

Abstract
Objective:
To evaluate the benefit of combined current focusing and steering to speech recognition in noise with cochlear implants (CIs).
Design:
Combined current focusing and steering was implemented using focused partial tripolar (pTP) mode with two current steering ranges. The two pTPsteering strategies were compared to a monopolar (MP) strategy without current focusing or steering and a pTP strategy with only current focusing using the Hearing in Noise Test. The strategies differed only in stimulation mode.
Study sample:
Ten post-lingually deafened adult CI users participated in this study.
Results:
Compared to the MP strategy, both pTPsteering strategies produced significantly better speech reception thresholds, while the pTP strategy did not. Subjects with better baseline MP performance had less improvements with the pTPsteering strategies. All four strategies were experimental low-rate strategies and none of them outperformed subjects’ clinical strategies.
Conclusions:
Speech recognition in noise was better with the pTPsteering strategies than with the MP strategy, but the effect of pTP-mode current steering on spectral resolution is yet to be tested.
Keywords: cochlear implant, current focusing, current steering, speech recognition
1. Introduction
Cochlear implants (CIs) successfully provide good speech recognition in quiet to many CI users. However, spectral resolution with CIs is too poor to support satisfactory speech recognition in noise (e.g., Friesen et al., 2001). The effective number of frequency channels in CIs is less than that of physical electrodes, because each electrode stimulated in monopolar (MP) mode (Figure 1a) generates a broad current spread and thus activates overlapping neural populations with the adjacent electrodes. The spatial selectivity of electrical stimulation may be increased to reduce the channel interaction by using focused partial tripolar (pTP) stimulation mode (Figure 1b). In pTP mode, the current on a main electrode ELn is partially and equally returned to the adjacent apical electrode ELn-1 and basal electrode ELn+1, while the remaining current is returned to a remote extra-cochlear ground. Landsberger et al. (2012) found that excitation patterns were narrower with pTP-mode stimulation than with equally loud MP-mode stimulation, if the proportion of intra-cochlear return current (i.e., the compensation coefficient σ) was ≥ 0.5.
Figure 1:
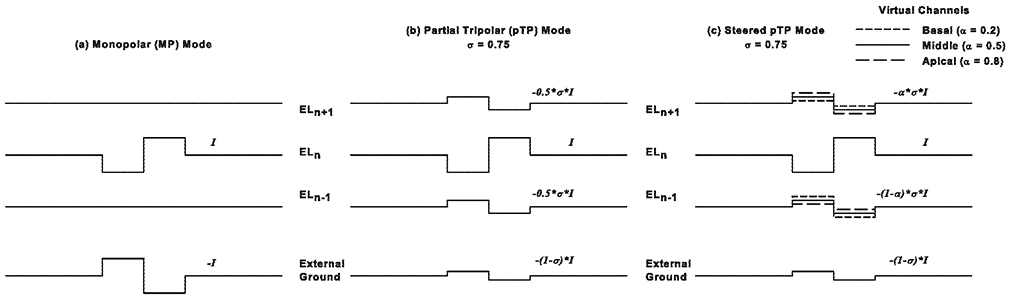
Biphasic current pulses on a main electrode ELn (the second line from the top), the adjacent basal electrode ELn+1 (the top line), the adjacent apical electrode ELn-1 (the third line from the top), and the external ground (the bottom line) for monopolar (MP; panel a), partial tripolar (pTP; panel b), and steered pTP modes (panel c). The MP mode returns all the current to the external ground. The pTP mode and steered pTP mode return part of the current (e.g., σ = 0.75) to the basal and apical electrodes. The middle virtual channel (VC; solid lines in panel c) is the same as the pTP mode and returns an equal amount of current to the basal and apical electrodes (i.e., α = 0.5). The basal VC (short-dashed lines in panel c) returns less current to the basal electrode than to the apical electrode (e.g., α = 0.2), while the apical VC (long-dashed lines) returns more current to the basal electrode than to the apical electrode (e.g., α = 0.8).
