

Abstract
This study examined mothers’ perceptions of the positive impact of having a child with an intellectual disability. Trajectories of positive impact from 7 time points were developed using latent growth modeling and 2 predictors: culture (Anglo, Latino) and child disability status (intellectual disability, typical development). Data were from 219 mothers of children from age 3 to 9 years. Growth trajectories reflected a general decline in positive impact on Anglo mothers. On average, at age 3, Anglo mothers reported significantly lower initial values on positive impact when their children had an intellectual disability, but Latino mothers did not. Across all time points, Latino mothers had higher scores on the positive impact, regardless of whether they had a child with an intellectual disability or a typically developing child.
Keywords: Latino culture, family impact, intellectual disability, longitudinal models
For over half a century the field of intellectual disability (previously, ‟mental retardation”) was dominated by research attesting to the devastating effects of having a child with a cognitive or intellectual impairment. Studies reported that children with intellectual disability (ID) had an overwhelmingly negative impact on their families or, more specifically, on their mothers (Blacher & Baker, 2002; Farber, 1959; Grebler, 1952).
Fortunately, family research around the juncture of the 20th and 21st centuries broadened in scope to consider parenting children with disabilities in a more nuanced way that included a recognition of family benefits as well. Initial qualitative studies that asked parents about the positive aspects of living with a child with ID were enlightening and heuristic (Durand, 2011; Patterson et al., 1993). Researchers began to examine directly the positive impact of a child with disabilities on the family with a variety of measurement approaches (Baker, Blacher, & Olsson, 2005; Blacher & Baker, 2007; Dura-Vila, Dein, & Hodes, 2010; Hastings, Beck, & Hill, 2005; Helff & Glidden, 1998; Scallan, Senior, & Reilly, 2011; Trute, Benzies, Worthington, Reddon, & Moore, 2010). This focus on positivity drew from the broader psychological literature on positive perceptions as a coping mechanism, documented in some classic papers with regard to women’s health (Taylor, 1983; Taylor, Lerner, Sherman, Sage, & McDowell, 2003a, 2003b) and generalized adaptation (Folkman, 1997).
The present study examined the positive impact of child-rearing throughout early and middle childhood, using latent growth modeling across seven assessment points. We examined the extent to which the trajectories of positive perceptions related to the child’s disability status (intellectual disability or typical cognitive development) and to the mothers’ cultural background (Anglo or Latino, defined below).
Conceptualizations of Positive Impact
There are various ways to conceptualize positive impact, regardless of the specific disability of interest. We previously considered three perspectives that often get confused in the discourse, using intellectual disability as an example (Blacher & Baker, 2007). The first is the “low negative” view, where positive impact is inferred by the absence of negative impact. Thus, parents who have low scores on measures of, for example, risk (Olsson, Larsman, & Hwang, 2008), stress, or depression (Blacher and Baker, 2007; Meirsschaut, Roeyers, & Warreyn, 2010) would be seen as coping positively with the disability. A corollary of the “low negative” perspective is “high positive”, where positive impact of disability is inferred from indicators that parents are doing well in other spheres, on measures of domains such as well-being, social support, or coping (Lloyd and Hastings, 2009). In one study of 119 mothers of children with autism spectrum disorders across all ages of childhood (2 to 18 years), positive impact was inferred from high positive affect, life satisfaction, and psychological well-being (Ekas, Lickenbrock, & Whitman, 2010). In another, positive impact was inferred by a higher sense of coherence (Olsson, Larsman, & Hwang, 2008). The obvious limitations of this first low negative or high positive perspective is that the positive impact of disability is not directly addressed and there is no comparison group.
The second conceptualization is the common benefits view, whereby parents of children with a disability report the same types of positive child-rearing experiences as parents of typically developing children. Examples of this conceptualization are less common, as it requires the inclusion of a control group of typically developing (TD) children and the use of measures of positive impact appropriate to mothers of both typically developing children and children with an intellectual disability (Bostrom et al., 2011) or autism (Ekas et al., 2010; Lickenbrock, Ekas, & Whiteman, 2011; Meirsschaut, Roeyers, & Warreyn, 2010; Phelps, McCammon, Wuensch, & Goldren, 2009).
The third perspective is the special benefits view, where parents of children with ID report unique benefits not experienced by parents of TD children. Studies stemming from this view often involve only a disability group, with interviews of parents (usually mothers) focused on benefits the child brings to the family (Rapanaro, Bartu, & Lee, 2008). Scallan et al. (2011) interviewed parents of young adults with ID (specifically, Williams syndrome) to determine, among other things, positive impact on the family. Themes that emerged included positive impact on siblings, joy brought by the child with ID, a sense of family closeness, a focus on the important things in life, and friendships with other parents in a similar situation.
Finally, findings from some studies suggest that positive and negative views of parenting impact in families may coexist and be relatively independent from one another (Blacher & McIntyre, 2006). In one study, maternal positive perceptions of the child with ID were not related to the other variables of interest in the study, which included maternal stress, anxiety, and depression, as well as child behavior problems (Lloyd and Hastings, 2008). The coexistence of positive and negative dimensions can occur when parents report high stress, but also positive ways to counteract it, such as enrichment through religion or spirituality (Phelps et al., 2009). There is also evidence that parents who “accentuate the positive” had lower negative cognitive appraisal of family impact (Trute, Benzies, Worthington, Reddon, & Moore, 2010).
Culture and Positive Perceptions
We are particularly interested in the positive perceptions of child-rearing held by two dominant cultural groups: Anglos and Latinos. Nearly all research on family impact of disability has involved white, non-Hispanic families. In Southern California, where this study took place, this group is often referred to as Anglos, and Hispanic families as Latinos. Latinos compose the fastest growing minority; they will be the majority ethnic group in California by 2015 (U.S. Census, 2011). Not surprisingly, some of the family issues addressed by disability researchers appear to be quite different across cultural groups. We use the term “culture,” even though the variable typically used to differentiate groups is ethnicity, because the growing literature on Latino families suggests some uniformity in beliefs, values, and practices. Among these are familism, particularly attitudinal familism, conceptualized as family closeness, concern for the overall well-being of the family, and a strong endorsement of family responsibility (Blacher, Shapiro, Lopez, Diaz, & Fusco, 1997; Cauce & Domenich-Rodríguez, 2002; Sabogal, Marín, Otero-Sabogal, Marín, & Perez-Stable, 1987).
In earlier studies, we examined positive impact of disability within a cultural context (Blacher & Baker, 2007; Blacher & McIntyre, 2006). We administered to parents the Family Impact Questionnaire (Donenberg & Baker, 1993), which has positive and negative scales summarizing how the child impacts their parenting, their relationships, and the family overall. In one study of families of young adults, Latino and Anglo parents reported similar perceptions of the negative impact of their young adult offspring with severe ID. Latino mothers reported higher scores on positive impact than did Anglo mothers (Blacher & McIntyre, 2006). In a second study of parents of children with developmental delays and a TD control group of children aged 3, 4, and 5 years, the story was more complex. In the TD group, Latino and Anglo mothers reported the same level of positive impact across time. However, there was a significant interaction between the culture and the delay group. Latino mothers of delayed children reported significantly higher positive impact (than Latino mothers in the TD group), whereas Anglo mothers of delayed children reported significantly lower positive impact (than Anglo mothers in the TD group). The more positive views of Latino mothers in the presence of child disability are intriguing and certainly require more examination (Blacher & Baker, 2007).
