

Abstract
Background: This study aims to assess COVID-19 related knowledge and practice among the Egyptians in Upper Egypt and to identify barriers that hinder adherence to these preventive measures.
Design and methods: We conducted a cross-sectional study using a structured questionnaire. Data was collected from 21 to 30 August 2020, via both online survey and personal interviews using a non-probability self-nominated sample.
Results: A total of 731 participants completed the questionnaire. The mean age was 32.1± 2.1 and 64.3% were females. The main sources of knowledge were, Internet and Social Media followed by TV then family and friends. More than 96% of the respondents knew the origin, nature, the main symptoms, and the modes of transmission of COVID-19, however, 37.6% of them thought that COVID-19 patients must develop symptoms. 75.8% and 73.6% of the participants respectively covered their nose and mouth during sneezing and washed their hands regularly, 65.4% wore masks in crowded places, while only 31.1% and 30% of them respectively avoided touching their faces or shaking hands with friends. Knowledge and practice were positively correlated and both were linked to younger age and higher education and the female gender was also a predictor of better practice. The most common perceived barriers to adherence to preventive measures were feeling uncomfortable, forgetfulness then financial causes.
Conclusions: the study subjects were aware of COVID-19 and its preventive measures however adherence to some of these measures was not prevalent amongst them, indicating an urgent need of addressing and targeting barriers that hinder adherence to COVID-19 preventive measures in the future policies to prevent the spread of COVID-19 in Egypt.
Significance for public health.
Previous studies were conducted in Egypt to assess knowledge, attitude and perception towards COVID-19 in Egypt, but no study assessed the actual practice regarding COVID-19. This study assessed knowledge and practice of the Egyptians regarding COVID-19 and its preventive measures and the perceived barriers regarding adherence to theses preventive measures. The importance of this topic is that it measures the behavior of the community in preventing spread of COVID-19 after release of lockdown measures by the government which play the main role in this pandemic and identify barriers in order to overcome them.
Key words: COVID-19, knowledge, practice, barriers
Introduction
COVID-19 is an emerging infectious disease caused by a novel coronavirus, now called Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2), that was first discovered in December 2019 in Wuhan city, Hubei Province, China.1 SARS-CoV-2 belongs to the larger family of (RNA) viruses, leading to infections, ranging from the common cold to more serious diseases, such as Middle East Respiratory Syndrome (MERSCoV) and Severe Acute Respiratory Syndrome (SARS-CoV).2 On January 30, 2020, the high transmission capacity of this virus to many countries, and high morbidity and mortality led to the declaration of WHO “SARS-CoV-2 is a public health emergency of international concern”. That was followed later by another declaration of COVID-19 as a global pandemic on 11 March 2020, due to a continual and a huge rise in the number of affected countries. 3COVID-19 is a highly infectious disease, that is transmitted via respiratory secretions through coughing or sneezing and /or contaminated surfaces,4 but evidence of fecal-oral transmission is also available.5 However, more details about the disease are evolving, so that, this may not be the only way of transmission. The main symptoms of COVID-19 that have been identified are fever, dry cough, fatigue, myalgia, shortness of breath, and dyspnea.6,7
In Egypt, by the beginning of April of 2020, there were over 800 confirmed cases of COVID-19, with more than 50 deaths.8 After less than two months, on 25 May 2020, Egypt was among the five countries reporting the highest number of cases in Africa with a total of 17, 265 cases.9 By end of August, there were 98.727 COVID-19 confirmed cases of whom about 39.638 improved cases and 5.399 deaths.8
Since the beginning of the pandemic, several international control measures had been instituted to reduce the spread of the disease, such as banning flights from and to infected countries, the lockdown of most countries, strict quarantine measures, application of social distancing measures for popular gatherings, strict personal hygiene such as frequent hand washing for the proper length of time, sanitization of surfaces and wearing face masks, avoiding close contact with probably infected or sick people, staying at home and isolated when feeling ill.10 Up to the date of this study start, no vaccine is available to prevent the spread of COVID-19. So, accordingly, public adherence to these preventive measures is the main strategy to limit the spread of the disease especially in developing countries, where health systems have, at best, the moderate capacity to respond to outbreaks. Adherence is likely to be influenced by increasing the public’s knowledge about COVID-19 in addition to understanding barriers that may hinder rational practice during this pandemic.11
Several studies were conducted to assess knowledge regarding COVID-19 and practice of the recommended preventive measures in different countries since the beginning of this pandemic. A considerable number of the studied subjects in researches conducted in Saudi Arabia,12 India,13 UK,14 Serbia15 and here in Egypt,16, exhibited true knowledge regarding COVID-19 symptoms, mode of transmission and preventive measures. However, adherence to such preventive measures varied widely between different countries between poor adherence in Nigeria17 and Philippines18 and strict adherence in China19 and Saudi Arabia.12
Understanding public knowledge and acceptance and current adherence to these recommended preventive behaviors can be useful for planning COVID-19 pandemic prevention. In Egypt assessment of knowledge regarding COVID-19 was done, but to our knowledge, no previous studies assessed public practice of COVID-19 preventive measures. So, the current study aims to assess COVID-19 related knowledge and practice of preventive measure and to identify barriers that hinder proper adherence to these preventive measures among the Egyptian community during the second wave of the outbreak in Egypt as indicated by the rising number of cases during August.
Study hypothesis
COVID-19 related knowledge and practice of preventive measures are prevalent among the Egyptian community. COVID- 19 related knowledge and practice of the preventive measures do not differ by socio-demographic variables (age, gender, residence, educational level, and occupation). No barriers are perceived by the community regarding adherence to preventive measures.
