

Abstract
BACKGROUND AND PURPOSE: This study was undertaken to analyze enhancement patterns of the dura around sellar tumors and to compare the results with tumor invasion or compression of the cavernous sinuses. Postoperative enhancement patterns on MR images were compared with preoperative findings.
METHODS: Contrast-enhanced coronal and sagittal MR images were examined prospectively in 96 patients with sellar tumors (65 macroadenomas, 15 microadenomas, 14 Rathke cleft cysts, and two chordomas at the sella). All patients underwent surgical treatment, and pre- and postsurgical features on MR images were compared.
RESULTS: Presurgical MR images showed dural enhancement in 36.5% of the patients: asymmetric tentorial enhancement in 24 patients, symmetric tentorial enhancement in seven, and sphenoidal ridge or clivus enhancement in four. Asymmetric tentorial enhancement disappeared after surgical decompression in seven patients. For evaluation of cavernous sinus invasion ipsilateral to the enhancement, sensitivity and specificity of the asymmetric tentorial enhancement sign were 81.3% and 86.3%, respectively. Sensitivity and specificity of the sign were 42.9% and 93.6% for cavernous sinus involvement, including compression and invasion.
CONCLUSION: Asymmetric tentorial enhancement is a useful sign in the diagnosis of invasion or severe compression of the cavernous sinus by sellar tumor. The sign may represent venous congestion or collateral flow in the tentorium due to obstructed flow in the medial portion of the cavernous sinus.
Enhancement of thickened dura on MR images is observed in association with various pathologic processes in the intracranial space (1). The clinical implication of prominent dural enhancement adjacent to a neoplasm has been discussed mainly in conjunction with the dural tail sign associated with meningiomas (2, 3). Few specific features of dural enhancement associated with other brain tumors have been reported.
We recently found that many sellar tumors show dural enhancement on MR images. In this study, we evaluated the features of prominent dural enhancement surrounding the sella to define its characteristics, especially as an indicator of cavernous sinus involvement.
Methods
Between 1990 and 2000, 104 patients with intra- and suprasellar mass lesions were examined prospectively using MR imaging in our institutes before surgical exploration. Patients were excluded from this study if they had a purely suprasellar tumor, an inflammatory process affecting the sella, a lesion associated with carotid-cavernous fistula, or incomplete imaging studies. A total of 96 patients were included in the analysis (43 men and 53 women, 18 to 78 years old, with a mean age of 45 years). All patients underwent transsphenoidal surgery, and their tumors were proved histopathologically. The extent of macroscopic invasion of each tumor was determined at the time of surgery.
Adenomas 10 mm or larger were designated as macroadenomas, and those less than 10 mm in diameter were defined as microadenomas. Sixty-five patients had macroadenomas, 15 had microadenomas, 14 had Rathke cleft cysts, and two had chordomas. Two of 65 macroadenomas were recurrent tumors, arising 5 and 6 years, respectively, after initial surgery. One microprolactinoma was a recurrent adenoma arising 2 years after endocrinologic treatment by surgery. Four of the 14 Rathke cleft cysts were recurrent lesions.
MR imaging was performed on either a 1.5-T or a 1.0-T MR unit. All examinations were performed with spin-echo T1-weighted sequences in coronal and sagittal planes with a 3- to 4-mm section thickness and 0.5-mm or no interleaving. Gadopentetate dimeglumine was administered intravenously at a dose of 0.1 mmol/kg to all patients. T1-weighted MR images were obtained in coronal and sagittal planes in all patients, and additional axial sections were obtained in five patients. Total examination time was about 40 to 45 minutes per patient, including a 10- to 15-minute waiting period after contrast injection. Fat-saturation sequences were not obtained.
Tentorial Enhancement and Other Dural Enhancement
We evaluated meningeal enhancement on and around the anterior clinoid processes, sphenoidal ridges, and floor of the middle fossa, clivus, and tentorium. Dural enhancement is subtle in healthy subjects, whereas dural thickening is an abnormal sign on spin-echo T1-weighted images (1). When clear dural enhancement was observed in continuity with the cavernous sinus or diaphragma sella, it was considered abnormal dural enhancement due to sellar disease.
Invasion into or Compression on the Cavernous Sinus
Because it is not possible to obtain biopsy specimens from the medial wall of the cavernous sinus, only surgical detection of real macroscopic infiltration can be regarded as definitive invasion into the cavernous sinus. Tumor invasion into the sinus was identified by direct observation of the carotid artery wall or the perforated medial cavernous sinus wall with the surgical microscope or an endoscope, or by a curette touching on the sinus trabeculae. When the medial wall was intact at surgery and no venous filling was observed in the medial part of the sinus on contrast-enhanced MR images, the tumor was judged to be compressing the cavernous sinus. Patients without these signs of invasion or compression were considered to have an intact cavernous sinus.