The Present Study
Primary limitations of nearly all of the studies that have explored the positive impact of a child with a disability are that measures were obtained at only one time point and that samples tend to range widely in age and developmental stage. Two exceptions involved a two-wave analysis (Lloyd & Hastings, 2008) and the three-wave analysis considered above (Blacher and Baker, 2007). In the present study, we assessed maternal perceptions of positive child impact across seven assessments for children ages 3 through 9 years. We compared two groups of families, one with Latino mothers and the other with Anglo mothers, and we used a measure of positive perceptions that was applicable to all families. Consistent with the earlier reported findings, which were not analyzed using time-sensitive models (Blacher & Baker, 2007), we anticipated finding initial differences by ethnic or cultural group, suggesting that the perceptions of the Latino mothers would represent the low negative view. However, we advanced no hypothesis about the trajectory from early through middle childhood. There were three primary research questions. First, do mothers’ perceptions of the positive impact of child-rearing change across early and middle childhood? Second, if we take culture into account, do we see differences in trajectories? Third, are differences in trajectories predicted by the disability status of the child?
Method
Participants
Participants were 219 families, recruited to take part in a longitudinal study of young children from ages 3 to 9 years. There were 168 Anglo and 51 Latino families. The goal of the longitudinal study was to examine family, school, and child contributions to the emergence of behavior disorders in children with and without intellectual disability. Participants were drawn from southern California and central Pennsylvania. The present sample comprised all families for whom data were available on the primary measures across children ages 3, 4, 5, 6, 7, 8, and 9; this constitutes 84% of the originally recruited sample. There were no statistically significant differences between participants included in the present study and participants excluded from the present study on child (mean age at testing, gender, mean Bayley scores) or mother/family (martial status, age, employment, education, income) characteristics.
General selection criteria were that children had to be between 30 and 40 months of age and not diagnosed with autism. Children in the typically developing (TD) group (N = 107) were recruited at age 3 from preschools and day care programs. TD children were excluded if they had any type of disability or were born prematurely. Children in the developmental disability group (N = 112) were recruited at age 3 through community agencies that provided services for people with developmental disabilities. Children who could not walk or had autism or an IQ below 40 were excluded from the ID group at initial assessment. Although developmental disability or risk status was determined at the beginning of the study, we refer to this group as having intellectual disability (ID), because there were subsequent assessments at ages 5 and 9, using a measure of both cognitive development and adaptive behavior. The chi-square was used to test if there was a difference between the frequency of 0s (typically developing) and 1s (intellectual disability) in the 3- and 5-year assessments. No statistically significant difference was found between age 3 and age 5, chi-square (1) = 2.01, p > .05, and therefore, disability status at age 3 was chosen as the predictor.
Table 1 shows demographic characteristics by ethnic status. Child age at initial intake averaged 35.1 months (SD = 2.9). At age 3, most children in the delayed group had not received a specific diagnosis; when there was one, the most frequent was Down syndrome or cerebral palsy. Most mothers (84%) were married because recruitment had initially focused on intact families. Mothers averaged about 15 years of school, and 49% of families had an annual income of $50,000 or more in 1999–2001 dollars. In the present study, 96.3% of the mothers were the target child’s biological mother.
Table 1.
Child and Mother Demographic Characteristics by Ethnic Status
| Variable | Anglo (n = 168) M (%) |
Latino (n = 51) M (%) |
t/χ2a |
|---|---|---|---|
| Child | |||
| Mean age at testing in months (SD) | 34.92 (2.80) | 35.57 (3.14) | t = −1.35 |
| Gender (% boys) | 59.1 | 57.1 | χ2 = .06 |
| Siblings (% yes) | 72.7 | 77.6 | χ2 = .45 |
| Mean BSID-II: MDI | 87.16 (25.43) | 74.57 (23.41) | t = 3.07** |
| Mother and family | |||
| Marital status (% married) | 87.0 | 75.5 | χ2 = 3.70† |
| Mean mother age (years) | 34.06 (5.97) | 31.43 (5.04) | t = 2.78* |
| Employment (% employed) | 57.1 | 59.2 | χ2 = .06 |
| Education (% bachelor of arts or higher) | 52.6 | 22.4 | χ2 = 13.63*** |
| Family income (% 50k or higher) | 52.9 | 36.7 | χ2 = 3.90* |
Note. Breakdowns of n are Anglo: 90 typically developing children, 78 children with a developmental disability; Latino: 17 typically developing children, 34 children with a developmental disability. BSID-II = Bayley Scales of Infant Development II; MDI = Mental Developmental Index. ats are used when standard deviations are reported.
p < .10.
p < .05.
p < .01.
p < .001.
The two groups did not differ on the child attributes shown in Table 1, except on the Bayley II scores. These differences in Bayley scores (which are not as robust as a more traditional IQ score) suggest an educational gap between Anglo and Latino children even at 3 years of age, at least in this sample. However, as shown, the scores were not related to the outcome variable of positive impact. On mother characteristics, the mean age was higher for Anglo than Latino mothers. On socioeconomic status variables, more Anglo mothers had a college degree or higher than Latino mothers, and more Anglo families had an annual income of $50,000 or higher than Latino families.
A covariate is used when it is related to the dependent variables of interest (Lomax, 2007). In the present study, mothers’ age and education as well as family income were not used as covariates because these variables did not relate to the observed time points of positive impact for Anglo or Latino mothers. For Anglo mothers, the average correlation between the observed time points of positive impact and age was −.01; between the observed time points of positive impact and grade was −.05; and between the observed time points of positive impact and income was .04. For Latino mothers, the average correlation between the observed time points of positive impact and age was .01; between the observed time points of positive impact and grade was .04; and between the observed time points of positive impact and income was −.15. For both Anglo and Latino mothers, when age, education, and income were entered into the conditional model, none of these covariates had a statistically significant effect on the Level or Shape factors.
Procedures
The institutional review boards of the three participating universities (Pennsylvania State University, University of California, Los Angeles, and University of California, Riverside) approved all procedures. The data used in the present study were obtained in three ways: home assessments, clinic assessments, and questionnaire packets. Prior to the initial assessment, parents completed a telephone interview with staff and received an informed consent. At the initial home assessment, two research assistants visited the family to review procedures and administer the Bayley II to the child. The Family Impact Questionnaire (FIQ) was part of a questionnaire packet completed by parents at each assessment session at the university child study centers.
Measures
Bayley Scales of Infant Development Second Edition (Bayley, 1993).
The Bayley Scales of Infant Development II (BSID-II) is a widely used measure of mental and motor development in children aged 1 to 42 months. The 36-month BSID-II was administered in the home with the mother present. Only the mental development items were administered. The Mental Development Index (MDI) is normed with a mean of 100 and a standard deviation of 15. Bayley reported high short-term test–retest reliability (r = .91) for the MDI. With children aged 36 to 42 months, the MDI correlated well with the Full Scale IQ of the Wechsler Preschool and Primary Scale of Intelligence—Revised (WPPSI-R), r = .73. The BSID-II was used to place each child into either the typically developing (TD) or delayed group at the start of the study.