Design and Methods
Study design and population
This is a cross-sectional survey conducted among the adult Egyptian community (≥18 years) from 21 to 30 August, during the second wave of COVID 19 pandemic in Egypt. Given social distancing measures and restricted movement during the extraordinary circumstances, the survey was conducted partially via the online survey platform (Google) shared on social media in addition to official sites of the universities and partially through personal interviews that were restricted to those with no access to the social network to limit the spread of infection.
Study subjects and sampling
The sample size was calculated using the Epi Info 7 software, based on the following assumption: the proportion of true knowledge 50%, level of confidence 95% and precision 5%, and design effect 1 to be 384 that is the minimal sample needed. For a proper representation of the Egyptian community, the survey was opened for 10 days to increase the studied sample as much as possible, accordingly, 631 subjects completed the study questionnaire. To overcome the un-representation of illiterate persons,100 illiterate persons were chosen randomly from local markets and interviewed to fill the questionnaires with the help of the researcher. The study subjects were selected using a non-probability, self-nominated sampling technique in total. The study sample was characterized by an overrepresentation of the females (64.3%), urban residents (75.1%) university graduates (52.1%), as internet usage and willingness to fill online surveys were linked more to such categories However, that hinder to some extent proper representation of the total population. Although, assessment of knowledge and practice of such population categories helps to formulate ideas about the current situation of non-educated and rural persons which may be worse.
Study tool
After reviewing the relevant available literature and the WHO’s published resources on COVID-19,20-22 a structured questionnaire was developed by the researchers using closed ending questions. The online survey questionnaire which was designed in Arabic was organized into four sections, the first section collected information on socio-demographic data of the participants such as age, gender, the governorate of residence and whether the residing area is urban or rural, educational level, and occupation. This section also included a question about the sources of knowledge about COVID-19 whether, social media TV, internet, family, or friends.
The second section assessed general knowledge about COVID-19 and knowledge about preventive measures against COVID-19 using 22 items tool. The general knowledge tool included 11 questions related to the nature of the disease, its incubation period, major symptoms of COVID-19, the prognosis of the diseases, groups that develop serious disease, modes of transmission, availability of COVID-19 pharmaceutical treatment, and effective vaccine. Preventive measures knowledge tool included 11questions that assessed knowledge regarding measures that reduce or prevent the spread of COVID -19, such as, the ideal distance that should be maintained in social distancing, the ideal length of time to wash hands, the ideal concentration of alcohol in hand sanitizer, the correct way of wearing a face mask. Questions in this section were also related to avoiding touching face and eyes, avoiding handshaking when meeting friends, the importance of staying at home, and avoiding unnecessary gatherings and crowded places. Responses of the participants to the 22 knowledge items that were either yes or no or I don’t know, were recorded into correct and incorrect answers. A score of 1 was given to each correct answer and 0 to each incorrect or don’t know the answer. The cumulative score ranged from 0 to22 and a higher score indicating a higher knowledge score.
The third section of the questionnaire assessed participants’ practice of COVID -19 preventive measures in the previous two weeks using 10 items tool having 4 point- Likert scale (0 = never, 1 = sometimes, to 2 = always). The practice tool included 10 questions such as whether the participant stayed at home or not, practiced social distancing, covered his\her nose and mouth during coughing or sneezing, washed his\ her hands regularly for enough time, touch routinely his\her eye and mouth, gave handshaking on meeting friends, attended any family or friend gathering and practiced self-isolation on contacting an infected person. For each question, the participant was allowed to choose one answer (always, sometimes, or never). Reverse coding was considered for questions (7.9), The cumulative score ranged from 0 to 20 and a higher score indicates a higher practice score.
The fourth section of the questionnaire included a question about perceived barriers against following safety precautions such as financial causes, unavailability of masks or sanitizers at stores, forgetting, feeling uncomfortable or unaccustomed to preventive measures, and lack of governmental push.
Questionnaire validation and pilot study
Questionnaire face validity and reliability were tested before its use in data collection. First, the degree to which items were relevant and can assess knowledge and practice of the Egyptian participants regarding COVID-19 were assessed by two university experts in epidemiology, and modifications were done as indicated. Then the questionnaire was pretested on 20 participants who were asked to fill the questionnaire twice two weeks apart and excluded from the study sample. The collected data in this phase was used in assessing internal consistency reliability using Cronbach’s alpha which was calculated for both the knowledge domain (22 questions that assessed COVID-19 related knowledge in the second section of the questionnaire) and practice domain (10 questions that assessed practice of COVID-19 preventive measures in the third section of the questionnaire). The analysis revealed a Cronbach’s alpha coefficient of 0.77 for knowledge domain and 0.7 for practice domain in the first time indicating adequate internal consistency that was also proved on retesting the questionnaire after two weeks (Cronbach’s alpha coefficient of knowledge and practice domain were 0.78 and 0.72, respectively). Test-retest reliability also was tested using the interclass correlation coefficient for the knowledge and practice domains and it was 0.8 and 0.7, respectively).
After completion of data collection, Cronbach’s alpha of knowledge and practice domains was calculated for the entire sample and it was found as 0.78 and 0.75, respectively.
Data collection process
Conducting a community based national sampling survey was difficult during this pandemic, so data was collected mainly through an online survey, by providing a link to fill and submit the questionnaire/survey tool. To maximize public outreach, the survey link was distributed to respondents on different social media platforms, such as Facebook, WhatsApp groups, in addition to the University website. And those with no access to smartphones (illiterate) completed the questionnaire by personal interviews, where the researcher filled the questionnaire after asking them. This survey took approximately 8 min to complete. Data privacy was secured and maintained as only core members of the study have access to the data repository. Six hundred and thirty-one (631) questionnaires were completed as Google forms, and 100 were collected as a printed questionnaire.