Experimental pTP- and MP-mode CI processing strategies matched in the number of main electrodes and pulse rate have been compared and the results have been mixed. Berenstein et al. (2008) found that spectral ripple discrimination (a measure of spectral resolution) was significantly better with a pTP strategy than with a MP strategy in CI users with σ = 0.75 but not in those with σ = 0.25. Word recognition scores were not separately analyzed for the two subject groups and did not significantly differ between the two strategies. Srinivasan et al. (2013) used σ = 0.75 and found that a pTP strategy produced significantly better sentence recognition in noise than a MP strategy. However, when Bierer and Litvak (2016) and Arenberg et al. (2018) used σ values ≥ 0.75, they did not find significantly better spondee recognition with a pTP strategy than with a MP strategy. A dynamic-focusing pTP strategy with more focusing (σ = 0.8) at the threshold and less focusing (σ = 0.5) at the most comfortable level offers a tradeoff between current focusing and power consumption, and may or may not produce better speech recognition in noise than a MP strategy (Arenberg et al., 2018; de Jong et al., 2019). When compared to the clinical strategy, the use of flanking electrodes in the experimental pTP strategy may increase the spatial selectivity, but it also reduces the total number of physical main electrodes that can be used. For example, the most apical and most basal main electrodes cannot be used, potentially decreasing spectral resolution.
Current steering may provide more spectral details to CI users by creating virtual channels (VCs) in addition to physical electrodes. MP-mode VCs (MPVCs) stimulate two adjacent main electrodes with current levels varied to steer the excitation centroid to different places between the electrodes. The clinical strategy HiRes120 or Fidelity120 of Advanced Bionics (Valencia, CA) uses MPVCs but did not always have better speech recognition than the HiRes strategy without current steering (e.g., Berenstein et al., 2008; Brendel et al., 2008). The benefit of MPVCs may be limited by the broad current spread of MP stimulation. To reduce VC interactions, Landsberger and Srinivasan (2009) used two flanking electrodes next to the two main electrodes to return an equal proportion of current and thus narrow the excitation pattern of current steering. The four-electrode quadrupolar VCs (QPVCs) provide better VC discrimination than MPVCs, but may elicit non-monotonic pitch changes across the electrodes. Virtual triples (VTPs; Padilla et al., 2017) with a six-electrode configuration vary the current levels of two main electrodes stimulated in spanned pTP mode (Luo and Wu, 2016) to elicit monotonic pitch changes across the electrodes. By returning different proportions of current to the two flanking electrodes of QPVCs, dynamically compensated VCs (DC-VCs; Nogueira et al., 2017) may reduce power consumption without affecting pitch sensitivity. However, QPVCs, VTPs, and DC-VCs have yet to be evaluated in a speech processing strategy.
Wu and Luo (2013) used the relatively simple three-electrode pTP configuration to combine current focusing and steering. pTP-mode current steering (Figure 1c) varies the proportions of return current on the two flanking electrodes to steer the excitation centroid around the main electrode. The proportion of basal return current or the steering coefficient α varies from 0 to 1 and is 0.5 for standard pTP mode. Wu and Luo (2016, 2013) found that higher α values (e.g., the long-dashed lines in Figure 1c) reduced the basal spread of excitation while increasing the apical spread and the resulted apical shift of excitation centroid lowered the perceived pitch. Also, an α range of 0.4-0.6 on each main electrode may elicit monotonic pitch changes across the electrodes with minimum risk of pitch reversals in more sensitive CI users. However, less sensitive CI users may need a larger α range (e.g., 0.2-0.8) to reliably perceive the pitch changes. With more spectral details, focused VCs created by pTP-mode current steering may improve speech recognition with CIs. To test the hypothesis, four experimental strategies different only in stimulation mode (MP, pTP, pTPsteering0.4-0.6, and pTPsteering0.2-0.8) were acutely tested with a clinical hearing in noise test in this study. Loudness balance and pitch ranking of focused VCs in pTPsteering strategies with the two α ranges were checked.