Family Impact Questionnaire (Donenberg & Baker, 1993).
The FIQ contains 50 items assessing parents’ perception of the child’s impact on the family compared to the impact of other children. Parents respond on a 4-point scale ranging from not at all to very much. There are five subscales measuring perceptions of the child’s negative impact on feelings about parenting (9 items); social relationships (11 items); finances (7 items); and if applicable, siblings (9 items); and marriage (9 items). The sixth subscale measures perceptions of the child’s impact on positive feelings about parenting (7 items). A sample item is (compared with children and parents with children the same age as my child): “My child makes me feel more confident as a parent.” In the present study, we used the mothers’ positive impact composite. Cronbach’s alpha for age 3 was .80; for age 4 was .86; for age 5 was .86; for age 6 was .86; for age 7 was .86; for age 8 was .87; and for age 9 was .88.
Analysis and Results
The proposed longitudinal so-called latent growth or latent curve model was fit to the data using Mplus with full information maximum likelihood (FIML) parameter estimation to handle the presence of missing data (Arbuckle, 1996; Muthén & Muthen, 2006). To ensure adequacy of sample size, power, and parameter estimate precision necessary for conducting the various analyses presented in this study, the procedures outlined in Muthén and Muthén (2002) and Marcoulides and Saunders (2006) were followed. Results indicated satisfactory evidence with respect to the stability of obtained parameter estimates and sufficient levels of power (well above .80, considered by most researchers as acceptable). The descriptive statistics for the total sample listed, respectively, for the Anglo and Latino mothers on the observed variables used in the study are presented in Table 2.
Table 2.
Descriptive Statistics for Anglo Mothers’ Positive Impact and Latino Mothers’ Positive Impact
| Variables | M | SD |
|---|---|---|
| Anglo mothers | ||
| Y1 = positive impact at age 3 | 15.29 | 4.62 |
| Y2 = positive impact at age 4 | 15.41 | 4.92 |
| Y3 = positive impact at age 5 | 15.17 | 5.00 |
| Y4 = positive impact at age 6 | 14.70 | 5.15 |
| Y5 = positive impact at age 7 | 14.42 | 5.49 |
| Y6 = positive impact at age 8 | 14.60 | 5.50 |
| Y7 = positive impact at age 9 | 14.73 | 5.35 |
| Latino mothers | ||
| Y1 = positive impact at age 3 | 17.43 | 4.45 |
| Y2 = positive impact at age 4 | 16.68 | 4.70 |
| Y3 = positive impact at age 5 | 16.47 | 5.13 |
| Y4 = positive impact at age 6 | 16.32 | 4.87 |
| Y5 = positive impact at age 7 | 17.23 | 4.74 |
| Y6 = positive impact at age 8 | 16.71 | 5.27 |
| Y7 = positive impact at age 9 | 16.35 | 4.60 |
Do Mothers’ Perceptions of the Positive Impact of Child-Rearing Change Across Early and Middle Childhood?
Figure 1 depicts the unconditional model for the seven repeated measurements on the Anglo mothers’ and the Latino mothers’ positive impact. As can be seen by examining the model displayed in Figure 1, each observed Y variable loads on two specific factors. The factor designated as F1 refers to the Level factor and that designated as F2 refers to the Shape factor (Raykov & Marcoulides, 2006). For both the Anglo and Latino groups considered in this study, each observed variable corresponds to Y1 = mothers’ positive impact at age 3; Y2 = mothers’ positive impact at age 4; Y3 = mothers’ positive impact at age 5; Y4 = mothers’ positive impact at age 6; Y5 = mothers’ positive impact at age 7; Y6 = mothers’ positive impact at age 8; and Y7 = mothers’ positive impact at age 9, respectively.
Figure 1.
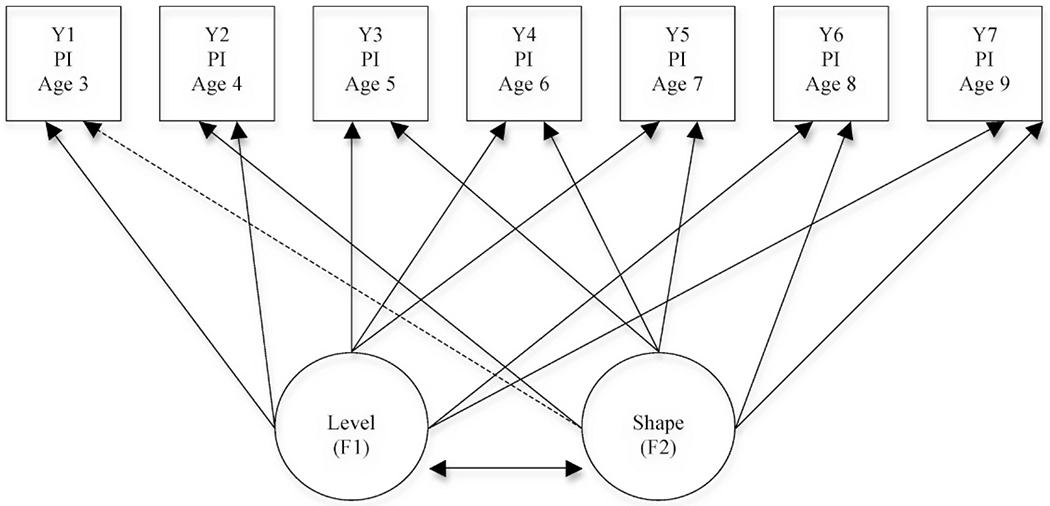
Unconditional model for positive impact (PI): Applicable to Anglo mothers and Latino mothers. Figure adapted from Blacher & Baker, 2007.
Although different approaches to the coding of time can be used in such longitudinal models (e.g., assuming an a priori specific linear trajectory in the so-called intercept-slope approach), we preferred to use the Level and Shape (LS) strategy, which does not a priori assume a particular trajectory shape but models the change process regardless of the actual trajectory encountered—whether it be linear, quadratic, cubic, and so forth (for more details, see Raykov & Marcoulides, 2006, 2008). The loadings of the assessment occasions on the first factor are all set to a value of 1 to ensure that it is interpreted as a baseline point. The loading of the first assessment occasion (i.e., the Anglo mothers’ positive impact at age 3 and Latino mothers’ positive impact at age 3 in each analyzed model, respectively) on the second factor (i.e., the Shape factor) is fixed to a value of 0 (as indicated by “0 =” in Table 3). In addition, the loading of the last assessment occasion on the Shape factor (i.e., the Anglo mothers’ positive impact at age 9 and Latino mothers’ positive impact at age 9 in each model, respectively) is fixed to a value of 1 (as indicated by “1 =” on Table 3). Fixing the loading of the first and last assessment occasion to 0 and 1, respectively, ensures that the Shape factor is interpreted as a change factor (i.e., reflecting the shape of the change process studied). Freeing the loadings of the remaining assessment occasions on the Shape factor ensures that they represent the change that occurs between the first and each of the later measurement occasions (Duncan, Duncan, Li, & Strycker, 1999; Duncan, Duncan, & Strycker, 2006; McArdle & Anderson, 1990).
Table 3.