Evaluation of the Data
A pituitary surgeon performed transsphenoidal surgery in all cases and evaluated the extent of macroscopic invasion into the cavernous sinus during surgery. A neuroradiologist and a neurosurgeon, blinded to surgical findings and recurrent cases, reviewed the images independently. κ statistics were calculated for the assessment of presence of asymmetric tentorial enhancement (4). After interobserver assessment, final results were arrived at by consensual agreement. Results were estimated for the diagnosis of cavernous sinus involvement or invasion by means of sensitivity and specificity (5).
Results
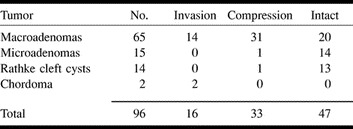
Table 1 shows the number of occurrences of compression and invasion of the cavernous sinus for each type of tumor. For macroadenomas, invasion into the sinus was observed in 21.5% of the patients, and compression on the sinus was seen in 47.7%.
TABLE 1:
Sellar tumors and their cavernous sinus involvement
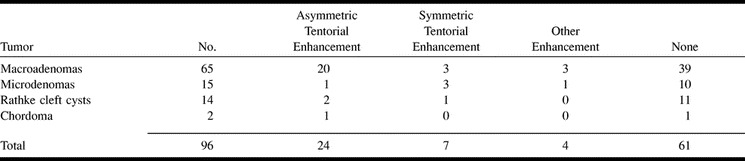
Findings of dural enhancement are summarized in Table 2. MR images showed dural enhancement in 35 (36.5%) of 96 patients: in 40% of macroadenomas, 33.3% of microadenomas, and 21.4% of Rathke cleft cysts. Tentorial enhancement was the most frequent type of abnormal enhancement. Other abnormal findings included enhancement in the retroclival region and around the tuberculum sellae and proximal sphenoidal ridge. Sagittal MR images provided the best information on tentorial enhancement from the lateral wall of the cavernous sinus through the tentorial edge. Coronal views were helpful for assessing tentorial enhancement in a plane containing the prepontine cistern. However, assessment of the posterior end of the cavernous sinus was frequently difficult on coronal sections. Coronal images through the anterior clinoid process best showed dural enhancement over the minor wing of the sphenoid bone. Axial images showed dural enhancement along the sphenoidal ridge and tentorial edge in a few cases.
TABLE 2:
Sellar tumors and dural enhancement
Macroadenomas
Postoperative follow-up ranged from 1 month to 10 years, with an average of 5.7 years. Unilateral or bilateral compression on the cavernous sinus was observed in 31 of 65 patients, and unilateral invasion into the cavernous sinus was observed in 14 patients. In 65 patients with macroadenomas, 26 had dural enhancement: 20 with asymmetric tentorial enhancement, three with symmetric tentorial enhancement, two with sphenoidal ridge and anterior clinoid enhancement, and one with clival enhancement. All 20 patients with asymmetric tentorial enhancement had large adenomas compressing or invading either side of the cavernous sinus; none had an intact cavernous sinus. Seven of 20 patients with asymmetric tentorial enhancement lost the sign during follow-up as early as 1 month after surgery. The asymmetric tentorial enhancement sign did not disappear after surgery in the other 13 patients; all had prolactinomas infiltrating into the dura mater surrounding the sella.
Microadenomas
Postoperative follow-up for patients with microadenomas ranged from 3 months to 10 years, with an average of 4.1 years. Unilateral compression on the cavernous sinus was observed in only one patient, and no invasion into the cavernous sinus was observed. In 15 patients with microadenomas, five showed dural enhancement: one with asymmetric tentorial enhancement, three with symmetric tentorial enhancement, and one with clival dural enhancement. The patient with asymmetric tentorial enhancement had a 5-mm prolactin-secreting adenoma on the side of clear tentorial enhancement; however, the same preoperative MR examination showed no sign of compression on the medial wall of the cavernous sinus. This patient lost the enhancement on MR images taken 1 year after surgery. In no other case did the enhancement change or disappear after surgery.
Rathke Cleft Cysts
Postoperative follow-up of patients with Rathke cleft cysts ranged from 3 months to 9 years, with an average of 3.6 years. Unilateral compression on the cavernous sinus was observed in one patient. No patient had invasion into the cavernous sinus. In 10 patients with Rathke cleft cysts, two showed asymmetric tentorial enhancement. They did not lose the enhancement on follow-up images obtained after surgery.
