

SUMMARY:
A ruptured dermoid cyst is rare and can present with various symptoms. We report imaging findings of an intracranial dermoid cyst that ruptured into the endolymphatic sac, causing sudden sensorineural hearing loss.
Dermoid cyst is a rare congenital intracranial tumor.1 It arises from ectopic inclusion of the embryonic ectoderm into the neural tube during the third to fifth weeks of embryonic life and is usually located in the midline.2 Dermoid cysts are composed of a stratified squamous epithelium and skin adnexal structures, such as hair follicles, sebaceous, or sweat glands; therefore, they contain products of these adnexal structures and epithelium, such as lipid metabolites, cholesterol crystals, hair, decomposed epithelial cells, and calcification.2,3 Radiologic diagnosis of dermoid cysts is made on the basis of lipid content.1,4 Symptoms related to unruptured dermoid cysts are nonspecific.1,3,5,6 A dermoid cyst can rupture and present with various symptoms, including headache, seizure, focal neurologic deficits, or even sudden death.2,7,8 We present a dermoid cyst that ruptured into the endolymphatic sac, causing sudden sensorineural hearing loss.
Case Report
A 17-year-old girl presented with sudden hearing loss of the right ear, which had developed 7 days earlier. On physical examination, her tympanic membrane appeared normal and mobile. Pure-tone audiometry showed sensorineural hearing loss of 64 dB (the average of values at 500, 1000, and 2000 Hz) in the right ear. Her speech discrimination scores were 24% at 80 dB in the right ear and 100% at 40 dB in the left ear.
Temporal bone CT showed a well-defined ovoid mass measuring approximately 1.5 × 1 × 1.2 cm with very low attenuation (−80 to −120 HU) between the sigmoid sinus and the cerebellum along the posterior petrous ridge. The mass extended into the vestibular aqueduct, which was also filled with very low-attenuation material (Fig 1). The mass showed heterogeneous hyperintensity on both T1WI and T2WI, and the signal intensity from the mass was suppressed on fat-suppressed T1WI (Figs 2 and 3). The mass was diagnosed radiologically as a dermoid cyst. It was found to be in contact with the right vestibular aqueduct, which showed slight dilation, and was filled with T1 and T2 high-signal-intensity lesions. High-resolution T2WI demonstrated a hypointense thin line between the dermoid cyst and vestibular aqueduct, suggesting the margin of the tumor and a dilated endolymphatic sac. High-resolution T1WI and T2WI showed foci of high signal intensity in the vestibule and cochlea, which were successfully suppressed on a fat-suppressed T1WI, representing lipid metabolites (Figs 2 and 3). Putting all of the findings together, we finally diagnosed the patient radiologically with a dermoid cyst, which had ruptured into the endolymphatic sac.
Fig 1.
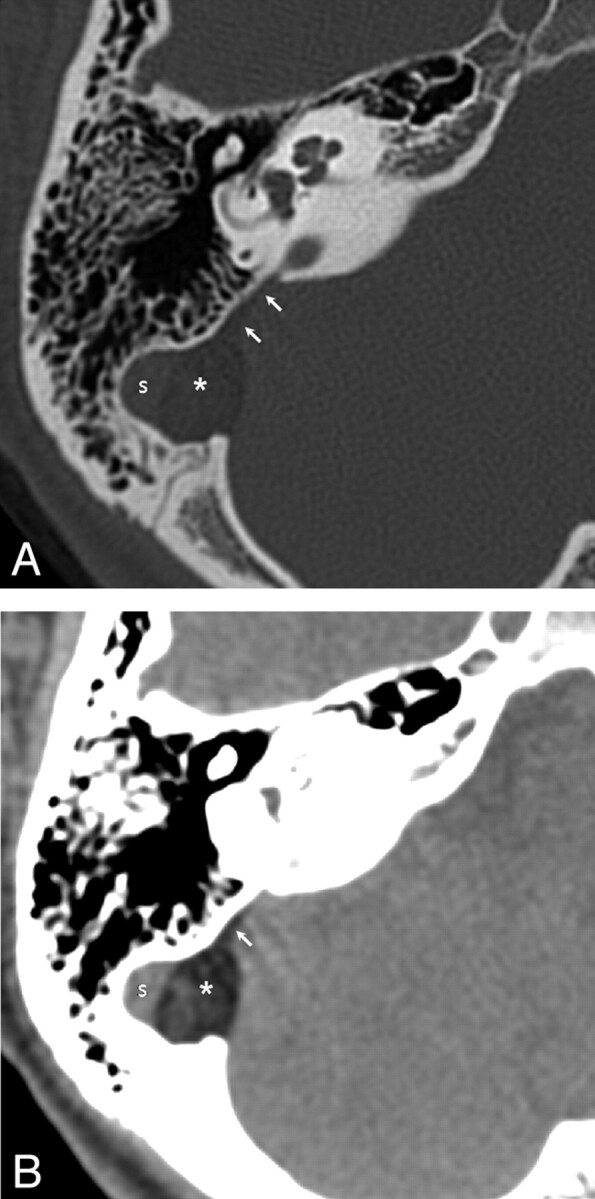
Bone window setting (A) and soft-tissue window setting (B) of temporal bone CT show a well-defined very low-attenuation ovoid mass (asterisk) between the sigmoid sinus and cerebellum. The mass extends into the right vestibular aqueduct (arrow).