Factor Loading Parameter Estimates, Standard Errors, and Critical t Ratios for Level and Shape Model
| Factor loadings | Estimate | Standard error | Critical ratio |
|---|---|---|---|
| Anglo mothers | |||
| Y1 = positive impact at age 3 | 0 = | ||
| Y2 = positive impact at age 4 | .10 | .16 | .62 |
| Y3 = positive impact at age 5 | .35* | .15 | 2.30 |
| Y4 = positive impact at age 6 | .76*** | .15 | 5.24 |
| Y5 = positive impact at age 7 | .93*** | .16 | 5.78 |
| Y6 = positive impact at age 8 | 1.21*** | .15 | 7.37 |
| Y7 = positive impact at age 9 | 1 = | ||
| Mean value on Level factor | 15.38 | .35 | 44.15*** |
| Mean value on Shape factor | − .83 | .34 | −2.41* |
| Latino mothers | |||
| Y1 = positive impact at age 3 | 0 = | ||
| Y2 = positive impact at age 4 | 1.15† | .62 | 1.85 |
| Y3 = positive impact at age 5 | 2.12* | .96 | 2.21 |
| Y4 = positive impact at age 6 | 2.13* | 1.08 | 1.97 |
| Y5 = positive impact at age 7 | 1.47* | .68 | 2.17 |
| Y6 = positive impact at age 8 | 1.83* | .83 | 2.22 |
| Y7 = positive impact at age 9 | 1 = | ||
| Mean value on Level factor | 17.27 | .65 | 26.44*** |
| Mean value on Shape factor | −.37 | .36 | −1.05 |
p < .10.
p < .05.
p < .01.
p < .001.
Because we posited an LS model to be tested, our initial interest is in the assessment of overall model fit. Once the overall model fit is determined, then the importance and interpretation of the specific parameter estimates can be more clearly evaluated. To evaluate model fit, three indices are commonly used: a nonsignificant χ2 goodness-of-fit value; a confirmatory fit index (CFI) greater than .90; a root mean square error of approximation (RMSEA) below 0.05; and the left endpoint of its 90% confidence interval is markedly smaller than 0.05 (with this interval not excessively wide; Raykov & Marcoulides, 2006, 2008). Additional information for the evaluation of model fit based on these fit indices can be found in Byrne (1998), Hu and Bentler (1999), and Marcoulides and Hershberger (1997). We note that because the chi-square test is notoriously sensitive to sample size and has a tendency to reject models that are only marginally inconsistent with the data, primary emphasis is placed on the other reported fit criteria (Raykov & Marcoulides, 2006, 2008).
The proposed unconditional LS model for Anglo mothers’ positive impact provided the following fit criteria: χ2 = (24, N = 168) = 51.01,p < .01, CFI = .96, and RMSEA = .08 (.05; .11); and the unconditional LS model for Latino mothers’ positive impact provided the following fit criteria: χ2 = (24, N = 51) = 31.29,p > .05, CFI = .97, and RMSEA = .08 (.00; .15). An examination of the fit criteria based on the above-outlined guidelines indicates that both the proposed unconditional models for Anglo mothers’ and Latino mothers’ positive impact fit the data well.
Table 3 presents the Mplus factor loading parameter estimates of the two proposed unconditional LS models tested. These coefficients summarize a number of relevant findings with respect to Anglo mothers’ and Latino mothers’ positive impact scores. With respect to Anglo mothers’ positive impact, the estimated coefficient of the Shape factor loadings representing the proportion of change relative to the total change occurring over all time points (i.e., 0, .10, .35, .76, .93, 1.12, 1) reflect a general decline in positive impact. Specifically, there was no evidence of growth in positive impact from age 3 to age 4 (.10,p > .05), a significant decline in positive impact from age 3 to age 5 (.35,p < .05), a significant decline in positive impact from age 3 to age 6 (.76, p < .001), a significant decline in positive impact from age 3 to age 7 (.93,p < .001), and a significant decline in positive impact from age 3 to age 8 (1.12, p < .001). Thus, based on the model, one can readily determine that over all time points measured the actual decline in positive impact was 0, −.083, −.290, −.630, −.772, −.930, −.830, respectively. We note that to compute the specific average decline of scores in positive impact at, for example, age 4, the value of the Shape factor loading at that age (.10) is multiplied by the overall mean value of the Shape factor (−.830, given below) to produce −.083. This value is then added to the mean value of the Level factor (15.38, given below) to provide the estimated average positive impact score at age 4 of 15.30.
There was significant variance in the Level factor (s2 = 15.56, t = 7.27, p < .001) and in the Shape factor (s2 = 7.79, t = 2.92, p < .01), reflecting significant individual differences in starting position as well as individual differences in the amount of change in Anglo mothers’ positive impact over the 7 years. The mean value on the Shape factor was negative and significantly different from zero 0 (μβy= −.83, t = −2.41, p < .05), indicating that overall there was a decline in Anglo mothers’ positive impact from the initial mean value on the Level factor (μαy = 15.38, t = 44.15, p < .01). The nonsignificant covariance between the Level and Shape factors (cov = .13, t = .09, p > .05) showed that for Anglo mothers, the initial levels of positive impact were not related to the decreasing levels of positive impact over time and vice versa.
There was also evidence of significant change in Latino mothers’ positive impact from age 3 to age 9. The estimated coefficients of the Shape factor loadings representing the proportion of change over time (i.e., 0, 1.15, 2.12, 2.13, 1.47, 1.83, 1) also reflect a decline in positive impact. Specifically, there was evidence of a trend toward decline in positive impact from age 3 to age 4 (1.15, p < .10), a significant decline in positive impact from age 3 to age 5 (2.12, p < .05), a significant decline in positive impact from age 3 to age 6 (2.13, p < .05), a significant decline in positive impact from age 3 to age 7 (1.83, p < .05), and a significant decline in positive impact from age 3 to age 8 (1.83, p < .05). Thus, based on the model, one can readily determine that over all time points measured the actual decline in positive impact was 0, −.426, −.784, −.788, − .544, −.677, −.370, respectively.
There was significant variance in the Level factor (s2 = 15.96, t = 3.87, p < .05), but no significant variance in the Shape factor (s2 = 1.74, t = .98, p > .05). These results indicate that there was significant individual variability in the initial status of Latino mothers’ positive impact scores, but no significant individual differences in the amount of change in Latino mothers’ positive impact over 7 years. The mean value on the Shape factor was negative, but not statistically different from 0 (μβy = −.37, t = −1.05, p > .05), indicating that overall there was not a significant decline in Latino mothers’ positive impact from the initial mean value on the Level factor (μβy= 17.27, t = 26.44, p < .01). The nonsignificant covariance between the Level and Shape factors (cov = Ȓ1.18, t = −.80, p > .05) showed that for Latino mothers, initial levels of positive impact were not related to the decreasing levels of positive impact over time and vice versa.
Linear and curvilinear trajectories were also tested. With regard to a linear trajectory, the unconditional model for Anglo mothers’ positive impact provided the following fit criteria: χ2 = (29, N = 168) = 59.60, p < .01, CFI = .96, and RMSEA = .08 (.05; .11), and the unconditional model for Latino mothers’ positive impact provided the following fit criteria: χ2 = (29, N = 51) = 43.07, p < .05, CFI = .94, and RMSEA = .10 (.02; .16). With regard to a curvilinear trajectory, the unconditional model for Anglo mothers’ positive impact provided the following fit criteria: χ2 = (29, N = 168) = 71.49, p < .001, CFI = .94, and RMSEA = .09 (.07; .12) and the unconditional model for Latino mothers’ positive impact provided the following fit criteria: χ2 = (29, N =51) = 44.26, p <.05), CFI = .94, and RMSEA = .10 (.03; .16).