Statistical analysis
Statistical Package of Social Science (SPSS) version 16 was used in data coding and analysis. Numerical variables were expressed as means and slandered deviations (SD), while frequencies and percentages were considered for categorical data. Comparing the mean score of knowledge and practice between two groups was done using Student’s t-test, while ANOVA test was used in comparing more than two groups. Testing the correlation between knowledge and practice score was done using Pearson correlation. Association between different socio-demographic factors and both knowledge and practice scores were done using multiple linear regression analyses. For the variables occupation and sources of information about COVID-19, they were handled as dummy variables, recoding of this variable was dome where health profession and governmental job and private jobs were re-coded as working and all other categories were re-coded as non-working also social media and internet as sources of information were recoded as one category and other sources were re-coded together as one category.
Results
A total of 731 subjects accepted to participate in the study and completed the survey, about half of them (48.9%) were from Sohag Governorate, 27.3% of them were from Assuit Governorate, 21% were from Qena and 2.7% were from Minia and Aswan. Participants’ age ranged between 18 and 77 years with a mean of 32.1±2.1 years. More than two-thirds of the study subjects were females (470; 64.3%) and the majority (549; 75.1%) were urban residents. As regards their education, more than half of the study subjects (381; 52.1) were university graduates, 22.7% of them had higher studies, 14.8% of them were illiterate, while 9% and 1.4% of them respectively had high school and basic education. Detailed socio-demographic data of the studied subjects are displayed in Table 1.
Sources of COVID-19 information to the study participants were the internet (34.5%), social media (28%), TV (13.8%), friends and family (11.9% and 11.8%, respectively) (Figure 1). Table 2 shows frequency and percentage distribution of participants’ correct answers to 22 items of the COVID-19 knowledge questionnaire. The mean knowledge score was 17.3±2.9, indicating the overall high knowledge of the participants about the disease and its main preventive measures. The majority of the participants were aware of the origin and nature of COVID-19 (97.9%), its main symptoms (96.6%), the main modes of transmission (97.1%), and the high risk of complication among people with underlying medical problems (91.7%) and most of the respondents (85.1%) knew COVID-19 incubation period. Out of the total participants, 83% negated the notion that COVID-19 is a fatal disease with no chance of survival while, 76.6%, and 73.9% respectively, knew that no specific treatment of vaccine is available yet. However, only 62.4% of the participants knew that the development of symptoms is not a must among persons infected with COVID-19. Most of the participants (more than 90%) were aware of all COVID-19 preventive measures assessed by the study, such as social distancing and frequent hand washing for 20 s, avoiding handshaking when meeting friends. Table 3 displays the practice of preventive measures among the participants, the mean practice score was 11.6± 2.6 indicating a lower rate of good practice towards COVID-19. Only half the participants (50.2%) always stayed at home and 41.6% of them always practiced social distancing, moreover, a much lower percentage of the study subjects avoided touching their eyes or faces routinely (31.1%) and never shake hands when meeting a friend (30.6%). On the other hand, about two-thirds of the respondents practiced wearing masks in crowded places (65.4%), self-isolation (62.8%), sanitizing surfaces and surrounding areas (59.5%), and avoided attending parties and family gatherings (62.1%). Most of the participants (75.8%and 73.6% respectively) covered their nose and mouth during sneezing and coughing and washed their hands regularly for enough time. Figure 2 displays perceived barriers against practicing COVID-19 safety precautions among the study participants. About two-thirds of the participants (66.3%) answered that they felt uncomfortable with wearing face masks, 47.3% of them reported that they usually forget and were unaccustomed to it while 45% and 44.3% of them claimed that lack of governmental push and financial causes respectively were barriers against adherence to COVID-19 preventive measures. Almost equal proportions (38%) reported that unavailability of masks or sanitizers at stores and that many other people did not follow SPs constituted barriers to them. Table 4 shows the association between COVID-19 knowledge and practice of safety precautions and both participants’ socio-demographic characteristics and sources of information regarding COVID-19. Both Knowledge and practice score mean scores were significantly higher among younger age, female gender, urban residence, highly educated, health care workers and government workers and those who gained COVID-19 related information from social media and internet (p<0.05). Multiple linear regression analysis results are presented in Tables 5 and 6. Younger age and higher education were predictors of both true knowledge and better practice of COVID-19 related preventive measures. Female gender was also found a predictor of the better practice of the preventive measures of COVID-19 among the study subjects. Figure 3 displays results of correlation between COVID-19 knowledge and practice of safety precautions. A very high significant positive correlation was found between participants knowledge about COVID-19 and practice of universal safety precautions (r=0.46, p<0.001, df=728).
Table 1.
Socio demographic profile of the studied participants.
| Characteristics | Summary statistics (n=731) n, % |
|---|---|
| Age mean (SD) 32.1 (2.1) years | |
| 18-30 | 355 (48.6) |
| 31-45 | 300(41) |
| 46-60 | 61 (8.3) |
| <61 | 15 (2.1) |
| Gender | |
| Males | 261(35.7%) |
| Females | 470 (64.3%) |
| Residence by governorate | |
| Sohag | 358 (48.9) |
| Assuit | 200 (27.3) |
| Qena | 153(21) |
| Other (Minia and Aswan) | 20 (2.7) |
| Residence | |
| Urban | 549 (75.1) |
| Rural | 182 (24.9%) |
| Education | |
| Illiterate | 108 (14.8) |
| Basic education (primary and preparatory) | 10 (1.4) |
| High school education | 66(9) |
| University | 381 (52.1) |
| Master and doctorate degrees | 166 (22.7) |
| Occupation | |
| Unemployed | 156 (21.3) |
| Health professional | 106 (14.5) |
| Governmental job | 162 (22.2) |
| Private work | 151 (20.7) |
| Student | 148 (20.2) |
| Retired | 8 (1.1) |
| Monthly income | |
| Low | 52 (7.1) |
| Medium | 570 (78.1) |
| High | 108 (14.8) |
Figure 1.
