

Abstract
Background:
Children reared in institutions experience profound deprivation that is linked to impairments in social communication (SC). However, little is known about the long-term consequences of institutional rearing on SC through adolescence, and how SC deficits relate to broad-spectrum psychopathology. It is also unclear whether early removal from deprivation and placement into socially-enriched environments remediates these difficulties.
Methods:
Children reared in Romanian institutions from the Bucharest Early Intervention Project were randomly assigned to care as usual or foster care intervention in early childhood. An age- and sex-matched group of never-institutionalized children was also recruited. SC data from 208 children at age 8 and 129 children at 16 were collected using the Social Communication Questionnaire. Psychopathology was assessed as saved factor scores for general (P) and specific internalizing (INT) and externalizing (EXT) problems. We examined (i) whether institutional rearing is associated with continued SC deficits into adolescence; (ii) whether early placement into foster care mitigates risk for SC problems; and (iii) associations between SC and psychopathology from middle childhood (age 8) to adolescence (age 16).
Results:
Findings suggest that: (i) institutionally-reared children have significantly more SC problems than never-institutionalized children at age 16; (ii) children placed into foster care early in life have fewer problems with reciprocal social interaction compared to those with prolonged institutional rearing; and (iii) deficits in SC at age 8 partially account for the link between institutional rearing and general psychopathology at age 16.
Conclusions:
Early deprivation is associated with impairments in SC that persist into adolescence, with evidence for the remedial benefit of family-based care in the domain of reciprocal social interaction. Moreover, deficits in SC among ever-institutionalized children in middle childhood may increase the risk of broad-spectrum psychopathology in adolescence, thus providing one putative target for early intervention to safeguard against later psychiatric problems.
Keywords: Institutional rearing, severe early neglect, maltreatment, social communication, psychopathology, foster care intervention
Child maltreatment is a pervasive problem affecting up to one billion children worldwide (Hillis, Mercy, Amobi, & Kress, 2016). Neglect is overwhelmingly the most common form of maltreatment, accounting for over 75% of substantiated cases (U.S. Department of Health and Human Services, 2018). A particularly severe form of neglect is being raised in institutions characterized by profound psychosocial deprivation, including the absence of a primary caregiver, lack of responsiveness to distress, and poor social, cognitive, and sensory stimulation. The long-term effects of early deprivation on brain and behavioral development have been documented in several influential studies of post-institutionalized children taking place in the United Kingdom, Russia, Greece, China, and Romania, among others (Muhamedrahimov et al., 2014; Sonuga-Barke et al., 2017; Tan, 2009; Vorria, Ntouma, & Rutter, 2015; Zeanah, Humphreys, Fox, & Nelson, 2017). While there is heterogeneity in the results across these studies with respect to the duration of deprivation and timing of adoption, most converge on the conclusion that institutionally-reared children have more social, cognitive, and psychiatric difficulties than non-deprived children that may persist years after removal from institutions.
An interesting and replicable finding across studies of post-institutionalized children is a deprivation-related phenotype termed “quasi-autism” or “post-institutional autistic syndrome” which is primarily marked by aberrant patterns of social communication (Hoksbergen, Ter Laak, Rijk, van Dijkum, & Stoutjesdijk, 2005; Rutter et al., 1999; Rutter et al., 2007). Social Communication (SC) refers to the skills with which children communicate verbally and non-verbally in social contexts. Unlike conventional cases of autism where psychosocial deprivation is not implicated, deprivation of institutionally-reared children may aggravate underlying risk factors such as genetic predispositions or prenatal exposures that contribute to SC problems throughout childhood. However, little is known about the long-term effects of early deprivation on SC in adolescence, as very few studies have tracked children through this period. In one prominent study, the English and Romanian Adoptees (ERA) study, Romanian adoptees who experienced more than 6 months of deprivation showed persistently higher SC problems than those with less than 6 months of deprivation and a group of non-deprived adoptees (Sonuga-Barke et al., 2017). These effects were observed by age 6 years and persisted into adolescence and early adulthood.
Another study that has examined the relations between institutionalization and SC is the Bucharest Early Intervention Project (BEIP), a randomized controlled trial (RCT) of foster care as an alternative to institutional care. Due to its randomized design, this study permits an experimental evaluation of how social enrichment afforded by foster care may protect against later problems. In the BEIP, institutionally-reared children have been shown to have more SC problems at age 8–10 years compared to a matched sample of never-institutionalized children (Levin, Fox, Zeanah Jr, & Nelson, 2015). Moreover, children placed into foster care early in life had fewer problems with reciprocal social interaction than those experiencing prolonged institutional rearing. Using data from the most recent wave of BEIP (age 16 years), the first primary goal of the current study was to examine whether institutionally-reared children continue to show more SC difficulties in adolescence, and whether the benefits of foster care intervention are maintained through this period.
The secondary goal of the current study was to examine the relation between deficits in SC and broad-spectrum psychopathology among institutionally-reared children. Epidemiological studies have shown that deficits in SC are associated with depression and psychotic experiences at 12 and 18 years (Sullivan, Thompson, Kounali, Lewis, & Zammit, 2017), as well as social anxiety from 7 to 10 years (Pickard, Rijsdijk, Happé, & Mandy, 2017). In children with classical autism, high rates of social anxiety disorder, attention-deficit hyperactivity disorder (ADHD), and oppositional defiant disorder (ODD) are observed (Simonoff et al., 2008), suggesting those with pronounced SC difficulties are at an increased risk for developing other psychiatric problems. Despite the clear overlap between SC deficits and heightened psychiatric morbidity, it remains unclear whether this association is directional or reciprocal. There is some evidence to suggest that early SC difficulties predict later social anxiety, but not the reverse (Pickard et al., 2017), perhaps indicating that SC deficits are involved in the pathogenesis of certain psychiatric conditions. Another unresolved issue is whether SC deficits are associated with a specific domain of psychopathology, or are transdiagnostically linked to multiple problems. As outlined above, the occurrence of SC deficits in several psychiatric disorders raises the possibility that this association cuts across diagnostic boundaries, as opposed to being disorder-specific.
To address these issues, we tested the following aims. First, we examined whether institutional rearing is associated with impairments in SC in adolescence (age 16 years). Second, we examined whether early placement into foster care mitigates risk for SC problems at this age. Third, we tested reciprocal relations between SC and psychopathology from middle childhood (age 8) to adolescence (age 16), including the mediating role of SC in the relation between institutional rearing and psychopathology (and vise versa). In this model, we used latent dimensions of general (P) and specific internalizing (INT) and externalizing (EXT) psychopathology to test whether the link between SC and psychopathology is transdiagnostic via associations with P, or specific to the INT or EXT dimensions.
