

Abstract
We conducted a longitidinal assessment of 806 respondents in the US to examine the trustworthiness of sources of information about COVID-19. Respondents were recontacted after four months. Information sources included mainstream media, state health departments, the CDC, the White House, and a well-known university. We also examined how demographics, political partisanship, and skepticism about COVID-19 were associated with the perceived trustworthiness of information sources and decreased trustworthiness over time. At baseline, the majority of respondants reported high trust in COVID-19 information from state health departments (75.6%), the CDC (80.9%), and a university (Johns Hopkins, 81.1%). Mainstream media was trusted by less than half the respondents (41.2%), and the White House was the least trusted source (30.9%). At the 4-month follow-up, a significant decrease in trustworthiness in all five sources of COVID-19 information was observed. The most pronounced reductions were from the CDC and the White House. In multivariate analyses, factors associated with rating the CDC, state health department, and a university as trustworthy sources of COVID-19 information were political party affiliation, level of education, and skepticism about COVID-19. The most consistent predictor of decreased trust was political party affiliation, with Democrats as compared to Republicans less likely to report decreased trust across all sources.
Keywords: Covid-19, SARS-CoV-2, skepticism, prevention
Background
Inaccurate public health, scientific, and medical information can have major health consequences (Lazer et al., 2018; Scheufele & Krause, 2019; Wang, McKee, Torbica, & Stuckler, 2019). With the SARS-CoV-2 (COVID-19) pandemic, there has been a barrage of news articles and media reports providing public health information and guidance on COVID-19 prevention. Health-related misinformation about the COVID-19 pandemic and infection prevention has been well documented (Peters, Tartari, Lotfinejad, Parneix, & Pittet, 2018; Shimizu, 2020; Allington, Duffy, Wessely, Dhavan, & Rubin, 2020). Prior studies have recorded the vast amount of false information on social media (Kanekar & Thombre, 2019), and concerns have been raised about the trustworthiness of sources of COVID-19 information (Miller, 2020). This misinformation can influence engagement in COVID-19 health behaviors and propagate the spread of the virus. Media is a critical health-information dissemination channel; however, media mistrust can lead to inattention and nonconsumption (Lee, 2010). Perceptions of trustworthiness of information can be a significant moderator of public health systems’ effectiveness (Abraham, 2009; Cairns de Andrade, MacDonald, 2013; Gilson, 2003). For example, Singapore’s consolidated media approach during the severe acute respiratory syndrome (SARS) epidemic focused on transparency and public education and was associated with perceptions of high trustworthiness (Menon & Goh, 2005). Moreover, trust has been found to be a key component of vaccine acceptance and hence will be critical for the uptake of any COVID-19 vaccine (Larson, Leask, Aggett, Sevdalis, & Thomson, 2013; MacDonald, 2015).
It is critical that the public have a trustworthy source of COVID-19 information, as the pandemic has caused massive disruptions and threats to the health of entire populations. Trustworthiness is also critical to promote COVID-19 prevention behaviors and to ensure an adequate level of vaccine uptake. Many media outlets have devoted special sections of their reporting to the COVID-19 pandemic, and some paywalls have been eliminated. Yet a Pew 2020 Research Center poll reported that only about half (54%) of Americans thought that media coverage was excellent or good at responding to the coronavirus (Pew Research Center, 2020). Previous research has identified that political partisanship can influence trust in news media (Lee, 2010). These findings are supported by a Pew poll taken in the two months prior to the COVID-19 pandemic in the US, which indicated that there was a large difference in the level of trust in mainstream media based on political party affiliation, with Democrats tending to trust a greater number of news sources (Jurkowitz, Mitchell, Shearer, & Walker, 2020). In the US, as well as other counties, there has been a politically partisan divide on opinions and coverage of the COVID-19 pandemic. During the early stages of the pandemic, right-leaning media outlets were found to be more likely to discuss misinformation about COVID-19 than mainstream outlets (Motta, Stecula, & Farhart, 2020). In turn, misinformed people were more likely to believe that the CDC exaggerated COVID-19 health risks (Motta, Stecula, & Farhart, 2020). Recent research also suggests that Republicans are less likely to engage in COVID-prevention behaviors than other party affiliates (Gollwitzer et al., 2020).
In the literature on health information, there has been a range of conceptualizations of trust (Balog-Way & McComas, 2020; Larson, Clarke, Jarrett, Eckersberger, Levine, Schulz, & Paterson, 2018; Sbaffi & Rowley, 2017). We used Cairns, de Andrade, and MacDonald’s (2013) conceptualization of trust in health risk communication as, in part, a heuristic to evaluate information, which is especially important during a time of uncertainty and is often based on reputation and historical accounts of institutions and systems. In this study, we asked participants to rate the trustworthiness of five key sources of COVID-19 health information. We then assessed changes in the trustworthiness of COVID-19 sources of information over time. We hypothesized that organizations that were seen as having a science focus (CDC and Johns Hopkins University) and that were independent from political spheres (Johns Hopkins University and state health departments) would have greater levels of perceived COVID-19 trust than mainstream media sources and the White House. We anticipated that the trust in news sources also might be influenced by political affiliation, with lower levels of trust among political conservatives due to the political polarization of attitudes and perceptions of COVID-19 (de Bruin, Saw, & Goldman, 2020). Additionally, we anticipated that higher levels of trust in COVID-19 news sources would be positively associated with a greater frequency of consuming COVID-19 news on TV and in newspapers, since prior research has found that consumption of a greater number of reported COVID-19 news sources has been linked to higher levels of COVID-19 knowledge and education (Ali et al., 2020). Based on prior research on vaccine hesitancy, we also anticipated that trustworthiness of sources of coronavirus information would be negatively associated with skeptical attitudes toward the COVID-19 pandemic (Larson, Jarrett, Eckersberger, Smith, & Paterson, 2014). Existing research on how demographic factors influence trust is scant. We therefore examined demographic factors of gender, age, education, and income. Additionally, we assessed whether perceived trustworthiness of sources of coronavirus information was negatively associated with minority race/ethnicity, since historical racism and contemporary discrimination may lead to medical distrust (Cuffee et al., 2013; Jacobs, Rolle, Ferrans, Whitaker, & Warnecke, 2006; Shavers, Lynch, & Burmeister, 2000).