2. Methods
2.1. Subjects
Subjects were a convenient sample of four male and six female post-lingually deafened adult users of the Advanced Bionics HiRes90K implant with the HiFocus1J lateral-wall electrode array that support pTP stimulation. Current focusing may be more effective in reducing the current spread with the lateral-wall electrode array than with the perimodiolar electrode array, due to the stronger interaction between electrical fields of the main and flanking electrodes (Kalkman et al., 2015; Litvak et al., 2007). Table 1 lists the subject demographics. The clinical strategies HiRes and HiRes120 with sequential or paired stimulation of frequency channels were used by subjects in daily life. Table 1 also lists the stimulation parameters and speech reception threshold (SRT) for the clinical strategy. The SRT measurement is described in Section 2.3. All subjects were tested with a single CI of their own with no hearing aid or CI in the non-tested ear. This study was approved by the local Institutional Review Board. All subjects provided informed consent.
Table 1:
Subject demographics and information of the clinical and experimental strategies.
| Age (years) |
Etiology | Years with CI |
Clinical strategy | Experimental strategies | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Strategy | Main ELs used |
Pulse phase duration (μs) |
Pulse rate (pps) |
SRT (dB) |
Main ELs used |
Pulse phase duration (μs) |
Pulse rate (pps) |
σ used |
||||
| S1 | 65 | Unknown | 6 | HiRes120-S | 1-14 | 18 | 3712 | 8.8 | 2-13 | 140 | 297 | 0.75 |
| S2 | 25 | Genetic | 2 | HiRes120-S | 1-16 | 26 | 2560 | 4.0 | 2-14 | 140 | 275 | 0.625 |
| S3 | 86 | Sudden HL | 6 | HiRes120-P | 1-16 | 18 | 3712 | 11.0 | 2-15 | 140 | 255 | 0.625 |
| S4 | 68 | Hereditary | 9 | HiRes-P | 1-16 | 25 | 2486 | 16.0 | 2-15 | 140 | 255 | 0.75 |
| S5 | 55 | Unknown | 8 | HiRes120-P | 1-15 | 20 | 3228 | 10.2 | 2-13 | 140 | 297 | 0.625 |
| S6 | 56 | Unknown | 8 | HiRes120-S | 1-16 | 49 | 1350 | 10.0 | 2-15 | 140 | 255 | 0.625 |
| S7 | 67 | Unknown | 3 | HiRes120-P | 1-13 | 18 | 3712 | 17.0 | 2-13 | 140 | 297 | 0.75 |
| S8 | 61 | AN Loss | 13 | HiRes120-S | 1-16 | 24 | 2750 | 12.7 | 2-15 | 140 | 255 | 0.75 |
| S9 | 66 | Osteoporosis | 5 | HiRes-S | 1-16 | 33 | 2007 | 15.9 | 2-15 | 140 | 255 | 0.75 |
| S10 | 73 | Unknown | 10 | HiRes-S | 1-14 | 18 | 3712 | 11.0 | 2-13 | 140 | 297 | 0.625 |
CI, cochlear implant; EL, electrode; pps, pulses per second; SRT, speech reception threshold; S, sequential stimulation; P, paired stimulation; HL, hearing loss; AN, auditory nerve.