Chordoma
In two patients, chordoma originated in the sella and the clivus, extending into the right cavernous sinus in one and into the bilateral cavernous sinuses in the other. In the latter patient (case 3), contrast-enhanced MR images showed asymmetric tentorial and bilateral petroclival enhancement of the dura. The enhanced areas of the dura were the most likely to be invaded by the chordoma, although we have no histologic confirmation of dural invasion in these areas.
Illustrative Cases
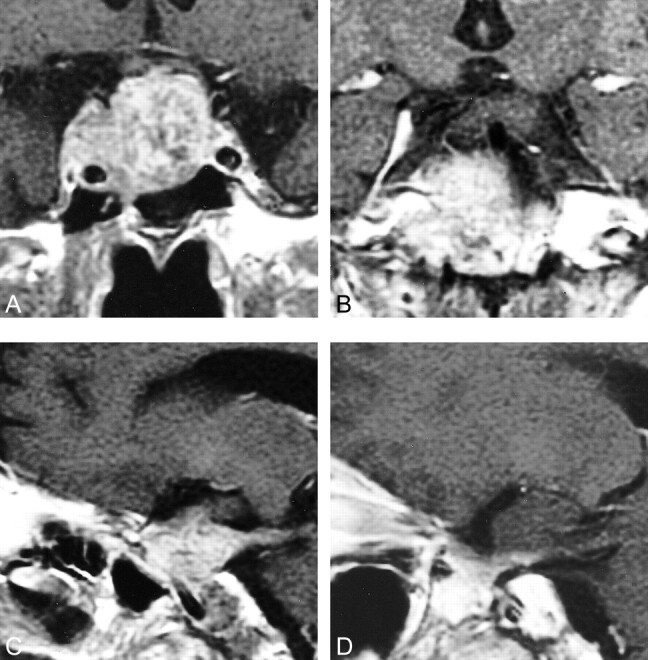
Case 1.—A 46-year-old woman presented with progressive acromegalic features (Fig 1). Preoperative MR images showed sellar to suprasellar tumor with slight enhancement of the pituitary gland on the left side. MR images and intraoperative findings revealed severe compression of the right cavernous sinus. Preoperative coronal and sagittal images showed asymmetric tentorial enhancement on the side of compression. This finding gradually disappeared on MR images obtained 10 months after surgery.
fig 1.

Case 1: 46-year-old woman with a growth hormone–secreting adenoma.
A, Coronal T1-weighted MR image after administration of contrast material shows a large sellar tumor compressing the right cavernous sinus. The left cavernous sinus is enhanced and normal in shape.
B, T1-weighted MR image shows clearly enhanced tentorium on the right side.
C and D, Sagittal T1-weighted images show linear enhancement of the tentorium from the posterior portion of the cavernous sinus on the right side (C). Note asymmetric tentorial enhancement sign.
E, Postoperative T1-weighted MR image after administration of contrast material shows enlarged posterior part of the cavernous sinus; however, no tentorial enhancement was seen preoperatively (C).
Case 2.—A 26-year-old man presented with visual disturbance (Fig 2). Preoperative MR images showed a sellar to suprasellar tumor with the flat pituitary gland on the right side. MR images and intraoperative findings revealed adenoma invasion into the left cavernous sinus. Preoperative sagittal MR images showed asymmetric tentorial enhancement on the side of invasion. This finding did not change on MR images obtained 2 years after subtotal removal and postoperative irradiation.
fig 2.

Case 2: 26-year-old man with a nonfunctioning adenoma.
A, Coronal T1-weighted MR image shows a sellar tumor invading the left cavernous sinus.
B and C, Sagittal T1-weighted MR images show tentorial enhancement in connection with the cavernous sinus, more prominent on the left (C) than on the right (B).
Case 3.—A 64-year-old man had a tumor in the sella and the clivus extending into the bilateral cavernous sinuses (Fig 3). Asymmetric enhancement of the tentorium was seen on contrast-enhanced MR images. The enhancement sign still persisted 14 months after partial (about 70%) removal of the tumor and postoperative irradiation.
fig 3.
Case 3: 64-year-old man with a chordoma.
A and B, Coronal T1-weighted MR images show sellar tumor infiltrating into both cavernous sinuses and into the right tentorium.
C and D, Sagittal T1-weighted MR images show bilateral thick tentorial enhancement with dominance on the right side.