Methods
Study population
Study respondents completed the first survey between March 24th −27th, after many governors had declared States of Emergency and enacted social distancing measures. By March 24th, 15 states had implemented statewide Stay At Home orders, including California, Connecticut, Delaware, Illinois, Indiana, Louisiana, Massachusetts, Michigan, New Jersey, New Mexico, New York, Ohio, Oregon, Washington, and West Virginia. By March 26th,, 21 states had enacted statewide Stay At Home orders. The first wave of the study was completed before the pandemic had fulminated in New York and surrounding jurisdictions. Participants were interviewed for the third survey from July 22nd-30th. At that time, there had been over 140,000 COVID-19 deaths in the US. A second survey was also conducted but was excluded from this analysis, as it did not contain the survey items on the trustworthiness of COVID-19 news sources. All respondents who successfully completed the first survey were invited to participate in the second and third rounds of data collection. The study was approved by the Johns Hopkins Bloomberg School of Public Health IRB.
Study participants were recruited through Amazon’s Mechanical Turk (MTurk). MTurk is an online forum where participants can complete surveys and other small tasks. MTurk has been extensively studied for its adequacy for survey research. Study populations recruited through MTurk have not been found to be nationally representative, but the platform outperforms other online opinion sampling on several dimensions (Huff & Tingley, 2015). Previous research has supported the reliability of data from MTurk participants (Follmer, Sperline, & Suen, 2017). Study protocols were designed following MTurk’s best practices (Chandler & Shapiro, 2016; Strickland & Stoops, 2019; Young & Young, 2019). Participants were eligible for this study if they were adults living in the United States, were English speaking and reading, had heard of the coronavirus or COVID-19, and provided consent to participate in the study. Additionally, to enhance reliability, eligible participants had to pass attention and validity checks embedded in the survey (Rouse, 2015); these included repeated questions and questions with certain responses that had an exceedingly low probability of being accurate. The median completion time was 13.4 minutes. At the baseline survey, participants were also informed that this was a longitudinal study, and if interested, they would have the opportunity to participate in a future study. Participants were compensated $2.50 for completing the first survey and $3.50 for the third, equivalent to approximately $14 per hour.
Measures
Trust was assessed at data collection points in late March and July, 2020. When the survey was first launched, there were no published measures on informational trust related to COVID-19. The survey items were thoroughly piloted with a racially, gender, and age diverse sample. To assess trust in sources of information, a set of questions asked participants, “how much do you trust information from [….] about coronavirus?” The following were the five sources of information: (1) the CDC, (2) the White House, (3) Johns Hopkins University, (4) major news outlets such as CNN, (5) your State Health Department. Response options were “(1) A great deal,” “(2) Quite a bit,” “(3) Some,” “(4) Very little or none.” These sources were chosen based upon popularity, prestige, and information sources anticipated to provide accurate information. Johns Hopkins University was chosen due to its major role in disseminating COVID-19 data on cases and deaths. As the first two response categories indicated high trust ratings, responses to trust in information sources were dichotomized as high (a great deal or quite a bit) versus low (some, very little, or none).
Choices for race/ethnicity were White, Non-Hispanic Black, Hispanic, Asian, Mixed, and Other. Due to small sample sizes, mixed race and “other” categories were collapsed into one category. For political affiliation, Libertarian and “other” were subsequently classified as other. Gender, education, and income were also assessed. Level of education was collapsed to reflect some college or less, associate degree, or technical degree or less, and bachelor’s degree or higher. Income was dichotomized at the median of $60,000 or below.
Perceived health status was assessed with the question, “In general, would you say that your health is excellent, good, fair, or poor?” Any COVID-19 health risk condition was assessed by the question, “Do you have any respiratory conditions; that is a condition that affects your lungs, such as emphysema?” or reporting one of the following conditions: diabetes, cancer, heart disease, or high blood pressure. Political party affiliation was assessed with the standard question, “Do you consider yourself Republican, Democrat, Independent, Libertarian or other?” To assess quantity of COVID-19 news consumption, participants were asked, “How much time do you spend reading or watching news about coronavirus per day, on average?” Skepticism of the COVID-19 pandemic was assessed by the survey items, “The health risks from coronavirus has been exaggerated,” “The coronavirus is a hoax,” and “The coronavirus isn’t any worse than the flu.” The response categories were “Strongly Agree,” “Agree,” “Neither agree nor disagree,” “Disagree,” and “Strongly disagree.” These three items were summed as a scale and had a Cronbach’s alpha of .76, with lower scores indicating greater skepticism.
Analyses
Paired t-tests were used to compare changes in the trustworthiness of sources of COVID-19 information from baseline (survey one in March) to wave 3 (survey three in July). Potential correlates of trust and change in trust were assessed at baseline. Unadjusted logistic regression analyses were used to assess the associations between the independent variables and level of trust. For the multivariate analyses, we employed multivariate logistic regression models. All models adjusted for demographic characteristics. To compare models with different dependent variables, we included variables that were statistically significant in any of the bivariate models. A second multivariable logistic model was then used to examine changes in the trustworthiness of sources of COVID-19 information. Respondents whose level of trust increased or stayed the same were compared to individuals who decreased their level of trust in the source of COVID-19 information. The statistical softwares SPSS Statistics Version 25 (IBM Corp, Armonk, New York) and Stata 15 (College Station, Texas) were used.
