc, L5S1 | Endo drill | 94.4% in FG | 1 recurrence | ||
| Lee et al., 2018 | 11 FS(27) | 76.7 | Foraminal Stenosis, Disc | BESS, chisel, Kerrison punch | 81.0% | 7.0(4.5 ‐ 8.5) | 1 dural tear |
| Our study | 21 | 63.6(33–114) | Foraminal Stenosis, L5S1 | Endo Trephine | 90.5% | 1.29(0 ‐ 2) | 1 dysesthesia, 1 revision surgery |
BESS, Biportal Endoscopic Spinal Surgery; Endo, Endoscopic; FG, Foraminoplasty group; FS, Feraminal stenosis.
Technical Considerations for Successful Decompression
The most important point of this technique was the placement of the working cannula and the sufficient decompression of the exiting nerve root. In the case of L5S1 degenerative foraminal stenosis, the hypertrophied SAP subluxated superiorly and anteriorly, and the foraminal height decreased, which made the foramen relative narrow 3 , 4 . So, the cannula was placed at the shoulder of SAP, away from the compressed exiting nerve root. The decompression procedure that started from the shoulder, might be safer than those that started from the tip. Another key point for this technique is that bony decompression should be performed until the cranial attachment of LF was exposed. In the L5S1 level, LF passed over the posterior of the foramen and covered the third cross‐sectional area of the foramen 26 . Moreover, the lateral LF went more obliquely and cranially which covered the dorsal space of the exiting nerve root. The thickened LF and the inferior and posterolateral part of the pedicle should also be removed (Fig. 6). Furthermore, the removed part of the facet joint was less than 50% (Fig. 6E,F). Besides, there was no postoperative back pain related to activities reported by patients during the follow‐up period, which we consider that stability was not affected 20 . The complete decompression for the full range of exiting nerve roots without excess removal of the facet joint should be achieved.
Limitation
The main limitation of our study was that the follow‐up time was relatively short. The second limitation is that the study lacked a control group which decreased the evidence quality. The long‐term efficacy of this technique still needs a large‐sample, prospective, controlled cohort study to confirm its findings.
Conclusion
The preliminary results of this technique were satisfying. Full‐endoscopic foraminotomy with the endoscopic trephine is an effective and safe technique for the treatment of degenerative lumbar foraminal stenosis.
Disclosure: This study was conducted according to the Declaration of Helsinki and approved by the Peking University Third Hospital Medical Science Research Ethics Committee (approval number: IRB00006761‐M2020022).
Grant Sources: This study was funded by Beijing Municipal Science and Technology Commission (Code: 2020–2‐4091). The authors have no other conflict of interest.
Contributor Information
Bin Zhu, Email: zhubin_ortho@163.com.
Xiao‐guang Liu, Email: liuxgspine@126.com.
References
- 1. Yuan SG, Wen YL, Zhang P, Li YK. Ligament, nerve, and blood vessel anatomy of the lateral zone of the lumbar intervertebral foramina. Int Orthop, 2015, 39: 2135–2141. [DOI] [PubMed] [Google Scholar]
- 2. Hasue M, Kunogi J, Konno S, Kikuchi S. Classification by position of dorsal root ganglia in the lumbosacral region. Spine (Phila Pa 1976), 1989, 14: 1261–1264. [DOI] [PubMed] [Google Scholar]
- 3. Hasegawa T, An HS, Haughton VM, Nowicki BH. Lumbar foraminal stenosis: critical heights of the intervertebral discs and foramina. A cryomicrotome study in cadavera. J Bone Joint Surg Am, 1995, 77: 32–38. [PubMed] [Google Scholar]
- 4. Jenis LG, An HS. Spine update. Lumbar foraminal stenosis. Spine (Phila Pa 1976), 2000, 25: 389–394. [DOI] [PubMed] [Google Scholar]
- 5. Akhgar J, Terai H, Rahmani MS, et al. Anatomical analysis of the relation between human ligamentum flavum and posterior spinal bony prominence. J Orthop Sci, 2017, 22: 260–265. [DOI] [PubMed] [Google Scholar]
- 6. Kunogi J, Hasue M. Diagnosis and operative treatment of intraforaminal and extraforaminal nerve root compression. Spine (Phila Pa 1976), 1991, 16: 1312–1320. [DOI] [PubMed] [Google Scholar]