Methods
Participants
Participants were children from BEIP (clinicaltrials.gov identifier: NCT00747396), a longitudinal RCT examining the effects of institutional rearing and foster care intervention on children’s brain and behavioral development. The study commenced in April 2001. The adolescent follow-up (age 16 years) was completed in September 2018. At a mean age of 22 months, 187 children living in institutions in Bucharest, Romania were assessed for eligibility by a pediatrician. Exclusion criteria included the presence of genetic syndromes, fetal alcohol syndrome, and micro- or macrocephaly. A total of 136 children met the inclusion criteria. Half of those children were then randomly assigned to a care as usual group (CAUG; remained in institutions), and half were assigned to a foster care intervention group (FCG) by drawing names from a hat. A description of the intervention is provided in Zeanah et al. (2017), and ethical considerations for randomization have been discussed previously (Zeanah, Fox, & Nelson, 2012). Baseline characteristics of the CAUG and FCG children are presented in Table S1. Together, these two groups are referred to as the ever-institutionalized group (EIG). An age- and sex-matched sample of 72 never-institutionalized children (NIG) reared in their biological families served as a comparison group. Study procedures were approved by the institutional review boards of the principal investigators and the local Commissions on Child Protection in Bucharest. Signed consent was obtained from each child’s legal guardian, and written or verbal assent was obtained from each child. The CONSORT diagram showing group assignment and progress of participants through the trial is presented in Figure 1.
Figure 1.
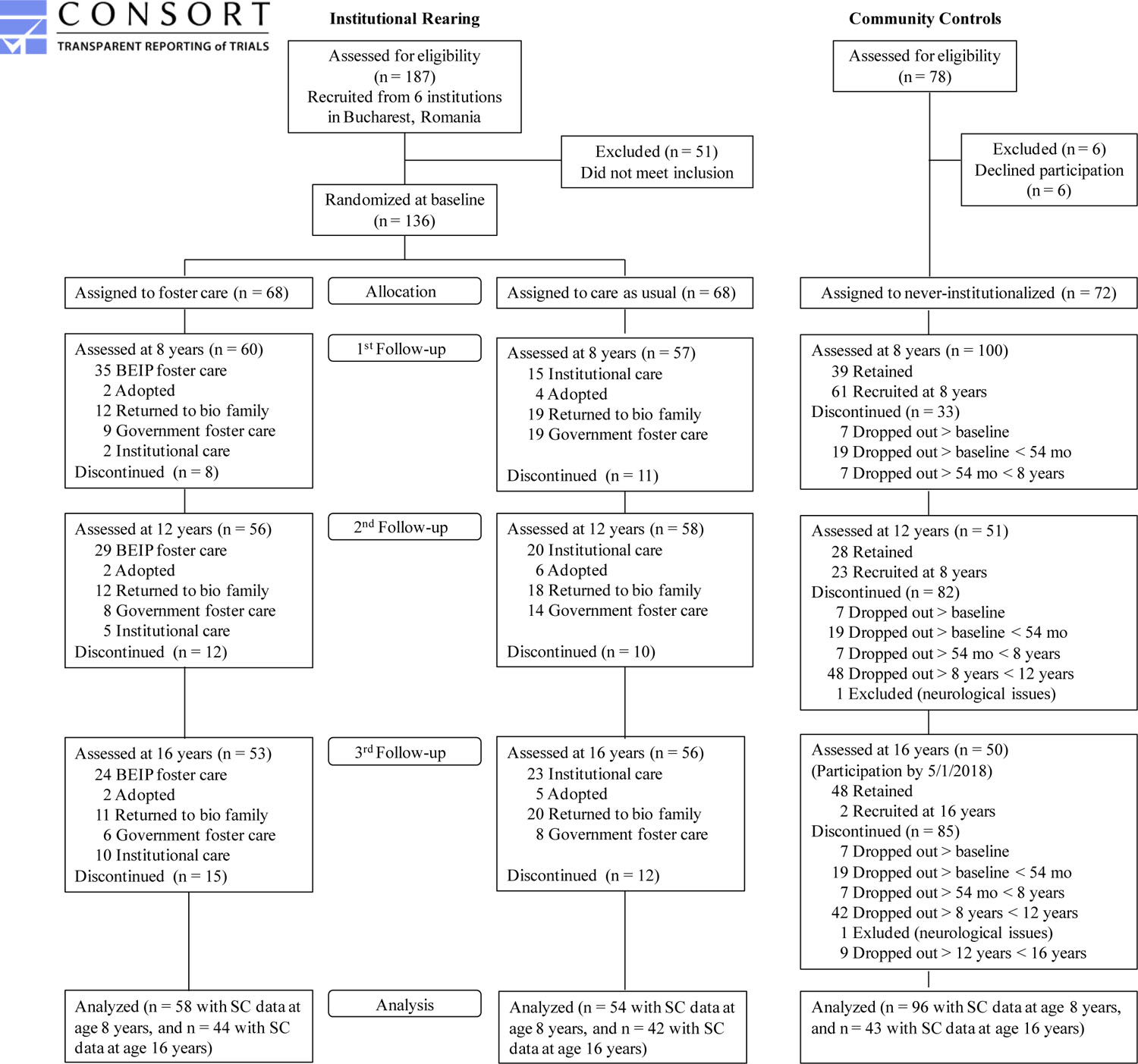
CONSORT Flow Diagram showing group assignment and follow-up measurement in the randomized control trial.
The current study examined children who provided data on SC and psychopathology at the 8 and 16 year follow-ups. A total of 208 children (112 EIG; 96 NIG) contributed data on SC at age 8 years, and 129 (86 EIG; 43 NIG) contributed data at 16 years. A total of 195 children (96 EIG; 99 NIG) contributed psychopathology data at 8 years, and 149 at 16 years (101 EIG; 48 NIG). Thus, for the cross-sectional analysis of SC difficulties at age 16, 129 children were analyzed. For the longitudinal analysis from age 8 to 16, all 208 children were included and full-information maximum-likelihood estimation (FIML) was used to handle missing data over time, described below. Table 1 presents demographic information for the three study groups.