Fig 2.

T2WI at the level of the bilateral vestibular aqueducts. Compared with the normal left vestibular aqueduct (long arrow), the right vestibular aqueduct (short arrow) is dilated and filled with hyperintense material. Between the dilated right vestibular aqueduct and the tumor, there is a thin hypointense line (arrowheads) representing the border of the dermoid cyst (asterisk) and endolymphatic sac (short arrow).
Fig 3.

High-resolution T2 (A), T1 (B), and fat-saturated T1WI (C) of the right inner ear. Foci of T2 (A) and T1 (B) high signal intensity (arrowheads) are seen at the right cochlea and vestibule. These high signals of the tumor (asterisk), in the right cochlea, vestibule, and vestibular aqueduct (arrow), are successfully suppressed on fat-saturated T1WI (C).
The patient underwent surgery, resulting in gross total resection. The tumor was located between the medial sigmoid dural sinus wall and the lateral cerebellar dura. Incision of the tumor capsule revealed dirty yellowish semisolid tissue contents containing black hairy filaments. The histopathologic specimen showed keratinous debris and sebaceous glands lined by stratified keratinizing squamous epithelium. The final diagnosis of a dermoid cyst that had ruptured into the endolymphatic sac was made on the basis of surgical and histopathologic findings and radiologic evidence of lipids in the endolymphatic structure.
Discussion
Dermoid cyst is a rare intracranial tumor.1 It originates from the embryonic ectoderm and, therefore, contains products of adnexal structures and epithelium, such as lipid metabolites, cholesterol crystals, hair, decomposed epithelial cells, and calcification.2,3 Dermoid cysts have imaging findings similar to those of fat because they contain lipid metabolites; therefore, they are hyperintense on T1WI and do not enhance.1,4 Their typical locations in the intracranium include the suprasellar, parasellar, temporal, frontobasal regions, and the posterior fossa; and intradural, interdural, or extradural regions in relation to the dura mater.1–3,5,8,9 Interdural location of a dermoid cyst is extremely rare, and the lateral wall of the cavernous sinus is the most frequent site.3,5 Dermoid cysts are not true neoplasms, which grow by cell division; however, with an increase of internal contents by desquamation of epithelium and secretion of adnexal glands, dermoid cysts can grow. The clinical presentation of dermoid cysts is usually related to elevated intracranial pressure and compression of adjacent structures.
Rupture of a dermoid cyst is a rare but well-documented phenomenon.2,7,8 The possible mechanism of rupture is an increase of glandular secretions due to age-dependent hormonal changes, movements of the head, or brain pulsation.2,7 Patients with ruptured dermoid cysts can present with various symptoms and complications, including headache, seizures, focal neurologic deficits, aseptic meningitis, hydrocephalus, vasospasm, or cerebral ischemia.1,2,7,8 The pathophysiology of symptoms is not fully understood; however, a meningeal inflammatory reaction caused by chemical irritation due to spillage of lipids and direct occlusion of the aqueduct caused by a large lipid globule could be a possible explanation.2,7,8 Disseminated lipid droplets in CSF can be detected with sensitivity on CT or T1WI.1,10
Tumors of the cerebellopontine angle cistern, such as vestibular schwannoma, meningioma, or leptomeningeal seeding of malignant disease, can also cause sensorineural hearing loss by direct compression or invasion of the cochlear nerve.11 In endolymphatic sac tumors, endolymphatic duct obstruction and secondary hydrops might be reasonable pathophysiologic mechanisms for sensorineural hearing loss.12 The endolymphatic sac is closed and is part of the membranous labyrinth, filled with only small amounts of endolymph and embedded along the posterior wall of the petrous bone with the intra- and extraosseous portion. The distal portion of the extraosseous portion of the endolymphatic sac lies between the dural leaflets of the sigmoid sinus and the posterior fossa.13,14 The saccule and utricle, which are vesicle-like organs of the membranous labyrinth, filled with endolymph, are located within the bony vestibule surrounded by perilymph; they communicate with endolymphatic structures of the cochlea and endolymphatic sac via the endolymphatic duct.13,15 In our patient, as the tumor grew, the distal extraosseous part of the endolymphatic sac, which was lined with flat or cuboidal epithelial cells and relatively weaker than the dural leaflet, was eroded. When the dermoid cyst ruptured, spillage of lipid metabolites into the endolymphatic system could have altered the composition of the endolymph and caused disturbance of function of the inner ear structure. The high signal intensity observed on T1WI in the vestibular aqueduct, vestibule, and cochlea might be due to lipid metabolites in the endolymphatic structure—that is, the endolymphatic duct, sac, utriculosaccular system, and cochlear duct.