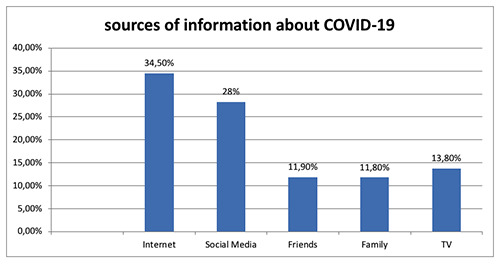
Sources of knowledge about COVID-19 among the study participants.
Table 2.
Distribution of the study participants by their correct answers on questions of COVID-19 knowledge questionnaire.
| Knowledge item | Correct answer (n=731) n, (%) |
|---|---|
| General knowledge regarding COVID-19 | |
| COVID-19 is an infectious disease caused by the most recently discovered novel coronavirus in Wuhan, China. | 714 (97.9) |
| The incubation period of COVID-19 is 14 days | 622 (85.1) |
| Fever, dry cough, tiredness, and body pains are the most common symptoms in COVID-19 | 706 (96.6) |
| Any person infected with COVID-19 definitely develops symptoms | 456 (62.4) |
| COVID-19 is a fatal disease as there is no chance of survival once the person is infected | 607(83) |
| Those with underlying medical problems like high BP, heart problems or diabetes, and old people are more likely to develop serious illness | 670 (91.7) |
| COVID-19 spread by droplets of affected person during cough or expiration | 710 (97.1) |
| COVID-19 can also spread by touching coins and banknotes | 38 (5.2) |
| COVID-19 can be transmitted through the air | 232 (31.7) |
| Medicines are available in the global market to prevent or treat COVID-19 | 540 (73.9) |
| An effective vaccine against the virus is currently available | 560 (76.6) |
| Knowledge regarding COVID-19 preventive measures | |
| Maintaining good personal hygiene and being socially responsible would prevent the spread of COVID-19 | 713 (97.5) |
| Washing hands frequently using soap for 20 s would prevent the spread of COVID-19 | 682 (93.3) |
| The use of hand sanitizer or alcohol 70% would prevent the spread of COVID-19 | 656 (89.7) |
| Avoiding handshaking behavior would prevent the spread of COVID-19 | 694 (94.9) |
| Avoiding placing fingers into eyes, nose, and mouth would prevent the spread of COVID-19 | 671 (91.8) |
| Coughing and sneezing into the elbow or within the clothing is a good practice in preventing the spread of COVID-19 | 679 (92.9) |
| Limiting eating meat, eggs, and fishes would prevent the spread of COVID-19 | 470 (64.3) |
| Following social distancing measures and avoiding crowded places would limit the spread of COVID-19 | 699 (95.6) |
| For someone without any symptoms of COVID-19, wearing a face mask is considered an appropriate and protective measure against COVID-19 | 643(88) |
| Proper usage of face mask during an outbreak should include covering nose, mouth, and chin with the colored side facing outside | 705 (94.6) |
| Staying at home would play a significant role in preventing the spread of COVID-19 | 679 (92.9) |
| Knowledge score (min-max) | 1-22 |
| Mean knowledge score ±SD | 17.3±2.9 |
Discussion
Since the beginning of the pandemic on 11th March 2020, till the 3rd of September 26,254,453 cases of COVID-19 and 868,809 deaths were recorded, while 18,500,721 persons were recovered.23 Egypt is among the most populous countries in Africa,24 where a higher risk of an enormous spread of coronavirus present and led to the exhaustion of the available health services. So the Egyptian Government adopted a series of preventive measures to face the COVID-19 pandemic including a partial lockdown of the country, night curfew and isolation of infected places, and forcing the use of personal protective measures like face masks. Since 27 June 2020, the government eased restrictions put on restaurants, cafes, and clubs and lift lockdown to limit the economic impact of the pandemic. Re-opening of the country put the main burden of preventing COVID-19 spread on Egyptian individuals by adherence to preventive measures.
This study aims to assess COVID-19 related knowledge and practice of preventive measures among the Egyptian community and to identify perceived barriers against adherence to these preventive measures. Understanding gaps between knowledge and practice and its backgrounds can help in planning effective control policies in the future wave of the pandemic or future outbreaks. Moreover, to the best of our knowledge, no previous study assessed the practice of preventive measures among the Egyptian community.
Figure 2.
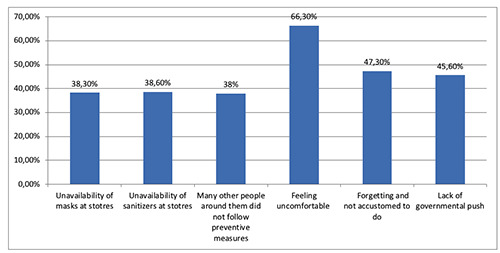
Participants’ perceived barriers against adherence to COVID-19 preventive measures in Egypt.
Table 3.