Table 1:
Demographic characteristics across groups at age 8
| Child Characteristics | CAUG (n = 54) |
FCG (n = 58) |
NIG (n = 96) |
|---|---|---|---|
| Gender (%) | |||
| Male | 50.0 | 48.3 | 50.0 |
| Female | 50.0 | 51.7 | 50.0 |
| Ethnicity (%) | |||
| Romanian | 46.3 | 58.6 | 90.6 |
| Roma (gypsy) | 37.0 | 27.6 | 8.3 |
| Unknown | 16.7 | 12.1 | 0.0 |
| Other | 0.0 | 1.7 | 1.0 |
| Age entered institution (months) | 2.65 | 2.87 | - |
CAUG - care as usual group; FCG - foster care group;
NIG - never-institutionalized group (control)
Measures
Social communication (SC).
At age 8 and 16 years, the 40 item caregiver-report Social Communication Questionnaire (SCQ) (Rutter, Bailey, & Lord, 2003) was used to assess total problems and specific difficulties in the subdomains of reciprocal social interaction, communication, and repetitive and stereotyped behaviors. The SCQ has good psychometric properties, including sensitivity and specificity for autism diagnoses (Chandler et al., 2007). We used the lifetime version of the questionnaire, which includes items reflecting whether certain difficulties were ever present up to the age of assessment (items 2–19), as well as a specific set of items reflecting functioning at age 4–5 (items 20–40). We refer to the former as “current” as they are measured during the current assessment point (age 8 or 16) and do not include items specific to the preschool period, even though such concerns may have been present at any point up that age; and we refer to the entire scale as “lifetime” functioning since these capture both preschool functioning and lifetime items. All items were scored as a dichotomous “yes”/”no” response, with a value of 1 assigned if the atypical behavior was present and 0 if it was absent. Although the SCQ is often used as a screener for autism, only five out of 136 children in BEIP met criteria for autism (Levin et al., 2015). Thus, the current study used dimensional SCQ scores for all analyses. Moreover, since the caregivers of many institutionally-reared children did not have access to information on their children’s functioning at age 4–5 years (i.e., the children were not yet in their care), we computed average scores across the items that were completed. This proration of scores was done because sum scores would be misleading if, for example, the 4–5 year items were missing for children who would have otherwise scored high on those items. In other words, a total score would underestimate the extent of SC difficulties for some institutionally-reared children whose caregivers were unable to report on childhood difficulties. Supporting this approach, current and preschool (age 4–5) SCQ total scores were significantly correlated for those with complete data (r = .64, p < .001). Moreover, current and lifetime SCQ total scores at age 16 were significantly correlated (r = .85, p < .001). There was no evidence that inclusion of age 4–5 items at both age 8 and age 16 years inflated the cross-time SCQ correlation, as the correlation between lifetime SCQ at age 8 and 16 (r = .71, p < .001) was comparable to the correlation for current SCQ at age 8 and 16 (r = .75, p < .001). Thus, we used lifetime SCQ (both preschool and lifetime items) in the primary analysis, consistent with Levin et al. (2015).
Psychopathology (P, INT, and EXT).
At age 8 and 16 years, various domains of psychopathology were assessed using the MacArthur Health and Behavior Questionnaire (HBQ) (Essex et al., 2002). Teachers and/or caregivers responded to several items on 3-point Likert scales (0 = “never or not true”; 1 = “sometimes true”; and 2 = “often or very true”). Subscales included: depression, overanxious, social anxiety, oppositional defiant, conduct problems, overt aggression, relational aggression, and ADHD. At age 8, 195 teachers reported on children’s difficulties. Parent ratings were not collected at this age. At age 16, 146 caregivers and 82 teachers reported on children’s difficulties, for a total sample of 149 children with psychopathology data. Caregiver and teacher ratings were significantly correlated for all domains of psychopathology (r = .24 to .56, all p’s < .05). The lowest correlation was for the overanxious scale; but in general correlations for internalizing and externalizing domains were all significant (Table S2). Ratings for teachers and caregivers were averaged into composite scores to reduce rater bias. These ratings were then subjected to latent bifactor models, consistent with recent work on the latent structure of psychopathology (Caspi et al., 2014). Previously-derived P, INT, and EXT factor scores (Wade, Fox, Zeanah, & Nelson, 2018) were saved and used in the longitudinal path model described below. Additional details are provided in the Supplementary Materials.
Statistical Analyses
Following the aims listed above, the analyses were conducted in several steps. First, we used linear regression to examine whether institutional care (NIG = 0, EIG = 1) predicted SCQ total score and specific subdomain scores for reciprocal social interaction, communication, and repetitive and stereotyped behaviors at age 16. Second, we used the same approach in an intent-to-treat analysis (based on participants’ original placement) to determine whether FCG had fewer SC problems (total and subdomains) compared to CAUG at age 16 (CAUG = 0, FCG = 1). Third, we implemented a cross-lagged longitudinal path model to test reciprocal relations between SC and P, INT, and EXT factors from age 8 to 16, including whether each mediated the effects of institutional rearing on the other over time. In this model, all effects were tested simultaneously and conditional on all other effects in the model, providing unique estimates. We repeated this analysis to determine whether similar patterns emerged for the intervention effect (i.e., whether SC accounted for reductions in psychopathology as a function of foster care). All analyses were conducted in SPSS v21 and Mplus v7. In the path analyses, FIML was used to handle missing data. FIML outperforms other methods such as listwise and deletion and mean substitution in terms of parameter bias, model fit, and model convergence (Enders & Bandalos, 2001). Analyses were performed using a maximum likelihood (ML) estimator. The significance of the indirect effects were evaluated across 5000 bootstrap samples (Preacher & Hayes, 2008).
Results
Aim 1: Effect of Institutional Rearing on Adolescent Social Communication
The effect of institutional rearing (difference between EIG and NIG) on SCQ total and subdomain scores at age 16 are presented in Table 2. There was a significant effect of institutional rearing on the SCQ total score, such that EIG had more difficulties than NIG. On the SCQ subdomains, EIG had more difficulties than NIG on reciprocal social interaction and repetitive and stereotyped behaviors, but not communication. However, Supplementary Analysis revealed that EIG did have more communication difficulties than NIG when the analysis was restricted to current as opposed to lifetime difficulties (Table S3).