2.2. Experimental strategies
Four experimental strategies were created on a research Harmony processor using the Bionic Ear Programming System Plus (BEPS+; Advanced Bionics, Valencia, CA) and the template of clinical strategy HiRes120 with sequential stimulation. The MP and pTP strategies stimulated each main electrode in MP and pTP mode, respectively, to represent a frequency channel without current steering. The two pTPsteering strategies stimulated each main electrode in steered pTP mode to encode the spectral peak in each frequency channel. Based on Wu and Luo (2013), a higher spectral peak frequency increased the apical while decreasing the basal return current to stimulate a more basal place. In the pTPsteering0.4-0.6 strategy, the steering coefficient α had a range of 0.4-0.6 for all the main electrodes except the most apical and basal ones. In the pTPsteering0.2-0.8 strategy, α had a larger range of 0.2-0.8 for all the main electrodes except the most apical and basal ones. Both pTPsteering strategies expanded the α range apically for the most apical main electrode (0.4-1 and 0.2-1 in the pTPsteering0.4-0.6 and pTPsteering0.2-0.8 strategies, respectively), because there was no apical main electrode for pitch overlap. Similarly, the α range was expanded basally for the most basal main electrode (0-0.6 and 0-0.8 in the pTPsteering0.4-0.6 and pTPsteering0.2-0.8 strategies, respectively).
The experimental strategies used the same main electrodes, pulse phase duration, and pulse rate. As listed in Table 1, the most apical and basal main electrodes in the clinical strategy were not used in the experimental strategies for most subjects, due to the lack of apical or basal flanking electrode for pTP stimulation. S7 used the least number of main electrodes in the clinical strategy among all subjects. The most basal main electrode in his clinical strategy did not elicit abnormal sensations or require a current level above the compliance limit when stimulated in pTP mode and was thus used in his experimental strategies. For S2 and S5, the second most basal main electrode in the clinical strategy (in addition to the most basal one) was also not used in the experimental strategies, due to a tinkling sensation and a required current level above the compliance limit, respectively. As in Srinivasan et al. (2013), a 140-μs pulse phase duration (longer than that in the clinical strategy) was used in the experimental strategies to help obtain full loudness growth within the compliance limit for pTP stimulation (see below). The longer pulse phase duration also led to a lower pulse rate in the experimental strategies than in the clinical strategy. The default overall input frequency range of BEPS+ (306-8054 Hz) was similar to that in the clinical strategy and was automatically allocated to the various main electrodes in each experimental strategy.
The fitting procedures for the experimental strategies were similar to that used in clinic. Loudness growth with gradually increasing current levels was measured using the clinical loudness scale of Advanced Bionics. The compensation coefficient σ started with 0.75. Using σ = 0.75, the most comfortable level (MCL) was reached with current levels within the compliance limit on each main electrode for S1, S4, S7, S8, and S9. However, for the other subjects, such full loudness growth within the compliance limit was only achieved when σ was reduced to 0.625. Once determined, the same σ was used for both the pTP and pTPsteering strategies. For each experimental strategy, all the used main electrodes were loudness balanced at MCL. The MCLs of the most apical and basal VCs with the highest and lowest α were also adjusted so that they were equally loud to the middle VC with α = 0.5 on each main electrode of the pTPsteering strategies. The MCLs of the three loudness-balanced VCs were linearly interpolated to estimate those of the other VCs on the same main electrode. The three loudness-balanced VCs were ranked in pitch to check potential pitch reversals. The task was to indicate which of the three sequentially stimulated VCs had the highest pitch and which had the lowest pitch. Subject responses showed that pitch decreased or remained similar from the most basal VC to the middle VC and then to the most apical VC without pitch reversals, consistent with the results of Wu and Luo (2013). Finally, in speech mode, MCLs were adjusted for all the main electrodes to equalize the loudness of experimental and clinical strategies, and for individual main electrodes to refine the sound quality.
2.3. Performance evaluation
Sentence recognition in noise was tested in a sound booth with a loudspeaker. The experimental strategies were tested in random order for each subject. Before being tested with an experimental strategy, the subject was given short-term adaptation to the strategy by listening to an audio book with and without captions for 10 minutes each. SRTs were measured using the Hearing in Noise Test (HINT; Nilsson et al., 1994) in a 10-talker babble noise. Two lists of 20 sentences were randomly selected without replacement to obtain two measures of SRT for each strategy. A one-down/one-up adaptive procedure was used to find the signal-to-noise ratio (SNR) with 50% correct keyword recognition. In each trial, a sentence was randomly selected from the list without replacement and was normalized to a root-mean-square level of 65 dBA. Starting at 10 dB, the SNR of the first sentence was increased in 2-dB steps until it was correctly repeated with ≥ 50% of the keywords. Then, the adaptive procedure began. The SNR was reduced or increased by 2 dB after a sentence was correctly repeated with ≥ or < 50% of the keywords, respectively. The procedure ended after ten reversals or 20 sentences and the SRT was the mean SNR over the last six reversals.