Practice of the study participants regarding preventive measures against COVID-19.
| Practice item | Always | Sometimes | Never |
|---|---|---|---|
| n, (%) | n, (%) | n, (%) | |
| How often do you avoid going outside and stay at home during this COVID-19 pandemic? | 367 (50.2) | 331(45.3) | 33 (4.5) |
| How often do you cover your mouth and nose when sneezing with a tissue or elbow? | 554 (75.8) | 169 (23.1) | 8 (1.1) |
| Do you wear a mask when you enter any crowded place such as market or governmental institutions? | 478 (65.4) | 215 (29.4) | 38 (5.2) |
| Do you follow social distancing (>1 m) when you meet other people or fiends? | 304 (41.6) | 354 (48.4) | 73(10) |
| Do you wash your hands regularly and for enough period of time? | 538 (73.6) | 181 (24.8) | 12 (1.6) |
| If you contact a probably infected person with COVID-19, do you isolate yourself at home? | 459 (62.8) | 155 (21.2) | 117(16) |
| Have you been in any ceremony like funeral or marriage parties? | 49 (6.7) | 228 (31.2) | 454 (62.1) |
| Do you sanitize the surfaces which are suspected of infection exposure? | 435 (59.5) | 242 (33.1) | 54 (7.4) |
| Do you give shake hand when you meet friends/family members/others? | 143 (19.6) | 362 (49.5) | 226 (30.9) |
| How often do you routinely touch your mouth, nose, and eyes? | 113 (18.2) | 371 (50.8) | 227 (31.1) |
| Mean practice of safety precaution score± SD. Min-max | 11.6±2.6 | ||
| 1-17 |
Since the declaration of the pandemic, people have sought relevant scientific information about this disease from every possible data source. Egypt’s Ministry of Health (MOH) used all means of communications, such, as television, mobile messages, and even sponsored ads on social media platforms (Facebook, Twitter, and Snapchat) in educating the public about the disease and its main preventive measures. Accordingly, it was not surprising that the study participants were well aware of COVID-19, and the mean knowledge score was17.3±2.9. These findings are in agreement with many previous studies conducted in Egypt,16 Saudi Arabia,12 India,13 UK14 and Serbia.15
The main sources of COVID-19 information to the study participants were the internet, followed by social media, TV, friends and family. These results are in line with the results of Abdehafez et al. in Egypt, who found that the most commonly stated sources of knowledge were social media (66.9%), the internet (58.3%) followed by TV/satellite channels (52.6%). Other sources included friends or family members (38.1%).16 The dominance of the internet as a source of knowledge about COVID- 19 was also reported in Jordan among (77.1%) of the studied university students, followed by TV (67.6%). While a very small proportion of the participants (7%) obtained their information from other sources such as friends and family.25 Similarly, Alzoubi et al.26 stated that social media was the most common source of information for Mutah university students. Also, Mohammed et al.12 claimed that people have gained awareness and knowledge about the disease and its transmission, via media platforms and television, to protect themselves and their families.
Figure 3.
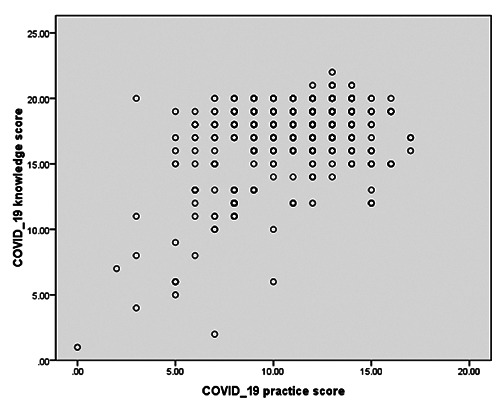
Correlation between COVID-19 knowledge and practice of safety precautions among the studied participants, Egypt.
Table 4.
Relation between COVID-19 knowledge and practice of safety precaution and socio demographic characteristics of the studied Egyptian participants and sources of COVID-19 related information.
| Variable | Knowledge score | Safety precaution practice score | ||||
|---|---|---|---|---|---|---|
| Mean (SD) | Test of sig | Mean | Test of sig | |||
| (p value) | (SD) | (p value) | ||||
| Age | F=12.23 | F=4.36 | ||||
| 18-30 | a | 17.7 (2.6) | (<0.001)* | 11.3 (2.7) | (0.005)* | |
| 31-45 | b | 17.6 (2.5) | a vs c; <0.001** | 11.5 (2.4) | a vs c; 0.04** | |
| 46-60 | c | 15.6 (3.7) | b vs c; <0.001** | 10.4 (2.3) | b vs c; 0.013** | |
| 61< | d | 16 (3.2) | df= 727 | 10 (2.7) | df= 727 | |
| Gender | t= 57.5 | t=28.4 | ||||
| Males | 16.5 (3.5) | (<0.001)* | 11.1(3) | (<0.001)* | ||
| Females | 17.8 (2.3) | df= 729 | 11.9 (2.2) | df= 729 | ||
| Residence | t= 8.76 | t=9.353 | ||||
| Urban | 17.8 (2.4) | (<0.001)* | 11.7 (2.5) | (0.002)* | ||
| Rural | 15.9 (3.7) | df= 729 | 11.4 (2.9) | df= 729 | ||
| Education | F=53.3 | F= 15.075 | ||||
| Illiterate | a | 12.2(3) | (< 0.001)* | 9.9 (3.6) | (< 0.001)* | |
| Basic education (primary and preparatory) | b | 15.1 (4.1) | a vs c, a vs d, a vs e; | 8.9 (3.2) | a vs d; (<0.001),** | |
| High school education | c | 17.3 (3.3) | (<0.001)** | 10.9 (2.9) | a vs e; (<0.001),** | |
| University | d | 18.3 (1.7) | b vs c; 0.02, b vs d; (<0.001), | 11.6 (2.3) | b vs d; 0.009, ** | |
| b vs e; (<0.001)** | ||||||
| Master& doctorate degrees | e | 18.4 (1.3) | c vs d; 0.004, c vs e; 0.004** | 11.6 (1.9) | b vs e; 0.01** | |
| df= 726 | df= 726 | |||||
| F=8.1 | F=1.794 | |||||
| Occupation | a | 16.6(3) | (<0.001)* | 11.6 (2.7) | (0.02)* | |
| Unemployed | b | 18.2 (2.1) | a vs b, a vs e; (<0.001)** | 11.3 (2.3) | a vs f; 0.04** | |
| Health professional | c | 17.8 (2.2) | b vs d; 0.002** | 11.4 (2.4) | c vs f; 0.05** | |
| Governmental job | d | 16.9 (3.3) | c vs f; 0.03** | 11.1 (2.7) | df=725 | |
| Private work | e | 18.1 (2.2) | d vs f; 0.003** | 11 (2.8) | ||
| Student | f | 14.8 (5.3) | e vs f; 0.01** | 9.6 (3.8) | ||
| Retired | df=725 | |||||
| F=29.5 | ||||||
| Sources of knowledge | F=3.4 | |||||
| Social media | a | 18.2 (2.1) | (<0.001)* | 11.6 (2.3) | (0.009)* | |
| Internet | b | 17.9 (2.2) | a vs d, a vs, e; (<0.001)** | 11.2 (2.4) | ||
| TV | c | 18 (1.8) | b vs c, b vs, e; (<0.001)** | 11.7 (2.3) | df=726 | |
| Friends | d | 15.7 (3.6) | c vs d, c vs, e; (<0.001)** | 10.7 (3.1) | ||
| Family | e | 15.4 (3.6) | df= 726 | 10.8(3.2) | ||
t, Students t-test; F, analysis of variance (ANOVA test); *statistically significant at p<0.05; **categories of variables with significant ANOVA results, multiple comparisons between each 2 categories are done by posthoc analysis (Hochberg G2); df, degree of freedom.