- 7. Burton CV, Kirkaldy‐Willis WH, Yong‐Hing K, Heithoff KB. Causes of failure of surgery on the lumbar spine. Clin Orthop Relat Res, 1981, 157: 191–199. [PubMed] [Google Scholar]
- 8. Chang HS, Zidan I, Fujisawa N, Matsui T. Microsurgical posterolateral transmuscular approach for lumbar foraminal stenosis. J Spinal Disord Tech, 2011, 24: 302–307. [DOI] [PubMed] [Google Scholar]
- 9. Epstein NE. Foraminal and far lateral lumbar disc herniations: surgical alternatives and outcome measures. Spinal Cord, 2002, 40: 491–500. [DOI] [PubMed] [Google Scholar]
- 10. Senker W, Gruber A, Gmeiner M, et al. Surgical and clinical results of minimally invasive spinal fusion surgery in an unselected patient cohort of a spinal care unit. Orthop Surg, 2018, 10: 192–197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Hodges SD, Humphreys SC, Eck JC, Covington LA. The surgical treatment of far lateral L3‐L4 and L4‐L5 disc herniations. A modified technique and outcomes analysis of 25 patients. Spine (Phila Pa 1976), 1999, 24: 1243–1246. [DOI] [PubMed] [Google Scholar]
- 12. Ahn JS, Lee HJ, Choi DJ, Lee KY, Hwang SJ. Extraforaminal approach of biportal endoscopic spinal surgery: a new endoscopic technique for transforaminal decompression and discectomy. J Neurosurg Spine, 2018, 28: 492–498. [DOI] [PubMed] [Google Scholar]
- 13. Choi KC, Shim HK, Park CJ, Lee DC, Park CK. Usefulness of percutaneous endoscopic lumbar Foraminoplasty for lumbar disc herniation. World Neurosurg, 2017, 106: 484–492. [DOI] [PubMed] [Google Scholar]
- 14. Ahn Y, Oh HK, Kim H, Lee SH, Lee HN. Percutaneous endoscopic lumbar foraminotomy: an advanced surgical technique and clinical outcomes. Neurosurgery, 2014, 75: 124–133; discussion 132‐123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Youn MS, Shin JK, Goh TS, Lee JS. Clinical and radiological outcomes of endoscopic partial facetectomy for degenerative lumbar foraminal stenosis. Acta Neurochir, 2017, 159: 1129–1135. [DOI] [PubMed] [Google Scholar]
- 16. Fan S, Hu Z, Zhao F, Zhao X, Huang Y, Fang X. Multifidus muscle changes and clinical effects of one‐level posterior lumbar interbody fusion: minimally invasive procedure versus conventional open approach. Eur Spine J, 2010, 19: 316–324. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Peng CW, Yue WM, Poh SY, Yeo W, Tan SB. Clinical and radiological outcomes of minimally invasive versus open transforaminal lumbar interbody fusion. Spine (Phila Pa 1976), 2009, 34: 1385–1389. [DOI] [PubMed] [Google Scholar]
- 18. Bao BX, Zhou JW, Yu PF, Chi C, Qiang H, Yan H. Transforaminal endoscopic discectomy and Foraminoplasty for treating central lumbar stenosis. Orthop Surg, 2019, 11: 1093–1100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Fan G, Wang T, Hu S, Guan X, Gu X, He S. Isocentric navigation of percutaneous endoscopic Transforaminal discectomy at the L5/S1 level in difficult puncture cases: a technical note. Pain Physician, 2017, 20: E531–E540. [PubMed] [Google Scholar]
- 20. Lee S, Lee JW, Yeom JS, et al. A practical MRI grading system for lumbar foraminal stenosis. Am J Roentgenol, 2010, 194: 1095–1098. [DOI] [PubMed] [Google Scholar]
- 21. Rodriguez CS. Pain measurement in the elderly: a review. Pain Manag Nurs, 2001, 2: 38–46. [DOI] [PubMed] [Google Scholar]
- 22. Liu H, Tao H, Luo Z. Validation of the simplified Chinese version of the Oswestry disability index. Spine (Phila Pa 1976), 2009, 34: 1211–1216 discussion 1217. [DOI] [PubMed] [Google Scholar]
- 23. Ahn Y, Lee SH, Park WM, Lee HY. Posterolateral percutaneous endoscopic lumbar foraminotomy for L5‐S1 foraminal or lateral exit zone stenosis. Technical note. J Neurosurg, 2003, 99: 320–323. [DOI] [PubMed] [Google Scholar]
- 24. Schubert M, Hoogland T. Endoscopic transforaminal nucleotomy with foraminoplasty for lumbar disk herniation. Oper Orthop Traumatol, 2005, 17: 641–661. [DOI] [PubMed] [Google Scholar]
- 25. Knight MT, Vajda A, Jakab GV, Awan S. Endoscopic laser foraminoplasty on the lumbar spine–early experience. Minim Invasive Neurosurg, 1998, 41: 5–9. [DOI] [PubMed] [Google Scholar]
- 26. Chau AM, Pelzer NR, Hampton J, et al. Lateral extent and ventral laminar attachments of the lumbar ligamentum flavum: cadaveric study. Spine J, 2014, 14: 2467–2471. [DOI] [PubMed] [Google Scholar]