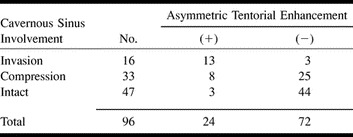
κ Value, Sensitivity, and Specificity of the Asymmetric Tentorial Enhancement Sign for the Diagnosis of Cavernous Sinus Involvement
κ was .78 for recognition of asymmetric tentorial enhancement on MR images. Table 3 shows cavernous sinus involvement versus presence of asymmetric tentorial enhancement on MR images preoperatively. For the diagnosis of invasion and compression together, the sensitivity of the sign was 42.9%. The sign has a specificity of 93.6% in distinguishing the intact cavernous sinus from cavernous sinus involvement. The sensitivity of the asymmetric tentorial enhancement sign was 81.3% for the diagnosis of cavernous sinus invasion among sellar tumors. The specificity of the sign for distinguishing cavernous sinus invasion from either the uninvolved cavernous sinus or cavernous sinus compression was 86.3%.
TABLE 3:
Asymmetric tentorial enhancement and cavernous sinus involvement of sellar tumors
Discussion
Sagittal MR images showed tentorial enhancement on the side of an obstructed cavernous sinus caused by sellar tumor invasion or compression. Many of the asymmetric tentorial enhancement signs disappeared or were reduced in intensity after simple decompression of the sella through a transsphenoidal approach. The transient nature of the enhancement suggests that asymmetric tentorial enhancement represents venous congestion or neovascularization caused by unilateral mechanical obstruction of the cavernous sinus. The cavernous venous plexus receives blood primarily from the superior ophthalmic vein (6). Minor venous supply to the sinus comes from the cortical veins: the middle cerebral veins through direct communication and the anterior petrosal veins via the superior petrosal sinus. The main compartment of the venous flow runs medial to the internal carotid artery. The venous network converges to form the inferior petrosal sinus, which drains down to the jugular vein. Compression on the medial part of the venous plexus by a slowly expanding tumor may obstruct the venous flow from the anterior portion into the inferior petrosal sinus. Meanwhile, the posterior part of the sinus still has to receive venous blood from cortical veins other than the superior ophthalmic vein. The resultant congestion in and around the lateral and posterior portions of the sinus may lead to venous dilatation or hypervascular reaction of the tentorium.
Symmetric tentorial enhancement was observed less frequently than asymmetric tentorial enhancement: we found three instances of symmetrical enhancement in macroadenomas and three in microadenomas. Because microadenomas exert little compression on the cavernous sinus, and because the symmetric enhancement did not disappear after surgical decompression of the cavernous sinus, the symmetric tentorial enhancement was regarded as a normal finding.
In the tentorium, sinuses receive venous blood from the brain and the cerebellum. Bridging veins to the tentorial free edge arise from the brain stem, forming the tentorial sinus in 7.6% of cadaveric hemispheres (7). These rare bridging veins together with the draining tentorial sinus may be seen as tentorial enhancement in subjects without congestion.
The dural tail sign was initially proposed as a specific sign of convexity meningiomas (8). Various kinds of intracranial pathologic changes have been found to show dural enhancement adjacent to the lesions (3). Only two cases of a dural tail in association with a pituitary adenoma have been reported in the English-language literature (9, 10). No reports have yet been published regarding the frequency of dural enhancement around pituitary tumors. We prospectively found that 20 (30.8%) of 65 patients with histologically proved macroadenomas had asymmetric tentorial enhancement. Sufficient scanning beyond the walls of the cavernous sinus and careful observation yielded frequent detection of abnormal dural enhancement around the sella.
Our study revealed that 20% of macroadenomas showed macroscopic invasion into the cavernous sinus. Cavernous sinus invasion reportedly occurs in 6% to 10% of patients at macroscopic observation during surgery (11, 12). In experienced hands, 6% to 20% of pituitary adenomas recur after initial remission (13, 14). This rate is far less than one might expect from the data of histologic dural infiltration; histopathologic infiltration into the adjacent dura has been found in 45% to 85% of patients who have undergone transsphenoidal surgery (15, 16). This means that gross invasiveness bears a more reliable prognostic value than does histologic dural infiltration in predicting the recurrence of adenoma. Preoperative diagnosis of cavernous sinus invasion by pituitary adenoma has been reported with internal carotid artery encasement and obstruction of the carotid sulcal venous compartment on coronal MR images (17). Asymmetric tentorial enhancement signs on MR images provide further preoperative information about difficult adenomas, leading to a better understanding of the prognosis. Postoperative disappearance of the sign assures sufficient decompression of the cavernous sinus. Note that asymmetric tentorial enhancement on MR images does not always indicate direct tumor invasion into the tentorium beyond the cavernous sinus.