The overall COVID-19 knowledge among our participants was optimal especially that related to knowledge about preventive measures. Although, serious myths are present, as more than onethird of the respondents (37.6%) thought that any COVID-19 cases develop symptoms. This misunderstanding leads to serious effects as it gives a false sense of security and enhances the spread of coronavirus from asymptomatic cases. Moreover, one-fourth of the respondents thought that treatment or vaccine for COVID-19 are currently available or just do not know the precise fact. This may lead to underestimation of the seriousness of the disease and the needed preventive measures. These misunderstandings indicate the need for a continuous supply of the public with timely accurate information.
Predictors of good knowledge in this study were the age and educational level of the respondent. Participants of the age groups 18-30 and 30-45 were more aware of COVID-19 compared to older age groups. These findings are comparable to many previous studies.12,16,19 Younger age is linked with longer time spent on social media, which enhances acquiring more knowledge about the pandemic. Although our results disagree with the Bawazir et al.’s study,27 who claimed that older people had better knowledge that arises from worry about their liability to develop a serious disease.
In line with previous literature,12,15,18 participants’ education was a strong predictor of good knowledge related to COVID-19. The linkage between the educational level of the participants and COVID-19 knowledge score is not surprising, the more educated a person was, the more knowledge they seek about major events or diseases, and the better understanding they had of the proposed preventive measures.
The mean practice score was 11.6±2.6. Irrational practice related to COVID-10 preventive measures among the study subjects agrees with many previous studies conducted in Nigeria,17 Philippines,18 Pakistan29 and Bangladesh.28 Although, Zhong et al. in China19 and Roy et al. in India,30 reported optimal public adherence to COVID-19 preventive measures. The suboptimal practice of the Egyptians in the current study may be due to understanding ease of restrictions as an indication of the end of COVID-19 danger. Especially when combined with the economic impacts of lockdown on a higher percentage of the Egyptians with low income. Out of the total study participants, only 36.7% of them were governmental employees with constant monthly income, compared to the rest whose income depended on their private daily work.
Table 5.
Predictors of good practice of COVID-19 preventive measures among the study participants by multiple linear regression analysis.
| Predictor coefficients | Unstandardized coefficients | Standardized | t | p | Residual df | Adjusted R square | |
|---|---|---|---|---|---|---|---|
| B | SE | Beta | |||||
| Knowledge | 725 | 0.406 | |||||
| Constant | 14.633 | 0.801 | 18.266 | 0.000 | |||
| Age | -0.043 | 0.008 | -0.162- | -5.199 | 0.000* | ||
| Gender | 0.222 | 0.172 | 0.038 | 1.188 | 0.19 | ||
| Residence | -0.125 | 0.205 | -0.019 | -0.611 | 0.54 | ||
| Education | 1.291 | 0.078 | 0.584 | -16.561 | 0.000* | ||
| Occupation | -0.157 | 0.187 | -0.027- | -0.841 | 0.4 | ||
| Sources of information | 0.258 | 0.178 | 0.045 | 1.446 | 0.149 | ||
| Practice | 725 | 0.062 | |||||
| Constant | 9.963 | 0.714 | 13.948 | 0.000 | |||
| Age | -0.019 | 0.010 | -0.077 | -1.962 | 0.045* | ||
| Gender | 0.565 | 0.205 | 0.103 | 2.763 | 0.006* | ||
| Residence | 0.023 | 0.243 | 0.004 | 0.093 | 0.926 | ||
| Education | 0.455 | 0.093 | 0.218 | 4.911 | 0.000* | ||
| Occupation | -0.193 | 0.222 | -0.036 | -1.646 | 0.04 | ||
| Sources of information | 0.017 | 0.243 | 0.003 | 0.067 | 0.946 | ||
t, Students t-test; *statistically significant.
Table 6.