Other causes of T1 hyperintensity within the inner ear include hemorrhage, highly proteinaceous fluid, or intravestibular lipoma.16 Hemorrhage or highly proteinaceous fluid can be differentiated from lipid metabolites of dermoid cysts because of their lack of signal-intensity suppression on fat-saturated MR imaging techniques. It seemed to be very difficult to differentiate lipid metabolites of dermoid cysts from intravestibular lipomas, because these are T1 hyperintense and show suppression of signal intensity on fat-suppressed MR imaging. The T1 hyperintensity of the lipoma is homogeneous and shows chemical shift artifacts. These findings are not seen with dermoid cysts.4 However, tiny T1 hyperintense dermoid cysts or intracranial lipomas cannot be differentiated. In summary, dermoid cysts may be located between dural leaflets of the sigmoid sinus and the posterior fossa with a close relationship to the extraosseous portion of the endolymphatic sac. Dermoid cysts in this location can rupture into the endolymphatic sac, spilling lipid metabolites into the endolymphatic sac, which can cause sudden sensorineural hearing loss.
ABBREVIATIONS:
- S
sigmoid sinus
References
- 1. Orakcioglu B, Halatsch ME, Fortunati M, et al. Intracranial dermoid cysts: variations of radiological and clinical features. Acta Neurochir (Wien) 2008;150:1227–34, discussion 1234. Epub 2008 Nov 20 [DOI] [PubMed] [Google Scholar]
- 2. Liu JK, Gottfried ON, Salzman KL, et al. Ruptured intracranial dermoid cysts: clinical, radiographic, and surgical features. Neurosurgery 2008;62:377–84 [DOI] [PubMed] [Google Scholar]
- 3. Tun K, Celikmez RC, Okutan O, et al. Dermoid tumour of the lateral wall of the cavernous sinus. J Clin Neurosci 2008;15:820–23. Epub 2008 May 6 [DOI] [PubMed] [Google Scholar]
- 4. Osborn AG, Preece MT. Intracranial cysts: radiologic-pathologic correlation and imaging approach. Radiology 2006;239:650–64 [DOI] [PubMed] [Google Scholar]
- 5. Sturiale CL, Mangiola A, Pompucci A, et al. Interdural giant dermoid cyst of the petrous apex. J Clin Neurosci 2009;16:1498–502 [DOI] [PubMed] [Google Scholar]
- 6. Tailor R, Mollan S, Burdon M. Intracranial dermoid cyst presenting as an isolated fourth nerve palsy. J Neurol 2009;256:820–21 [DOI] [PubMed] [Google Scholar]
- 7. El-Bahy K, Kotb A, Galal A, et al. Ruptured intracranial dermoid cysts. Acta Neurochir (Wien) 2006;148:457–62 [DOI] [PubMed] [Google Scholar]
- 8. DeMonte F, al-Mefty O. Ruptured dermoid tumor of the cavernous sinus associated with the syndrome of fat embolism: case report. J Neurosurg 1992;77:312–15 [DOI] [PubMed] [Google Scholar]
- 9. Neugroschl C, David P, Sadeghi N, et al. Unusual CT features of dermoid cyst in the posterior fossa. Eur Radiol 2002;12:2726–29. Epub 2002 May 8 [DOI] [PubMed] [Google Scholar]
- 10. Smith A, Benson J, Blaser S, et al. Diagnosis of ruptured intracranial dermoid cyst: value MR over CT. AJNR Am J Neuroradiol 1991;12:175–80 [PMC free article] [PubMed] [Google Scholar]
- 11. Morley S, Beale TJ. Imaging of deafness and tinnitus. Imaging 2007;19:55–70 [Google Scholar]
- 12. Ni Y, Wang S, Huang W, et al. Surgery for endolymphatic sac tumor: whether and when to keep hearing? Acta Otolaryngol 2008;128:976–83 [DOI] [PubMed] [Google Scholar]
- 13. Lo W, Daniels D, Chakeres D, et al. The endolymphatic duct and sac. AJNR Am J Neuroradiol 1997;18:881–87 [PMC free article] [PubMed] [Google Scholar]
- 14. Friberg U, Jansson B, Rask-Andersen H, et al. Variations in surgical anatomy of the endolymphatic sac. Arch Otolaryngol Head Neck Surg 1988;114:389–94 [DOI] [PubMed] [Google Scholar]
- 15. Lane JI, Witte RJ, Henson OW, et al. Imaging microscopy of the middle and inner ear. Part II. MR microscopy. Clin Anat 2005;18:409–15 [DOI] [PubMed] [Google Scholar]
- 16. Dahlen RT, Johnson CE, Harnsberger HR, et al. CT and MR imaging characteristics of intravestibular lipoma. AJNR Am J Neuroradiol 2002;23:1413–17 [PMC free article] [PubMed] [Google Scholar]