Results
806 respondents completed the baseline survey, and 593 (74%) completed the wave 3 survey. An attrition analysis revealed that there were no statistically significant differences between respondents who stayed in the study compared to those who dropped out in terms of race, education, income, or gender. However, those who dropped out tended to be younger (mean 34.0, SD=10.8 vs. 39.7, SD=11.4, t=6.3, p<.01). The baseline sample was primarily White (78.2%), female (55.6%), and had a bachelor’s degree or higher (55.0%; Table 1). The mean age was 38.2, with a median age of 36, and 12.5% were 65 years of age or older. There were 58.4% who were employed full-time, 14% part-time, 10.3% unemployed, 2.9% retired, 1.7% were unable to work due to health reasons, 4.3% were students, and 8.3% reported other types of employment. Of the sample, 27.8% reported earning $35,000 (USD) or less a year, 27.9% earned $35,000-$60,000, 24.1% earned $60,00-$90,000 a year, and 20.2% earned $90,000 or more per year. For analysis, income was dichotomized at $60,000. Most respondents reported good or excellent health (79.7%). Most reported that they watch, listen, or read news about the coronavirus at least a couple of times per day, while 4.6% said that they consumed news about coronavirus less than once a day.
Table 1.
Reports of high ratings of trust in sources of information about coronavirus among respondents (N=806)
| Total | High Trust, the CDCa | High Trust, Johns Hopkins Universityb | High Trust, State Health Departmentc | High Trust, the White Housed | High Trust, Mainstream Mediae | |
|---|---|---|---|---|---|---|
| (N=806) | (n=652; 80.89%) | (n=654; 81.14%) | (n=609; 75.56%) | (n=249; 30.9%) | (n=394; 48.19%) | |
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | |
| Age (mean ± SD) | 38.17± 11.53 | 38.27 ± 11.64 | 38.77 ± 11.69 | 38.16 ± 11.80 | 38.47 ± 12.02 | 38.61 ± 11.68 |
| Race/ethnicity | ||||||
| White | 630 (78.16) | 517 (79.29) | 522 (79.82) | 482 (79.15) | 200 (80.32) | 303 (76.90) |
| Non-Hispanic Black | 59 (7.32) | 42 (6.44) | 44 (6.73) | 46 (7.55) | 16 (6.43) | 31 (7.87) |
| Hispanic (all) | 30 (3.72) | 23 (3.53) | 25 (3.82) | 22 (3.61) | 9 (3.61) | 17 (4.31) |
| Asian | 64 (7.94) | 53 (8.13) | 47 (7.19) | 44 (7.22) | 19 (7.63) | 33 (8.38) |
| Mixed race/Other | 23 (2.85) | 17 (2.61) | 16 (2.45) | 15 (2.46) | 5 (2.01) | 10 (2.54) |
| Female Gender | 447 (55.56) | 360 (55.21) | 371 (56.73) | 337 (55.34) | 125 (50.20) | 234 (59.39) |
| High Education | 443 (54.96) | 378 (57.98) | 382 (58.41) | 352 (57.80) | 128 (51.41) | 233 (59.14) |
| High Income | 357 (44.29) | 306 (46.93) | 308 (47.09) | 279 (45.81) | 116 (46.59) | 177 (44.92) |
| High news frequency | 672 (83.37) | 555 (85.12) | 561 (85.78) | 512 (84.07) | 211 (84.74) | 353 (89.59) |
| Excellent/Good Self-rated health | 642 (79.65) | 525 (80.52) | 522 (79.82) | 490 (80.46) | 215 (86.35) | 322 (81.73) |
| Skepticism (mean ± SD) | 12.88 (2.31) | 13.12 ± 2.07 | 13.19 ± 2.08 | 13.10 ± 2.08 | 11.89 ± 2.53 | 13.34 ± 1.95 |
| Political affiliation | ||||||
| Republican | 178 (22.08) | 145 (22.24) | 142 (21.71) | 143 (23.48) | 123 (49.40) | 68 (17.26) |
| Democrat | 358 (44.42) | 305 (46.78) | 315 (48.17) | 283 (46.47) | 51 (20.48) | 228 (57.87) |
| Independent | 233 (28.91) | 181 (27.76) | 172 (26.30) | 164 (26.93) | 64 (25.70) | 84 (21.32) |
| Other | 37 (4.59) | 21 (3.22) | 25 (3.82) | 19 (3.12) | 11 (4.42) | 14 (3.55) |
How much do you trust information from [A to E above] about coronavirus. High ratings of trust were considered those who reported that they trusted the source a great deal or quite a bit.
Participants at baseline showed relatively low rates of COVID-19 skepticism, with 13.4% of respondents reporting that they agreed or strongly agreed with the statement that “the health risks from the coronavirus have been exaggerated,” and 9.9% reporting that they neither agreed or disagreed. To the statement that “the coronavirus isn’t any worse than the flu,” 7% agreed or strongly agreed, and 8.7% neither agreed or disagreed. Only 2.7% agreed or strongly agreed with the statement that “the coronavirus is a hoax,” and 3.8% neither agreed or disagreed. These three items on COVID-19 skepticism were summed with a scale, which had a mean of 12.88 (SD=2.31)
At baseline, in response to the five questions on, “How much do you trust information from [blank]”, the highest rated sources of trustworthiness for COVID-19 information were the CDC (42.4% a great deal and 38.5% quite a bit), state health department (33.6% a great deal and 41.9% quite a bit) and universities (Johns Hopkins 43.7% a great deal and 37.5% quite a bit). Mainstream media such as CNN rated in the middle (12.3% a great deal and 36.6% quite a bit). The White House was rated low (10.7% a great deal and 20.2% quite a bit). The categories of “a great deal” and “quite a bit” were combined into a high trust category and compared to low trust, which combined the categories of “some” and “very little or none.” The rating of very little or no trust was lowest for CDC (3.7%), state health department (3.6%), and Johns Hopkins (3.6%) and highest for the White House (40%).