Conclusion
We prospectively analyzed enhancement patterns of the dura around sellar tumors, with particular attention to the involvement of the cavernous sinus. Dural enhancement was seen on MR images in 36.5% of patients with parasellar tumors. An asymmetric tentorial enhancement sign indicates either invasion into or compression on the ipsilateral cavernous sinus. The sensitivity of the asymmetric tentorial enhancement sign was 81.3% for the diagnosis of cavernous sinus invasion into sellar tumors. This sign frequently disappears after decompression surgery for pituitary adenomas, suggesting that the sign reflects venous congestion but no direct invasion of the tentorium. Symmetric tentorial enhancement and little asymmetric tentorial enhancement may represent normal variants.
Acknowledgments
We thank Dr. Hirofumi Nioka, Department of Neurosurgery, Yujin-Yamazaki Hospital, Shiga, for referring his patient and for his technical support.
Footnotes
Address reprint requests to Y. Nakasu, MD, Department of Neurosurgery, Yasu Hospital, Yasu, Shiga, 520-2331, Japan.
References
- 1.Sze G. Diseases of the intracranial meninges: MR imaging features. AJR Am J Roentgenol 1993;160:727-733 [DOI] [PubMed] [Google Scholar]
- 2.Gupta S, Gupta RK, Banerjee D, Gujral RB. Problems with the “dural tail” sign. Neuroradiology 1993;35:541-542 [DOI] [PubMed] [Google Scholar]
- 3.Bourekas EC, Wildenhain P, Lewin JS, et al. The dural tail sign revisited. AJNR Am J Neuroradiol 1995;16:1514-1516 [PMC free article] [PubMed] [Google Scholar]
- 4.Kerr M. Issues in the use of kappa. Invest Radiol 1991;26:78-83 [DOI] [PubMed] [Google Scholar]
- 5.Krieg AF, Ggambino R, Galen RS. Why are clinical laboratory tests performed? When are they valid? JAMA 1975;233:76-78 [PubMed] [Google Scholar]
- 6.Knosp E, Mueller G, Perneczky A. Anatomical remarks on the fetal cavernous sinus and on the veins of the middle cranial fossa. In: Dolenc VV, ed. The Cavernous Sinus. Wien: Springer; 1987:104–116
- 7.Matsushima T, Suzuki SO, Fukui M, Rhoton AL Jr, De Oliveira E, Ono M. Microsurgical anatomy of the tentorial sinuses. J Neurosurg 1989;71:923-928 [DOI] [PubMed] [Google Scholar]
- 8.Goldsher D, Litt AW, Pinto RS, Bannon KR, Kricheff II. Dural “tail” associated with meningiomas on GD-DTPA–enhanced MR images: characteristics, differential diagnostic value and possible implications for treatment. Radiology 1990;176:447-450 [DOI] [PubMed] [Google Scholar]
- 9.Koenigsberg RA, Patil K. Pituitary apoplexy associated with dural (tail) enhancement. AJR Am J Roentgenol 1994;163:227. [DOI] [PubMed] [Google Scholar]
- 10.Celli P, Cervoni L, Cantore G. Dural tail in pituitary adenoma. J Neuroradiol 1997;24:68-69 [PubMed] [Google Scholar]
- 11.Ahmadi J, North CM, Segall HD, Zee CS, Weiss MH. Cavernous sinus invasion by pituitary adenomas. AJNR Am J Neuroradiol 1985;6:893-898 [DOI] [PubMed] [Google Scholar]
- 12.Fahlbusch R, Buchfelder M. Transsphenoidal surgery of parasellar pituitary adenomas. Acta Neurochir (Wien) 1988;92:93-99 [DOI] [PubMed] [Google Scholar]
- 13.Laws ER Jr. Surgical management of pituitary tumors. In: Mzzaferri EL, Samaan N, eds. Endocrine Tumours. Boston: Blackwell; 1993:215–222
- 14.Fahlbusch R, Buchfelder M, Honegger J, Nomikos P. Nonfunctional pituitary adenomas. In: Krisht AF, Tindall GT, eds. Pituitary Disorders: Comprehensive Management. Baltimore: Lippincott Williams & Wilkins; 1999;281–285
- 15.Selman WR, Lans EF, Scheithauer BW. The occurrence of dural invasion in pituitary adenomas. J Neurosurg 1986;64:402-407 [DOI] [PubMed] [Google Scholar]
- 16.Landolt AM, Schiller A. Surgical technique: transsphenoidal approach. In: Landolt AM, Vance ML, Reilly PL, eds. Pituitary Adenomas. New York: Churchill Livingstone; 1996:315–331
- 17.Cottier J-P, Destrieux C, Brunereau L, et al. Cavernous sinus invasion by pituitary adenoma: MR imaging. Radiology 2000;215:463-469 [DOI] [PubMed] [Google Scholar]