Can These Trajectories Be Predicted by the Disability Status of the Child (The Conditional Model)?
The addition of other variables that can potentially be used to predict the variation in the growth trajectories subsequently requires the examination of a so-called conditional latent curve model (Bollen & Curran, 2006). Figure 2 presents a path diagram that corresponds interchangeably to models for Anglo mothers’ and Latino mothers’ positive impact scores. In the conditional model, the specific predictor of disability status at age 3 (x1) is now considered. Disability status at age 3 was categorized as a binary variable with 0 to indicate children with typical development and a 1 to indicate children with developmental delays.
Figure 2.
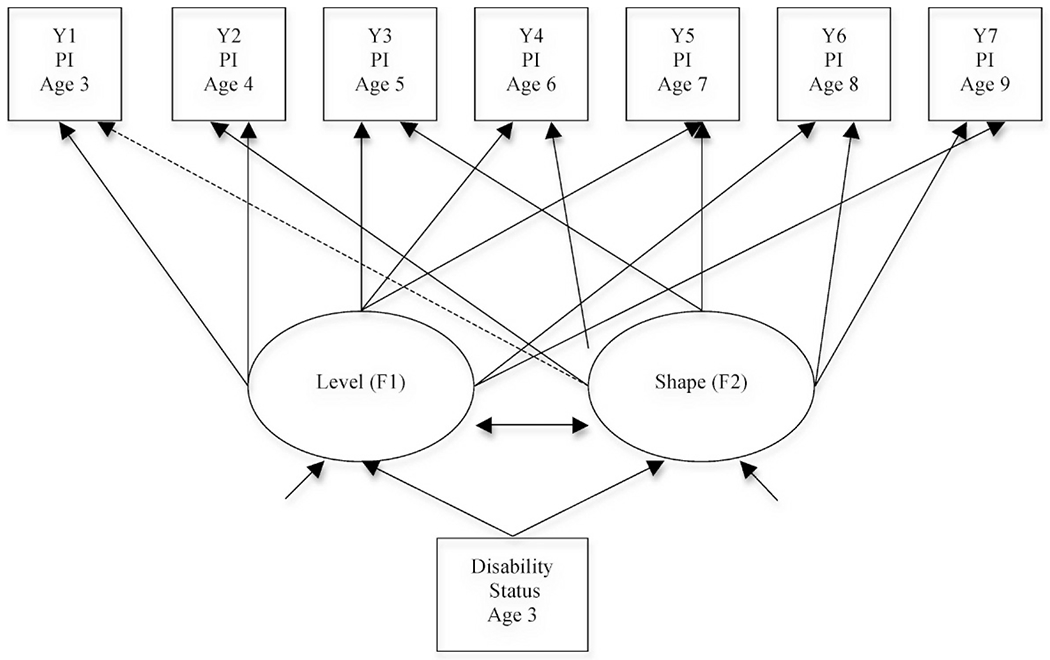
Proposed conditional model for positive impact (PI): Applicable for Anglo mothers and Latino mothers. Figure adapted from Blacher & Baker, 2007.
Table 4 displays the means and standard deviations for Anglo mothers’ positive impact and Latino mothers’ positive impact by disability status. To determine the trajectory of these means, we examined the fit of the proposed conditional LS model for Anglo mothers’ and Latino mothers’ positive impact as presented in Figure 2 using the same criteria described above. We emphasize that the conditional LS model now includes disability status at age 3 (0 = typically developing and 1 = developmental delay) as a predictor. The following fit criteria were obtained for the Anglo and Latino model considered, respectively: (i) χ2 (29) = 57.29, p < .01, CFI = .96, and RMSEA = .08 (.05; .11), and (ii) χ2 (29) = 40.99, p >.05, CFI = .95, and RMSEA = .09 (.00; .15). An examination of the fit criteria based on the previously outlined guidelines indicates that the proposed conditional models also fit the data well.
Table 4.
Means and Standard Deviations for Anglo Mothers’ Positive Impact and Latino Mothers’ Positive Impact by Disability Status
| Variables | Child with typical development | Child with intellectual disability |
|---|---|---|
| Anglo mothers | n = 90 | n = 78 |
| Y1 = positive impact at age 3 | 15.85 (4.45) | 14.56 (4.88) |
| Y2 = positive impact at age 4 | 15.80 (4.94) | 14.56 (4.98) |
| Y3 = positive impact at age 5 | 15.74 (5.05) | 14.02 (4.95) |
| Y4 = positive impact at age 6 | 14.94 (5.34) | 14.45 (4.97) |
| Y5 = positive impact at age 7 | 14.46 (5.72) | 14.35 (5.41) |
| Y6 = positive impact at age 8 | 15.08 (5.36) | 14.39 (5.66) |
| Y7 = positive impact at age 9 | 14.54 (5.63) | 14.58 (5.30) |
| Latino mothers | n = 17 | n = 34 |
| Y1 = positive impact at age 3 | 16.88 (4.61) | 17.53 (4.51) |
| Y2 = positive impact at age 4 | 15.06 (4.63) | 17.25 (4.81) |
| Y3 = positive impact at age 5 | 15.65 (5.30) | 17.10 (5.25) |
| Y4 = positive impact at age 6 | 15.64 (4.27) | 16.36 (5.47) |
| Y5 = positive impact at age 7 | 16.14 (4.88) | 17.70 (5.11) |
| Y6 = positive impact at age 8 | 18.15 (3.41) | 16.05 (5.49) |
| Y7 = positive impact at age 9 | 16.46 (4.01) | 15.80 (5.70) |
Table 5 presents the conditional coefficient estimates for the Level and Shape factors of Anglo mothers’ and Latino mothers’ positive impact regressed on disability status at age 3. These coefficients summarize a number of important findings with respect to the predictive capabilities of disability status. First, disability status significantly predicted the Level factor for Anglo mothers’ positive impact, but not for Latino mothers’ positive impact (γ = −1.51, p < .05, and γ = 0.88, p > .05, respectively), indicating that on average when their child was at age 3, Anglo mothers reported significantly lower initial values on positive impact when their children had developmental delays. However, on average when their child was at age 3, Latino mothers did not report significantly different initial values on positive impact when their children had developmental delays. These regression-like coefficients indicate that a change in disability status (from typically developing to developmental delay) is associated with a specific change in positive impact for Anglo mothers.
Table 5.
Conditional Coefficient Estimates for Level and Shape Factors Regressed on Disability Status
| Model | Unstandardized estimate | Standard error | Critical ratio |
|---|---|---|---|
| Model to explain Level factor | |||
| Anglo PI regressed on DS | −1.51* | .71 | −2.14 |
| Latino PI regressed on DS | .88 | 1.46 | .60 |
| Model to explain Shape factor | |||
| Anglo PI regressed on DS | −1.49* | .75 | 2.01 |
| Latino PI regressed on DS | −.12 | .75 | −.16 |
Note. PI = positive impact; DS = disability status at age 3.
p < .05.