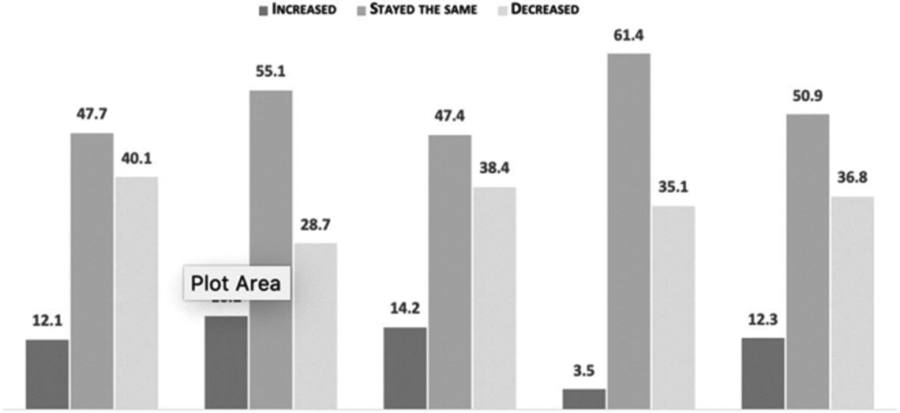
Next, changes in the level of trustworthiness of information sources for the 592 respondents who completed both the March and July 2020 surveys and had complete data were assessed (Table 2). For all five sources of COVID-19 information, there was a larger proportion of decreases in trustworthiness as compared to increases. Net change in trust was assessed by subtracting percent decrease in trust by percent increase in trust. Any positive percentage indicated a net decrease in trust. The net decrease in trust of COVID-19 information from the CDC was 28% (t=10.35, p<001). For state health departments, the net decrease in trustworthiness of COVID-19 information was 24.2% (t=8.72, p<001); for Johns Hopkins University, the net decrease was 12.5% (t=4.53, p<001); for the mainstream media, the net decrease was 24.5% (t=9.62, p<001), and, for the White House, there was a 31.6% net decrease in trustworthiness in COVID-19 information (t=12.97, p<001).
Table 2:
Percent change in trustworthiness of sources of COVID-19 information among respondents who completed surveys in March and July 2020 (N=592)
 | |||||
|---|---|---|---|---|---|
| Model 1: CDC | Model 2: Johns Hopkins University | Model 3: Health Department | Model 4: White House | Model 5: Mainstream News | |
| N = 593 | N (%) | N (%) | N (%) | N (%) | N (%) |
| High Trust in March, 2020 | 482 (81.3) | 494 (83.3) | 446 (75.2) | 174 (29.3) | 378 (63.7) |
| High Trust in July, 2020 | 378 (63.7) | 452 (76.2) | 378 (63.7) | 85 (14.3) | 203 (34.2) |
Table 3 provides the bivariate analyses of factors associated with ratings of trust. Individuals with higher education levels and those who viewed news about COVID-19 more frequently tended to exhibit higher trust ratings in information sources from CDC, state health departments, mainstream media, and Johns Hopkins University. Trust in the White House was associated with respondents reporting higher subjective health and male gender. There were strong partisan divides, with Democrats and Independents providing lower odds of rating the White House as trustworthy compared to Republicans. However, Republicans reported multiple information sources as more trustworthy than the White House, with 80% or more reporting high ratings of trust in their state health department, Johns Hopkins University, and the CDC compared to 69% of Republicans reporting high trust in the White House (data not shown). Individuals with higher levels of income also reported higher ratings of trust in the CDC and universities compared to those with lower levels of income.
Table 3.
Predictors of baseline trust in sources of COVID-19 information and decrease in trust.
| Model 1: CDC | Model 2: Johns Hopkins University | Model 3: State Health Department | Model 4: White House | Model 5: Mainstream News | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Wave 3 | Baseline | Wave 3 | Baseline | Wave 3 | Baseline | Wave 3 | Baseline | Wave 3 | ||||||||||
| OR (95% CI) | aOR * (95% CI) | Reduced Trust aOR* (95% CI) | OR (95% CI) | aOR* (95% CI) | Reduced Trust aOR* (95% CI) | OR (95% CI) | aOR* (95% CI) | Reduced Trust aOR * (95% CI) | OR (95% CI) | aOR* (95% CI) |
Reduced Trust aOR* (95% CI) |
OR (95% CI) | aOR* (95% CI) |
Reduced Trust aOR* (95% CI) | |||||
| High self-rated health | 1.31 (0.86–1.98) | 1.43 (0.91–2.27) | 0.82 (0.53–1.28) | 1.06 (0.68–1.63) | 1.26 (0.77–2.04) | 1.01 (0.62–1.65) | 1.22 (0.83–1.80) | 1.33 (0.88–2.02) | 1.38 (0.88–2.17) | 1.93 (1.28–2.91) | 1.67 (1.03–2.71) | 1.10 (0.70–1.74) | 1.29 (0.91–1.82) | 1.56 (1.07–2.27) | 1.04 (0.67–1.61) | ||||
| High news consumption | 1.81 (1.18–2.78) | 1.37 (0.86–2.18) | 1.19 (0.74–1.93) | 2.23 (1.46–3.39) | 1.59 (1.00–2.54) | 1.33 (0.79–2.23) | 1.22 (0.80–1.85) | 0.96 (0.61–1.50) | 1.45 (0.90–2.34) | 1.16 (0.77–1.74) | 1.60 (0.98–2.62) | 1.01 (0.63–1.63) | 2.51 (1.69–3.74) | 2.07 (1.35–3.16) | 1.42 (0.88–2.30) | ||||
| Low skepticism | 1.23 (1.15–1.32) | 1.25 (1.15–1.35) | 0.94 (0.86–1.02) | 1.31 (1.22–1.41) | 1.27 (1.18–1.38) | 0.90 (0.83–0.98) | 1.17 (1.01–1.25) | 1.20 (1.11–1.29) | 0.94 (0.86–1.02) | 0.77 (0.72–0.82) | 0.80 (0.74–0.87) | 0.92 (0.85–1.00) | 1.20 (1.12–1.28) | 1.14 (1.06–1.22) | 1.05 (0.97–1.14) | ||||
| Political party affiliation Ref: Republican | |||||||||||||||||||
| Democrat | 1.31 (0.81–2.11) | 1.03 (0.61–1.74) | 0.36 (0.23–0.58) | 1.86 (1.14–3.02) | 1.58 (0.92–2.72) | 0.41 (0.26–0.67) | 0.92 (0.59–1.45) | 0.70 (0.43–1.13) | 0.59 (0.37–0.94) | 0.07 (0.05–0.12) | 0.09 (0.06–0.14) | 0.40 (0.25–0.64) | 2.84 (1.96–4.11) | 2.57 (1.71–3.83) | 0.51 (0.32–0.81) | ||||
| Independent | 0.79 (0.49–1.29) | 0.81 (0.48–1.38) | 0.60 (0.37–0.96) | 0.72 (0.45–1.14) | 0.82 (0.49–1.37) | 0.50 (0.30–0.81) | 0.58 (0.37–0.93) | 0.55 (0.34–0.90) | 0.71 (0.44–1.14) | 0.17 (0.11–0.26) | 0.17 (0.11–0.27) | 0.39 (0.24–0.64) | 0.91 (0.61–1.37) | 0.99 (0.65–1.51) | 0.64 (0.40–1.03) | ||||