3. Results
The two measures of SRT using different sentence lists did not significantly differ from each other (paired t-tests: t9 = −0.06, p = 0.95 for MP, t9 = 0.78, p = 0.46 for pTP, t9 = 0.10, p = 0.92 for pTPsteering0.4-0.6, and t9 = 1.64, p = 0.14 for pTPsteering0.2-0.8), showing no learning effect from test to retest. Among the subjects, the SRT difference from test to retest ranged from −2.7 to 4.0 dB (mean: 0.08 dB) for MP, from −3.5 to 3.3 dB (mean: −0.75 dB) for pTP, from −2.7 to 2.7 dB (mean: −0.09 dB) for pTPsteering0.4-0.6, and from −2.7 to 0.3 dB (mean: −1.07 dB) for pTPsteering0.2-0.8. The two SRT measures for each strategy were averaged for further analyses.
Figure 2A shows the SRTs of individual subjects for each experimental strategy. The SRTs were normally distributed and had equal variance. A mixed-design analysis of variance (ANOVA) showed that both the within-subject factor of strategy (F3,24 = 4.75, p = 0.01) and the between-subject factor of σ (F1,8 = 16.16, p = 0.004) significantly affected the SRTs. The two factors had no interaction (F3,24 = 1.92, p = 0.15). Post-hoc Bonferroni t-tests showed that compared to the MP strategy, both the pTPsteering0.4-0.6 (p = 0.01) and pTPsteering0.2-0.8 strategies (p = 0.04) produced significantly better or lower SRTs, while the pTP strategy did not (p = 0.55). The pTP, pTPsteering0.4-0.6, and pTPsteering0.2-0.8 strategies produced similar SRTs (all p = 1.00). The lack of interaction between strategy and σ suggests that the effect of strategy on SRTs was similar for subjects with the two σ values. As shown in Figure 2A, subjects with σ = 0.625 had significantly better SRTs than those with σ = 0.75 (p = 0.004) for all the experimental strategies including the non-focused MP strategy. This group difference was thus not due to their different σ values per se. Instead, subjects with σ = 0.625 were better CI users than those with σ = 0.75, as indicated by their SRTs with the clinical strategy in Table 1. Note that σ was selected for each subject based on their loudness growth during the fitting procedure, but not pre-determined by any demographic factor or clinical performance. The two subject groups did not differ in the age at testing (t-test: t8 = 0.62, p = 0.55) or duration of CI use (t-test: t8 = 0.18, p = 0.86). The SRT with each experimental strategy was not correlated with the age at testing or duration of CI use across all subjects (all p > 0.05).
