

Key message
Tuberculous bronchopleural fistula is a rare complication of pulmonary tuberculosis with presentation ranging from patients who are asymptomatic with incidental findings on imaging to those who present with acute tension pneumothorax.
Keywords: Bronchopleural fistula, tuberculosis
Tuberculous bronchopleural fistula is a rare complication of pulmonary tuberculosis with presentation ranging from patients who are asymptomatic with incidental findings on imaging to those who present with acute tension pneumothorax.

Clinical Image
A 21‐year‐old man presented to the emergency department with a three‐week history of cough, dyspnoea, night sweats, and 25‐kg weight loss over two months. Admission chest X‐ray (CXR; Fig. 1A1) and computed tomography (CT) scan (Fig. 1A2) demonstrated a large right upper lobe cavity, confluent right middle lobe consolidation, and left‐sided infiltrates. Pulmonary tuberculosis was diagnosed by positive sputum microscopy and Xpert® MTB/RIF, Cepheid, USA, and confirmed by culture. First‐line anti‐tuberculous therapy was commenced. Repeat imaging with CXR (Fig. 1B1) and CT (Fig. 1B2) at four months demonstrated improvement of right‐sided consolidation with interval development of a bronchopleural fistula and large pneumothorax. Tube thoracostomy was not performed as the patient was clinically stable and the pleural thickening and dense consolidation surrounding the cavity indicated that lung re‐expansion was unlikely. At the end of treatment, the patient was asymptomatic and CXR (Fig. 1C) demonstrated resolution of the right‐sided consolidation and a small residual pneumothorax. Bronchopleural fistula is a rare and potentially life‐threatening complication of pulmonary tuberculosis [1, 2]. Presentations range from incidental findings on CXR to acute tension pneumothorax. The mainstay of treatment is anti‐tuberculous therapy combined with tube or open thoracostomy, but bronchoscopic intervention or surgical repair may be required [1, 2]. However, in this case, conservative management led to a satisfactory clinical outcome.
Figure 1.
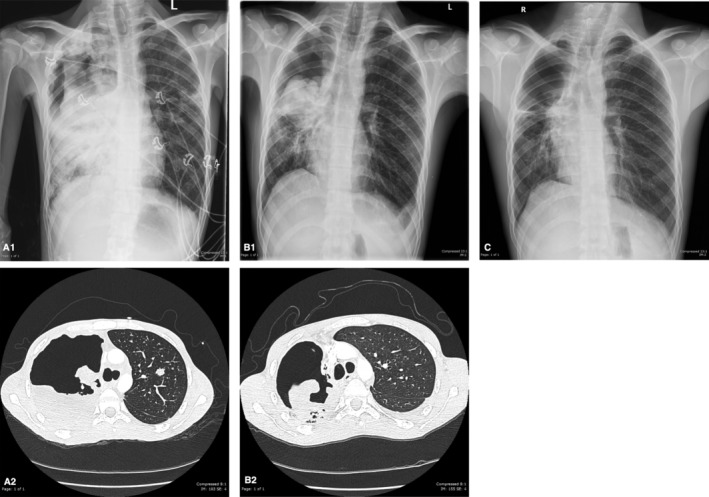
(A1, A2) Chest X‐ray (CXR) and computed tomography (CT) chest showing a large right upper lobe cavity with nodular margins in association with areas of confluent consolidation in the right lung and areas of patchy consolidation in the left lung. (B1, B2) CXR and CT chest displaying a right apical pneumothorax with collapse of the right upper lobe and the right upper lobe cavity in continuity with the pleural space consistent with a bronchopleural fistula. (C) CXR demonstrating resolution of the right and left lobe consolidation and a persisting right upper lobe pneumothorax.
Disclosure Statement
Appropriate written informed consent was obtained for publication of this case report and accompanying images.
Stewart, AGA , Boyd, SC . (2021) Tuberculous bronchopleural fistula. Respirology Case Reports, 9(4), e00740. 10.1002/rcr2.740
Associate Editor: Phan Nguyen
References
- 1. Sarkar P, Chandak T, Shah R, et al. 2010. Diagnosis and management bronchopleural fistula. Indian J. Chest Dis. Allied Sci. 52:97–104. [PubMed] [Google Scholar]
- 2. Shekar K, Foot C, Fraser J, et al. 2010. Bronchopleural fistula: an update for intensivists. J. Crit. Care 25:47–55. [DOI] [PubMed] [Google Scholar]