| Other | 0.30 (0.14–0.63) | 0.30 (0.13–0.65) | 0.30 (0.12–0.79) | 0.53 (0.24–1.15) | 0.59 (0.26–1.36) | 0.49 (0.19–1.28) | 0.26 (0.12–0.54) | 0.23 (0.11–0.51) | 0.79 (0.33–1.90) | 0.19 (0.09–0.41) | 0.16 (0.07–0.36) | 0.58 (0.24–1.41) | 0.99 (0.48–2.04) | 1.12 (0.53–2.37) | 0.75 (0.31–1.80) | ||||
| Age | 1.00 (0.99–1.02) | 1.00 (0.98–1.01) | 1.03 (1.01–1.04) | 1.03 (1.01–1.04) | 1.02 (1.00–1.04) | 1.00 (0.99–1.02) | 1.00 (0.99–1.01) | 0.99 (0.98–1.01) | 1.00 (0.99–1.02) | 1.00 (0.99–1.02) | 1.00 (0.98–1.02) | 1.01 (0.99–1.03) | 1.01 (1.00–1.02) | 1.01 (0.99–1.02) |
1.00 (0.99–1.02) | ||||
| Female gender | 0.95 (0.67–1.35) | 1.25 (0.85–1.83) | 0.92 (0.64–1.32) | 1.31 (0.92–1.87) | 1.03 (0.69–1.52) | 1.00 (0.68–1.47) | 0.98 (0.71–1.35) | 1.19 (0.84–1.69) | 1.10 (0.77–1.56) | 0.74 (0.55–0.99) | 1.32 (0.92–1.89) | 0.65 (0.45–0.94) | 1.37 (1.03–1.81) | 0.85 (0.63–1.15) | 0.95 (0.67–1.35) | ||||
| High education | 1.89 (1.32–2.70) | 1.78 (1.20–2.65) | 0.92 (0.63–1.32) | 2.10 (1.46–3.00) | 2.04 (1.35–3.09) | 1.08 (0.73–1.61) | 1.60 (1.16–2.20) | 1.68 (1.17–2.40) | 0.83 (0.58–1.19) | 0.81 (0.60–1.10) | 0.76 (0.53–1.11) | 0.93 (0.65–1.35) | 1.39 (1.05–1.84) | 1.27 (0.93–1.74) | 0.87 (0.61–1.25) | ||||
| High income | 1.79 (1.24–2.58) | 1.43 (0.95–2.15) | 1.45 (1.01–2.10) | 1.87 (1.29–2.72) | 1.56 (1.03–2.37) | 1.33 (0.90–1.96) | 1.29 (0.93–1.79) | 1.05 (0.73–1.50) | 1.07 (0.74–1.54) | 1.14 (0.85–1.54) | 0.98 (0.67–1.43) | 0.73 (0.50–1.06) | 1.05 (0.80–1.39) | 0.94 (0.69–1.29) | 0.91 (0.64–1.31) | ||||
Bold= p<.05, OR= Odds Ratio, aOR= Adjusted Odds Ratio, CI=Confidence Interval, Reduced Trust=From baseline to wave 3, N=592. Baseline N=806*In addition to the variables presented, the aOR also adjusted for race/ethnicity (data not shown).
Table 3 also reports multivariable models of factors associated with trust at baseline. The adjusted models (aOR) included age, education, gender, race/ethnicity, income, health status, COVID-19 Skepticism, frequency of news consumption, and political party affiliation. As seen in Table 3, trust in the White House was significantly negatively associated with not being a Republican (Democrats, Independents, and others) and positively associated with higher subjective health. Those who were less skeptical about the COVID-19 pandemic, as assessed on the scale of COVID-19 skepticism, were less likely to view the White House as a trustworthy source of coronavirus news. In contrast, high ratings of trust in information from their state health department were positively associated with higher education and scoring lower on the scale of COVID-19 skepticism. Independents and others were less likely to report a high rating of trust in their state health department as compared to Republicans. This pattern of associations was similar for rating CDC as a highly trusted source of COVID-19 information. Reporting higher ratings of trust in Johns Hopkins as an information source was associated with more frequent news consumption, lower COVID-19 skepticism, higher income, and higher education levels. Trust in mainstream media was significantly associated with being a Democrat compared to a Republican, scoring lower on the scale of COVID-19 skepticism, more frequently obtaining news about COVID-19, and reporting higher subjective health.
The last set of multivariable regression models assessed baseline factors associated with reduced trust in sources of COVID-19 information at wave 3 (July 2020) compared to baseline (March, 2020; Table 3). The aOR model compares reports of reduced trust over the two time periods compared to no change or increased trust. All models for reduced trust are adjusted for the same baseline variables that were included in the baseline aOR model. The most consistent predictor of decreased in trust was political party affiliation, with Democrats less likely to report decreased trust across all sources compared to Republicans. Higher income level (OR=1.45, CI=1.01–2.10) and older age (OR=1.03, CI=1.01–1.04) were associated with a decreased trustworthiness of COVID-19 information from the CDC. Decreased trustworthiness of COVID-19 information from Johns Hopkins University was associated with higher levels COVID-19 skepticism (OR=0.90, CI=0.83–0.98). Higher income level (OR=1.07, CI=0.74–1.54) was associated with a decrease in the trustworthiness of COVID-19 information from state health departments and the CDC. Decreased trustworthiness of COVID-19 information from the White House was negatively associated with low levels of COVID-19 skepticism (OR=0.92, CI=0.85–1.00), female gender (OR=0.65, CI=0.45–0.94), and Democratic (OR=0.40, CI=0.25–0.64) or Independent (OR=0.39, CI=0.24–0.64) political party affiliation.