Next, we note that disability status significantly predicted the Shape factor for Anglo mothers’ positive impact, but not for Latino mothers’ positive impact (γ = 1.49, p < .05, and γ = −.12, p > .05, respectively), reflecting that having a child with a developmental delay was associated with changes in the shape of positive impact for Anglo mothers, but not Latino mothers.
Discussion
This study examined Anglo and Latino mothers’ perceived positive impact of a child with or without a disability across seven waves of data. Overall, there were similarities in the trajectory of positive impact for Anglo and Latino mothers. While there were significant individual differences in initial levels of positive impact when children were 3 years old, these initial levels were not related to decreasing levels of positive impact over time. For Anglo mothers, there were significant individual differences in the amount of change in positive impact over time; this was not the case for Latino mothers. Furthermore, for Anglo mothers there was a significant decline in positive impact over the 7 years examined. For Latino mothers, there was no significant decline in positive impact from the initial value.
Although we were initially interested in ethnic differences, the inclusion of the child disability variable had an effect on these differences. In families with a child with ID, at every time point Latino mothers reported higher positive impact than Anglo mothers. In families with a child with TD, Latino mothers also reported higher positive impact than Anglo mothers for five of the seven time points. Anglo mothers of a child with TD were more positive than Anglo mothers with a child with ID at every time point except age 9, when the scores were highly similar. In contrast, Latino mothers of a child with ID were more positive than Latino mothers with a child with TD over the first five time points. Although there was a shift in trend for the final two time points, the magnitude was not statistically significant. Too, for Anglo mothers, having a child with ID was associated with change in the trajectory of positive impact (that is, decreasing over time), whereas for Latino mothers ID was not associated with significant change in the trajectory of positive impact.
Generally speaking, these findings reflect an interaction between ethnicity and disability status and are consistent with other findings that we have reported. In Blacher and McIntyre (2006), Latino mothers reported higher positive impact scores than did Anglo mothers, even after controlling for demographic and well-being variables that differentiated the two groups. That study involved mothers raising young adults with very severe disabilities, unlike the current sample in which the children were young and had only mild-to-moderate intellectual disability. Blacher and Baker (2007), studying families who were a subsample of the present sample, reported similar findings, although only across three waves and without the benefit of the longitudinal methodology presented here. In that previous study, Anglo mothers of children with ID reported less positive views of parenting than Anglo mothers of typically developing children. Although we did not enter a child behavior problems variable into the model (mainly because of the complexity and length of reporting each additional variable), we know that children with ID in this sample have more behavior problems and create more stress on their mothers than children with typical cognitive development (Baker, Blacher, Crnic, & Edelbrock, 2002; Baker et al., 2003; Gerstein, Crnic, Blacher, & Baker, 2009).
These findings beg the question of why there are such significant differences across the two cultural groups in which Latino families with a child with ID reported higher positive impact of the child on their parenting. Although there could be many reasons for this, the extant literature offers two broad categories of explanation: parenting beliefs and cultural context. Because of their parenting beliefs, Latino mothers less often attributed negative behaviors to the child him- or herself and harbored more positive attributions about the child’s potential. An earlier study of attributions by Chavira, Lopez, Blacher, and Shapiro (2000) demonstrated how Latina mothers of adolescents attributed problem behaviors to some other element outside of their adolescents’ control. In addition, when a child with intellectual disability resides in the family home, Latina mothers might extend their caregiving behaviors across more stages of the child’s lifespan (Rueda, Monzo, Shapiro, Gomez, & Blacher, 2005). This expanded maternal role and the belief in the capabilities of the offspring with intellectual disability may have had an adaptive influence on the Latino mothers’ positive perceptions.
Extant literature suggests that Latino mothers embrace the role of motherhood and often approach child-rearing with the attitude of giving more than they receive, sometimes referred to as self-sacrifice or marianismo (Comas-Diaz, 1998; Gil & Vazquez, 1996). These mothers might view the challenges of raising a child with intellectual disability with resignation or even acceptance. Walsh (2003) postulated that resilient mothers possess the ability to make meaning out of adversity, and perhaps these mothers did so. Positive perceptions and acceptance can protect them from some of the negative aspects of disability or of their life circumstances (Taylor, 1983; Zuniga, 2004). Too, acceptance has been shown to be negatively related to anxiety and depression in mothers of children with ID and also to predict maternal well-being (Lloyd & Hastings, 2008). Here, acceptance may have facilitated more positive perceptions of the parenting experience. Thus, the overwhelming historical emphasis in the families and disability literature on stress and adjustment difficulties on the part of mothers in adapting to their children with ID (Blacher & Baker, 2002) may have less relevance to coping in contemporary Latino families.
We also note several methodological caveats. First, we realize that another measure of positive impact may have yielded different findings, particularly if it emphasized different aspects of positive perceptions, or if it was administered at different points in the family’s or child’s lifespan. Second, there are aspects of family or parent adaptability not addressed here, such as religious beliefs, dispositional optimism, siblings with or without disabilities, or social support. We know, for example, that optimism has been identified as a buffer or mediator of behavior problems on parental stress (Baker et al., 2005), but such studies have not yet established this within a cultural context. Religious coping has helped families with a child with disability to find meaning (Crnic, Friedrich, & Greenberg, 1983; Haworth, Hill, & Glidden, 1996; Miltiades & Pruchno, 2002), and for Latino families, in particular, faith is paramount (Skinner, Correa, Skinner, & Bailey, 2001; Skinner, Rodriguez, & Bailey, 1999; Zuniga, 2004). Third, it is also possible that the presence of other children with disabilities in the household may increase burden and, consequentially, decrease the target child’s positive impact. Fourth, another variable that was not examined was social support (number, quality). Social support, whether provided via kinship networks or formal services, has been shown to be especially important to Latino families raising a child with developmental disabilities (Bailey et al., 1999; Blanes-Reyes, Correa, & Bailey, 1999; Correa, Bonilla, & Blanes, 2010). Too, in the Latino population, family members are part of an ethnic network that provides confidente support (Zuniga, 1992). Latino mothers who do not receive such support from family members (perhaps because of having a child with ID) may feel the additional burden (Blacher, Lopez, Shapiro, & Fusco (1997) and report less positive impact.
Finally, we are keenly aware of the lack of “thick description” of culture in this study, and recognize that the ethnicity variable fails to convey a more nuanced description of the cultural context. Nonetheless, the analyses reported do suggest a fairly robust pattern of adaptive perceptions and remarkable resilience of these Latino mothers raising children with ID. Perhaps the benefits of protective factors such as one’s faith or the positive personal transformations inspired by the child with a disability (Skinner, Bailey, Correa, & Rodriguez, 1999) could be harnessed for the purpose of developing positive interventions. After all, despite the extensive demographic disadvantages that the Latino mothers in this study faced, relative to the Anglo mothers, they emerged on the sunny side of the street.
Contributor Information
Jan Blacher, University of California-Riverside, Graduate School of Education, 1207 Sproul Hall, Riverside, CA 92521, USA.
Gazi F. Begum, University of California-Riverside
George A. Marcoulides, University of California-Riverside
Bruce L. Baker, University of California, Los Angeles.