Figure 2:
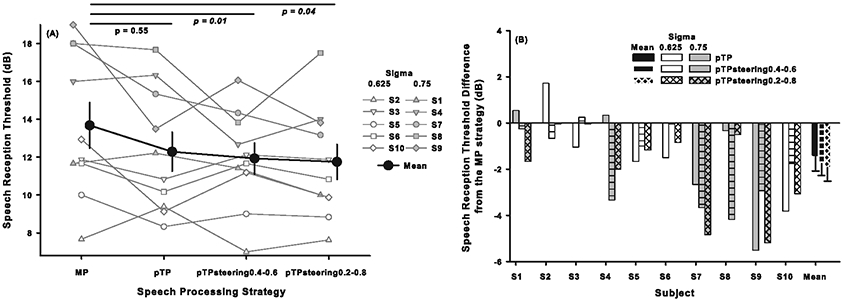
(A) Speech reception thresholds (SRTs) for 50% correct keyword recognition in the Hearing in Noise Test for each experimental strategy. Black circles represent the mean while error bars represent the standard error across all subjects. White and gray symbols show the individual results with σ = 0.625 and 0.75, respectively. p values of post-hoc Bonferroni t-tests between the MP strategy and the pTP, pTPsteering0.4-0.6, and pTPsteering0.2-0.8 strategies are shown at the top, with italic p values indicating significant differences in SRT. (B) SRT differences between the MP strategy and the pTP (blank bars), pTPsteering0.4-0.6 (bars with horizontal lines), and pTPsteering0.2-0.8 strategies (bars with crossed lines). Black bars represent the mean while error bars show the standard error across all subjects. White and gray bars show the individual results with σ = 0.625 and 0.75, respectively. A few bars are hardly visible because the related SRT differences were close to 0 dB. Negative values indicate better pTP or pTPsteering results than MP results.
To normalize for the individual variability in baseline performance with the MP strategy and to quantify the benefit of current focusing and steering, the SRT with MP strategy was subtracted from those with the pTP, pTPsteering0.4-0.6, and pTPsteering0.2-0.8 strategies for each subject, as shown in Figure 2B. After verifying the normal distribution and equal variance of SRT differences, a mixed-design ANOVA showed that the SRT differences were significantly affected by the between-subject factor of σ (F1,8 = 4.82, p = 0.04), but not by the within-subject factor of strategy (F2,16 = 0.47, p = 0.64). The two factors had no interaction (F2,16 = 1.67, p = 0.22). Post-hoc Bonferroni t-tests showed that subjects with σ = 0.625 had significantly less SRT improvements (i.e., decreases) from the MP to the pTP and pTPsteering strategies than those with σ = 0.75 (p = 0.04). It is difficult to disentangle whether this group difference was due to the different σ values or baseline MP performance since the two factors co-varied with each other. The SRT differences from the MP to the pTPsteering0.4-0.6 and pTPsteering0.2-0.8 (but not pTP) strategies were significantly correlated with the SRT with MP strategy across all subjects (r = −0.85, p = 0.002 for pTPsteering0.4-0.6, r = −0.67, p = 0.03 for pTPsteering0.2-0.8, and r = −0.52, p = 0.12 for pTP). Subjects with better SRTs with the MP strategy received less benefit from steered pTP mode.
4. Discussion
Although the idea of combining current focusing and steering with CIs is not new (e.g., Landsberger and Srinivasan, 2009; Nogueira et al., 2017; Padilla et al., 2017), this exploratory study is the first to implement focused VCs in speech processing strategies and test their effect on speech recognition performance in an acute trial. Steered pTP mode was used with two current steering ranges. Compared to the MP strategy without current focusing or steering, the pTPsteering strategies with combined current focusing and steering produced significantly better SRTs, while the pTP strategy with only current focusing did not. However, it is difficult to know the relative effects of current focusing and steering in the pTPsteering strategies. Subjects with σ = 0.625 showed significantly better SRTs with the MP strategy and less SRT improvements from the MP to the pTPsteering strategies than those with σ = 0.75. Because all the experimental strategies used the same low pulse rate with limited temporal cues, the SRT improvements with the pTPsteering strategies were likely due to more spectral cues. Future studies should use spectral ripple discrimination to assess the spectral resolution of different experimental strategies (e.g., Berenstein et al., 2008). It is worth noting that due to the small number of subjects, the present results should be interpreted with caution.