Table 2:
Group differences in social communication (total and subdomains) at age 16 years
| Institutionalization effect | Intervention effect | |||||
|---|---|---|---|---|---|---|
| Outcome | NIG (n = 43) M (SE) |
EIG (n = 86) M (SE) |
z | FCG (n = 44) M (SE) |
CAUG (n = 42) M (SE) |
z |
| SCQ total score | .09 (.01) | .15 (.02) | 3.58*** | .12 (.02) | .18 (.03) | 1.46 |
| Reciprocal social interaction | .05 (.01) | .12 (.03) | 3.43** | .07 (.03) | .17 (.04) | 2.12* |
| Communication | .11 (.02) | .14 (.02) | 1.51 | .11 (.02) | .18 (.04) | 1.32 |
| Repetitive and stereotyped behaviors | .05 (.02) | .11 (.02) | 2.31* | .10 (.03) | .11 (.04) | .28 |
p < 0.001.
p < 0.01.
p < 0.05.
z – standardized estimate/SE(standardized estimate)
NIG – never-institutionalized group; EIG – ever-institutionalized group; FCG – foster care group; CAUG – care-as-usual group
Aim 2: Effect of Foster Care Intervention on Adolescent Social Communication
In terms of the intervention effect of foster care placement, FCG did not differ from CAUG on the SCQ total score, nor did they differ on the subdomains of communication or repetitive and stereotyped behaviors (Table 2) However, there was a specific intervention effect on reciprocal social interaction, with FCG having significantly fewer problems compared to CAUG at age 16. Moreover, FCG did not differ from NIG on reciprocal social interaction, suggesting complete attenuation of problems in this subdomain as a function of the intervention. In contrast, when the analysis was restricted to current as opposed to lifetime functioning, no intervention effect on reciprocal social interaction (or any other subdomain) was observed at age 16 (Table S3).
Aim 3: Relations between Social Communication and Psychopathology
Table S4 presents bivariate correlations between SCQ total score (current, lifetime, and preschool) and psychopathology factors at ages 8 and 16. At age 8, P was positively associated with lifetime SCQ total score, whereas INT and EXT were unrelated to SCQ. At age 16, P was again positively associated with lifetime SCQ total score, and INT and EXT were unrelated to SCQ. Across time, lifetime SCQ total score at age 8 was positively associated with P and EXT at age 16. None of the psychopathology factors at age 8 were associated with lifetime SCQ total score at age 16. A similar pattern was observed for current SCQ total scores. Moreover, SCQ total score for preschool (age 4–5) items was positively related to P at age 16 only. Finally, Table S5 shows that all SCQ subdomain scores at age 8 were correlated with P at age 16. Restricting the analysis to current difficulties revealed a similar, but weaker, pattern of association.
Institutional Rearing Model Linking SC and Psychopathology over Time
We then examined reciprocal relations between SC and psychopathology from age 8 to 16, and whether each mediated the effects of institutional rearing on the other. This path model is presented in Figure 2A. The model was just-identified with zero degrees of freedom, and thus model fit cannot be assessed, but the parameters are still interpretable (Brown, 2014). As seen in Figure 2A, there was stability in P, EXT, and SCQ total score, but not INT, from age 8 to 16. Moreover, institutional rearing (NIG = 0, EIG = 1) was associated a higher SCQ total score at age 8, which was in turn associated with higher P, but not INT or EXT, at age 16. Institutional rearing was also associated with higher P at age 8. None of P, INT, or EXT at age 8 were associated with SCQ total score at age 16. Supplementary Table S6 presents the within-time residual covariances between the variables in this model at ages 8 and 16.
Figure 2.
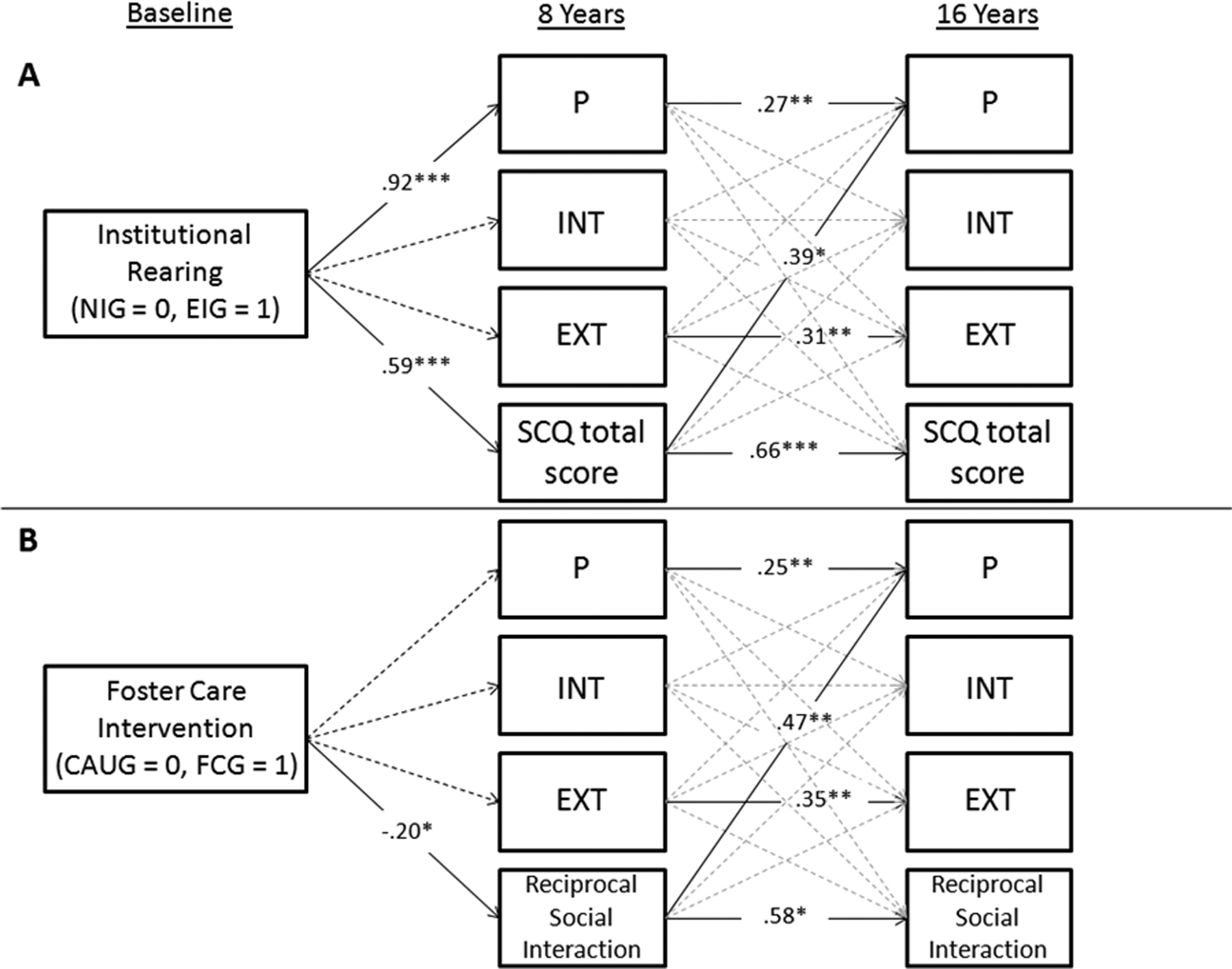
Longitudinal cross-lagged path model showing the association between SC difficulties and P, INT, and EXT factor scores in the (A) Institutional Rearing model; and (B) Intervention model. Coefficients are standardized β coefficients. Solid lines are significant paths, and hashed lines are non-significant paths. Note that in the Institutional Rearing Model, SC is the SCQ total score. In the Intervention Model, SC is the reciprocal social interaction subdomain score, as this was the only subdomain showing an intervention effect. ***p < .001. **p < .01. *p < .05.