Discussion
In this study, there were reports of a high level of trust in COVID-19 information from the CDC, the state health department, and a major university at baseline. There was a moderate level of trust from mainstream media and low trust ratings in information from the White House. Major differences based on political party affiliations were identified for COVID-19 information from mainstream media and the White House. However, Republicans reported greater trust in CDC, state health departments, and a major university than in the White House. This finding is consistent with a prior Mturk study of United States residents in which mainstream media was perceived as more trustworthy among Democrats than Republicans, but with both groups reporting higher trust in mainstream media, such as New York Times and Washington Post, than in hyper-partisan and fake news, such as Infowars and Breitbart (Pennycook & Rand, 2019). We did not find ethnic/racial differences in the trustworthiness of sources of COVID-19 information. However, we did not examine specific mainstream media news sources that may target audiences based on ethnicity and race.
At baseline, the correlates of trustworthiness of sources of COVID-19 information differed substantially by source. In the multivariate analyses, one of the most consistent correlates was COVID-19 skepticism. Political party affiliation was significantly associated with trustworthiness for four of the sources of COVID-19 information, and education level was associated with three of the sources.
There was a statistically significant decrease in the trustworthiness of sources of COVID-19 information over four months for all five sources. The finding of a substantial decrease in the trustworthiness of all five measured sources of COVID-19 information over a relatively brief period is of great concern due to the need for trustworthy public health messages on COVID-19 prevention behaviors and potentially on vaccines. Some of this erosion in trust may be due to information about the sources of the infection, potential vaccines, and recommended preventive measures that have themselves been changing, as the underlying science has been evolving. However, this change over time may be perceived by the public as proof that even experts do not have a clear understanding of the disease and the various risk factors. The public health challenge, of course, is to find the appropriate balance between communicating the evolving nature of knowledge about the epidemic, on the one hand, with providing consistent guidelines, on the other.
The largest reductions in trust in information sources were for the White House and the CDC. The smallest reduction was for Johns Hopkins University. Likely, inconsistent and contradictory messages from the CDC, the White House, and other government agencies lead to this decrease in trust (Lipton et al., 2020). This confusion may lead individuals to not know whom to trust for accurate COVID-19 information. The political polarization and partisan dialog on COVID-19 may have also led to a decrease in trusting COVID-19 information from all sources (Zhao, Wu, Crimmins, & Ailshire, 2020). Only one variable, Democrat political party affiliation, was consistently associated with no decrease in the trustworthiness of sources of COVID-19 information. Additionally, at the March 2020 baseline, Republicans were, in general, less trusting of COVID-19 news sources than others. These data suggest that although the CDC, health departments, and major universities are trusted for information about COVID-19, more attention is needed in addressing politically partisan audiences.
Notably, a small percentage of individuals expressed COVID-19 skepticism, which was associated with reduced trust in all sources, except for the White House. COVID-19 skepticism is a critical area meriting intervention, because if these individuals do not socially distance and engage in preventive behaviors, they could impact the spread of COVID-19. Future research should assess how sources of news and trustworthiness may lead to behavior change to stop the spread of COVID-19 and increase hygienic practices as well as vaccine-related behaviors.
These findings also suggest the need to segment audiences and encourage more coherent messaging within and among government agencies and develop community-based programs to provide COVID-19 information. Without coherent and scientifically based messages, it may be difficult to mobilize large sectors of the US population to engage in prevention behaviors and to receive effective COVID-19 vaccines.
This research also points to the need to determine who comprises the most credible and trustworthy sources among the various audience groups. For example, our finding that trust eroded the most among Republican respondents suggests that we need to identify sources of information for this group that can be most effective in persuading them to take preventive measures. Even though this study focused on information sources, other aspects of the communication process (including message framing, channel characteristics, identifying key influencers, etc.) should also be a part of the equation in public health communication efforts. We know, for example, that different message frames produce different effects (Kühberger, 1998), and that losses loom larger in people’s minds than equivalent gains (Tverysky & Kahneman, 1991). Future studies should investigate how trust erosion among different audience segments can be minimized through the use of appropriate message frames.
This study is not without limitations. One of the study’s limitations was that since trustworthiness did not start at the same level among all participants, there were different potentials for increases or decreases in trust levels among the five sources of information. There may have been regression to the mean with those that started at very high or low trustworthiness. Regression to the mean may also help to explain why COVID-19 skepticism was associated with lower likelihood of a reduction in trust in information from Johns Hopkins University. At baseline, COVID-19 skepticism was associated with lower levels of trust in information from Johns Hopkins University. Consequently, there was less room for a decrease in trust among those who scored high on COVID-19 skepticism. The study also did not incude a representative sample. The sample has similar demographic characteristics found in other online studies (Berinsky, Huber, & Lenz, 2012; Huff & Tingley, 2015; Paolacci & Chandler, 2014). In general, MTurk samples tend to be younger, more educated, less religious, and more liberal as well as less likely to be married, a racial minority, or fully employed than those in a nationally representative study (Berinsky et al., 2012; Huff & Tingley, 2015; Paolacci & Chandler, 2014). Mturk studies tend to be under-representative of Republicans and older individuals. However, approximately a quarter of the sample was Republican, allowing for adequate comparisons with other political groups. The lack of racial diversity in the sample is problematic, especially since the pandemic has disproportionately impacted people of color. Online survey researchers need to develop best practices for recruiting racially diverse samples to ensure that their opinions and perspetives are adequately represented. We also did not have information about specific sources of mainstream media information (e.g., FOX News, or MSNBC) or ask about frequency and use of social media, which may have a strong influence on opinions and sources of COVID-19 misinformation. We followed the best practice guidelines for using online data collection to enhance the survey’s validity and included several validity checks. However, we do not know if trust in information sources or perceptions of COVID-19 influenced survey participation or responses. However, prior research has found that comparisons of MTurk to other forms of sampling, such as college or community sampling, suggest that MTurk participants are no more or less likely to engage in dishonest or disingenuous behavior (e.g., responding in socially acceptable ways or without paying attention) (Necka, Cacioppo, Norman, & Cacioppo, 2016). In the current study, it should also be noted that there were little missing data, even though respondents were not required to answer all the questions. Moreover, there were high response rates for open-ended questions, and these responses tended to be detailed and thoughtful. The study was also conducted before the US President and other White House officials tested positive for COVID-19. This event and the ensuing contradictory information about the transmission dynamics in the White House, the health of the President, and the severity of COVID-19 may also impact perceptions of trust in information sources about COVID-19.