Final regression model of predictors of COVID-19 knowledge and practice of COVID-19 safety precautions among the study participants,
| Variable | Coefficient | SE | t | p | Residual df | Adjusted R square |
|---|---|---|---|---|---|---|
| Knowledge | 728 | 0.406 | ||||
| Age | -0.179 | 0.008 | -6.276 | 0.000 | ||
| Education | 0.606 | 0.063 | 21.246 | 0.000 | ||
| Practice | 727 | 0.062 | ||||
| Age | -0.080 | 0.009 | -2.232 | 0.026 | ||
| Gender | 0.103 | 0.204 | 2.778 | 0.006 | ||
| Education | 0.192 | 0.077 | 5.182 | 0.000 |
Items of preventive measures that were the least practiced in the previous two weeks by the study participants, were avoiding shaking hands when meeting friends and touching face and eye (30.6% and 31.1%, respectively). This can be linked to the power of habits and the friendly personality of the Egyptians. In agreement with Lau et al.,18 practicing social distancing was reported by only 41.6% of the participants, this can be linked to overcrowding seen in each facility or street due to high population density especially in urban areas where about two-thirds of the participants resided (64.3%). On the other hand, about two-thirds of the respondents practiced wearing masks in crowded places (65.4%), which was higher than what was reported by Lau et al.18 Most of the participants (75.8%and 73.6% respectively) covered their nose and mouth during sneezing and coughing and washed their hands regularly for enough time. These results are comparable to Afzal et al. in Pakistan.29 Predictors of good practice of COVID-19 preventive measures among the study participants were younger age and higher education and female gender. Although, Azlan et al.31 reported that older persons were more adherent to COVID-19 preventive measures. Higher education was a strong predictor of rational practice related to COVID-19, in agreement with studies conducted in Saudi Arabia, Malaysia, and Pakistan.31,32 Also in agreement with Al-Hanawi et al. and Narayana et al.,12,33 female gender was a predictor of good practice. Besides, a significant positive correlation was found between knowledge and practice in line with Zhong et al.19 and Lau et al.18 Although the study sample was not random and has problems of over-representation of females, urban and well-educated persons, the provided findings help us to predict that the level of knowledge and practice can be worse in under-represented groups of the population. The perceived barriers against practicing COVID-19 preventive measures among the study participants were mainly feeling uncomfortable with the use of masks and other preventive measures, forgetfulness, and unaccustomed to it. A proportion of them claimed lack of governmental push and financial causes respectively. Almost an equal proportion (38%) reported that the unavailability of masks or sanitizers at stores was another barrier to them. This could explain the poor practice in presence with overall good knowledge among the study subjects. These findings in line with previous literature,34-37 that claimed that lack of resources, health literacy, poverty are among the most severe barriers in the prevention of COVID-19. On the other hand, Noreen et al.35 in Pakistan concluded that low literacy rate and general lack of awareness were limitations for people in practicing social distancing and hand hygiene.
Limitations
Using an online survey in data collection was the main limitation. As the sample was not random, females, urban residence, and highly educated were overrepresented in the study. Besides the absence of participants from other governorates in Lower Egypt, hinder the generalization of the study results on all the country.
Conclusions
Prevention of COVID-19 pandemic can be accomplished by collaboration between political policy and public behavior taking into considerations compacting barriers that hinder proper behavior among the public. The Egyptian participates of the current study exhibited true knowledge about COVID-19 and its preventive measures although some myths were presents as a considerable proportion of the study subjects thought that every diseased person with COVID-19 will develop symptoms and the main sources of information to the study subject were the internet and social media, However, respondent’s practice regarding COVID- 19 preventive measures had many problems especially regarding the habits of shaking hands and touching the face and nose. Younger age and higher education were predictors of better knowledge, while predictors of good practice included young age, female gender, high education, and better COVID-19 related knowledge. Perceived barriers to adherence to preventive measures according to the study participants were feeling uncomfortable, forgetfulness, financial causes, lack of governmental push, and un-availability of face masks and sanitizers at stores. Designing future policies for the prevention of COVID-19 needs to address correcting COVID- 19 related misperceptions taking into consideration best use of the internet and social media platform in directing and modeling health awareness and health behavior of the community together with governmental help in compacting and removing barriers that hinder adherence to the recommended COVID-19 preventive measures.
Acknowledgments
We thankfully acknowledge the cooperation of our participants in spending time in filling the survey questionnaire and also the dedications of our friends and colleges in sharing the questionnaire on social media.
References
- 1.Wu F, Zhao S, Yu B, et al. A new coronavirus associated with human respiratory disease in China. Nature 2020;579:265–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Zhou P, Yang X-L, Wang X-G, et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020;579:270–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.WHO. Director-General’s opening remarks at the media briefing on COVID-19-11 March 2020. Accessed: May 13, 2020. Available from https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-themedia-briefing-on-covid-19---11-march-2020 [Google Scholar]
- 4.Chan JF, Kok KH, Zhu Z, et al. Genomic characterization of the 2019 novel human-pathogenic coronavirus isolated from a patient with atypical pneumonia after visiting Wuhan. Emerg. Microbes Infect 2020;9:221-36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Holshue ML, DeBolt C, Lindquist S, et al. First case of 2019 novel coronavirus in the United States. N Engl J Med 2020;382:929-36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Riou J, Althaus CL. Pattern of early human-to-human transmission of Wuhan 2019 novel coronavirus (2019-nCoV), December 2019 to January 2020. Euro Surveill 2020;25:2000058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Chan JF, Yuan S, Kok K, et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating personto- person transmission: a study of a family cluster. Lancet 2020;395:514-23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Egypt Today [Internet]. PM: Egypt’s coronavirus figures still within range. Accessed: April 17, 2020. Available from: https://www.egypttoday.com/Article/1/83291/PMEgypt%E2%80%99s-coronavirus-figures-still-within-range [Google Scholar]