Table 3 presents total, direct, and indirect effects of institutional rearing on P, INT, EXT, and SCQ total score at age 16 through these same factors at age 8 from the bootstrapped ML model. The total effect of institutional rearing on P at age 16 was significant. The analysis of specific indirect effects revealed two significant pathways to P: (i) institutional rearing was indirectly associated with higher P at age 16 through higher P at age 8, z = 3.22, p = .001; and (ii) institutional rearing was indirectly associated with higher P at age 16 through higher SCQ total score at age 8, z = 2.04, p = .041. The direct effect of institutional rearing on P at age 16 was still significant after accounting for these indirect paths, suggesting partial mediation. In contrast to P, there were no total, indirect, or direct effects on INT at age 16. There was a marginal total effect of institutional rearing on EXT at age 16. However, the analysis of specific indirect effects did not reveal any specific pathways to EXT through age 8 variables. Finally, for SCQ total score at age 16, there was a significant total effect of institutional rearing. The analysis of specific indirect effects revealed a single pathways through SCQ total score at age 8, z = 3.03, p = .002. The direct effect of institutional rearing on SCQ total score at age 16 was no longer significant after accounting for the indirect effect.1
Table 3:
Total, direct, and indirect effects of institutional rearing on P, INT, EXT, and SC at age 16
| P | INT | EXT | SCQ total score | |||||
|---|---|---|---|---|---|---|---|---|
|
B (SE) |
β [95% CI] |
B (SE) |
β [95% CI] |
B (SE) |
β [95% CI] |
B (SE) |
β [95% CI] |
|
| Total effect | .95*** (.15) |
.89 [.61, 1.17] |
.23 (.14) |
.28 [−.06, .62] |
.28† (.15) |
.29 [−.02, .59] |
.05* (.02) |
.33 [.02, .64] |
| Direct effect | .44** (.15) |
.41 [.13, .69] |
.25 (.18) |
.30 [−.12, .72] |
−.01 (.19) |
−.01 [−.38, .37] |
−.02 (.02) |
−.16 [−.47, .16] |
| z | STD ES 95% CI |
z | STD ES 95% CI |
Z | STD ES 95% CI |
z | STD ES 95% CI |
|
| Total indirect effect | 3.64*** | .48 [.22, .74] |
−.16 | −.02 [−.26, .22] |
2.06* | .29 [.01, .57] |
3.12** | .49 [.18, .80] |
p < .001.
p < .01.
p < .05.
p < .10.
B – unstandardized estimate
SE – boostrapped standard error around unstandardized estimate
β – standardized beta estimate
95% CI – bootstrapped confidence interval around standardized estimate
z – unstandardized estimate/SE(unstandardized estimate)
STD ES – standardized effect size (a*b) for the indirect effect
Given that EIG and NIG differed on the SCQ subdomains of reciprocal social interaction and repetitive and stereotyped behavior at age 16, we re-analyzed the above model, replacing SCQ total score with these subdomain scores. This was not done for communication since there were no group differences on this subdomain for lifetime difficulties. Briefly, the same pattern was observed for reciprocal social interaction, but not repetitive and stereotyped behaviors. Thus, it appears that reciprocal social interaction was the primary dimension of SC driving the mediation effects reported above. Results from this model are presented in Supplementary Table S7.
Intervention Model Linking SC and Psychopathology over Time
Given that FCG showed better reciprocal social interaction than CAUG at age 16 (current study) and previously at age 8 (Levin et al., 2015), and given that we previously demonstrated intervention effects on psychopathology at age 16 (Wade et al., 2018), we examined whether improvements in reciprocal social interaction at age 8 mediated intervention effects on psychopathology at age 16. This model is presented in Figure 2B. As seen in this figure, the intervention (CAUG = 0, FCG = 1) was associated with fewer difficulties with reciprocal social interaction at age 8, which was in turn associated with lower P at age 16. No effects of P, INT, or EXT at age 8 on reciprocal social interaction at age 16 were observed. There was a significant total effect of the intervention on P at age 16, β (SE) = −.47 (.21), p = .029, and a modest total indirect effect, z = −.17, p = .09. However, there were no significant indirect effects through reciprocal social interaction at age 8. Thus, improvements in reciprocal social interaction did not mediate foster care benefits on psychopathology. Supplementary Table S6 presents the within-time residual covariances between the variables in this model at ages 8 and 16.
Supplementary Analysis
In the Supplementary Materials, we present several supporting analyses. First, we present a sensitivity analysis in which is it shown that the effect of duration of institutionalization on P at age 16 is partially mediated by reciprocal social interaction difficulties at age 8. Thus, it appears that the extent of deprivation is meaningfully related to both SC and psychopathology. Second, as noted above, we examine how current SC difficulties, as opposed to lifetime SC difficulties, differ between intervention groups at age 16. In brief, we continue to see that EIG have more SC total difficulties than NIG, but we do not observe differences between EIG and NIG, nor between FCG and CAUG, on reciprocal social interaction as we did in the primary analysis. This may reflect the finding that CAUG children appear to “catch up” to the FCG and NIG over time, with declines in their reciprocal social interaction difficulties from the preschool period to age 16 (Figure S2). Third, given that many children experienced placement changes over the course of the study, we examined whether one’s current living environment was related to SC (Figure S1). This analysis shows that CAUG youth who still resided in a non-family placement by age 16 (including institutional care) had more SCQ total difficulties than CAUG youth who now resided in family care. The former group had more difficulties than all other children on the subdomains of reciprocal social interaction and communication. Interestingly, the small subset of FCG youth who resided in a non-family placement (including back in institutions) at age 16 did not differ from FCG youth who still resided in family-based care or NIG youth on any SCQ domain.