Pitch ranking of VCs on each main electrode during the fitting of pTPsteering strategies was to address the concern of pitch reversals that may arise from salient side lobes around the flanking electrodes with large proportions of return current, as observed in phantom electrodes (PEs; Saoji and Litvak, 2010). Although pitch ranking was only roughly tested for the most apical, middle, and most basal VCs due to the time limitation, no pitch reversals were found in this study. PEs sent all the intra-cochlear return current σ×I to one flanking electrode, while steered pTP mode split the return current by ratios of α and 1-α between two flanking electrodes, which may reduce the risk of pitch reversals. Considering the similar SRTs with both pTPsteering strategies, the smaller α range (0.4-0.6) may be preferred because it did not result in a large proportion of return current per flanking electrode.
The effects of σ on the SRTs with pTP and pTPsteering strategies and on the SRT improvements with current focusing and steering were confounded by the different SRTs with MP strategy of the two subject groups with different σ values. Subjects with σ = 0.625 had better MP performance and thus better pTP and pTPsteering performance than those with σ = 0.75, although the higher σ may further narrow the excitation patterns (Landsberger et al., 2012). Both the better MP performance and lower σ of subjects with σ = 0.625 may have led to smaller SRT improvements with the pTPsteering strategies, similar to the findings with a pTP strategy in Bierer and Litvak (2016). A lower σ may be needed for a poorer electrode-neuron interface with longer electrode-neuron distance, less neural survival, and shallower loudness growth, which may explain the less benefit from pTP-mode current steering but not the better MP performance of subjects with σ = 0.625. Also, age at testing, duration of CI use, and strategy parameters did not account for the group difference in SRT with the baseline MP strategy. Duration of deafness may be an important factor, but was not collected because it was difficult for our subjects to recall exactly when their deafness became severe.
This study did not replicate the results of Srinivasan et al. (2013) that SRTs were significantly better with a pTP strategy than with a MP strategy, even though both studies used the HINT test and matched the strategies as closely as possible. The baseline MP performance and strategy parameters were also similar between the two studies. Half of our subjects used the same σ (0.75) as those in Srinivasan et al. (2013), while the other half used σ = 0.625. Although the effect of strategy on SRTs was similar for both subject groups in this study, those with σ = 0.625 did have less SRT improvements with the pTP strategy. The different results of the two studies were perhaps due to the low sample size in both studies and further suggest that the benefit of current focusing varies across CI users, possibly due to the variable electrode-neuron interface (e.g., Arenberg et al., 2018; Bierer and Litvak, 2016).
Compared to the clinical strategy, the MP strategy had significantly worse SRTs (paired t-test: p = 0.005), possibly because it used a lower pulse rate, less main electrodes, and no current steering. The impact of each factor is still unknown. Using the same pulse rate and main electrodes as the MP strategy but introducing current focusing and current steering, the pTP and pTPsteering strategies had comparable SRTs to the clinical strategy (paired t-tests: p > 0.89). This suggests that the poorer performance of MP strategy relative to the clinical strategy may be mainly due to the lack of current steering. To have better speech recognition than the clinical strategy, the pTP and pTPsteering strategies should optimize the pulse phase duration for a trade-off between pulse rate and current level, use paired rather than sequential stimulation of frequency channels to increase the pulse rate, and activate the main electrodes at both ends of the array in another mode (e.g., MP or bipolar). These strategies should then be tested in a take-home trial.
Acknowledgments
We are grateful to all subjects for their participation in this study. Research was supported in part by the NIH grant R21-DC-011844.