References
- Arbuckle JL (1996). Full information estimation in the presence of incomplete data. In Marcoulides GA & Schumacker RE (Eds.), Advanced structural equation modeling: Issues and techniques (pp. 243–277). Mahwah, NJ: Lawrence Erlbaum. [Google Scholar]
- Bailey D, Skinner D, Correa V, Arcia E, Reyes-Blanes M, Rodriguez P, ... Skinner M (1999). Needs and supports reported by Latino families of young children with developmental disabilities. American Journal of Mental Retardation, 104, 437–451. [DOI] [PubMed] [Google Scholar]
- Baker BL, Blacher J, Crnic KA, & Edelbrock C (2002). Behavior problems and parenting stress in families of three-year old children with and without developmental delays. American Journal on Mental Retardation , 107, 433–444. [DOI] [PubMed] [Google Scholar]
- Baker BL, Blacher J, & Olsson MB (2005). Preschool children with and without developmental delay: Behavioural problems, parents’ optimism and well being. Journal of Intellectual Disability Research, 49, 575–590. [DOI] [PubMed] [Google Scholar]
- Baker BL, McIntyre LL, Blacher J, Crnic K, Edelbrock C, & Low C (2003). Preschool children with and without developmental delay: Behavior problems and parenting stress over time. Journal of Intellectual Disability Research, 47, 217–230. [DOI] [PubMed] [Google Scholar]
- Bayley N (1993). Bayley scales of infant development second edition: Manual. San Antonio, TX: Psychological Corporation. [Google Scholar]
- Blacher J, & Baker BL (2002). The best of AAMR: Families and mental retardation: A collection of notable AAMR journal articles across the 20th century. Washington, DC: American Association on Mental Retardation. [Google Scholar]
- Blacher J, & Baker BL (2007). Positive impact of intellectual disability on families. American Journal of Mental Retardation, 112(5), 330–348. [DOI] [PubMed] [Google Scholar]
- Blacher J, Lopez S, Shapiro J, & Fusco J (1997). Contributions to depression in Latino mothers with and without children with retardation: Implications for caregiving. Family Relations, 46(4), 325–334. [Google Scholar]
- Blacher J, & McIntyre LL (2006). Syndrome specificity and behavioral disorders in young adults with intellectual disability: Cultural differences in family impact. Journal of Intellectual Disability Research, 50(3), 184–198. [DOI] [PubMed] [Google Scholar]
- Blacher J, Shapiro J, Lopez S, Diaz L, & Fusco J (1997). Depression in Latino mothers of children with mental retardation: A neglected concern. American Journal on Mental Retardation, 101, 483–496. [PubMed] [Google Scholar]
- Blanes-Reyes ME, Correa VI, & Bailey DB (1999). Perceived needs and support of Puerto Rican mothers of young children with disabilities living in Puerto Rico and in Florida. Topics in Early Childhood Special Education, 19, 54–63. [Google Scholar]
- Bollen K, & Curran PJ (2006). Latent curve models: A structural equation perspective. New York, NY: Wiley. [Google Scholar]
- Bostrom PK, Broberg M, & Bodin L (2011). Child’s positive and negative impacts on parents: A person-oriented approach to understanding temperament in preschool children with intellectual disabilities. Research in Developmental Disabilities, 32 (5), 1860–1871. [DOI] [PubMed] [Google Scholar]
- Byrne BM (1998). Structural equation modeling with LISREL, PRELIS, and SIMPLIS: Basic concepts, applications, and programming. Mahwah, NJ: Lawrence Erlbaum. [Google Scholar]
- Cauce A, & Domenech-Rodríguez M (2002). Latino families: Myths and realities. In Contreras J, Neal-Barnett A, & Kerns K (Eds.), Latino children and families in the United States (pp. 3–26). Westport, CT: Praeger. [Google Scholar]
- Chavira V, Lopez SR, Blacher J, & Shapiro J, (2000). Mothers’ attributions, emotions, and reactions to the problem behaviors of their children with developmental disabilities. Journal of Child Psychology and Psychiatry, 41(2), 245–252. [PubMed] [Google Scholar]
- Comas-Diaz L (1998). Ethnic minority psychology: Identity, empowerment, and transformation. Cultural Diversity and Mental Health, 4(3), 151–152. [DOI] [PubMed] [Google Scholar]
- Correa V, Bonilla Z, & Blanes M (May 2010). Social support networks of single Puerto Rican mothers of young children with disabilities. Journal of Child and Family Studies, 20, 66–77. [Google Scholar]
- Crnic KA, Friedrich WN, & Greenberg MT (1983). Adaptation of families with mentally retarded children: A model of stress, coping, and family ecology. American Journal on Mental Deficiency, 88, 125–136. [PubMed] [Google Scholar]
- Donenberg G, & Baker BL (1993). The impact of young children with externalizing behaviors on their families. Journal of Abnormal Child Psychology, 21, 179–198. [DOI] [PubMed] [Google Scholar]
- Duncan TE, Duncan SC, Li F, & Strycker LA (1999). An introduction to latent variable growth curve modeling: Concepts, issues, and applications. Mahwah, NJ: Lawrence Erlbaum. [Google Scholar]
- Duncan TE, Duncan SC, & Strycker LA (2006). An introduction to latent variable growth curve modeling: Concepts, issues and applications (2nd ed). Mahwah, NJ: Lawrence Erlbaum. [Google Scholar]
- Durand VM (2011). Optimistic parenting. Hope and help for you and your challenging child. Baltimore, MD: Paul H. Brookes. [Google Scholar]
- Dura-Vila G, Dein S, & Hodes M (2010). Children with intellectual disability: A gain not a loss: Parental beliefs and family life. Clinical Child Psychology and Psychiatry, 15(2), 171–184. [DOI] [PubMed] [Google Scholar]
- Ekas NV, Lichenbrock DM, & Whitman TL (2010). Optimism, social support, and well-being in mothers of children with autism spectrum disorder. Journal of Autism and Developmental Disorders, 40, 1274–1284. [DOI] [PubMed] [Google Scholar]
- Farber B (1959). Effects of a severely mentally retarded child on family integration. Monographs of the Society for Research in Child Development 24(2, Serial No. 71). [Google Scholar]
- Folkman S (1997). Positive psychological states and coping with severe stress. Social Science and Medicine, 45(8), 1207–1221. [DOI] [PubMed] [Google Scholar]
- Gerstein ED, Crnic KA, Blacher J, & Baker BL (2009). Resilience and the course of daily parenting sress in families of young children with intellectual disabilities. Journal of Intellectual Disability Research, 53, 981–997. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gil RM , & Vazquez CI (1996). The Maria paradox: How Latinos can merge old world tradition with new world self-esteem. New York, NY: G. P. Putnam’s Sons. [Google Scholar]
- Grebler AM (1952). Parental attitudes toward mentally retarded children. American Journal of Mental Deficiency, 56, 475–483. [PubMed] [Google Scholar]
- Hastings RP, Beck A, & Hill C (2005). Positive contributions made by children with intellectual disability in the family: Mothers’ and fathers’ perceptions. Journal of Intellectual Disabilities, 9(2), 155–165. [DOI] [PubMed] [Google Scholar]