Discussion
In the current study we sought to examine the long-term effects of institutional deprivation on SC in adolescence, the role of foster care intervention in reducing risk for SC difficulties, and the relation between SC difficulties and broad-spectrum psychopathology. There are several notable findings. First, consistent with previous studies of post-institutionalized children (Levin et al., 2015; Sonuga-Barke et al., 2017), those raised in institutions had more SC difficulties in adolescence than children who had never experienced institutional deprivation, and these effects were most prominent for the subdomains of reciprocal social interaction and repetitive and stereotyped behaviors. Second, early placement into high-quality foster care was associated with fewer lifetime SC difficulties measured at age 16, most notably reciprocal social interaction, consistent with previous findings at age 8–10 years (Levin et al., 2015). Third, deficits in SC were associated with higher levels of general psychopathology (P) at age 8 and 16 years, and longitudinal analysis showed that SC difficulties at age 8 were associated with higher P at age 16. Indeed, SC deficits at age 8 partially mediated the effects of institutional rearing on P at age 16, but no such effects were observed for INT or EXT. Fourth, despite clear intervention effects on reciprocal social interaction, improvements in this subdomain did not mediate treatment benefits on psychopathology in adolescence, although better SC at age 8 did predict lower P at age 16 among institutionally-reared youth.
Supplementary Analysis revealed several additional findings. First, the duration of institutional rearing was shown to predict P at age 16, and this effect was partially mediated by deficits in reciprocal social interaction at age 8. Thus, despite limited evidence that improved reciprocal social interaction mediated intervention effects on psychopathology, a shorter duration of deprivation was associated with lower levels of psychopathology in adolescence through better reciprocal social interaction in middle childhood. Second, when examining current SC (lifetime items excluding those at age 4–5 years), we continued to observe an effect of institutional rearing on total SC difficulties, but there was no effect of institutional rearing or foster care intervention on reciprocal social interaction. This lack of group difference may suggest that items indexing functioning at age 4–5 are important in picking up on children’s SC difficulties, which for many children may be pervasive and longstanding. Similarly, associations between current SC and psychopathology were somewhat weaker than lifetime SC and psychopathology (Table S4 and S5), suggesting that behaviors indexing SC both currently and early in development (preschool period) are more sensitive in capturing risk of psychopathology than current functioning alone. The lack of group differences in current reciprocal social interaction may also reflect a catch-up effect among the CAUG over time (Figure S2). However, this analysis had several limitations and the results should be interpreted cautiously (see Supplementary Analysis). Finally, when examining the effects of current placement, we observed that CAUG youth who still resided in non-family/institutional care at age 16 had more SC difficulties than CAUG youth who were now residing in family care. Also, a small subset of FCG who were now residing in non-family/institutional care at age 16 did not differ from FCG youth who continued to reside in family care or NIG youth. Thus, chronic exposure to institutional deprivation appears to be particularly noxious for SC development. In contrast, early placement into family care may protect against SC difficulties in adolescence, even if children are re-exposed to later deprivation. While this finding is consistent with the idea of a sensitive period in early childhood, the results must be interpreted cautiously given the small sample sizes of each group. Moreover, the FCG were a heterogeneous group who experienced varying lengths of time in institutional care. This analysis only focused on current placement and therefore may not capture the duration of deprivation or number of placement changes experienced by the FCG.
The current study adds to a growing literature suggesting that there are negative long-term consequences of severe early psychosocial deprivation on SC development. Optimistically, social enrichment afforded by foster care appears to at least partially attenuate these effects, with full remediation in the subdomain of reciprocal social interaction. This specific domain may especially benefit from the enhanced contingent responsiveness that accompanies entry into foster care. It has been suggested that early deprivation constrains basic forms of associative learning that depend on social inputs from caregivers (McLaughlin, Sheridan, & Nelson, 2017). Caregivers play an instrumental role in facilitating associative learning by directing infants’ attention to relevant and rewarding stimuli with the use of vocalizations, gestures, and facial displays. Through repeated and reliable interactions with caregivers, the infant comes to associate their signals (e.g. crying) with predictable responses from the environment (e.g. caregiver soothing), and this contingent responsiveness refines children’s capacity for understanding cause-and-effect during social interactions. The absence of experience-expectant input in deprived environments may constrain the development of these processes. Experimental evidence for this comes from recent work which shows deficits in two forms of associative learning among children with prolonged institutional deprivation: reward responsivity and implicit learning (Sheridan et al., 2018). Encouragingly, these processes are normalized among children placed into foster care early in life. Thus, it is plausible that difficulties with reciprocal social interaction among institutionally-reared children reflect deficits in basic associative learning processes due to early deprivation, but that these difficulties are rescued when children are re-exposed to environments rich in contingent responsiveness.
The current study also showed that deficits in SC are both concurrently and longitudinally associated with higher levels of general psychopathology (P), but not strongly linked to either INT- or EXT-specific problems. This is the first study to show that deficits in SC may increase transdiagnostic vulnerability to mental health difficulties following severe early neglect. These results also suggest that specific problems with reciprocal social interaction may be related to transdiagnostic processes such as emotion dysregulation and negative emotionality (Caspi & Moffitt, 2018). For instance, difficulties with reciprocal social interaction may constrain opportunities for social scaffolding of key self-regulatory abilities that are required to effectively manage and control emotions, especially under conditions of stress. In other words, poor psychosocial stimulation in deprived environments may give rise to SC deficits which limit interpersonal experiences that promote the development of emotion regulation skills, or which buffer against social stress; in turn, this may trigger or amplify psychopathology risk.
These findings complement previous studies showing associations between SC and specific disorders such as depression and anxiety in non-deprived children (Halls, Cooper, & Creswell, 2015; Pickard et al., 2017; Sullivan et al., 2017). It is believed that SC deficits may hinder children’s ability to navigate complex social interactions over the course of childhood, which increases the risk for peer victimization or bullying that exacerbates psychopathology (Adams, Fredstrom, Duncan, Holleb, & Bishop, 2014; Pickard, Happé, & Mandy, 2018). However, unlike non-institutionalized youth who tend to become withdrawn or socially avoidant following victimization, post-institutionalized youth demonstrate significantly more disinhibited behavior (Pitula et al., 2014). This is consistent with recent work from our group that shows higher levels of disinhibited social engagement disorder among institutionally-reared children which is, in turn, related to lower social competence (Guyon-Harris, Humphreys, Fox, Nelson, & Zeanah, 2018, 2019). While not a primary goal of the current study, supplementary analysis showed that more SC difficulties at age 8 (and to a lesser extent at age 16) are related to multiple behavioral problems at age 16, including signs of disinhibited social engagement disorder, reactive attachment disorder, and ADHD, even after controlling for general psychopathology risk (Table S8). This constellation of difficulties is part of a deprivation-specific syndrome described by Rutter, Sonuga-Barke and colleagues (Kumsta et al., 2010; Sonuga-Barke et al., 2017). As such, the SC difficulties among institutionally-reared children may not only place them at risk for later common psychopathology risk, but may relate to other problems that are etiologically linked to social deprivation and neglect. Most encouraging, however, is the finding that family care following severe early deprivation at least partially safeguards against later SC deficits, which may in turn prevent the onset or exacerbation of psychopathology over the transition to adolescence. Uncovering the neural and physiological mechanisms by which this social buffering occurs is a critical next step in this field.