- 9.European Centre for Disease Prevention and Control [Internet]. COVID-19 situation update worldwide, as of 25 May 2020. [Google Scholar]
- 10.Cowling BJ, Leung GM. Epidemiological research priorities for public health control of the ongoing global novel coronavirus (2019-nCoV) outbreak. Euro Surveill 2020;25:2000110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Chirwa GC. “Who knows more, and why?” Explaining socio economic related inequality in knowledge about HIV in Malawi. Sci African 2020;7:e00213. [Google Scholar]
- 12.Al-Hanawi MK, Angawi K, Alshareef N, et al. Knowledge, attitude and practice toward COVID-19 among the public in the Kingdom of Saudi Arabia: A cross-sectional study. Front Public Health 2020;8:217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Dkhar SA, Quansar R, Saleem SM, Khan SM. Knowledge, attitude, and practices related to COVID-19 pandemic among social media users in J&K, India. Indian J Public Health 2020;64:S205-10. [DOI] [PubMed] [Google Scholar]
- 14.McFadden SM, Malik AA, Aguolu OG, et al. Perceptions of the adult US population regarding the novel coronavirus outbreak. PLoS One 2020;15:e0231808. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Cvetković VM, Nikolić N, Nenadić UR, et al. Preparedness and preventive behaviors for a pandemic disaster caused by COVID-19 in Serbia. Int J Environ Res Public Health 2020;17:4124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Abdelhafz AS, Mohammed Z, Ibrahim ME, et al. Knowledge, perceptions, and attitude of Egyptians towards the novel coronavirus disease (COVID-19). Journal of Community Health 2020;45:881-90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Reuben RC, Danladi MM, Saleh DA, Ejembi PE. Knowledge, attitudes and practices towards COVID-19: An epidemiological survey in North-Central Nigeria. J Community Health 2020;7;1-14. [Epub ahead of print]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Lau LL, Hung N, Go DJ, et al. Knowledge, attitudes and practices of COVID-19 among income-poor households in the Philippines: A cross-sectional study. J Glob Health 2020;10:011007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Zhong BL, Luo W, Li HM, et al. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: A quick online cross-sectional survey. Int J Biol Sci 2020;16:1745-52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.WHO. Coronavirus disease (COVID-19) advice for the public. Accessed: April 1, 2020. Available from https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public#:~:text=If%20COVID%2D19%20is%20spreading,Do%20it%20all [Google Scholar]
- 21.Fricker RD. Sampling methods for web and e-mail surveys. Fielding N., Lee R.M., Blank G., Editors. The Sage handbook of online research methods. London: SAGE Publication; 2008. p. 195-216. [Google Scholar]
- 22.Eysenbach G. Improving the Quality of Web Surveys: The Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J Med Internet Res 2004;6:e34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Worldometer [Internet]. COVID-19 corona virus pandemic. Available from: https://www.worldometers.info/coronavirus/?utm_campaign=homeAdvegas1? [Google Scholar]
- 24.Central Agency for Public Mobilization and Statistics [Internet]. [Population clock, Egypt now].[in Arabic]. Accessed: April 4, 2020. Available from: http://www.capmas.gov.eg/Pages/populationClock.aspx [Google Scholar]
- 25.Olaimat AN, Aolymat I, Hafiz M, Holley SR. Knowledge and information sources about COVID-19 among university students in Jordan: A cross-sectional study. Front Public Health 2020;8:254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Alzoubi H, Alnawaiseh N, Al-Mnayyis A, et al. COVID-19 - knowledge, attitude and practice among medical and non-medical university students in Jordan. J Pure Appl Microbiol 2020;14:17-24. [Google Scholar]
- 27.Bawazir A, Al-Mazroo E, Jradi H, et al. MERS-CoV infection: mind the public knowledge gap. J Infect Public Health 2018;11:89-93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Paul A, Sikdar D, Hossain MM, et al. Knowledge, attitudes, and practices toward the novel coronavirus among Bangladeshis: Implications for mitigation measures. PLoS One 2020;15:e0238492. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Afzal MS, Khan A, Qureshi UUR, et al. Community-based assessment of knowledge, attitude, practices and risk factors regarding COVID-19 among Pakistanis residents during a recent outbreak: A cross-sectional survey. J Community Health 2020;1-11. [Epub Ahead of Print]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Roy D, Tripathy S, Kar SK, et al. Study of knowledge, attitude, anxiety & perceived mental healthcare need in Indian population during COVID-19 pandemic. Asian J Psychiatr 2020;51:102083. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Azlan AA, Hamzah MR, Sern TJ, et al. Public knowledge, attitudes and practices towards COVID-19: A cross-sectional study in Malaysia. PLoS One 2020;15:e0233668. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Salman M, Mustafa Z, Asif N, et al. Knowledge, attitude and preventive practices related to COVID-19 among health professionals of Punjab province of Pakistan. J Infect Dev Ctries 2020;14:707-12. [DOI] [PubMed] [Google Scholar]
- 33.Narayana G, Pradeepkumar B, Ramaiah JD, et al. Knowledge, perception, and practices towards COVID-19 pandemic among general public of India: A cross-sectional online survey. Curr Med Res Pract 2020;10:153-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Maqbool A, Khan NZ. Analyzing barriers for implementation of public health and social measures to prevent the transmission of COVID-19 disease using DEMATEL method. Diabetes Metab Syndr 2020;14:887-92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Noreen N, Dil S, Niazi SU, et al. Coronavirus disease (COVID-19) pandemic and Pakistan; Limitations and gaps. Global Biosecurity 2020;1(3). [Google Scholar]
- 36.Yazdani A, Wells R. Barriers for implementation of successful change to prevent musculoskeletal disorders and how to systematically address them. Appl Ergon 2018;73:122-40. [DOI] [PubMed] [Google Scholar]
- 37.Lucero-Prisno D III, Adebisi Y, Lin X. Current efforts and challenges facing responses to 2019-nCoV in Africa. Global Health Res Policy 2020;5:21. [DOI] [PMC free article] [PubMed] [Google Scholar]