- Haworth A, Hill A, & Glidden L (1996). Measuring religiousness in parents of children with developmental disabilities. Mental Retardation, 34(5), 271–279. [PubMed] [Google Scholar]
- Helff CM, & Glidden LM (1998). More positive or less negative? Trends in research on adjustment of families rearing children with developmental disabilities. Mental Retardation, 36(6), 457–464. [DOI] [PubMed] [Google Scholar]
- Hu L, & Bentler PM (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling, 6, 1–55. [Google Scholar]
- Lickenbrock DM, Ekas NV, & Whiteman TL (2011). Feeling good, feeling bad: Influences on maternal perceptions of the child and marital adjustment on well-being in mothers of children with autism spectrum disorders. Journal of Autism and Developmental Disorders, 41, 848–858. [DOI] [PubMed] [Google Scholar]
- Lloyd T, & Hastings RP (2008). Psychological variables as correlates of adjustment in mothers of children with intellectual disabilities: Cross-sectional and longitudinal relationships. Journal of Intellectual Disability Research, 52, 37–48. [DOI] [PubMed] [Google Scholar]
- Lloyd T, & Hastings RP (2009). Hope as a psychological resilience factor in mothers and fathers of children with intellectual disabilities. Journal of Intellectual Disability Research, 53, 957–968. [DOI] [PubMed] [Google Scholar]
- Lomax RG (2007). Statistical concepts. Mahwah, NJ: Lawrence Erlbaum. [Google Scholar]
- Marcoulides GA, & Hershberger SL (1997). Multivariate statistical methods: A first course. Mahwah, NJ: Lawrence Erlbaum. [Google Scholar]
- Marcoulides GA, & Saunders C (2006). PLS: A silver bullet? A commentary on sample size issues in PLS modeling. MIS Quarterly, 30(2), 3–10. [Google Scholar]
- McArdle JJ, & Anderson E (1990). Latent variable growth models for research on aging. In Birren JE & Schaie KW. Handbook of the psychology of aging (pp. 21–44). New York, NY: Academic Press. [Google Scholar]
- Miersschaut M, Roeyers H, & Warreyn P (2010). Parenting in families with a child with autism spectrum disorder and a typically developing child: Mothers’ experiences and cognitions. Research in Autism Spectrum Disorders, 4, 661–669. [Google Scholar]
- Miltiades HB, & Pruchno R (2002). The effect of religious coping on caregiving appraisals of mothers of adults with developmental disabilities. Gerontologist, 42, 82–91. [DOI] [PubMed] [Google Scholar]
- Muthén LK, & Muthén BO (2002). How to use a Monte Carlo study to decide on sample size and determine power. Available at http://www.statmodel.com/download/FinalSEMsingle.pdf [Google Scholar]
- Muthén LK, & Muthén BO (2006). Mplus user’s guide. Los Angeles, CA: Author. [Google Scholar]
- Olsson MB, & Larsman P, & Hwang PC (2008). Relationships among risk, sense of coherence, and well-being in parents of children with and without intellectual disabilities. Journal of Policy and Practice in Intellectual Disabilities, 5(4), 227–236. [Google Scholar]
- Patterson JM, Turnbull AP, Behr SK, Murphy DL, Marquis JG, & Blue-Banning MJ (1993). Cognitive coping, families and disability. Baltimore, MD: Paul H. Brookes. [Google Scholar]
- Phelps KW, McCammon SL, Wuensch KL, & Goldren JA (2009). Enrichment, stress, and growth from parenting an individual with autism spectrum disorder. Journal of Intellectual and Developmental Disability, 34, 133–141. [DOI] [PubMed] [Google Scholar]
- Rapanaro C, Bartu A, & Lee AH (2008). Perceived benefits and negative impact of challenges encountered in caring for young adults with intellectual disabilities in the transition to adulthood. Journal of Applied Research in Intellectual Disabilities, 21, 34–47. [Google Scholar]
- Raykov T, & Marcoulides GA (2006). A first course in structural equation modeling. Mahwah, NJ: Lawrence Erlbaum. [Google Scholar]
- Raykov T, & Marcoulides GA (2008). An introduction to applied multivariate analysis. New York, NY: Routledge. [Google Scholar]
- Rueda R, Monzo L, Shapiro J, Gomez J, & Blacher J (2005). Cultural models of transition: A view from Latino mothers of young adults with developmental disabilities. Exceptional Children, 71, 401–414. [Google Scholar]
- Sabogal F, Marín G, Otero-Sabogal R, Marín BV, & Perez-Stable EJ (1987). Hispanic familism and acculturation: What changes and what doesn’t? Hispanic Journal of Behavioral Sciences, 9(4), 397–412. [Google Scholar]
- Scallan S, Senior J, & Reilly C (2011). William syndrome: Daily challenges and positive impact on the family. Journal of Applied Research in Intellectual Disabilities, 24, 181–188. [Google Scholar]
- Skinner D, Bailey D, Correa V, & Rodriguez P (1999). Narrating self and disability: Latino mothers’ construction of identities vis-à-vis their child and special needs. Exceptional Children, 65, 481–495. [Google Scholar]
- Skinner D, Correa V, Skinner M, & Bailey D (2001). The role of religion in the lives of Latino families of young children with developmental delays. American Journal on Mental Retardation, 106,297–313. [DOI] [PubMed] [Google Scholar]
- Skinner D, Rodriguez P, & Bailey D (1999). Qualitative analysis of Latino parents’ religious interpretations of their child’s disability. Journal of Early Intervention, 22, 271–285. [Google Scholar]
- Taylor SE (1983). Adjustment to threatening events. A theory of cognitive adaptation. American Psychologist, 38, 1161–1173. [Google Scholar]
- Taylor SE, Lerner JS, Sherman DK, Sage RM, & McDowell NK (2003a). Are self-enhancing cognitions associated with healthy or unhealthy biological profiles? Journal of Personality and Social Psychology, 85(4), 605–615. [DOI] [PubMed] [Google Scholar]
- Taylor SE, Lerner JS, Sherman DK, Sage RM, & McDowell NK (2003b). Portrait of the self-enhancer: Well adjusted and well liked or maladjusted and friendless. Journal of Personality and Social Psychology, 84(1), 165–176. [PubMed] [Google Scholar]
- Trute B, Benzies KM, Worthington C, Reddon JR, & Moore M (2010). Accentuate the positive to mitigate the negative: Mother psychological coping resources and family adjustment in childhood disability. Journal of Intellectual and Developmental Disability, 35, 36–43. [DOI] [PubMed] [Google Scholar]
- U.S. Census Bureau. (2011). State and county quick facts. Available at http://quickfacts.census.gov/qfd/states/06000.html [Google Scholar]
- Walsh F (2003). Family resilience: A framework for clinical practice. Family Process, 42, 1–18. [DOI] [PubMed] [Google Scholar]
- Zuniga ME (1992). Families with Latino roots. In Lynch EW & Hanson MJ (Eds.), Developing cross-cultural competence (pp. 151–179). Baltimore, MD: Paul H. Brookes. [Google Scholar]
- Zuniga ME (2004). Families with Latino roots. In Lynch EW & Hanson MJ (Eds.), Developing cross-cultural competence (pp. 179–218). Baltimore, MD: Paul H. Brookes. [Google Scholar]