Strengths and Limitations
Strengths of the current study include the objective measurement of neglect as a function of institutional rearing and the RCT design, which allows for causal inferences around the benefits of social enrichment on SC following deprivation. Moreover, use of a multi-wave longitudinal analysis permitted an assessment of the directional link between SC and psychopathology from childhood to adolescence. Several limitations are also noteworthy. First, the sample was relatively small, which may have limited power to detect certain effects, especially the mediational effect of SC in the intervention model, which closely resembled the more highly-powered institutional rearing model but did not yield significant indirect effects. Second, the limited number of children diagnosed with autism (n = 5; 4.3% of institutionalized children) prevented an analysis of SC relations with psychopathology in children with clinical levels of symptoms. Third, all analysis relied on parent and/or teacher reports of SC and psychopathology, and future research would benefit from an approach that uses objective assessments. Fourth, it is notable that the pattern of results was not identical when we used current compared to Lifetime SC measures. These results suggest that care must be taken when interpreting these results since the choice of SC indicator may lead to differences in the conclusions that are drawn. Fifth, while not a limitation per se, the fact there continued to be direct effects of institutional rearing on psychopathology after accounting for SC suggests that other unmeasured factors may be involved in this mechanism, and future research should test competing pathways through other domains of cognitive, emotional, and social functioning. Finally, this was a unique sample of severely deprived children, so generalizability to less severe forms of neglect cannot be assumed.
Supplementary Material
Key Points:
Institutional deprivation during early childhood is associated with later social communication deficits
Family-based foster care following institutional deprivation remediates some social communication difficulties, especially reciprocal social interaction
Deficits in social communication partially mediate the link between institutional deprivation and broad-spectrum psychopathology in adolescence
Targeting social communication problems with early intervention may have cross-cutting benefits on reducing the risk or severity of later psychopathology
Acknowledgements
We thank the families and the children that participated in this study, as well as the research team and staff in Romania for their support and investment in this project.
Funding
This study was supported by the John D. and Catherine T. MacArthur Foundation, the Binder Family Foundation, and NIMH (R01MH091363) to Charles A. Nelson. The funding sources had no role in the design of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; or decision to submit the manuscript for publication.
Declaration of Interests
Dr. Nelson has received grant support from NIH, the Jacobs Foundation, the John D. and Catherine T. MacArthur Foundation, the James S. McDonnel Foundation, the Binder Family Foundation, the Lumos Foundation, the Bill and Melinda Gates Foundation, and Harvard University. He has received royalties from MIT and Harvard University Press. He has received honoraria for lectures to professional audiences, and legal consulting fees. Dr. Zeanah has received grant support from NIMH, the Palix Foundation, the Irving Harris Foundation, the Substance Abuse and Mental Health Services Administration, and the Lumos Foundation. He has received royalties from Guilford Press and Harvard University Press. He has received honoraria for lectures to professional audiences. Dr. Fox receives grant support from NIMH, NICHD, NSF, the NIH ECHO consortium, the Russell Sage Foundation, and the Lumos Foundation. He has received royalties from Guilford Press and Harvard University Press. He has received honoraria for lectures to professional audiences. Dr. Wade has no disclosures to report.
Abbreviations:
- P
general psychopathology
- INT
internalizing problems
- EXT
externalizing problems
- SC
social communication
Footnotes
We re-examined the path model linking institutional rearing to psychopathology via SC among only those participants with complete data at age 8 and 16 (n = 109). Despite this smaller sample, the pattern of results was similar to the original analysis. Specifically, we observed a significant indirect effect of institutional rearing on P at age 16 through SCQ total score at age 8, unstandardized estimate (SE) = .16 (.07), z = 2.29 p = .022. The indirect effect of institutional rearing on P at age 16 via P at age 8 was still significant, unstandardized estimate (SE) = .25 (.10), z = 2.59 p = .009. Unlike in the primary analysis, we also observed a significant indirect effect of institutional rearing on EXT at age 16 via SCQ total score at age 8, unstandardized estimate (SE) = .13 (.06), z = 2.26 p = .024. This effect was due to a significant relation between SCQ total score (age 8) and EXT (age 16) that was not observed in the original analysis but which is consistent with the bivariate correlations in Table S4.