References
- Arenberg JG, Parkinson WS, Litvak L, Chen C, Kreft HA, Oxenham AJ, 2018. A dynamically focusing cochlear implant strategy can improve vowel identification in noise. Ear Hear. 39, 1136–1145. 10.1097/aud.0000000000000566 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berenstein CK, Mens LHM, Mulder JJS, Vanpoucke FJ, 2008. Current steering and current focusing in cochlear implants: comparison of monopolar, tripolar, and virtual channel electrode configurations. Ear Hear. 29, 250–260. 10.1097/AUD.0b013e3181645336 [DOI] [PubMed] [Google Scholar]
- Bierer JA, Litvak L, 2016. Reducing channel interaction through cochlear implant programming may improve speech perception: Current focusing and channel deactivation. Trends Hear. 20, 1–12. 10.1177/2331216516653389 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brendel M, Buechner A, Krueger B, Frohne-Buechner C, Lenarz T, 2008. Evaluation of the Harmony sound processor in combination with the speech coding strategy HiRes 120. Otol. Neurotol 29, 199–202. [DOI] [PubMed] [Google Scholar]
- de Jong MAM, Briaire JJ, van der Woude SFS, Frijns JHM, 2019. Dynamic current focusing for loudness encoding in cochlear implants: a take-home trial. Int. J. Audiol 58, 553–564. [DOI] [PubMed] [Google Scholar]
- Friesen LM, Shannon RV, Baskent D, Wang X, 2001. Speech recognition in noise as a function of the number of spectral channels: comparison of acoustic hearing and cochlear implants. J. Acoust. Soc. Am 110, 1150–1163. 10.1121/1.1381538 [DOI] [PubMed] [Google Scholar]
- Kalkman RK, Briaire JJ, Frijns JHM, 2015. Current focussing in cochlear implants: An analysis of neural recruitment in a computational model. Hear. Res 322, 89–98. [DOI] [PubMed] [Google Scholar]
- Landsberger DM, Padilla M, Srinivasan AG, 2012. Reducing current spread using current focusing in cochlear implant users. Hear. Res 284, 16–24. 10.1016/j.heares.2011.12.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Landsberger DM, Srinivasan AG, 2009. Virtual channel discrimination is improved by current focusing in cochlear implant recipients. Hear. Res 254, 34–41. 10.1016/j.heares.2009.04.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Litvak LM, Spahr AJ, Emadi G, 2007. Loudness growth observed under partially tripolar stimulation: model and data from cochlear implant listeners. J. Acoust. Soc. Am 122, 967–981. 10.1121/1.2749414 [DOI] [PubMed] [Google Scholar]
- Luo X, Wu CC, 2016. Symmetric electrode spanning narrows the excitation patterns of partial tripolar stimuli in cochlear implants. J. Assoc. Res. Otolaryngol 17, 609–619. 10.1007/s10162-016-0582-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nilsson M, Soli SD, Sullivan J, 1994. Development of the Hearing In Noise Test for the measurement of speech reception thresholds in quiet and in noise. J. Acoust. Soc. Am 95, 1085–1099. [DOI] [PubMed] [Google Scholar]
- Nogueira W, Litvak LM, Landsberger DM, Büchner A, 2017. Loudness and pitch perception using Dynamically Compensated Virtual Channels. Hear. Res 344, 223–234. 10.1016/j.heares.2016.11.017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Padilla M, Stupak N, Landsberger DM, 2017. Pitch ranking with different virtual channel configurations in electrical hearing. Hear. Res. 348, 54–62. 10.1016/j.heares.2017.02.013 [DOI] [PubMed] [Google Scholar]
- Saoji AA, Litvak LM, 2010. Use of “phantom electrode” technique to extend the range of pitches available through a cochlear implant. Ear Hear. 31, 693–701. 10.1097/AUD.0b013e31820407f7 [DOI] [PubMed] [Google Scholar]
- Srinivasan AG, Padilla M, Shannon RV, Landsberger DM, 2013. Improving speech perception in noise with current focusing in cochlear implant users. Hear. Res 299, 29–36. 10.1016/j.heares.2013.02.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wu C-C, Luo X, 2016. Excitation patterns of standard and steered partial tripolar stimuli in cochlear implants. J. Assoc. Res. Otolaryngol 17, 145–158. 10.1007/s10162-015-0549-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wu CC, Luo X, 2013. Current steering with partial tripolar stimulation mode in cochlear implants. J. Assoc. Res. Otolaryngol 14, 213–231. 10.1007/s10162-012-0366-8 [DOI] [PMC free article] [PubMed] [Google Scholar]