The study findings clearly documented a decline in the perceived trustworthiness of COVID-19 information from key sources of health information during the early months of the COVID-19 pandemic in the United States. Although there may be multiple causes for this decline, the findings highlight the importance of developing strategies to increase the perceived trustworthiness of COVID-19 information and identifying and addressing factors that have led to the decrease in the perceived trustworthiness of COVID-19 information. Ensuring the perceived trustworthiness of COVID-19 information is critical in order to promote COVID-19 prevention behaviors and vaccine uptake.
Acknowledgment:
Study participants
Funding sources: R01 DA040488
Footnotes
Financial disclosures: None
Conflict of interest: None
References
- Abraham T (2009). Risk and outbreak communication: Lessons from alternative paradigms. Bulletin of the World Health Organization, 87, 604–607. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ali SH, Foreman J, Tozan Y, Capasso A, Jones AM, & DiClemente RJ (2020). Trends and predictors of COVID-19 information sources and their relationship with knowledge and beliefs related to the pandemic: Nationwide cross-sectional study. JMIR Public Health and Surveillance, 6(4), e21071. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Allington D, Duffy B, Wessely S, Dhavan N, & Rubin J (2020). Health-protective behaviour, social media usage and conspiracy belief during the COVID-19 public health emergency. Psychological Medicine, 1–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berinsky AJ, Huber GA, & Lenz GS (2012). Evaluating online labor markets for experimental research: Amazon.com’s mechanical turk. Political Analysis, 20(3), 351–368. 10.1093/pan/mpr057 [DOI] [Google Scholar]
- Cairns G, de Andrade M, MacDonald L. (2013). Reputation, relationships, risk communication, and the role of trust in the prevention and control of communicable disease: a review. Journal of Health Communication. 18(12):1550–65. doi: 10.1080/10810730.2013.840696. [DOI] [PubMed] [Google Scholar]
- Chandler J, & Shapiro D (2016). Conducting Clinical Research Using Crowdsourced Convenience Samples. Annual Review of Clinical Psychology, 12(1), 53–81. 10.1146/annurev-clinpsy-021815-093623 [DOI] [PubMed] [Google Scholar]
- Cuffee YL, Hargraves JL, Rosal M, Briesacher BA, Schoenthaler A, Person S, … Allison J (2013). Reported racial discrimination, trust in physicians, and medication adherence among inner-city African Americans with hypertension. American Journal of Public Health, 103(11), 55–62. 10.2105/AJPH.2013.301554 [DOI] [PMC free article] [PubMed] [Google Scholar]
- de Bruin WB, Saw H, & Goldman DP (2020). Political polarization in US residents’ COVID-19 risk perceptions, policy preferences, and protective behaviors. Journal of Risk and Uncertainty, 1–18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Balog-Way Dominic H. P. & McComas Katherine A. (2020). COVID-19: Reflections on trust, tradeoffs, and preparedness, Journal of Risk Research, DOI: 10.1080/13669877.2020.1758192 [DOI] [Google Scholar]
- Follmer D, Sperline R, & Suen H (2017). The role of MTurk in education research: Advantages, Issues, and Future Directions. Educational Researcher, 46(6), 329–334. [Google Scholar]
- Gilson L (2003). Trust and the development of health care as a social institution. Social Science & Medicine, 56, 1453–1468 [DOI] [PubMed] [Google Scholar]
- Gollwitzer A, Martel C, Brady WJ, Pärnamets P, Freedman IG, Knowles ED, & Van Bavel JJ (2020). Partisan differences in physical distancing are linked to health outcomes during the COVID-19 pandemic. Nature Human Behaviour, 1–12. [DOI] [PubMed] [Google Scholar]
- Huff C, & Tingley D (2015). “Who are these people?” Evaluating the demographic characteristics and political preferences of MTurk survey respondents. Research and Politics, 2(3). 10.1177/2053168015604648 [DOI] [Google Scholar]
- Jacobs EA, Rolle I, Ferrans CE, Whitaker EE, & Warnecke RB (2006). Understanding African Americans’ views of the trustworthiness of physicians. Journal of General Internal Medicine, 21(6), 642–647. 10.1111/j.1525-1497.2006.00485.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jurkowitz M, Mitchell A, Shearer E, & Walker M (2020). U.S. media polarization and the 2020 election: A nation divided. Retrieved from https://www.journalism.org/2020/01/24/democrats-report-much-higher-levels-of-trust-in-a-number-of-news-sources-than-republicans/ [Google Scholar]
- Kanekar AS, & Thombre A (2019). Fake medical news: Avoiding pitfalls and perils. Family Medicine and Community Health, 7(4), 1–4. 10.1136/fmch-2019-000142 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kühberger A (1998). The influence of framing on risky decisions: A meta-analysis. Organizational behavior and human decision processes, 75(1), 23–55. [DOI] [PubMed] [Google Scholar]
- Larson HJ, Clarke RM, Jarrett C, Eckersberger E, Levine Z, Schulz WS, & Paterson P (2018). Measuring trust in vaccination: A systematic review. Human vaccines & immunotherapeutics, 14(7), 1599–1609. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Larson HJ, Jarrett C, Eckersberger E, Smith DM, & Paterson P (2014). Understanding vaccine hesitancy around vaccines and vaccination from a global perspective: A systematic review of published literature, 2007–2012. Vaccines, 32(19), 2150–2159. [DOI] [PubMed] [Google Scholar]
- Larson H, Leask J, Aggett S, Sevdalis N, & Thomson A (2013). A multidisciplinary research agenda for understanding vaccine-related decisions. Vaccines, 1(3), 293–304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lazer DMJ, Baum MA, Benkler Y, Berinsky AJ, Greenhill KM, Menczer F, … Zittrain JL (2018). The science of fake news: Addressing fake news requires a multidisciplinary effort. Science, 359(6380), 1094–1096. 10.1126/science.aao2998 [DOI] [PubMed] [Google Scholar]
- Lee T-T (2010). Why They Don’t Trust the Media: An Examination of Factors Predicting Trust. American Behavioral Scientist, 54(1), 8–21. [Google Scholar]
- MacDonald NE (2015). Vaccine hesitancy: Definition, scope and determinants. Vaccine, 33(34), 4161–4164. [DOI] [PubMed] [Google Scholar]
- Lipton E, Goodnough A, Shear M, Twohey M, Mandavilli A, Fink S, & Walker M (2020). The C.D.C. waited ‘Its entire existence for this moment.’ what went wrong? Retrieved from https://www.nytimes.com/2020/06/03/us/cdc-coronavirus.html.