References
- Adams RE, Fredstrom BK, Duncan AW, Holleb LJ, & Bishop SL (2014). Using self-and parent-reports to test the association between peer victimization and internalizing symptoms in verbally fluent adolescents with ASD. Journal of Autism and Developmental Disorders, 44(4), 861–872. [DOI] [PubMed] [Google Scholar]
- Brown TA (2014). Confirmatory factor analysis for applied research: Guilford Publications. [Google Scholar]
- Caspi A, Houts RM, Belsky DW, Goldman-Mellor SJ, Harrington H, Israel S, … Poulton R (2014). The p factor: one general psychopathology factor in the structure of psychiatric disorders? Clinical Psychological Science, 2(2), 119–137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Caspi A, & Moffitt TE (2018). All for one and one for all: Mental disorders in one dimension. American Journal of Psychiatry, appi. ajp. 2018.17121383. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chandler S, Charman T, Baird G, Simonoff E, Loucas T, Meldrum D, … Pickles A, (2007). Validation of the social communication questionnaire in a population cohort of children with autism spectrum disorders. Journal of the American Academy of Child & Adolescent Psychiatry, 46(10), 1324–1332. [DOI] [PubMed] [Google Scholar]
- Enders CK, & Bandalos DL (2001). The relative performance of full information maximum likelihood estimation for missing data in structural equation models. Structural equation modeling, 8(3), 430–457. [PubMed] [Google Scholar]
- Essex MJ, Boyce WT, Goldstein LH, Armstrong JM, Kraemer HC, Kupfer DJ, & Group MABW (2002). The confluence of mental, physical, social, and academic difficulties in middle childhood. II: Developing the MacArthur Health and Behavior Questionnaire. Journal of the American Academy of Child & Adolescent Psychiatry, 41(5), 588–603. [DOI] [PubMed] [Google Scholar]
- Gunnar MR, & Reid BM (2019). Early Deprivation Revisited: Contemporary Studies of the Impact on Young Children of Institutional Care. Annual Review of Developmental Psychology, 1. [Google Scholar]
- Guyon-Harris KL, Humphreys KL, Fox NA, Nelson CA, & Zeanah CH (2018). Course of disinhibited social engagement disorder from early childhood to early adolescence. Journal of the American Academy of Child & Adolescent Psychiatry, 57(5), 329–335. e322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guyon-Harris KL, Humphreys KL, Fox NA, Nelson CA, & Zeanah CH (2019). Signs of attachment disorders and social functioning among early adolescents with a history of institutional care. Child abuse & neglect, 88, 96–106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Halls G, Cooper PJ, & Creswell C (2015). Social communication deficits: specific associations with social anxiety disorder. Journal of affective disorders, 172, 38–42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hillis S, Mercy J, Amobi A, & Kress H (2016). Global prevalence of past-year violence against children: a systematic review and minimum estimates. Pediatrics, 137(3), e20154079. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hoksbergen R, Ter Laak J, Rijk K, van Dijkum C, & Stoutjesdijk F (2005). Post-institutional autistic syndrome in Romanian adoptees. Journal of Autism and Developmental Disorders, 35(5), 615–623. [DOI] [PubMed] [Google Scholar]
- Kumsta R, Kreppner J, Rutter M, Beckett C, Castle J, Stevens S, & Sonuga-Barke EJ (2010). III. Deprivation-specific psychological patterns. Monographs of the Society for Research in Child Development, 75(1), 48–78. [DOI] [PubMed] [Google Scholar]
- Levin AR, Fox NA, Zeanah CH Jr, & Nelson CA (2015). Social communication difficulties and autism in previously institutionalized children. Journal of the American Academy of Child & Adolescent Psychiatry, 54(2), 108–115. e101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McLaughlin KA, Sheridan MA, & Nelson CA (2017). Neglect as a violation of species-expectant experience: neurodevelopmental consequences. Biological psychiatry, 82(7), 462–471. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muhamedrahimov RJ, Agarkova VV, Vershnina EA, Palmov OI, Nikiforova NV, McCall RB, & Groark CJ (2014). Behavior problems in children transferred from a socioemotionally depriving institution to St. Petersburg (Russian Federation) families. Infant mental health journal, 35(2), 111–122. [DOI] [PubMed] [Google Scholar]
- Pickard H, Happé F, & Mandy W (2018). Navigating the social world: The role of social competence, peer victimisation and friendship quality in the development of social anxiety in childhood. Journal of anxiety disorders, 60, 1–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pickard H, Rijsdijk F, Happé F, & Mandy W (2017). Are social and communication difficulties a risk factor for the development of social anxiety? Journal of the American Academy of Child & Adolescent Psychiatry, 56(4), 344–351. e343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pitula CE, Thomas KM, Armstrong JM, Essex MJ, Crick NR, & Gunnar MR (2014). Peer victimization and internalizing symptoms among post-institutionalized, internationally adopted youth. Journal of abnormal child psychology, 42(7), 1069–1076. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Preacher KJ, & Hayes AF (2008). Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behavior research methods, 40(3), 879–891. [DOI] [PubMed] [Google Scholar]
- Rutter M, Andersen-Wood L, Beckett C, Bredenkamp D, Castle J, Groothues C, … O’Connor TG (1999). Quasi-autistic patterns following severe early global privation. The Journal of Child Psychology and Psychiatry and Allied Disciplines, 40(4), 537–549. [PubMed] [Google Scholar]
- Rutter M, Bailey A, & Lord C (2003). The social communication questionnaire: Manual: Western Psychological Services. [Google Scholar]
- Rutter M, Kreppner J, Croft C, Murin M, Colvert E, Beckett C, … Sonuga-Barke E (2007). Early adolescent outcomes of institutionally deprived and non-deprived adoptees. III. Quasi-autism. Journal of Child Psychology and Psychiatry, 48(12), 1200–1207. [DOI] [PubMed] [Google Scholar]
- Sheridan MA, McLaughlin KA, Winter W, Fox N, Zeanah C, & Nelson CA (2018). Early deprivation disruption of associative learning is a developmental pathway to depression and social problems. Nature communications, 9(1), 2216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Simonoff E, Pickles A, Charman T, Chandler S, Loucas T, & Baird G (2008). Psychiatric disorders in children with autism spectrum disorders: prevalence, comorbidity, and associated factors in a population-derived sample. Journal of the American Academy of Child & Adolescent Psychiatry, 47(8), 921–929. [DOI] [PubMed] [Google Scholar]
- Sonuga-Barke EJ, Kennedy M, Kumsta R, Knights N, Golm D, Rutter M, … Kreppner J (2017). Child-to-adult neurodevelopmental and mental health trajectories after early life deprivation: the young adult follow-up of the longitudinal English and Romanian Adoptees study. The Lancet, 389(10078), 1539–1548. [DOI] [PubMed] [Google Scholar]
- Sullivan SA, Thompson A, Kounali D, Lewis G, & Zammit S (2017). The longitudinal association between external locus of control, social cognition and adolescent psychopathology. Social psychiatry and psychiatric epidemiology, 52(6), 643–655. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tan TX (2009). School-Age Adopted Chinese Girls’ Behavioral Adjustment, Academic Performance, and Social Skills: Longitudinal Results. American Journal of Orthopsychiatry, 79(2), 244–251. [DOI] [PubMed] [Google Scholar]
- U.S. Department of Health and Human Services, C. s. B. (2018). Child maltreatment 2016. Washington, DC: U.S. [Google Scholar]
- Vorria P, Ntouma M, & Rutter M (2015). Vulnerability and resilience after early institutional care: The Greek Metera study. Development and psychopathology, 27(3), 859–866. [DOI] [PubMed] [Google Scholar]
- Wade M, Fox NA, Zeanah CH, & Nelson CA (2018). Effect of foster care intervention on trajectories of general and specific psychopathology among children with histories of institutional rearing: A randomized clinical trial. JAMA Psychiatry, 75(11), 1137–1145. doi:doi: 10.1001/jamapsychiatry.2018.2556 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zeanah CH, Fox NA, & Nelson CA (2012). The Bucharest Early Intervention Project: case study in the ethics of mental health research. The Journal of nervous and mental disease, 200(3), 243–247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zeanah CH, Humphreys KL, Fox NA, & Nelson CA (2017). Alternatives for abandoned children: insights from the Bucharest Early Intervention Project. Current opinion in psychology, 15, 182–188. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.