- Menon K, Goh KT. (2005). Transparency and trust: Risk communications and the Singapore experience in managing SARS. Journal of Communication Management. 9(4):375–383. [Google Scholar]
- Miller G (2020). Researchers are tracking another pandemic, too—of coronavirus misinformation. Retrieved July 15, 2020, from https://www.sciencemag.org/news/2020/03/researchers-are-tracking-another-epidemic-too-misinformation [Google Scholar]
- Motta M, Stecula D, & Farhart C (2020). How Right-Leaning Media Coverage of COVID-19 Facilitated the Spread of Misinformation in the Early Stages of the Pandemic in the U.S.. Canadian Journal of Political Science. Revue Canadienne De Science Politique, 1–8. 10.1017/S0008423920000396 [DOI] [Google Scholar]
- Necka EA, Cacioppo S, Norman GJ, & Cacioppo JT (2016). Measuring the prevalence of problematic respondent behaviors among MTurk, campus, and community participants. PLoS ONE, 11(6), 1–19. 10.1371/journal.pone.0157732 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Paolacci G, & Chandler J (2014). Inside the Turk: Understanding Mechanical Turk as a Participant Pool. Current Directions in Psychological Science, 23(3), 184–188. 10.1177/0963721414531598 [DOI] [Google Scholar]
- Pennycook G, & Rand DG (2019). Fighting misinformation on social media using crowdsourced judgments of news source quality. Proceedings of the National Academy of Sciences of the United States of America, 116(7), 2521–2526. 10.1073/pnas.1806781116 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peters A, Tartari E, Lotfinejad N, Parneix P, & Pittet D (2018). Fighting the good fight: the fallout of fake news in infection prevention and why context matters. Journal of Hospital Infection, 100(4), 365–370. 10.1016/j.jhin.2018.08.001 [DOI] [PubMed] [Google Scholar]
- Pew Research Center. (2020). Election News Pathways project. Retrieved July 15, 2020, from https://www.pewresearch.org/pathways-2020/covidegfp_f/total_us_adults/us_adults/ [Google Scholar]
- Rouse SV (2015). A reliability analysis of Mechanical Turk data. Computers in Human Behavior, 43, 304–307. 10.1016/j.chb.2014.11.004 [DOI] [Google Scholar]
- Sbaffi L, & Rowley J (2017). Trust and credibility in web-based health information: A review and agenda for future research. Journal of Medical Internet Research, 19(6), 1–17. 10.2196/jmir.7579 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Scheufele DA, & Krause NM (2019). Science audiences, misinformation, and fake news. Proceedings of the National Academy of Sciences of the United States of America, 116(16), 7662–7669. 10.1073/pnas.1805871115 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shavers VL, Lynch CF, & Burmeister LF (2000). Knowledge of the Tuskegee Study and its impact on the willingness to participate in medical research studies. Journal of the National Medical Association, 92(12), 563–572. [PMC free article] [PubMed] [Google Scholar]
- Shimizu K (2020). 2019-nCoV, fake news, and racism. The Lancet, 395(10225), 685–686. 10.1016/S0140-6736(20)30357-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Strickland JC, & Stoops WW (2019). The use of crowdsourcing in addiction science research: Amazon Mechanical Turk. Experimental and Clinical Psychopharmacology, 27(1), 1–18. [DOI] [PubMed] [Google Scholar]
- Tversky A, & Kahneman D (1991). Loss aversion in riskless choice: A reference-dependent model. The quarterly journal of economics, 106(4), 1039–1061. [Google Scholar]
- Wang Y, McKee M, Torbica A, & Stuckler D (2019). Systematic Literature Review on the Spread of Health-related Misinformation on Social Media. Social Science and Medicine, 240(August), 112552. 10.1016/j.socscimed.2019.112552 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Young J, & Young K (2019). Don’t Get Lost in the Crowd: Best Practices for Using Amazon’s Mechanical Turk in Behavioral Research. Journal of the Midwest Association for Information Systems, (July), 7–34. 10.17705/3jmwa.000050 [DOI] [Google Scholar]
- Zhao E, Wu Q, Crimmins EM, & Ailshire JA (2020). Media trust and infection mitigating behaviours during the COVID-19 pandemic in the USA. BMJ Global Health, 5(10), 10.1136/bmjgh-2020-003323. [DOI] [PMC free article] [PubMed] [Google Scholar]